
ABSTRACT
Evidence suggests that providing out-of-home care to children is associated with high levels of compassion fatigue, possibly due to various work-related factors. This review examined the existing literature to determine the extent to which out of home care work results in compassion fatigue. To do so, it established which out of home care settings compassion fatigue has been measured in, how, and what factors contribute to developing compassion fatigue in this work. The study conducted a comprehensive search of five electronic databases (CINAHL, MEDLINE, PsycINFO, PubMED, and CENTRAL) for full-text articles examining compassion fatigue in out-of-home care workers caring for children aged 0–18 years. Out of the 2,759 articles initially identified, 14 articles were included. Studies were assessed against the Joanna Briggs Institute (JBI) Critical Appraisal Checklists for risk of bias. The findings suggest that compassion fatigue is prevalent in various out-of-home care settings and has been measured using validated quantitative and qualitative measures. Out of home care workers caring for children reported symptoms consistent with compassion fatigue, but a range of protective factors were also identified that may reduce its negative impact. This review highlights the need for further research in this area, using larger sample sizes and including a more comprehensive range of out-of-home care workers, settings, and countries.
Practice Implications
Compassion fatigue has been investigated in foster carers but very few studies on workers in residential care facilities
Despite the high levels of compassion fatigue identified in Out of Home Care Workers, few studies included interventions to improve outcomes in this population
Further investigation into protective factors against compassion fatigue needed, e.g. staff supervision and emotional support programs
Higher levels of job satisfaction were associated with lower levels of compassion fatigue, thus should be cultivated within residential care
Introduction
It is conservatively estimated that worldwide approximately 2.7 million children, aged from 0 to 17 years, are in a form of government residential care (Cappa et al., Citation2022). While there are various terms for residential care used across different countries and this has often evolved over time (Ainsworth & Thoburn, Citation2014), a consistency is that many of these children have been removed from their parents or guardians as a result of maltreatment, neglect or abuse (Australian Institute of Health and Welfare, Citation2020). Care options in the Australian context typically include kinship care, where children are placed with other family members, or out of home care, which can include foster care (where they are placed in the carer’s own home) or residential care (where paid carers look after children in designated houses or facilities) (Hiles Howard et al., Citation2015; Leloux-Opmeer et al., Citation2017). Residential treatment or youth detention facilities may also be a care option if the child has severe mental health needs or has been sentenced to a period of detention due to criminal offending (Zelechoski et al., Citation2013). In Australia, over 46,000 children are currently in some form of out of home care (Australian Institute of Health and Welfare, Citation2021). Of these children, over 16,000 have been placed in foster care and a further ~ 3,000 into residential care (Australian Institute of Health and Welfare, Citation2021). Given the increasing number of children who are being placed into out of home care there is an associated increase in need for out of home care workers (OHCW). Organisations must therefore encourage staff retention and minimize turnover. However, there are a range of work-related factors that make staff retention difficult, including the psychological impact of the working environment (Purdy & Antle, Citation2022).
Out of home care workers often provide care to children who have experienced trauma (Hughes, Citation2004). As a result of this trauma, these children can manifest overt aggressive and anti-social behaviors or can have symptoms consistent with anxiety and depression, which the people caring for them are subsequently exposed to (Li et al., Citation2019). As a result of the vicarious trauma that the OHCW are exposed to by their role, compassion fatigue and associated concerns, such as secondary traumatic stress, are a significant risk for this population (Papovich, Citation2020; Reinhardt, Citation2016). Evidence suggests that residential treatment facility workers, similar to like other out of home care workers such as residential care workers and foster carers, also have a high risk of developing compassion fatigue (Eastwood & Ecklund, Citation2008).
Compassion fatigue has been characterized as a form of “empathy based stress,” which is closely linked with secondary traumatic stress and vicarious traumatization (Rauvola et al., Citation2019). Exposure to trauma (e.g., via working closely with children who have experienced trauma) combined with experiencing empathy can result in these forms of stress (Rauvola et al., Citation2019). Countertransference can also occur between workers and clients. This is when negative reactions of the care worker may be elicited from projective identifications, the interactions between client and worker, or unresolved issues or traumas for the worker that arise while working with the client (Berzoff & Kita, Citation2010). While this is an important and associated concept and can co-occur or precede compassion fatigue, it is not explored in this review. The terms compassion fatigue, secondary traumatic stress, and vicarious trauma are often used interchangeably within the literature to reflect the emotional impact of exposure to trauma within the work environment. For the purposes of this review, the term compassion fatigue will be used to encompass compassion fatigue, secondary traumatic stress and vicarious trauma. Individuals experiencing compassion fatigue can have negative physical, emotional and psychological outcomes (de Figueiredo et al., Citation2014). Physical symptoms can include increased arousal, sleep disturbances, fatigue, change in eating habits, and headaches (Figley, Citation2013; Gentry, Citation2002; Showalter, Citation2010). Psychological symptoms can include anxiety, depression, outbursts of anger, a sense of an inability to perform their job well, and a sense of dread regarding working with the people in their care (Figley, Citation2013; Gentry, Citation2002). Despite the impacts of compassion fatigue, research has also demonstrated that “compassion training” – including understanding empathetic distress, self-care and self-compassion practices, alongside emotion regulation and psychological flexibility – has been effective in increasing resilience and protective against the negative impacts of compassion fatigue (Hofmeyer et al., Citation2020). This has been investigated in residential care workers, with compassion training deemed a promising approach to counteract burnout, anxiety, and depression on OHCWs, helping to improve their functioning and the quality of the care they provide (Santos et al., Citation2023).
Since compassion fatigue was first identified, research has focused primarily on health care occupations, such as nursing (Cavanagh et al., Citation2020; Xie et al., Citation2021). Comparatively, few studies appear to address compassion fatigue in OHCW. A recent review found 40 studies related to the study of compassion fatigue in health care, with just one study on child protection social workers (Sorenson et al., Citation2016). Similarly, Cocker and Joss (Citation2016) conducted a systematic review, and identified 13 studies that met their inclusion criteria, of which 10 related to nursing (Cocker & Joss, Citation2016). Research into how the different type of out of home care work settings and their relationship with compassion fatigue has not, as of yet, been reviewed and evaluated. This is despite the increased need for OHCW as the demand for child placements increases, and the concerns in this setting with staff retention. Thus, there is a developing need for compassion fatigue to be better understood in out of home care settings.
