

Abstract
Unexpected anti-red blood cell (RBC) alloantibodies are routinely investigated in immunohematology and blood banking since their existence in pregnant women may induce haemolytic disease of the foetus and newborn, and their presence in donors may induce haemolytic transfusion reactions or hyperacute rejection in solid organ transplantation. Unexpected anti-RBC alloantibodies may target antigens of the most blood types excluding the expected antibodies targeting the ABO antigens. Their incidence in humans was originally linked to alloimmunization events such as blood transfusions, transplants, or pregnancies. But later, many findings revealed their existence in pathogenic processes such as malignancies, infections, and autoimmune diseases; and usually (but not always) associated to autoimmune haemolytic anaemia (AIHA). Nevertheless, unexpected anti-RBC autoantibodies are also occasionally found in healthy individuals in the absence of AIHA and with no history of alloimmunization or the associated pathologic processes. Hence, they are generally known as non-clinically significant, are excluded for typification and called “silent red blood cell autoantibodies (SRBCAA)”. This review highlights evidence related to genetic predisposition, molecular mimicry, immune dysregulation, and immune tolerance loss surrounding the existence of anti-RBC antibodies, describing the presence of SRBCAA as possible early witnesses of the development of autoimmune diseases.
Graphical Abstract
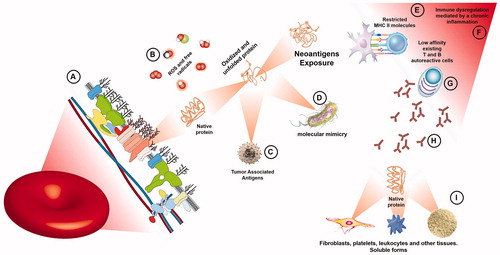
Red blood cells antigens as targets for the loss of immune tolerance. A) Native structures of RBC antigens are membrane-anchored molecules, tough some of them present soluble forms or are also expressed in tissues. B) RBC distribution throughout inflammatory milieus makes them vulnerable targets to structural changes induced by oxidative species and free radicals. C) During malignances, overexpression, mutations, changes in half-lives, misfolding, aberrant degradation and altered post-translational modifications of RBC antigens produce TAA. D) Molecular mimicry between pathogenic microorganisms and RBC antigens, E) the ability to present certain donor RBC antigens restricted by the recipient MHC molecules in genetically predisposed individuals and an immune dysregulation mediated by chronic inflammation are relevant factors likely associated to the activation of F) low-affinity existing autoreactive T and B cells, G) with the subsequent production of SRBCAA. H) Depending on intrinsic properties of the produced anti-RBC autoantibody and the expression of its target molecule; I) SRBCAA detecting RBC antigens expressed in other cells might become pathogenic by producing intravascular or extravascular hemolysis (on RBC), immune complexes (on soluble forms), ITP (on platelets), leukopenia (on leukocytes) or another autoimmune process (e.g. on fibroblasts), and even keep silent until detected by a stochastic event. MHC, Mayor Histocompatibility Complex; ITP (Immune thrombocytopenic purpura), RBC, Red Blood Cells; SRBCAA, Silent Red Blood Cells Auto Antibodies; TAA, Tumor Associated Antigens.
Acknowledgements
The authors thank to MSc. López Díaz PE for valuable discussions and technical assistance.
Disclosure statement
The authors declare that they have no conflict of interest.