
ABSTRACT
Clinical relevance
Anisometropia can affect visual development in children. Investigations of anisometropia in high myopes would explore potential causes related to anisometropia, highlighting the management of anisometropia in high myopia.
Background
The prevalence of anisometropia ranged from 0.6% to 4.3% in general paediatric population and from 7% to 14% in myopes. Anisometropia is regarded as an associated factor for myopia development, while myopia progression is a stimulus driving anisometropic development. The purpose of this study was to investigate the prevalence of anisometropia and its association with refraction development in Chinese children with high myopia.
Methods
In the cohort study, a total of 1,577 highly myopic (spherical equivalent ≤−5.0D) children aged 4–18 years were included. Refractive parameters (dioptre of sphere, dioptre of cylinder, corneal curvature radius, and axial length) of both eyes were measured after cycloplegia. The prevalence and degree of anisometropia were compared among refractive groups (non-parametric tests or chi-square tests), and regression analyses were used to determine associated factors of anisometropia. The statistical significance was set to P < 0.05 (two-tailed).
Results
In highly myopic children with a mean (standard deviation) age of 13.06 (2.80) years, the proportions of spherical equivalent anisometropia, cylindrical anisometropia and spherical anisometropia ≥1.00 D were 34.5%, 21.9% and 39.9%, respectively. There was more spherical equivalent anisometropia associated with more severe astigmatism (P for trend <0.001). In the multivariate regression analysis, more spherical equivalent anisometropia, cylindrical anisometropia and spherical anisometropia were associated with higher degrees of astigmatism (standard beta = −0.175, −0.148 and −0.191, respectively). More spherical anisometropia was associated with better spherical power (standard beta = 0.116).
Conclusion
The proportion of anisometropia in highly myopic children was high, compared with previously reported general population, and more severe anisometropia was associated with higher degree of cylindrical power, but not spherical power.
Introduction
Anisometropia is a unique example of human ocular development where two eyes grow asymmetrically despite being exposed to the same genetics and environmental influences.Citation1–4 Anisometropia was usually considered to be caused by the difference of fundamental axial length between the right and left eyes,Citation5–7 but there was also other evidence to suggest that anisometropia can be attributed to the interocular difference of optical parameters, such as spherical power and cylindrical power.Citation7–9 Studies on general paediatric population suggest that the prevalence of anisometropia ranges from 0.6% to 4.3%, covering a large proportion of children worldwide, but in myopes, this estimate is likely between 7% and 14%.Citation6,Citation10–15 If unaddressed, anisometropia can affect visual development in children and cause complications including strabismus and anisometropic amblyopia.Citation1,Citation16,Citation17
The relationship between myopia and anisometropia is complicated and is far from consensus. On the one hand, the asymmetric lengthening of one eye has been hypothesised to originate from stochastic factors or randomness in the process of eye development.Citation18 Thus, anisometropia also inevitably leads to concomitant unilateral myopia progression in some people and is regarded as an associated factor for myopia development.Citation1,Citation18,Citation19 On the other hand, some research hypothesises that progression of myopia is the stimulus promoting anisometropia in children.Citation6,Citation20
According to the potential interrelation of anisometropia and myopia, it is plausible that anisometropia would be associated with high myopia, although investigations of anisometropia in high myopes have rarely been reported. According to one of the previous studies performed in high myopes, anisometropia may affect the development of high myopia,Citation21 but this relationship is far from being clearly illustrated. Moreover, anisometropia has been involved in the surgical treatment of high myopia.Citation22–24 While the sample sizes of these studies are suboptimal, they do hint to relationships between high myopes and anisometropia severity.
Considering the research gaps about how high myopia could affect anisometropia, this work utilised the large sample of highly myopic eyes in the Shanghai Child and Adolescent Large-scale Eye Study – High Myopia (SCALE-HM) to describe the distribution of anisometropia in this population group. Moreover, ocular biometrics were compared between anisometropic and non-anisometropic children to explore potential causes and factors related to anisometropia. The present results may facilitate new discussion about the management of anisometropia, which might benefit the control of high myopia.
Methods
Participants
Participants were included from the existing database – SCALE-HM into the current analysis.Citation25 Highly myopic patients (defined as at least one eye with spherical equivalent less than or equal to −5.00 D) aged 4–18 years were selected.Citation26 Participants with other organic eye diseases (amblyopia, strabismus, congenital cataract, glaucoma, etc.) were excluded.