This review aims to examine the existing literature to determine the extent to which out of home care work results in compassion fatigue, with the following specific research questions:
Which out of home care work settings has compassion fatigue been investigated in?
What methods have been used to measure compassion fatigue in OHCW?
What factors within out of home care work settings contribute to the development of compassion fatigue?
Methods
Registration and Protocol
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review (PRSIMA) (2020) model and was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on 16 August 2021 (CRD42021273798).
Eligibility Criteria
Studies were required to meet the following criteria for inclusion:
Examination of compassion fatigue, secondary traumatic stress, or vicarious trauma.
Population of OHCW, defined as paid care workers, including residential care workers, treatment facility workers, and those providing foster care (in line with a recent scoping review of out of home care (Leloux-Opmeer et al., 2016)), who provided care to children aged 0–17 years.
No search restrictions were applied to the year of publication, but studies were required to have been published in a peer reviewed journal with the full text available in English.
Both quantitative and qualitative studies were eligible for inclusion.
Cross-sectional and experimental studies were eligible for inclusion.
Whilst being intrinsically linked to compassion fatigue, burnout is a symptom, or predictor, of compassion fatigue, and according to Stamm (Citation2005) needs to be measured on its own as well as in conjunction with the other indicators of compassion satisfaction and secondary traumatic stress. Hence studies that specifically focused on burnout without the other compassion fatigue indicators were not included.
Information Sources
Searches were conducted of five electronic databases, including CINAHL, MEDLINE, PsycINFO, PubMED and CENTRAL. Searches were conducted 1 July 2021 to 11 July 2021.
Search Strategy
The search string utilized was (“residential support worker*” OR “residential child care worker*” OR “residential care worker*” OR “institutionalization*” OR “foster parent*” OR “foster care*” OR “foster home care” OR “group home” OR “out of home care*” OR “youth residential care*” OR “youth care facilit*” OR “care facility*” OR “residential care*” OR “residential facilit*” OR “residential”) AND (“empath*” OR “secondary trauma* stress” OR “secondary trauma*” OR “vicarious trauma*” OR “compassion fatigue”).
Selection Process
Studies returned by the search were extracted into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org). A pilot was performed to ensure consistency in inclusion/exclusion of studies. The pilot included the identification of 100 studies using the pre-defined search terms from the electronic database CINAHL, which were subsequently downloaded. Authors (DS, TB, CG, MS) applied the defined inclusion criteria to the titles and abstracts of the pilot studies, verifying that the studies were consistently included or excluded. A subsequent search, utilizing the same search strategy was then conducted through the specified electronic databases from 1 July 2021 to 11 July 2021. Two authors (DS and CG) screened titles and abstracts to identify relevant articles. They worked independently, and without consultation, recording and reviewing the identified studies. Studies included at the title and abstract level were then screened at the full text level by the same screeners. Where the two screeners disagreed, a third screener (MS) was consulted. All screening was conducted with the support of systematic review software Covidence (Veritas Health Innovation, 2021) including noting reasons for exclusion at the full text stage.
Data Collection Process
Details of included studies were exported into Microsoft Excel version 2109 (2016), which was used to store information about study design and methodology, participant demographics and baseline characteristics, and numbers of events or measures of effect.
Data Items
Data extracted from the included studies were recorded in an extraction table, containing the author’s details, year of publication, country of origin, type of OHCW, study setting, whether the study was measuring compassion fatigue, secondary traumatic stress or vicarious trauma, the study design, tests or scales used to measure outcomes (for quantitative studies: credible scales and measures such as the Professional Quality of Life Scale (ProQOL), Adverse Child Experience questionnaire (ACE), the Resilience Questionnaire, Self-Care Practices Questionnaire, Secondary Traumatic Stress Scale; for qualitative studies: themes identified from interviews with participants), statistical tests applied to results, demographic details of participants, and the outcomes of each study.
Risk of Bias Assessment
A structured approach to reduce the risk of bias in studies included in this review was achieved by utilizing the Joanna Briggs Institute (JBI) Critical Appraisal Checklists. The 12 cross-sectional studies were assessed utilizing the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies (Joanna Briggs Institute, Citation2016) and the JBI Checklist for Quasi-Experimental Studies (Non-Randomised) Experimental Studies (Joanna Briggs Institute, Citation2020) was completed the one quasi-experimental study. The JBI Critical Appraisal Checklist for Qualitative Research was completed for the one qualitative study.
Synthesis Method
A narrative synthesis and appraisal of the studies were utilized to describe the findings, along with data extraction tables summarizing the statistics and overall quality of studies identified. The use of narrative synthesis was to allow “the story” of the findings in the studies to be told via words and text (Popay et al., Citation2006) due to the heterogeneity of their methods and settings. Quantitative descriptive analysis was conducted on the included studies. This identified the types of tests and measures that were applied, results from the different studies that measured rates of compassion fatigue, secondary traumatic stress, or vicarious trauma. Qualitative studies were thematically summarized to examine perceptions and issues identified by OHCW caring for children relating to compassion fatigue.
Results
Study Selection
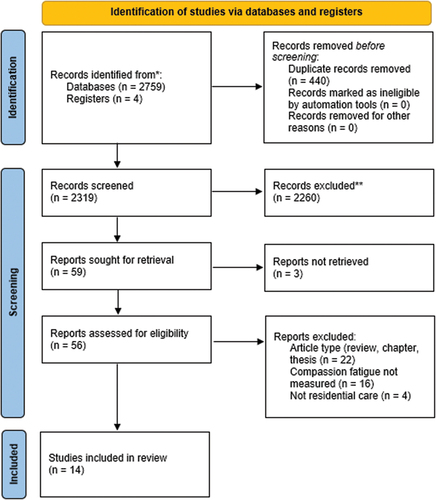
The electronic database search returned 2,759 potential studies with 440 duplicates subsequently removed (). The titles and abstracts of the remaining 2,319 studies were then screened, and a further 2,260 studies were removed as they did not meet the inclusion criteria. The remaining 59 studies were retrieved for full text review with a further 44 studies excluded for the following reasons: not being the correct type of study (n = 22); not measuring compassion fatigue, secondary traumatic stress, or vicarious trauma (n = 16); did not relate to OHCW (n = 4); full text studies could not be located (n = 3). Fourteen studies were included in the final review.
