
Abstract
Background
Chronic kidney disease (CKD) poses a significant public health challenge globally while impacting patients’ physical function and quality of life. Addressing the issues of physical inactivity and pain management is essential during treatment to improve health-related quality of life. The present study investigated the effect of an aerobic training program with core stabilization exercises for hemodialysis (HD) patients on a transplant waiting list and renal transplant (RTx) patients.
Methods
A total of 45 patients with CKD were included in the 12-week study: 25 patients receiving HD (12 HD treatment group, 13 HD control group) and 20 patients with RTx (9 RTx treatment group, 11 RTx control group). Functional capacity was measured using the 6-min walk test, pain was measured using the visual analog scale, and health-related quality of life was measured using the Kidney Disease Quality of Life–Short Form 12 questionnaire. Nonparametric statistical tests were performed at a significance level of 0.05.
Results
Both the HD and RTx treatment groups showed significantly reduced times for the 6-min walking test (p = 0.002 and p = 0.008, respectively), significantly reduced pain severity (p = 0.002 and p = 0.008, respectively), and significantly improved quality of life scores (p = 0.006 and p = 0.041, respectively) by the end of the study compared with control groups.
Conclusion
Based on the results, structured exercise programs could be effective therapies in CKD management. Therefore, health providers should promote their integration into routine care practices to enhance patient outcomes and well-being.
1. Introduction
Chronic kidney disease (CKD) is a major public health problem worldwide, with a significant impact on patients’ physical function and quality of life. Health providers have placed increasing emphasis on patient-centered, symptom-oriented management of the disease, aimed at alleviating patient suffering, improving quality of life, and supporting patients in coping with kidney disease [Citation1,Citation2]. All stages of the disease are characterized by the development of cardiovascular disease, musculoskeletal and muscle pain, and loss of muscle strength, leading to a decline in quality of life [Citation3]. Physical inactivity is already present in the early stages and increases as the disease progresses [Citation4,Citation5]. The most common causes of physical inactivity are fatigue and pain [Citation6,Citation7]. Studies have shown that therapy interventions combining both aerobic and resistance exercises are the most effective in reducing the development of complications in this patient population [Citation8–10]. According to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, all CKD patients should engage in at least 150 min of physical activity per week, with the form and intensity of exercise being individualized [Citation11].
The most effective treatment for CKD is renal transplantation (RTx) [Citation12]. However, the waiting time for nonliving donor transplantation is unpredictable. Accordingly, it is crucial to maintain or, if possible, increase the physical activity and functional capacity of patients on the transplant waiting list who are on a chronic dialysis program. Prehabilitation interventions planned during this time can improve patients’ physical fitness and cooperation, reduce the burden of kidney disease, reduce postrenal transplant frailty, and support postoperative recovery [Citation13]. Studies suggest that HD and RTx patients have lower physical functioning and physical activity compared with the nonrenal population and that, although the prevalence of pain is the same in chronic hemodialysis (HD) and RTx patients, HD patients experience a higher intensity of pain [Citation6,Citation14,Citation15].
Core stabilization exercises are designed to ensure functional stability of the spine. Strengthening the core muscles is recommended for the prevention and rehabilitation of various lumbar spinal and musculoskeletal disorders as well as for the treatment of pain [Citation16–18]. However, although stabilization exercises have been effective in reducing musculoskeletal pain in several patient groups, they have not been studied in a CKD patient group. Thus, this study aimed to evaluate and compare the effects of a core stabilization exercise program combined with aerobic training in HD patients on the waiting list for RTx and RTx patients.