The study protocol was explained to all participants. Oral assent was obtained from children under 12 years old, and written informed consent form was obtained from children aged 12 years old and over and the parents or legal guardians of all subjects. The study was performed under compliance with the principles from the Declaration of Helsinki. Ethics approval from the institutional review board of Shanghai General Hospital, Shanghai Jiao Tong University, was obtained.
Measurements and calculations
A series of general physical and ophthalmic examinations were performed on all participants by well-trained ophthalmologists, optometrists, coordinators and nurses.
Before cycloplegia, each participant underwent a slitlamp examination, and intra-ocular pressure (IOP) measurements were taken with a noncontact tonometer (NT-510, Nidek, Japan). Those with an anterior chamber depth below 2.5 mm or an IOP > 24 mmHg were excluded. The detailed procedure for cycloplegia was previously mentioned.Citation25 The refractive status (dioptre of sphere, dioptre of cylinder and corneal curvature radius) was measured using an autorefractor (KR-8900, Topcon, Japan) after cycloplegia. Three measurements were obtained for each eye, and the procedure was repeated if the difference between any two records was >0.50 D (dioptre of sphere and dioptre of cylinder). The spherical equivalent was calculated as spherical equivalent = dioptre of sphere + 0.50 × dioptre of cylinder. Axial length was measured by an IOL Master (Carl Zeiss Meditec, Germany). Each eye was measured three times, and if the difference between any two measurements was >0.05 mm, the measurement was repeated until the difference decreased below this value.
Anisometropia was classified into three subgroups; spherical equivalent anisometropia, cylindrical anisometropia and spherical anisometropia. They were calculated by the following formulas: spherical equivalent anisometropia = |spherical equivalent right eye – spherical equivalent left eye|; cylindrical anisometropia = |dioptre of cylinder right eye – dioptre of cylinder left eye| and spherical anisometropia = |dioptre of sphere right eye – dioptre of sphere left eye|. In addition, axial length anisometropia = |axial length right eye – axial length left eye| and corneal curvature radius anisometropia= |corneal curvature radius right eye – corneal curvature radius left eye|.
Statistics
SPSS (version 22.0; IBM Co., Armonk, NY, USA) was used for all data analyses. Data from both eyes were recorded, and their mean values were used for analysis. Data distribution was examined using the Kolmogorov–Smirnov test, and the parameters were presented as mean (standard deviation [SD]) and median (quartile) for continuous variables and counts (proportions) for categorical variables. Comparisons were performed using non-parametric tests (non-normally distributed data) or chi-square tests.
The following non-parametric tests were performed. The Mann–Whitney U-test was used for the comparison of groups with spherical equivalent anisometropia <1.0 and ≥1.0. Wilcoxon test was used for the comparison of more myopic eye and less myopic eye.
Correlations between refraction parameters were analysed using Spearman’s correlation coefficients. Multivariate regression analysis explored factors associated with anisometropia. The statistical significance was set to P < 0.05 (two-tailed).
Results
General characteristics
A total of 1,577 highly myopic children with a mean (SD) age of 13.06 (2.80) years and 49.5% of being male were included for analysis (). The mean (SD) spherical equivalent and axial length of eyes were −7.55 (1.87) D and 26.43 (1.06) mm, respectively. The median (quartile) of equivalent and axial length of eyes was −7.19 (−8.50, −6.25) D and 26.38 (25.71, 27.11) mm, respectively (). The mean (SD) spherical equivalent anisometropia, spherical anisometropia and cylindrical anisometropia values were 0.93 (1.03) D, 0.97 (1.04) D and 0.58 (0.51) D, respectively. The median (quartile) of spherical equivalent anisometropia, spherical anisometropia and cylindrical anisometropia values was 0.63 (0.25, 1.25) D, 0.75 (0.25, 1.25) D and 0.50 (0.25, 0.75) D, respectively.
Table 1. General characteristics and refraction parameters of participants with spherical equivalent anisometropia <1.00 D and ≥1.00D.
Comparison of <1.00 D and ≥1.00 D spherical equivalent anisometropia
Spherical equivalent anisometropia of 1.00 D or above had significantly older age, less astigmatism, higher amounts of myopia, larger interocular differences in spherical equivalent, axial length, astigmatism and corneal curvature radius, compared to spherical equivalent anisometropia <1.00 D (all P < 0.05; ).