Figure 1. PRISMA (2020) flow diagram.
Quality Assessment
The JBI Critical Appraisal Checklist of cross-sectional studies revealed scores ranging from 28.57% to 71.43% (see ), indicating that these studies are of a weak to moderate quality. The JBI Critical Appraisal Checklist used to analyze the quasi-experimental study revealed a score of 75% (see ), indicating that this study was of moderate quality. The JBI Critical Appraisal Checklist for Qualitative Research indicated that the included qualitative study was of moderate quality (70%) (). The criteria that make up each JBI Critical Appraisal Checklist can be seen in the Supplementary Materials.
Table 1. JBI critical appraisal checklist for analytical cross-sectional studies.
Table 2. JBI checklist for quasi-experimental studies (non-randomised) experimental studies.
Table 3. JBI critical appraisal checklist for qualitative research.
Q1:
Which out of home care work settings has compassion fatigue been investigated in?
Study characteristics from the 14 studies included in this review can be seen in . Out of home care settings included foster care arrangements (n = 6) (Bridger et al., Citation2020; Hannah & Woolgar, Citation2018; Harker et al., Citation2016; Steen & Berhardt, Citation2023; Teculeasa et al., Citation2023; Whitt-Woosley et al., Citation2020), residential care houses (n = 4) (Eastwood & Ecklund, Citation2008; Garwood et al., Citation2020; McNamara, Citation2010; Steinlin et al., Citation2017), (;), and four studies included mixed settings including foster, residential and boarding houses (Borjanić Bolić, Citation2019; Hiles Howard et al., Citation2015; Whitt-Woosley et al., Citation2022; Zerach, Citation2013). As outlined in , studies included in this review identified research on compassion fatigue and its components of secondary traumatic stress or vicarious trauma.
Table 4. Study and participant characteristics.
Six studies were conducted in the United States, two were conducted in Australia, two were conducted in the United Kingdom, one study in Romania, and one study was conducted in Israel, Switzerland, and Serbia. Participants across the 14 studies ranged in age from 22 to 73 years. Eight studies contained more than 50% female participants. Marital status was recorded in four studies, with > 59% of participants being married. Education levels were measured in five studies with the proportion of participants with tertiary level qualifications ranging from 35% to 100%. The amount of experience in out of home care was measured in five studies, with years of experience ranging from less than 1 year to over40 years.
Q2:
What methods have been used to measure compassion fatigue in OHCW?
The quantitative studies included in this review used psychometrically valid tests to measure compassion fatigue in OHCW (). Measures used included the Professional Quality of Life (ProQOL) scale (n = 10), Resilience Questionnaire (n = 1), Sense of Coherence (SOC) scale (n = 2), the Group Environment (GES) scale (n = 1), and the Secondary Traumatic Stress Scale (STSS) (n = 3).
Table 5. Study design, measurement tools and results.
Qualitative methodologies were used by two included studies. Garwood et al. (Citation2020) used mixed methods, with questions devised in line with the Sanctuary Model® Assessment that included 3 open-ended questions. Additionally, semi-structured interviews were used by McNamara (Citation2010). These studies assessed compassion fatigue in OHCW before and after a program that was implemented, and results were thematically analyzed.
Q3:
What factors influence compassion fatigue in the out of home care work environment?
Work Related Factors
Compassion Satisfaction Seven studies examined the relationship between compassion fatigue and job or compassion satisfaction (defined as positive feelings derived from doing helping work effectively (Thomas, Citation2013). Compassion satisfaction was primarily measured with the ProQOL, which was utilized in seven studies. Hannah and Woolgar (Citation2018) found a correlation between those with low intent to continue with fostering, compassion fatigue and compassion satisfaction. Similarly, Hiles Howard et al. (Citation2015) found foster carers differed significantly from a normative sample on all ProQOL subscales, with foster carers reporting higher levels of compassion satisfaction, burnout, and compassion fatigue when compared to the normative sample. Teculeasa et al. (Citation2023) suggested that compassion satisfaction, the perceived quality of relationship between foster carer and child, and the perceived closeness in the foster parent–child relationship were protective against compassion fatigue and contributed to lower compassion fatigue scores. No significant differences were found by Zerach (Citation2013) between their sample of residential care workers compared to boarding school workers with respect to compassion fatigue and burnout, however residential care workers reported higher levels of compassion satisfaction than boarding school workers. In foster carers, Whitt-Woosley et al. (Citation2020) found that on average, burnout was not reported in high levels, but high compassion satisfaction was evident in their sample. Bridger et al. (Citation2020) also found higher than relative scores on compassion satisfaction in foster carers, suggesting that this may be mitigating the overall distress levels among their participants.
Job satisfaction was measured with the Questionnaire on Job Satisfaction in Trauma-Sensitive Care (Hannah & Woolgar, Citation2018), and two Likert scales developed from previous studies were utilized (Steinlin et al., Citation2017). Participants with low job satisfaction had significantly higher compassion fatigue and burnout scores, and lower compassion satisfaction scores (Hannah & Woolgar, Citation2018). Steinlin et al. (Citation2017) also identified a correlation between higher job satisfaction (measured by support from employer, communication with peers, pleasure in doing work and, organizational structures and resources) and lower secondary traumatic stress symptoms.
Exposure to Trauma and Violence within Workplace Four studies (Borjanić Bolić, Citation2019; Hannah & Woolgar, Citation2018; Steinlin et al., Citation2017; Whitt-Woosley et al., Citation2020) collected data on workers’ exposure to trauma, either vicariously through the children they provided care to or through threats or acts of violence directed toward them. A significant number of foster carers were exposed to children’s trauma, with Whitt-Woosley et al. (Citation2020) finding that 77.8% of foster parents reported distressing thoughts or feelings about their child’s trauma for more than 30 days and 25.8% of these foster parents described this distress as moderate to extreme. In the study by Steinlin et al. (Citation2017) approximately 83% of residential care workers reported experiencing an assault or threatening situation during work, which could have resulted in death or injury, and 73% of residential care workers reported having heard or read about at least one traumatic event in the life of a child or adolescent. In foster care settings, Hannah and Woolgar (Citation2018) also found that 48% of carers had been physically hurt or threatened by a young person in their care. Borjanić Bolić (Citation2019) found that residential workers who spent up to half of their working hours directly working with youths in care reported compassion fatigue at higher rates than workers who had longer periods of exposure.