2. Materials and methods
2.1. Participants
A total of 45 patients with CKD participated in our study: 25 patients receiving HD (12 HD treatment group, 13 HD control group) and 20 patients with RTx (9 RTx treatment group, 11 RTx control group). The participants in the treatment groups completed a 12-week training program, three times a week for 60 min each. HD patients exercised on non-dialysis days. Participants were divided into groups of four or five by dialysis day, fitness level, and age. Members of the treatment groups reported not engaging in any regular physical activity before the study. The control group members carried out their normal daily activities and completed questionnaires and functional assessments. Inclusion criteria for all participants were age over 18 years, ability to walk, and willingness to participate in the study. Additional inclusion criteria for the HD group were at least 3 months of maintenance HD with regular HD at least three times per week for ≥4 h per treatment, on-line Kt/V of at least 1.4 (dialysis machine Fresenius 5008), and on the kidney transplant waiting list. Additional criteria for the RTx group were physically fit and on stable medication for more than 6 months after kidney transplantation. Exclusion criteria for all participants were diabetes mellitus, anemia (hemoglobin less than 100 g/l), any contraindication to physical exertion, such as limited mobility of large joints, decompensated heart failure, untreated hypertension, major neurological dysfunction, severe peripheral polyneuropathy, or combined organ transplantation. In the first part of the study, all participants received a leaflet with details of the study and ethical information. Voluntary, informed consent was provided by all participants before data collection. Members of the exercise training group agreed to participate regularly in the exercise programs, whereas members of the control group were only required to complete the questionnaire and functional assessment. The Regional and Institutional Research Ethics Committee of the University of Debrecen Clinical Center approved the research protocol. Protocol ID: DE RKEB/IKEB: 5551 A-2020.
2.2. Data collection
Data collection was performed at the Department of Nephrology Dialysis Center, University of Debrecen, between May and November 2020. Demographic data, information on treatment, and comorbidities were recorded using a questionnaire prepared by our team. Functional capacity was measured using the 6-min walk test (6MWT) and pain intensity was measured using the visual analog scale (VAS) [Citation19,Citation20]. The Kidney Disease Quality of Life–Short Form 12 questionnaire (KDQOL–SF-12) was used to measure quality of life [Citation21]. The tests described were carried out before and after the 12 weeks of treatment.
2.3. Intervention
The exercise program included a moderate-intensity endurance workout on an indoor bike followed by a core stabilization workout. Each training session started with a 10-min warm-up on indoor bikes at the lowest resistance level. After the warm-up, participants performed moderate-intensity physical activity not exceeding 50%–60% of the heart rate range. In the second and third training sessions, they were able to reach and maintain the set training heart rate. During the first 2 weeks, the duration of the workout was gradually increased from 15 min to 30 min to achieve a continuous, steady intensity of training. The core stabilization training involved targeted strengthening of the core muscles responsible for the stability of the spine. The training consisted of two phases. In the first phase (1 to 6 weeks), we taught activation and awareness of the core muscles. Following the principle of gradualness, exercises were first performed in a supine position, followed by a side-lying position, quadrupedal position, static standing position, and finally in movement. Then, exercises were performed on an unstable surface (i.e., fit-ball ball, sponge cushion, or BOSU trainer). In the second phase (7 to 12 weeks), functional strengthening exercises were performed in the form of circuit training in three sets of 15–20 repetitions. The training program was concluded with dynamic stretching, with particular attention on the heavily used muscle groups [Citation22].
2.4. Statistical analysis
Data were analyzed using Mann-Whitney U tests and Wilcoxon signed-rank tests to determine the differences between the variables since most of the data did not follow a normal distribution, as determined by the Shapiro-Wilk test. The results are presented with median values and interquartile ranges with their corresponding p-values. Statistical analysis was performed using Stata statistical software (version 13.0, Stata Corp., College Station, TX, USA), and a p-value less than 0.05 was taken to indicate statistical significance.
3. Results
The HD treatment group consisted of six men and six women with a median age of 49 years (46–55) and a mean time on HD of 43 months (30–55). The HD control group consisted of eight men and five women with an average age of 52 years (47–58) and 39 months (26–51) on HD. The RTx treatment group consisted of four men and five women with an average age of 49 years (45–59) and 84 months (72–104) since transplantation. The RTx control group consisted of five men and six women with an average age of 50 years (47–58) and 81 months (72–98) since transplantation.