Comparison of more myopic eye and less myopic eye
Significant interocular differences between spherical equivalent, dioptre of sphere, dioptre of cylinder, axial length and corneal curvature radius were observed between more myopic and less myopic eyes (all P < 0.01; ).
Table 2. Refraction parameters of more myopic eye and less myopic eye.
Proportions of anisometropia ≥1.00 D
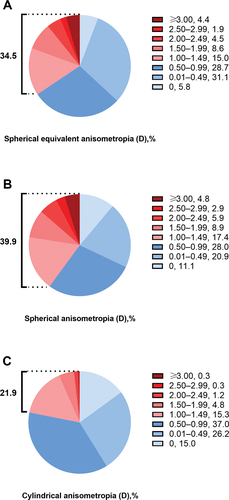
Upon further stratifying the anisometropia values into several levels, the proportions of spherical equivalent anisometropia, cylindrical anisometropia and spherical anisometropia ≥1.00 D were 34.5%, 39.9% and 21.9% ( and Supplementary Table S1), respectively.
Figure 1. The proportion of anisometropia in different degree groups. The proportions of A: spherical equivalent anisometropia, B: spherical anisometropia and C: cylindrical anisometropia in different degree groups are shown. Those with anisometropia (spherical equivalent anisometropia, spherical anisometropia and cylindrical anisometropia) ≥1.00 D are in red and those with anisometropia <1.00 D were in blue. The proportion of spherical equivalent anisometropia ≥1.00 D is 34.5%, spherical anisometropia ≥1.00 D is 39.9% and cylindrical anisometropia ≥1.00 D is 21.9%.
Distribution of anisometropia in different spherical equivalent, axial length, dioptre of sphere and dioptre of cylinder groups
The degree of anisometropia was also described according to different spherical equivalent, axial length, dioptre of sphere and dioptre of cylinder groups in and Supplementary Table S1. The dioptre of cylinder was conversely associated with increasing spherical equivalent anisometropia (P for trend <0.001, ). No significant increasing trends of spherical equivalent anisometropia with decrease in spherical equivalent and dioptre of sphere or increase in axial length were observed ().
Figure 2. Degree and proportion of anisometropia in different spherical equivalent, axial length, dioptre of sphere and dioptre of cylinder groups.
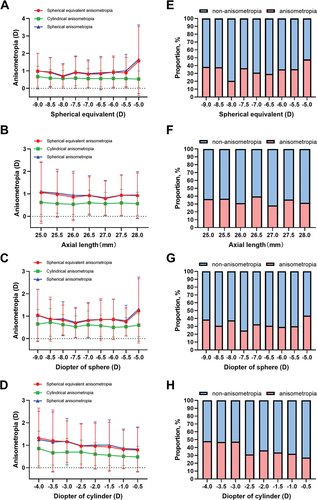
The proportions of anisometropia (spherical equivalent anisometropia ≥1.00 D) for their respective spherical equivalent, axial length, dioptre of sphere and dioptre of cylinder groups are described in and Supplementary Table S2. The dioptre of cylinder was conversely associated with increasing anisometropia (, P for trend <0.001), and no significant trends were observed in spherical equivalent, axial length or dioptre of sphere groups (, P for trend = 0.409, 0.276 and 0.150, respectively).
Correlated factors of anisometropia
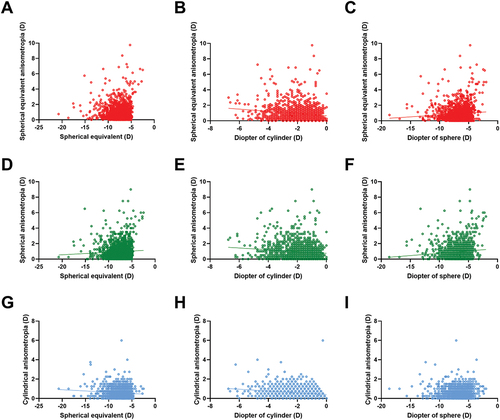
The correlation analysis showed that spherical equivalent anisometropia, spherical anisometropia and cylindrical anisometropia were weakly negatively correlated with dioptre of cylinder (correlation coefficient = −0.148, −0.119 and −0.194, respectively, all P < 0.01). Spherical equivalent anisometropia and spherical anisometropia were weakly positively correlated with dioptre of sphere and spherical equivalent (correlation coefficient = 0.106, 0.056; 0.124, 0.081, respectively, all P < 0.05). Cylindrical anisometropia was weakly negatively correlated with spherical equivalent (correlation coefficient = −0.096, P < 0.01) (). The distribution and univariate linear regression of anisometropia with spherical equivalent, dioptre of cylinder and dioptre of sphere are shown in . Spherical equivalent anisometropia was linearly correlated with dioptre of cylinder (y = −0.142 × x + 0.654, P < 0.001) and dioptre of sphere (y = 0.049 × x + 1.246, P < 0.001).