Burnout The relationships between compassion fatigue and burnout were examined in five studies. Whitt-Woosley et al. (Citation2020) found significant relationships between reported levels of burnout and compassion satisfaction in foster carers. In residential care workers, Eastwood and Ecklund (Citation2008) found a relationship between burnout and compassion fatigue. Similarly, Bridger et al. (Citation2020) found compassion fatigue in foster carers was directly and positively predicted by burnout and primary trauma. Hiles Howard et al. (Citation2015) did not report the relationship between burnout and compassion fatigue but did identify that those who were more direct care providers (as compared to indirect care providers) predictably reported less burnout. Zerach (Citation2013) also didn’t report the interaction between burnout and secondary trauma, however, did report that males were more likely to report burnout than females.
Other The impact of the COVID-19 pandemic was explored in Whitt-Woosley et al. (Citation2022), who found significant increases in compassion fatigue symptoms including intrusion and alterations in cognition and mood.
Individual Factors
Resilience
Resilience was one of the individual factors investigated in relation to compassion fatigue, however, was only measured in two studies. Hiles Howard et al. (Citation2015) found high levels of supportive factors and resilience were correlated with lower levels of compassion fatigue. Harker et al. (Citation2016) also found higher scores on resilience correlated to lower scores on compassion fatigue. When mindfulness was added to the regression it was found that higher scores on mindfulness were related to lower levels of psychological distress (Harker et al., Citation2016).
Sense of Coherence Two studies investigated sense of coherence (SoC) in relation to compassion fatigue. SoC is defined as the extent to which one has a pervasive, enduring yet dynamic feeling of confidence that the internal and external environment are predictable, and that there is a high probability that things will work out as well as can reasonably be expected. SoC was found to predict compassion fatigue and burnout, but not compassion satisfaction (Zerach, Citation2013). Steinlin et al. (Citation2017) also found correlation between sense of coherence and lower compassion fatigue symptoms.
Psychological traits Two studies looked at individual psychological traits of OHCWs in relation to compassion fatigue. For example, attachment anxiety (Zerach, Citation2013) and thought suppression (Hannah & Woolgar, Citation2018), were found to significantly impact compassion fatigue levels in residential care workers and foster carers. Attachment anxiety was positively associated with compassion fatigue and negatively related to compassion satisfaction (Zerach, Citation2013). Higher levels of psychological inflexibility and increased thought suppression were associated with higher compassion fatigue, with thought suppression positively associated with compassion fatigue (Hannah & Woolgar, Citation2018).
Age Mixed results were evident in relation to the impact of age on compassion fatigue in OHCW. For example, some studies found that younger age was associated with increased compassion fatigue. Steen and Berhardt (Citation2023) found that older foster parents had significantly lower scores on the STSS. Garwood et al. (Citation2020) utilized results from residential care workers on the ProQOL questionnaire comparing participants by age group. They found that compassion fatigue was correlated with age for the under 30 years, 30–40 years, 41–50 years, and over 51-year groups, with younger workers reporting higher levels (Garwood et al., Citation2020). Harker et al. (Citation2016) also found age was not significantly correlated to compassion fatigue levels. However, Bridger et al. (Citation2020) found no significant impact of age on compassion fatigue in foster carers.
Gender Just two studies compared outcomes based on gender. Bridger et al. (Citation2020) found that female OHCW reported higher levels of compassion fatigue than male OHCW (Bridger et al., Citation2020). Similarly, Hiles Howard et al. (Citation2015) found that female OHCW reported higher levels of compassion fatigue than males.
Having their Own Children Two studies also investigated whether workers having their own children impacted compassion fatigue. Hannah and Woolgar (Citation2018) found that workers with their own children had lower levels of compassion fatigue than those workers that did not. However, the only other study that examined this did not find a significant effect (Hiles Howard et al., Citation2015).
Education Only one study investigated the impact of education and found that overall education was not a significant predictor of compassion fatigue based on scores from the Resilience Questionnaire (Hiles Howard et al., Citation2015).
Support Strategies
Staff Supervision and Workplace Support Three studies investigated the role of supervision and workplace supports in mitigating the impacts of compassion fatigue. For example, the evaluation of the Staff Supervision and Support Program by McNamara (Citation2010) indicates the program was relevant to identifying, managing, and improving issues pertaining to compassion fatigue of staff at a residential treatment facility. This was achieved through professional development and the ways in which supervisors respond to staff with symptoms of compassion fatigue. The thematic analysis done by Garwood et al. (Citation2020) examined the effect of the Sanctuary Model®® Assessment with their findings indicating that changes in staff awareness of the impact of trauma have led to more support across teams, including more one-on-one time and adjustments to how staff approach interactions with each other in the workplace (Garwood et al., Citation2020). Steinlin et al. (Citation2017) also found that increased communication and support within the team and institutional structures and resources correlated with fewer compassion fatigue symptoms.
Support Outside of Work Support factors outside the work environment were discussed by two studies in relation to protecting against compassion fatigue. Eastwood and Ecklund (Citation2008) found that feelings of being supported outside of work were a protective factor against the negative component of compassion fatigue and burnout. The study by Whitt-Woosley et al. (Citation2020) found that the number of foster parenting resources utilized, and general caregiver support as important to reducing burnout and compassion fatigue symptoms of foster carers. They found that foster carer support was a significant beneficial factor, as was emotional support, on lowering compassion fatigue levels (Whitt-Woosley et al., Citation2020).
Self-Care Four studies examined self-care practices of residential care workers and foster carers, and whether that provided a protective measure against compassion fatigue. This was assessed with scales such as the Professional Self-Care Scale, the Trauma Informed Self-Care Measure, and questionnaires devised by the authors themselves. Reading and socialization with family were identified as self-care methods which acted as protective factors against compassion fatigue in residential care workers (Eastwood & Ecklund, Citation2008). Bridger et al. (Citation2020) found self-care had an indirect effect on reducing compassion fatigue and was correlated with empathy and resilience. Self-care was also assessed in Garwood et al. (Citation2020) where participants who undertook the Sanctuary Model® Assessment outlined how the model facilitated increased self-awareness and encouraged permission for self-care.
