
The importance of meticulous arterial preservation in subfertile men is recently highlighted by a randomized controlled study [Citation1]. However, elimination of arterial injury remains a challenge during the procedure of microsurgical subinguinal varicocelectomy (MSV) due to the more difficult dissection with a greater number of internal spermatic arteries and veins at subinguinal level [Citation2]. Currently, micro-Doppler is the most widely adopted adjunct and represents an effective means to locate the testicular artery [Citation3]. However, the technique remains operator dependent, and interpretation requires certain level of experience. More recently, the application of indocyanine green angiography (ICGA) has been reported in the literature [Citation4]. ICGA has demonstrated its capability in provision of objective assessment of testicular artery, and the technique is potentially superior to and provides additional information compared to the current armamentarium [Citation5]. In this issue of the Journal of Investigative Surgery, Dr Kuihara, from Japan, produced an elegant manuscript that presents their experience in testicular artery preservation during MSV by utilizing different adjunctive measures [Citation6].
To our knowledge, this is the first report comparing various adjunctive measures of testicular artery preservation during MSV, namely optical magnification, micro-Doppler, and ICGA. The role of combined use of micro-Doppler and ICGA was also explored. Non-randomized retrospective design, small study population, and lack of reporting of surgical outcomes and follow-up data are some of the obvious pitfalls of the study. Nonetheless, comparative study on efficacy of testicular artery preservation is inherently difficult in view of the presumably low incidence of testicular artery injury during the procedure of MSV [Citation7].
The major finding of the study was the highest number of preserved arteries could be achieved with the complementary use of micro-Doppler and ICGA compared to either technique alone. While the number of arteries preserved with either micro-Doppler or ICGA alone was similar, more arteries were preserved compared to the use of operative microscope alone. The authors proposed that the short arterial phase after a single ICG injection may not be sufficient for securing all the identified arteries. The use of micro-Doppler may overcome the shortcoming and possibly explain the larger number of preserved arteries with the combined use of micro-Doppler and ICGA [Citation6]. However, this is in contrary to our experience in using ICGA during MSV. The technique of ICGA repeatedly demonstrated its ability in clearly identifying small testicular arteries of less than 1 mm diameter. Moreover, small deferential and cremasteric arteries were often visualized clearly in the majority of patients [Citation7]. Although further studies are required to delineate the role of ICGA as an valuable adjunct during MSV, the real-time high-contrast images of ICGA appear promising in identifying small arteries that may be missed by micro-Doppler.
The specific setting of ICG use in the authors’ center may explain the study result and represent a source of bias. It is of note that the procedures of MSV were performed under local anesthesia, and ICG dose was limited to 25 mg [Citation6]. This is in contrast to the common practice of performing MSV under general anesthesia by most andrologists. A stable operative field by eliminating patient movement under general anesthesia facilitates the delicate microsurgical procedure. General anesthesia also offers the microsurgeons with sufficient time which is essential for meticulous arterial preservation. In addition, the low toxicity of ICG implies safety with repeated injections [Citation8]. The short plasma half-life of ICG allows repeated administration without compromising the quality of images on intraoperative ICGA (). Repeated ICGA allows preservation of all testicular arteries which were identified irrespective of the short arterial phase of each ICG injection. ICGA at the end of the procedure also provides objective confirmation of successful arterial preservation. Therefore, the reported results from this study should be interpreted in a confined setting with limited ICG use. The result is possibly different if the operation was performed under general anesthesia with more liberal use of ICG.
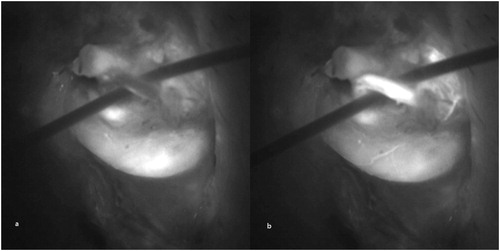
FIGURE 1. Intraoperative indocyanine green angiography was performed after ligation of all internal spermatic veins. (a) Significant quantity of residual indocyanine green signal remained in the field after the previous three angiograms. (b) The strong signal from testicular artery was visualized and clearly differentiated from the background.
In conclusion, the use of adjuncts for arterial identification increases the number of preserved arteries and is probably valuable to the procedure of MSV. While the use of micro-Doppler has been more clearly defined, the role of ICGA remains less clear. Despite its promising initial results, the value of ICGA requires further supporting evidence particularly in the setting of its optimized use. The combined use of adjunctive measures is controversial and should be adopted only after justification of its cost-effectiveness.
Declaration of Interests
The author has no competing interests to declare.
References
- Almekaty K, Zahran MH, Zoeir A, Minhas S, Salem K. The role of artery-preserving varicocelectomy in subfertile men with severe oligozoospermia: a randomized controlled study. Andrology. 2019. [Epub ahead of print]
- Hopps C, Lemer M, Schlegel P, Goldstein M. Intraoperative varicocele anatomy: a microscopic study of the inguinal versus subinguinal approach. J Urol. 2003;170(6):2366–2370. doi:10.1097/01.ju.0000097400.67715.f8.
- Cocuzza M, Pagani R, Coelho R, Srougi M, Hallak J. The systematic use of intraoperative vascular Doppler ultrasound during microsurgical subinguinal varicocelectomy improves precise identification and preservation of testicular blood supply. Fertil Steril.2010;93(7):2396–2399. doi:10.1016/j.fertnstert.2009.01.088.
- Shibata Y, Kurihara S, Arai S, Kato H, Suzuki T, Miyazawa Y. Efficacy of indocyanine green angiography on microsurgical subinguinal varicocelectomy. J Invest Surg. 2016;13:1–5.
- Cho CL, Ho KL, Chan WK, Chu RW, Law IC. Use of indocyanine green angiography in microsurgical subinguinal varicocelectomy - lessons learned from our initial experience. Int Braz J Urol. 2017;43(5):974–979. doi:10.1590/s1677-5538.ibju.2017.0107.
- Kuihara S, Shibata Y, Arai S, et al. Improved arterial preservation achieved by combined use of indocyanine green angiography and Doppler detector during microsurgical subinguinal varicocelectomy. J Invest Surg. in press.
- Chan PT, Wright EJ, Goldstein M. Incidence and postoperative outcomes of accidental ligation of the testicular artery during microsurgical varicocelectomy. J Urol. 2005;173(2):482–484. doi:10.1097/01.ju.0000148942.61914.2e.
- Hope-Ross M, Yannuzzi LA, Gragoudas ES, et al. Adverse reactions due to indocyanine green. Ophthalmology. 1994;101(3):529–533.