Figure 3. Correlation analysis of anisometropia and the refraction parameters. The correlation analysis of anisometropia (spherical equivalent anisometropia, spherical anisometropia and cylindrical anisometropia) and the refraction parameters (spherical equivalent, dioptre of sphere and dioptre of cylinder) is shown. Correlation coefficients are in figure. Positive correlation is in red and negative correlation is in blue. * P < 0.05, ** P < 0.01.
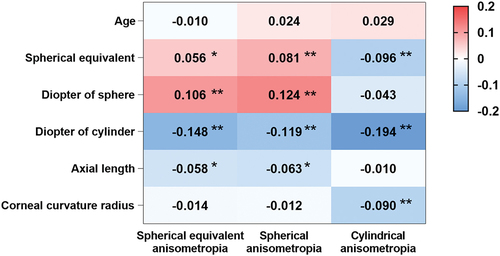
Figure 4. The distribution and univariate linear regression of anisometropia with spherical equivalent, dioptre of cylinder and dioptre of sphere. Univariate linear regression: A~C: the distribution of spherical equivalent anisometropia with spherical equivalent (P = 0.179), dioptre of cylinder (y = −0.142 × x + 0.654, P < 0.001) and dioptre of sphere (y = 0.049 × x + 1.246, P < 0.001). D~F: The distribution of spherical anisometropia with spherical equivalent (y = 0.032 × x + 1.204, P = 0.017), dioptre of cylinder (y = −0.115 × x + 0.742, P < 0.001) and dioptre of sphere (y = 0.060 × x + 1.358, P < 0.001). G~I: the distribution of cylindrical anisometropia with spherical equivalent (y = −0.026 × X + 0.384, P < 0.001), dioptre of cylinder (y = −0.091 × x + 0.409, P < 0.001) and dioptre of sphere (P = 0.095).
In the multivariable regression analysis (), spherical equivalent anisometropia was negatively associated with dioptre of cylinder (standard beta = −0.175) (R2 = 0.038). Spherical anisometropia was negatively associated with dioptre of cylinder (standard beta = −0.148), and positively associated with age (standard beta = 0.072) and dioptre of sphere (standard beta = 0.116) (R2 = 0.037, P < 0.001). Cylindrical anisometropia was negatively associated with dioptre of cylinder (standard beta = −0.191) (R2 = 0.043, P < 0.001).
Table 3. Multivariate regression of anisometropia.
Discussion
The current study covered 1,577 patients with high myopia to investigate the distribution of anisometropia and identified potential risk factors for the presence of anisometropia. A major finding of this study was the high proportion of anisometropia in high myopia, which was prevalent in 34.5% of the sample size. For high myopes, spherical equivalent anisometropia significantly increased with the severity of astigmatism, but not with myopia severity. More spherical equivalent anisometropia was associated with higher degrees of astigmatism, longer axial length and better spherical power. Considering this is the first large-scale study investigating anisometropia in high myopes, these findings may have significant implications and warrant further discussion in the context of the current literature.