Discussion
This systematic review evaluated the evidence addressing compassion fatigue in OHCW. In particular, it focused on which out of home care settings compassion fatigue has been assessed in, how compassion fatigue has been measured, and what factors contribute to compassion fatigue. Findings from this review indicated that compassion fatigue and associated constructs have been investigated in a range of out of home care settings – though there was limited evidence available for all settings in comparison to other industries (i.e., only 14studies in total). Compassion fatigue was generally measured via self-report on validated scales, though some studies used non-validated self-report measures. Overall, a range of work-related factors (e.g., job and compassion satisfaction, exposure to trauma and violence, burnout), individual factors (e.g., age, gender), and support strategies (e.g., supervisor support, support outside of work) contributed to compassion fatigue.
Which Out of Home Care Work Settings Has Compassion Fatigue Been Investigated In?
Compassion fatigue (encompassing related terms secondary traumatic stress, or vicarious trauma) were assessed in each type of OHCW included in this review (residential care workers, foster carers and residential treatment workers) and their associated settings. Evidence was spread across a number of countries; however, the majority of studies were undertaken in the United States. The included studies were predominantly from English-speaking countries due to the search restrictions; however, this may also point to higher concern for OHCW in particular regions. For example, the high rates of children being placed in residential care and foster care in the United States (United States Department of Health and Human Services, Citation2017), Australia (Australian Institute of Health and Welfare, Citation2021), and the United Kingdom (GOV.UK, Citation2022) may have led to these studies being more likely to be conducted.
In conducting this review, it was evident that there is ambiguity surrounding the terms compassion fatigue, secondary traumatic stress, and vicarious trauma. This review suggests that in out of home care settings, the terms compassion fatigue and secondary traumatic stress outweighed the use of vicarious trauma. However, there appeared to be some overlap in the use of these terms across studies.
Although the evidence in this space is limited and should be grown in all settings, foster care settings are currently the higher researched setting (6 out of 14 studies). Four of the studies also did investigate multiple settings and types of workers within the one study. Arguably, workers in residential care settings and residential care treatment facilities (through the nature of design and requirement to care for higher numbers of children per setting), are potentially at higher risk for compassion fatigue (Audin et al., Citation2018); yet less researched. Prevalence of foster care versus residential care settings may be causing this, but it may be of interest to investigate further.
What Methods Have Been Used to Measure Compassion Fatigue in OHCW?
The scale most used to measure compassion fatigue in OHCW was the ProQOL questionnaire (Stamm, Citation2005). This scale has been extensively used to measure the components of compassion fatigue, burnout, and compassion satisfaction, has been continually updated, is reliable and valid, and has been translated into other languages (Stamm, Citation2005). Interestingly, only one study measured resilience. The focus was also largely on the individual, and less so on the residential setting or environment. This is likely due to most studies focusing on foster care, however, could be a key factor in supporting and reducing the impacts of compassion fatigue for OHCW.
What Factors within Out of Home Care Settings Contribute to the Development of Compassion Fatigue?
Work Related Factors
According to Stamm (Citation2005) compassion fatigue comprises high levels of secondary traumatic stress (or vicarious trauma) and burnout with low levels of compassion satisfaction. The development of compassion fatigue occurs for OHCW through prolonged exposure to the traumatic details of the children that they provide care to (Stamm, Citation2005). Length of time and rate of exposure (to traumatized children) was a significant predictor of secondary traumatic stress (Borjanić Bolić, Citation2019; Whitt-Woosley et al., Citation2020). OHCW are at a significant risk of exposure to trauma and violence within the workplace. Extremely high rates of exposure were reported in the studies included and are likely to be reflected in other settings that have not yet been investigated. A larger scale study to investigate the prevalence and nature of the exposure to trauma and violence in these workplace settings may be justified, but more importantly, supporting and providing training and appropriate counseling or responses to OHCWs is essential. As one of the largest groups of OHCW (Australian Institute of Health and Welfare, Citation2022), foster care providers may be at higher risk than residential care workers, as they would be living in their own environment and will not have the support of other workers. However, this could also be a protective factor, and residential care workers are also expected to work under shift work environments which can also be problematic for a number of additional reasons (e.g., sleep, impacts on home life etc.) (Dorrian et al., Citation2017). Interventions could potentially look to support workers who have experienced certain rates of exposure to trauma or violence within the workplace or have been working for particular periods of time and may exhibit symptoms of burnout, by intervening prior to workers choosing to remove themselves from the situation by quitting or relocating.
Importantly, while burnout has been conceptualized as a contributing factor to compassion fatigue, and therefore strategies to address burnout will also reduce compassion fatigue, some argue that there are questions remaining about the directionality of the relationship and how much compassion fatigue may contribute to overall burnout. Further understanding and research into the specific needs of those struggling with compassion fatigue could tease this out further.
Several included studies found that higher levels of job satisfaction were also associated with reduced compassion fatigue (Hannah & Woolgar, Citation2018; Steinlin et al., Citation2017; Zerach, Citation2013).This suggests that improving OHCW level of job satisfaction may provide a mitigating effect against the negative effects of compassion fatigue, which in turn may improve intent to remain in this profession, providing stability for children in care. Similarly, Hannah and Woolgar (Citation2018) found that greater intent to continue to work as a foster carer was associated with lower levels of compassion fatigue and burnout, and higher compassion satisfaction scores (Hannah & Woolgar, Citation2018).
Individual Factors
There was some evidence that certain demographic factors, such as whether OHCW had their own children, age, and gender, may affect compassion fatigue (Garwood et al., Citation2020; Harker et al., Citation2016; Hiles Howard et al., Citation2015). Taken together, this evidence is inconclusive, and therefore may require further investigation as to whether certain groups should be targeted for intervention or protection measures against compassion fatigue. For example, 11 of 14 studies had over 50% female participants suggesting this is a more female dominated industry and it may be worthwhile to target interventions accordingly.