3.1. 6-min walk test
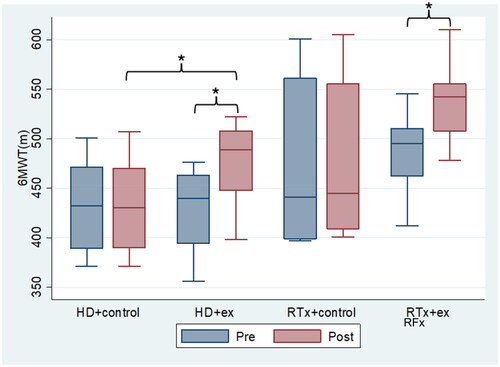
For the 6MWT, the median value for the 12-person HD treatment group increased significantly from 440 (395–463) before the training to 489 (448–508) after the training (p = 0.002). For the 13-person HD control group, the median value increased from 432 (389–471) to 430 (390–470) following training, but this association was nonsignificant (p = 0.461). The median value for the nine-person RTx treatment group significantly increased from 495 (462–510) to 542 (508–555) (p = 0.008). No significant increase was found for the median value for the 11-person RTx control group: 441 (399–561) to 445 (409–555) (p = 0.118). Further, no significant differences were found in the baseline values between patients in the treatment and control groups within the HD group (p = 0.849) or the RTx group (p = 0.621). After the 12-week training program, the median value of the patients in the HD treatment group was significantly higher compared to its control group (p = 0.030). No significant difference was found between the median values among patients in the RTx group (p = 0.081). The median change measured at the individual level was 46 (43–51) in the HD treatment group and 2 (-3–5) in the control group, with a significant difference between the two groups (p < 0.001). The median increase measured at the individual level for the RTx treatment group was 55 (47–66) compared to 3 (-2–9) for the control group, and this change was significant (p < 0.001). When comparing the delta of the exercisers in the HD group with the delta of the exercisers in the RTx group, the median value was significantly lower in the HD group (p = 0.023). Significant differences were also observed regarding the initial and the post-training median values when HD and RTx groups with no stratification were compared (p = 0.010 and p = 0.011, respectively). However, the median increase between the groups was not significantly different (p = 0.367) ().
Figure 1. Figure Box plot regarding 6 min walking test. 6 MWT (m): 6-min walk test (meter); HD: hemodialysis; HD+ex: hemodialysis exercise group; HD+control: hemodialysis control group; RTx: renal transplant, RTx+ex: renal transplant exercise group; RTx+control: renal transplant control group. Significant findings are marked with ‘*’.
3.2. Pain
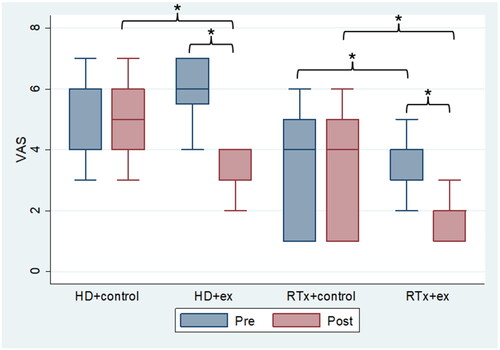
For pain, the initial median score in the HD group was 6 (5.5–7) in the 12-person training group, which significantly reduced to 3 (3–4) by the end of the study (p = 0.002). In the 13-patient HD control group, the median scores were 6 (4–6) initially and 5 (4–6) at the end of the study period; however, this change was nonsignificant (p = 0.083). In the RTx group, the initial median score for the nine patients who completed the training was 4 (3–4), which significantly reduced to 2 (1–2) at the end of the program (p = 0.008). The median scores for the 11 participants in the RTx control group for the two timepoints remained unchanged at 4 (1–5), a non-significant change (p = 0.157). No significant difference was found regarding self-assessed pain at baseline between patients in the treatment and control groups for either the HD group or the RTx group (p = 0.084 and p = 0.621, respectively). After the 12-week training program, patients in the HD treatment group showed significant improvement compared to the HD control group (p = 0.001). We also found a significant improvement in patients in the RTx treatment group compared to the RTx control group (p = 0.003). The median change at the individual level was −3 (-3.5–-2) in the HD treatment group and 0 (0–0) in the control group, indicating a significant difference between the two groups (p < 0.001). The median change at the individual level was −2 (-2–-1) in the RTx treatment group and 0 (0–0) in the control group, indicating a significant difference between the two groups (p = 0.008). Comparing the delta of exercisers in the HD group and the delta of exercisers in the RTx group showed no significant difference between the two groups (p = 0.051). However, a significant difference was observed for the initial and post-training median values when comparing the HD and RTx groups without stratification (p = 0.001 and p = 0.003, respectively). However, the median increase between groups was not significantly different (p = 0.215) ().