The current study reported that anisometropia was present in 34.5% of children with high myopia, which was much higher than that observed by previous studies. Hu et al. observed in proportion of 7% in 6,025 schoolchildren aged 4–18 years with spherical equivalent anisometropia ≥1.0 D,Citation27 and compared with non-myopic children, Tong et al. found that myopes exhibited an anisometropia proportion of 2.4% when spherical equivalent anisometropia ≥2.00 D.Citation6 A retrospective study of 146 longitudinal myopic case histories found a 14.4% proportion of unilateral myopic anisometropia in myopic children aged <19 years.Citation14 Although the proportion reported by Pointer and Gilmartin most aligns with the present findings, this figure is likely an underestimation due to its smaller sample size in comparison with the current study. The study of Pointer and Gilmartin reported the prevalence of anisometropia among myopes, which was defined as spherical equivalent ≤−0.50 D, while the current study investigated the prevalence of anisometropia among highly myopic children with the definition of spherical equivalent ≤−5.00 D. The discrepancy of these study populations might explain the difference in the prevalence of anisometropia found.
The present findings suggested that children with high myopia were much more likely to have anisometropia. To some degree, this reinforces the hypothesis that both myopia and anisometropia represent failures of posterior chamber development, and excessive eye growth might drive anisometropia.Citation1,Citation20,Citation28 An interaction of myopia and anisometropia has been reported whereby anisometropia leads to concomitant unilateral myopia progression,Citation1,Citation18,Citation19 and progression of myopia might promote anisometropia in children.Citation6,Citation20 Previous studies have observed risk factors for myopia such as time spent indoors and paternal education levels, which were significantly correlated with anisometropia.Citation27 Orthokeratology lenses for unilateral high myopia treatments improved high anisometropia.Citation29,Citation30 Taken together, the pathogenesis of each condition is likely related or affected by the other. Considering these findings, children with high myopia should be also monitored for the development of anisometropia.
Although the presence of anisometropia and myopia was surprisingly high, the present findings suggest that anisometropia is not related to spherical development for high myopes, considering dioptre of sphere did not correlate with anisometropia nor anisometropia with spherical equivalent, dioptre of sphere or axial length. Moreover, the prevalence and degree of spherical equivalent anisometropia reduced with higher degree of spherical equivalent and dioptre of sphere. These findings are surprising and inconsistent with many previous studies observing trends between anisometropia and myopia progression,Citation27 although they are consistent with a retrospective study of longitudinal case histories that found myopia progression was unrelated to anisometropia progression.Citation14 This may be because, in high myopes, the progression of myopia in the eye with lower spherical equivalent gradually slowed, while that the other eye still progressed relatively rapidly. On the other hand, although anisometropia is also be thought to be driven by stochastic factors. The effect on refraction growth may not be as pronounced in highly myopic children such that genetic and environmental factors to play more critical roles.Citation18
Unlike myopia, the present study found that astigmatism might be related to anisometropia severity in highly myopic children. When subjects were grouped according to dioptre of cylinder, those with higher astigmatism, but not a higher degree of myopia, tended to have more severe anisometropia, with a statistically significant difference and trend. Additionally, there was a significant difference in dioptre of cylinder between subjects with spherical equivalent anisometropia ≥1.00 D and <1.00 D. This contrasts with Pärssinen et al., who found that baseline astigmatism did not relate to magnitude of anisometropia in 238 myopic children.Citation19 Although it may not account for all differences, the inclusion of only highly myopic children may suggest that anisometropia is associated with astigmatism in the later stages of myopic development and may signal a late phase of disease course that is unrelated to axial length.
Astigmatism is driven by anterior chamber changes, while myopia is predominated by posterior chamber lengthening.Citation31 Perhaps, an ocular homoeostatic mechanism in high anisomyopia is to shift changes happening in the posterior chamber to the anterior segment such that the posterior segment is spared from further degeneration. To confirm this hypothesis, long-term follow-up studies should follow worsening myopes and establish whether there are cut-off axial lengths which herald the worsening of astigmatism in anisometropia development.
The present study described anisometropia in a large sample of highly myopic children. In high myopes, astigmatism tends to be related to anisometropia rather than myopia. While this study provides new insights to the pathogenesis and potential course of high anisometropia, some limitations must be acknowledged. Considering the population was only composed of high myopes, the results may not be applicable to children with refractive status more than −5.00 D. Future studies will need to enrol children of all ranges of myopia and stratify myopia by severity in large population studies to identify the prevalence in each subgroup.
This was a cross-sectional study, and the development of anisometropia and high myopia was difficult to assess without temporal data. As causal relationships cannot be distinguished in by the current study design, future studies are required to reveal any casual relationships between myopia and anisometropia. The large sample size might lead to some statistically significant but not clinically significant results, such as the difference of corneal curvature radius anisometropia between those with spherical equivalent anisometropia <1.00 D and ≥1.00 D (), dioptre of cylinder and corneal curvature radius between those with more myopic eye and less myopic eye (). Thus, the present results should be assessed in combination with the value of the parameters.