Further investigation into resilience and sense of coherence (which has been linked to health variables including psychological wellbeing, social support, stress, and adaptive coping strategies) (Olsson et al., Citation2006), in developing protective strategies for OHCW against the impacts of compassion fatigue is also recommended.
Support Strategies
Out of the 14 studies included in this review, only 2 investigated interventions to support OHCW with compassion fatigue (Garwood et al., Citation2020; McNamara, Citation2010). Trauma informed care (Kim et al., Citation2021) and staff supervision and support (Dehlin & Lundh, Citation2018) had promising results and are evident in the wider literature. This suggests they should both be key components of professional development and ongoing support for OHCWs, but should also be investigated more widely, alongside other strategies. Encouraging OHCW to seek emotional and practical support such as training outside of work (particularly where work environments are not currently providing such things) may also reduce the impacts of compassion fatigue and secondary traumatic stress in this population (Gentry et al., Citation2004). However, arguably this is too much to ask, and this training and support should be built into their work rather than eating into their free time as well. Self-care has some promising but inconclusive evidence in its effect on compassion fatigue (Eastwood & Ecklund, Citation2008).
The Staff Support and Supervision Program in McNamara (Citation2010) looked at improving levels of support for workers, and the Sanctuary Model® Assessment (Garwood et al., Citation2020) was used to determine if increased knowledge in trauma and self-care was effective against compassion fatigue. Both programs provided some insight into the benefits that interventions can have in reducing compassion fatigue (Garwood et al., Citation2020; McNamara, Citation2010).
Limitations of Evidence
Out of the fourteen included studies, just two were published prior to 2016. This suggests that research into the impact that out of home care work on compassion fatigue is still in its infancy. As a result, the range of evidence available for this review was limited. After the JBI Checklists were applied, the studies were also assessed as only from weak to moderate quality. As such, we must be cautious in generalizing all results to the broader populations of OHCW. A further issue with the quality of the studies can be seen with the lack of power analyses, which was only reported by two included studies. It is therefore possible that some studies may have been underpowered, further limiting generalizability.
Limitations of Review Process
The review process confirmed that there is significant confusion in terminology across the literature investigating and describing compassion fatigue, such as secondary traumatic stress, vicarious trauma, and burnout, which are often used interchangeably (Salmond et al., Citation2019). However, according to Stamm (Citation2005) secondary traumatic stress, burnout and compassion satisfaction are separate traits that need to be measured separately. Whilst being intrinsically linked to compassion fatigue, burnout is a symptom, or predictor, of compassion fatigue, and according to Stamm (Citation2005) needs to be measured on its own as well as in conjunction with the other indicators of compassion satisfaction and secondary traumatic stress. Hence, studies that specifically focused on burnout without the other compassion fatigue indicators were not included. This could have excluded studies in which other psychometric tests that measure burnout, such as the Maslach Burnout Inventory (Maslach et al., Citation1997), that has been previously used to study this component of compassion fatigue in out of home care work settings. Our eligibility criteria were designed to capture both cross-sectional and experimental studies and did not exclude any particular methodologies. While this allowed us to determine how compassion fatigue has been assessed and measured in residential care settings, results reported on experimental studies could be linked to the intervention as opposed to the setting itself. Whilst a thorough and reproducible search strategy was designed for this systematic review, some studies may have been missed if they were contained on databases other than the five that were searched. Furthermore, only full text studies in English were included. Studies in other languages may have provided international context that may have provided further supplemental evidence for this review.
Implications and Future Directions
Despite the high levels of compassion fatigue identified in OHCW, few studies included interventions to improve outcomes in this population. Due to the nature of work being conducted in this setting, and the extremely high rates of exposure to children’s trauma, as well as violence toward themselves in the workplace, OHCW are arguably inevitably going to experience compassion fatigue at some point. Therefore, we need to move beyond recording and problematizing these constructs and experiences, toward interventions and protective factors for these vital carers. This is likely due to the nature of out of home care work, with a lack of control over the trauma these workers are exposed to. There is an indication that some interventions, such as those examined in McNamara (Citation2010) and Garwood et al. (Citation2020) may minimize some of the risk of compassion fatigue. These interventions are based on improving OHCW understanding of trauma, communication and support via internal organizational programs or with a program such as the Staff Supervision and Support Program. Early findings suggest that those programs may be beneficial and warrant further study to determine their efficacy in different out of home care settings (Garwood et al., Citation2020; McNamara, Citation2010). While this was not the intended focus of our review, future reviews may look to target more experimental studies that have introduced interventions to support OHCW with compassion fatigue.
Compassion fatigue has been identified as a condition that poses a risk to OHCW across the world. With an ongoing need for OHCW, the identification of factors that influence their wellbeing, level of job satisfaction, and intent to continue working in this area is invaluable. This review indicated that, as expected, out of home care work is associated with compassion fatigue, in workers. These outcomes were seen across a range of out of home care settings. However, it appears that there are certain personal and situational factors (e.g., levels of support) which are likely to be protective against compassion fatigue. Furthermore, this review identified that there are a range of validated quantitative and qualitative measures used to identify compassion fatigue and associated psychological outcomes, which will ideally be used to grow this field of research.
Supplemental Material
Download MS Word (34.2 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/0886571X.2024.2310583
References
- Ainsworth, F., & Thoburn, J.(2014). An exploration of the differential usage of residential childcare across national boundaries. International Journal of Social Welfare, 23(1), 16–24.
- Audin, K., Burke, J., & Ivtzan, I. (2018). Compassion fatigue, compassion satisfaction and work engagement in residential child care. Scottish Journal of Residential Child Care, 17(3), 5–27.