Figure 2. Figure Box plot regarding visual analog scale. HD: hemodialysis; HD+ex: hemodialysis exercise group; HD+control: hemodialysis control group; RTx: renal transplant; RTx+ex: renal transplant exercise group; RTx+control: renal transplant control group. Significant findings are marked with ‘*’.
3.3. Quality of life
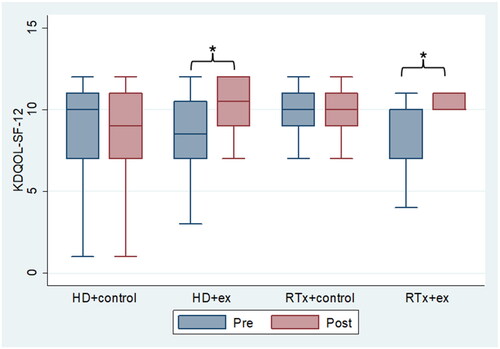
For quality of life, the initial median score in the HD treatment group of 12 was 8.5 (7–10.5), which increased significantly to 10.5 (9–12) by the end of the study (p = 0.006). In the HD control group of 13 patients, the initial median score was 10 (7–11), which reduced to 9 (7-11) at the end of the study period, although this change was nonsignificant (p = 0.317). In the RTx group, the initial median score for the nine patients in the treatment group was 10 (7–10), which changed to 10 (10–11) at the end of the program, indicating a significant increase (p = 0.041). The median scores for the 11 participants in the RTx control group remained unchanged at 10 (9–11). No significant difference in baseline quality of life scores was found between patients in the treatment vs control groups in either the HD group (p = 0.721) or RTx group (p = 0.150). After the 12-week training program, no significant difference was found between the median scores of patients in the HD treatment vs control group (p = 0.121) or between the median scores of patients in the RTx treatment vs control group (p = 0.809). The median change at the individual level was 1.5 (0–3.5) in the HD treatment group and 0 (0–0) in the control group, indicating a significant difference between the two groups (p < 0.001). The median change at the individual level was 1 (0–3) in the RTx treatment group and 0 (0–0) in the control group, also indicating a significant difference between the two groups (p = 0.014). Comparing the delta of those who trained in the HD group with the delta of those who trained in the RTx group, no significant difference was found between the two groups (p = 0.913). In terms of quality of life, no significant difference was found between the initial and post-training median scores when comparing the HD and RTx groups without stratification (p = 0.319 and p = 0.272, respectively). The median increase between groups was also not significant (p = 0.883) ().
Figure 3. Figure Box plot regarding kidney disease quality of life -short form 12 questionnaire. HD: hemodialysis; HD+ex: hemodialysis exercise group; HD+control: hemodialysis control group; RTx: renal transplant; RTx+ex: renal transplant exercise group; RTx+control: renal transplant control group. Significant findings are marked with ‘*’.
4. Discussion
Increasing physical activity is a priority area for lifestyle change for people with CKD, as a growing number of studies have demonstrated the benefits of exercise programs in reducing cardiovascular risk factors and pain and improving the quality of life in this patient group [Citation23]. In our study, we investigated the effect of a combined aerobic and core stabilization exercise program in Hungarian HD and RTx patients. Our main outcomes in both groups of patients were improvement in functional capacity, reduction in pain, and improvement in quality of life measured at the individual level. We measured functional capacity using the 6MWT in line with Kohl et al. who found the test has prognostic value in the lifespan of CKD patients [Citation24]. Their results showed that for every 100 m increase in walking distance measured with the 6MWT, the risk of death is reduced by 5%. In our study, walking distance measured with the 6MWT increased significantly in the HD exercise group but decreased slightly in the HD control group. In RTx patients, walking distance increased significantly in the exercise group but did not change significantly in the control group. When comparing the 6MWT scores of the HD and RTx groups, the RTx group demonstrated better functional status at the first assessment. Concerning the mean (delta) scores, a significant difference was not found, indicating similar improvement among patients in the HD and RTx groups. In other words, the program was useful for improving physical functioning at both stages of the disease. People with CKD often cite pain as a limiting factor for physical activity. In addition to pharmacological options, nonpharmacological options are also used to manage pain. Although few studies have investigated the effectiveness of exercise programs in relieving pain in CKD patients, their data have shown positive results [Citation14,Citation25]. In our study, we found a significant reduction in pain severity in both the HD exercise and RTx exercise groups, whereas no change was in the control groups, suggesting that our exercise program is effective in both patient groups. Looking at the overall sample, members of the HD group reported higher baseline pain levels compared to the RTx group. Quality of life is another important indicator of the effectiveness and quality of CKD treatments. Studies have shown that the health-related quality of life of CKD patients is significantly reduced regardless of the stage of CKD [Citation4,Citation26]. In our study, quality of life was significantly improved in the HD treatment group. In contrast, scores were slightly reduced in the HD control group; however, this was not statistically significant. The same trend was seen in the RTx group, as the median remained the same in the treatment group but the change in interquartile ranges (in 50% of the sample) was more favorable (7–10 at baseline vs 10–11 after intervention), while no change was seen in the control group. The effectiveness of the exercise program is indicated by the fact that the median change in quality of life was significant in both the HD and RTx treatment and control groups, suggesting the program was equally effective and efficient in both groups.