The correlation coefficients were low, which indicates minimal association between the variables. Moreover, these findings could provide better insight for astigmatism and myopia with anisometropia if they had incorporated questionnaire-specific findings such as ocular trauma, family history and time spent outdoors.Citation18,Citation32 This cohort was of Chinese ethnicity, and considering the geographic distribution in Western countries is strikingly different to Asian populations, these findings may not be generalisable to them.
Conclusion
The current study found a higher proportion of anisometropia in highly myopic children compared with previously reported studies of the general population. More severe anisometropia was associated with a higher degree of cylindrical power, but not spherical power. This may symbolise later phases of anisometropic myopia where the anterior segment attempts to compensate for the damaging effects of continued axial length elongation. Considering the high incidence of anisometropia with myopia, anisometropia should be addressed when managing high myopia.
Supplementary table 1
Download MS Word (19.8 KB)Supplementary table 2
Download MS Word (16.8 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/08164622.2023.2198635.
Additional information
Funding
References
- Barrett BT, Bradley A, Candy TR. The relationship between anisometropia and amblyopia. Prog Retin Eye Res 2013; 36: 120–158. doi:10.1016/j.preteyeres.2013.05.001
- Lovasik JV, Szymkiw M. Effects of aniseikonia, anisometropia, accommodation, retinal illuminance, and pupil size on stereopsis. Invest Ophthalmol Vis Sci 1985; 26: 741–750.
- Group M-ePEDS. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology 2008; 115: 1229–1236. e1221. doi:10.1016/j.ophtha.2007.08.001
- Vincent SJ, Collins MJ, Read SA et al. Myopic anisometropia: ocular characteristics and aetiological considerations. Clin Exp Optom 2014; 97: 291–307. doi:10.1111/cxo.12171
- Cass K, Tromans C. A biometric investigation of ocular components in amblyopia. Ophthalmic Physiol Opt 2008; 28: 429–440. doi:10.1111/j.1475-1313.2008.00585.x
- Tong L, Saw SM, Chia KS et al. Anisometropia in Singapore school children. Am J Ophthalmol 2004; 137: 474–479. doi:10.1016/j.ajo.2003.10.028
- O’Donoghue L, McClelland JF, Logan NS et al. Profile of anisometropia and aniso-astigmatism in children: prevalence and association with age, ocular biometric measures, and refractive status. Invest Ophthalmol Visual Sci 2013; 54: 602–608. doi:10.1167/iovs.12-11066
- Dobson V, Miller JM, Clifford-Donaldson CE et al. Associations between anisometropia, amblyopia, and reduced stereoacuity in a school-aged population with a high prevalence of astigmatism. Invest Ophthalmol Visual Sci 2008; 49: 4427–4436. doi:10.1167/iovs.08-1985
- Qin XJ, Margrain TH, To CH et al. Anisometropia is independently associated with both spherical and cylindrical ametropia. Invest Ophthalmol Visual Sci 2005; 46: 4024–4031. doi:10.1167/iovs.05-0120
- Dirani M, Chan YH, Gazzard G et al. Prevalence of refractive error in Singaporean Chinese children: the strabismus, amblyopia, and refractive error in young Singaporean Children (STARS) study. Invest Ophthalmol Vis Sci 2010; 51: 1348–1355. doi:10.1167/iovs.09-3587
- Afsari S, Rose KA, Gole GA et al. Prevalence of anisometropia and its association with refractive error and amblyopia in preschool children. Br J Ophthalmol 2013; 97: 1095–1099. doi:10.1136/bjophthalmol-2012-302637
- Borchert M, Tarczy-Hornoch K, Cotter SA et al. Anisometropia in Hispanic and African American infants and young children the multi-ethnic pediatric eye disease study. Ophthalmology 2010; 117: 148–153. e141. doi:10.1016/j.ophtha.2009.06.008