- Australian Institute of Health and Welfare. (2020). Australia’s children. https://www.aihw.gov.au/getmedia/6af928d6-692e-4449-b915-cf2ca946982f/aihw-cws-69-print-report.pdf.aspx?inline=true
- Australian Institute of Health and Welfare. (2021). Child protection Australia 2019 - 2020. https://www.aihw.gov.au/reports/child-protection/child-protection-australia-2019-20/summary
- Australian Institute of Health and Welfare. (2022). Child protection Australia 2020 - 2021. https://www.aihw.gov.au/reports/child-protection/child-protection-australia-2020-21/contents/out-of-home-care/what-type-of-placements-were-children-in
- Berzoff, J., & Kita, E. (2010). Compassion fatigue and countertransference: Two different concepts. Clinical Social Work Journal, 38(3), 341–349. https://doi.org/10.1007/s10615-010-0271-8
- Borjanić Bolić, E. (2019). Secondary traumatic stress and vicarious traumatization in child welfare professionals in Serbia. Journal of Public Child Welfare, 13(2), 214–233. https://doi.org/10.1080/15548732.2018.1502117
- Bridger, K. M., Binder, J. F., & Kellezi, B. (2020). Secondary traumatic stress in foster carers: Risk factors and implications for intervention. Journal of Child and Family Studies, 29(2), 482–492. https://doi.org/10.1007/s10826-019-01668-2
- Cappa, C., Petrowski, N., Deliege, A., & Khan, M. R. (2022). Monitoring the situation of children living in residential care: Data gaps and innovations. Vulnerable Children and Youth Studies, 17(2), 110–118. https://doi.org/10.1080/17450128.2021.1996669
- Cavanagh, N., Cockett, G., Heinrich, C., Doig, L., Fiest, K., Guichon, J. R., Page, S., Mitchell, I., & Doig, C. J. (2020). Compassion fatigue in healthcare providers: A systematic review and meta-analysis. Nursing Ethics, 27(3), 639–665. https://doi.org/10.1177/0969733019889400
- Cocker, F., & Joss, N. (2016). Compassion fatigue among healthcare, emergency and community service workers: A systematic review. International Journal of Environmental Research and Public Health, 13(6), 618. https://doi.org/10.3390/ijerph13060618
- de Figueiredo, S., Yetwin, A., Sherer, S., Radzik, M., & Iverson, E. (2014). A cross-disciplinary comparison of perceptions of compassion fatigue and satisfaction among service providers of highly traumatized children and adolescents. Traumatology, 20(4), 286. https://doi.org/10.1037/h0099833
- Dehlin, M., & Lundh, L. G. (2018, December). Compassion fatigue and compassion satisfaction among psychologists: Can supervision and a reflective stance be of help? Journal of Pers Oriented Res, 4(2), 95–107. https://doi.org/10.17505/jpor.2018.09
- Dorrian, J., Grant, C., & Banks, S. (2017). An industry case study of ‘stand-up’and ‘sleepover’night shifts in disability support: Residential support worker perspectives. Applied Ergonomics, 58, 110–118. https://doi.org/10.1016/j.apergo.2016.05.016
- Eastwood, C. D., & Ecklund, K. (2008). Compassion fatigue risk and self-care practices among residential treatment center childcare workers. Residential Treatment for Children & Youth, 25(2), 103–122. https://doi.org/10.1080/08865710802309972
- Figley, C. R. (2013). Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. Routledge.
- Garwood, M. M., Beyer, M. R., Hammel, J., Schutz, T., & Paradis, H. A. (2020). Trauma-informed care intervention for culture and climate change within a child welfare agency. Child Welfare, 98(4), 1–26.
- Gentry, J. E. (2002). Compassion fatigue: A crucible of transformation. Journal of Trauma Practice, 1(3–4), 37–61. https://doi.org/10.1300/J189v01n03_03
- Gentry, J. E., Baggerly, J., & Baranowsky, A. (2004). Training-as-treatment: Effectiveness of the certified compassion fatigue specialist training. International Journal of Emergency Mental Health, 6(3), 147–155.
- GOV.UK. (2022). Children looked after in England including adoptions: Reporting year 2022. https://explore-education-statistics.service.gov.uk/find-statistics/children-looked-after-in-england-including-adoptions
- Hannah, B., & Woolgar, M. (2018). Secondary trauma and compassion fatigue in foster carers. Clinical Child Psychology and Psychiatry, 23(4), 629–643. https://doi.org/10.1177/1359104518778327
- Harker, R., Pidgeon, A. M., Klaassen, F., & King, S. (2016). Exploring resilience and mindfulness as preventative factors for psychological distress burnout and secondary traumatic stress among human service professionals. Work, 54(3), 631–637. https://doi.org/10.3233/WOR-162311
- Hiles Howard, A. R., Parris, S., Hall, J. S., Call, C. D., Razuri, E. B., Purvis, K. B., & Cross, D. R. (2015). An examination of the relationships between professional quality of life, adverse childhood experiences, resilience, and work environment in a sample of human service providers. Children and Youth Services Review, 57, 141–148. https://doi.org/10.1016/j.childyouth.2015.08.003
- Hofmeyer, A., Kennedy, K., & Taylor, R. (2020). Contesting the term ‘compassion fatigue’: Integrating findings from social neuroscience and self-care research. Collegian, 27(2), 232–237. https://doi.org/10.1016/j.colegn.2019.07.001
- Hughes, D. (2004). An attachment-based treatment of maltreated children and young people. Attachment & Human Development, 6(3), 263–278. https://doi.org/10.1080/14616730412331281539
- Joanna Briggs Institute. (2016). JBI critical appraisal checklist for analytical cross sectional studies. The Joanna Briggs Institute.
- Joanna Briggs Institute. (2020). JBI critical appraisal checklist for quasi-experimental studies. Adelaide.
- Kim, J., Aggarwal, A., Maloney, S., & Tibbits, M. (2021). Organizational assessment to implement trauma-informed care for first responders, child welfare providers, and healthcare professionals. Professional Psychology: Research and Practice, 52(6), 569. https://doi.org/10.1037/pro0000408
- Leloux-Opmeer, H., Kuiper, C. H., Swaab, H. T., & Scholte, E. M. (2017). Children referred to foster care, family-style group care, and residential care: (how) do they differ? Children and Youth Services Review, 77, 1–9. https://doi.org/10.1016/j.childyouth.2017.03.018
- Li, D., Chng, G. S., & Chu, C. M. (2019). Comparing long-term placement outcomes of residential and family foster care: A meta-analysis. Trauma, Violence, & Abuse, 20(5), 653–664. https://doi.org/10.1177/1524838017726427
- Maslach, C., Jackson, S. E., & Leiter, M. P. (1997). Maslach burnout inventory. Scarecrow Education.