5. Conclusion
Our study focused on HD and RTx patients. The combination of a core stabilization exercise program with aerobic training, which has not been studied in this patient group, revealed promising results in terms of functional capacity, pain management, and improvement in quality of life. Functional capacity, assessed by the 6MWT, was found to be a key indicator of improvement in both patient groups. This improvement highlights the importance of structured exercise programs in increasing mobility and reducing cardiovascular risk factors in CKD patients. Chronic pain, which may prevent CKD patients from increasing their physical activity, was significantly reduced following participation in an exercise program. This result confirms that exercise as a nonpharmacological therapy is a good tool to alleviate pain and improve the overall well-being of CKD patients. Furthermore, our study highlights the positive impact of exercise on the quality of life of CKD patients and the holistic benefits of exercise beyond physical fitness to psychological and emotional well-being.
Our results support the incorporation of personalized exercise programs highlighting the significant benefits of combined aerobic and core stabilization exercises.
6. Study limitations
The vast majority of the parameters analyzed were based on self-reporting, therefore a possible limitation of this study is the reliance on self-reported measures for pain assessment and health-related quality of life, which may introduce subjectivity and recall bias.
Authors’ contributions
Conceptualization, methodology, study design: EK, IK, ZJ, JB; Analysis and interpretation of data: EK, GJS; Drafting of the manuscript: EK, GJS; Critical revision of the manuscript for important intellectual content: EK, IK, ZJ, JB; Statistical expertise: GJS; Study supervision: IK; GJS. All authors have read and approved the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Brück K, Stel VS, Gambaro G, et al. CKD prevalence varies across the European general population. J Am Soc Nephrol. 2016;27(7):1–7. doi:10.1681/ASN.2015050542.
- Kalantar-Zadeh K, Lockwood MB, Rhee CM, et al. Patient-centred approaches for the management of unpleasant symptoms in kidney disease. Nat Rev Nephrol. 2022;18(3):185–198. doi:10.1038/s41581-021-00518-z.
- Luyckx VA, Cherney DZI, Bello AK. Preventing CKD in developed countries. Kidney Int Rep. 2020;5(3):263–277.
- Filipčič T, Bogataj Š, Pajek J, et al. Physical activity and quality of life in hemodialysis patients and healthy controls: a cross-sectional study. Int J Environ Res Public Health. 2021;18(4):1–10. doi:10.3390/ijerph18041978.
- Barcellos FC, Santos IS, Umpierre D, et al. Effects of exercise in the whole spectrum of chronic kidney disease: a systematic review. Clin Kidney J. 2015;8(6):753–765. doi:10.1093/ckj/sfv099.
- dos Santos PR, Mendonça CR, Noll M, et al. Pain in hemodialysis patients: prevalence, intensity, location, and functional interference in daily activities. Healthcare. 2021;9(10):1375. Oct 14doi:10.3390/healthcare9101375.
- Molina M, Sorolla C, Samsó E, et al. Quality of life in long-term renal transplant patients: a controversial subject. Transplant Proc. 2022;54(1):91–93. doi:10.1016/j.transproceed.2021.11.025.
- Segura-Ortí E, Kouidi E, Lisón JF. Effect of resistance exercise during hemodialysis on physical function and quality of life: randomized controlled trial. Clin Nephrol. 2009;71(5):527–537. doi:10.5414/cnp71527.