- Tong L, Chan YH, Gazzard G et al. Longitudinal study of anisometropia in Singaporean school children. Invest Ophthalmol Vis Sci 2006; 47: 3247–3252. doi:10.1167/iovs.05-0906
- Pointer JS, Gilmartin B. Clinical characteristics of unilateral myopic anisometropia in a juvenile optometric practice population. Ophthalmic Physiol Opt 2004; 24: 458–463. doi:10.1111/j.1475-1313.2004.00226.x
- Huynh SC, Wang XY, Ip J et al. Prevalence and associations of anisometropia and aniso-astigmatism in a population based sample of 6 year old children. Br J Ophthalmol 2006; 90: 597–601. doi:10.1136/bjo.2005.083154
- Brooks SE, Johnson D, Fischer N. Anisometropia and binocularity. Ophthalmology 1996; 103: 1139–1143. doi:10.1016/S0161-6420(96)30555-1
- Smith EL 3rd, Hung LF, Arumugam B et al. Observations on the relationship between anisometropia, amblyopia and strabismus. Vision Res 2017; 134: 26–42. doi:10.1016/j.visres.2017.03.004
- Flitcroft I, McCullough S, Saunders K. What can anisometropia tell us about eye growth? Br J Ophthalmol 2021; 105: 1211–1215. doi:10.1136/bjophthalmol-2020-316406
- Pärssinen O. Anisometropia and changes in anisometropia in school myopia. Optom Vis Sci 1990; 67: 256–259. doi:10.1097/00006324-199004000-00005
- Deng L, Gwiazda JE. Anisometropia in children from infancy to 15 years. Invest Ophthalmol Vis Sci 2012; 53: 3782–3787. doi:10.1167/iovs.11-8727
- Xu S, Xu A, Tao A et al. Corneal biomechanical properties and intraocular pressure in high myopic anisometropia. Eye Contact Lens 2010; 36: 204–209. doi:10.1097/ICL.0b013e3181e4a60a
- Valente P, Buzzonetti L, Dickmann A et al. Refractive surgery in patients with high myopic anisometropia. J Refract Surg 2006; 22: 461–466. doi:10.3928/1081-597X-20060501-07
- Ali A, Packwood E, Lueder G et al. Unilateral lens extraction for high anisometropic myopia in children and adolescents. J Aapos 2007; 11: 153–158. doi:10.1016/j.jaapos.2006.09.004
- Kraus CL, Trivedi RH, Wilson ME. Intraocular lens exchange for high myopia in pseudophakic children. Eye (Lond) 2016; 30: 1199–1203. doi:10.1038/eye.2016.152
- He X, Deng J, Xu X et al. Design and pilot data of the high myopia registration study: Shanghai Child and Adolescent Large-scale Eye Study (SCALE-HM). Acta Ophthalmol 2021; 99: e489–500. doi:10.1111/aos.14617
- Myopia JWHO-BHVIGSMo, Mariotti SP, Kocur I et al. The impact of myopia and high myopia. Report of the Joint World Health Organization-Brien Holden Vision Institute Global Scientific Meeting on Myopia; 2015.
- Hu YY, Wu JF, Lu TL et al. Prevalence and associations of anisometropia in children. Invest Ophthalmol Vis Sci 2016; 57: 979–988. doi:10.1167/iovs.15-18647
- Flitcroft DI. Is myopia a failure of homeostasis? Exp Eye Res 2013; 114: 16–24. doi:10.1016/j.exer.2013.02.008
- Tsai WS, Wang JH, Lee YC et al. Assessing the change of anisometropia in unilateral myopic children receiving monocular orthokeratology treatment. J Formos Med Assoc 2019; 118: 1122–1128. doi:10.1016/j.jfma.2019.02.001
- Fu AC, Qin J, Rong JB et al. Effects of orthokeratology lens on axial length elongation in unilateral myopia and bilateral myopia with anisometropia children. Cont Lens Anterior Eye 2020; 43: 73–77. doi:10.1016/j.clae.2019.12.001
- Read SA, Collins MJ, Carney LG. A review of astigmatism and its possible genesis. Clin Exp Optom 2007; 90: 5–19. doi:10.1111/j.1444-0938.2007.00112.x
- Lingham G, Mackey DA, Sanfilippo PG et al. Influence of prenatal environment and birth parameters on amblyopia, strabismus, and anisometropia. J Aapos 2020; 24: 74.e71–74.e77. doi:10.1016/j.jaapos.2019.12.013