- McNamara, P. M. (2010). Staff support and supervision in residential youth justice: An Australian model. Residential Treatment for Children & Youth, 27(3), 214–240. https://doi.org/10.1080/0886571X.2010.501630
- Olsson, M., Hansson, K., Lundblad, A.-M., & Cederblad, M. (2006). Sense of coherence: Definition and explanation. International Journal of Social Welfare, 15(3), 219–229. https://doi.org/10.1111/j.1468-2397.2006.00410.x
- Papovich, C. (2020). Trauma & children in foster care: A comprehensive overview. Forensic Scholars Today, 5(4), 1–5.
- Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., Britten, N., Roen, K., & Duffy, S. (2006). Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme version. 1(1), b92. https://d1wqtxts1xzle7.cloudfront.net/39246301/02e7e5231e8f3a6183000000-libre.pdf?1445068016=&responsecontent-disposition=inline%3B+filename%3DGuidance_on_the_conduct_of_narrative_syn.pdf&Expires=1706510326&Signature=W4vgxAzWnZkkdYc3nJV70seiP8ovpPRW0ckgG6UyA53whA3X~Pair-Id=APKAJLOHF5GGSLRBV4ZA
- Purdy, L. M., & Antle, B. F. (2022). Reducing trauma in residential direct care staff. Residential Treatment for Children & Youth, 39(2), 179–191. https://doi.org/10.1080/0886571X.2021.1960240
- Rauvola, R. S., Vega, D. M., & Lavigne, K. N. (2019). Compassion fatigue, secondary traumatic stress, and vicarious traumatization: A qualitative review and research agenda. Occupational Health Science, 3(3), 297–336. https://doi.org/10.1007/s41542-019-00045-1
- Reinhardt, C. (2016). Compassion Fatigue and Compassion Satisfaction in Foster Carers: A Mixed Methods Approach, University of Limerick [ PhD thesis].
- Salmond, E., Salmond, S., Ames, M., Kamienski, M., & Holly, C. (2019). Experiences of compassion fatigue in direct care nurses: a qualitative systematic review. JBI Evidence Synthesis, 17(5), 682–753. https://doi.org/10.11124/JBISRIR-2017-003818
- Santos, L., Pinheiro, M. D. R., & Rijo, D. (2023). The effects of the compassionate mind training for caregivers on professional quality of life and mental health: outcomes from a cluster randomized trial in residential youth care settings. Child & Youth Care Forum, 53(1), 195–215. https://doi.org/10.1007/s10566-023-09749-6
- Showalter, S. E. (2010). Compassion fatigue: what is it? Why does it matter? Recognizing the symptoms, acknowledging the impact, developing the tools to prevent compassion fatigue, and strengthen the professional already suffering from the effects. American Journal of Hospice & Palliative Medicine®, 27(4), 239–242. https://doi.org/10.1177/1049909109354096
- Sorenson, C., Bolick, B., Wright, K., & Hamilton, R. (2016). Understanding compassion fatigue in healthcare providers: A review of current literature. Journal of Nursing Scholarship, 48(5), 456–465. https://doi.org/10.1111/jnu.12229
- Stamm, B. (2005). The professional quality of life scale: compassion satisfaction, burnout & compassion fatigue/secondary trauma scales. Sidran Press. Retrieved from. http://www.isu.edu/irh/documents/proqol
- Steen, J., & Berhardt, C. (2023). Secondary traumatic stress and posttraumatic growth among foster parents. Journal of Public Child Welfare, 17(2), 375–389. https://doi.org/10.1080/15548732.2022.2036293
- Steinlin, C., Dölitzsch, C., Kind, N., Fischer, S., Schmeck, K., Fegert, J. M., & Schmid, M. (2017). The influence of sense of coherence, self-care and work satisfaction on secondary traumatic stress and burnout among child and youth residential care workers in Switzerland. Child & Youth Services, 38(2), 159–175. https://doi.org/10.1080/0145935X.2017.1297225
- Teculeasa, F., Golu, F., & Gorbănescu, A. (2023). What mediates the link between foster parents’ sensitivity towards child posttraumatic stress symptoms and job satisfaction? The role of compassion fatigue and foster parent-child relationship. Journal of Child & Adolescent Trauma, 16(2), 309–320. https://doi.org/10.1007/s40653-022-00513-x
- Thomas, J. (2013). Association of personal distress with burnout, compassion fatigue, and compassion satisfaction among clinical social workers. Journal of Social Service Research, 39(3), 365–379. https://doi.org/10.1080/01488376.2013.771596
- U.S. Department of Health and Human Services. (2017). The AFCARS Report. https://web.archive.org/web/20190810064805/https://www.acf.hhs.gov/sites/default/files/cb/afcarsreport24.pdf
- Whitt-Woosley, A., Sprang, G., & Eslinger, J. (2020). Exploration of factors associated with secondary traumatic stress in foster parents. Children and Youth Services Review, 118, 105361. https://doi.org/10.1016/j.childyouth.2020.105361
- Whitt-Woosley, A., Sprang, G., & Eslinger, J. (2022). The impact of COVID-19 and experiences of secondary traumatic stress and burnout. Psychological Trauma: Theory, Research, Practice, & Policy, 14(3), 507. https://doi.org/10.1037/tra0001183
- Xie, W., Chen, L., Feng, F., Okoli, C. T., Tang, P., Zeng, L., Jin, M., Zhang, Y., & Wang, J. (2021). The prevalence of compassion satisfaction and compassion fatigue among nurses: A systematic review and meta-analysis. International Journal of Nursing Studies, 120, 103973. https://doi.org/10.1016/j.ijnurstu.2021.103973
- Zelechoski, A. D., Sharma, R., Beserra, K., Miguel, J. L., DeMarco, M., & Spinazzola, J. (2013). Traumatized youth in residential treatment settings: Prevalence, clinical presentation, treatment, and policy implications. Journal of Family Violence, 28(7), 639–652. https://doi.org/10.1007/s10896-013-9534-9
- Zerach, G. (2013). Compassion fatigue and compassion satisfaction among residential child care workers: The role of personality resources. Residential Treatment for Children & Youth, 30(1), 72–91. https://doi.org/10.1080/0886571X.2012.761515