- Kouidi E, Karagiannis V, Grekas D, et al. Depression, heart rate variability, and exercise training in dialysis patients. Eur J Cardiovasc Prev Rehabil. 2010;17(2):160–167. doi:10.1097/HJR.0b013e32833188c4.
- Scapini KB, Bohlke M, Moraes OA, et al. Combined training is the most effective training modality to improve aerobic capacity and blood pressure control in people requiring haemodialysis for end-stage renal disease: systematic review and network meta-analysis. J Physiother. 2018;65(1):4–15. http://www.ncbi.nlm.nih.gov/pubmed/30581137
- Rovin BH, Adler SG, Barratt J, et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021;100(4):753–779. doi:10.1016/j.kint.2021.05.015.
- Johansen KL, Painter P. Exercise in individuals with CKD. Am J Kidney Dis. 2012;59(1):126–134. doi:10.1053/j.ajkd.2011.10.008.
- McAdams-DeMarco MA, Ying H, Van Pilsum Rasmussen S, et al. Prehabilitation prior to kidney transplantation: results from a pilot study. Clin Transplant. 2019;33(1):e13450.
- Gerogianni G. Factors affecting pain in hemodialysis and non-pharmacological management. Cureus. 2023;15(2):e35448. doi:10.7759/cureus.35448.
- Wilkinson TJ, Nixon DGD, Palmer J, et al. Differences in physical symptoms between those with and without kidney disease: a comparative study across disease stages in a UK population. BMC Nephrol. 2021;22(1):147. doi:10.1186/s12882-021-02355-5.
- Haruyama K, Kawakami M, Otsuka T. Effect of core stability training on trunk function, standing balance, and mobility in stroke patients: a randomized controlled trial. Neurorehabil Neural Repair. 2017;31(3):240–249. doi:10.1177/1545968316675431.
- Cabrera-Martos I, Jiménez-Martín AT, López-López L, et al. Effects of a core stabilization training program on balance ability in persons with Parkinson’s disease: a randomized controlled trial. Clin Rehabil. 2020;34(6):764–772. doi:10.1177/0269215520918631.
- Salik Sengul Y, Yilmaz A, Kirmizi M, et al. Effects of stabilization exercises on disability, pain, and core stability in patients with non-specific low back pain: a randomized controlled trial. Work. 2021;70(1):99–107. doi:10.3233/WOR-213557.
- Hamilton DM, Haennel RG. Validity and reliability of the 6-minute walk test in a cardiac rehabilitation population. J Cardiopulm Rehabil. 2000;20(3):156–164. doi:10.1097/00008483-200005000-00003.
- Thong ISK, Jensen MP, Miró J, et al. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018;18(1):99–107. doi:10.1515/sjpain-2018-0012.
- Barotfi S, Molnar MZ, Almasi C, et al. Validation of the kidney disease quality of life-short form questionnaire in kidney transplant patients. J Psychosom Res. 2006;60(5):495–504. doi:10.1016/j.jpsychores.2005.09.009.
- Akuthota V, Ferreiro A, Moore T, et al. Core stability exercise principles. Curr Sports Med Rep. 2008;7(1):39–44.
- Theodorakopoulou MP, Boutou AK, Pella E, et al. Cardiorespiratory fitness in kidney transplant recipients compared to patients with kidney failure: a systematic review and meta-analysis. Transpl Int. 2021;34(10):1801–1811. doi:10.1111/tri.13961.
- Kohl LdM, Signori LU, Ribeiro RA, et al. Prognostic value of the six-minute walk test in end-stage renal disease life expectancy: a prospective cohort study. Clinics. 2012;67(6):581–586. doi:10.6061/clinics/2012(06)06.
- Dos Santos PR, Mendonça CR, Hernandes JC, et al. Pain in patients with chronic kidney disease undergoing hemodialysis: a systematic review. Pain Manag Nurs. 2021;22(5):605–615. doi:10.1016/j.pmn.2021.05.009.
- Gil APP, Lunardi AC, Santana FR, et al. Impact of renal transplantation and immunosuppressive therapy on muscle strength, functional capacity, and quality of life: a longitudinal study. Transplant Proc. 2020;52(5):1279–1283. doi:10.1016/j.transproceed.2020.02.038.