
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
This study sought to identify subpopulations of caregivers of older persons based on their profiles of individual characteristics and caregiving contexts and aimed at examining the associations between caregiver profiles and elder mistreatment. A convenient sample of 600 adult caregivers of community-dwelling older people in Hong Kong participated. Results of latent profile analysis support a typology of 3 distinctive caregiver profiles: (a) non-vulnerable caregivers; (b) isolated, vulnerable caregivers; and (c) traumatized, vulnerable caregivers. Isolated and traumatized caregivers reported greater risk factors related to elder mistreatment: They had higher levels of caregiver stress and burden, lower levels of social support and resilience, greater neurotic personality orientation and problematic gambling behavior, and more severe childhood traumatic experiences. The two groups also display significantly higher level of abusive behaviors than non-vulnerable caregivers.
Elder mistreatment is a severe global health problem that urgently requires the attention of all stakeholders and the public. Reports from international organizations, such as the World Health Organization (WHO) and the United Nations (UN), have prominently underlined the seriousness of the issue and the severity of its consequences (e.g., UN, Citation2015; WHO, Citation2015). Differences in the conceptualization and operationalization of elder mistreatment may highlight the complexity and multidimensionality of the phenomenon: Victims, perpetrators, and contexts can vary to a great extent (Santo et al., Citation2019). Regardless of the characterization and description employed, there has been a general consensus that elder mistreatment needs to be addressed in a timely manner (WHO, Citation2015). As found in a meta-analytical study (Ho et al., Citation2017), the pooled prevalence of elder mistreatment was 10% (95% confidence interval: 5%–19%) in population-based research, and 34% (95% confidence interval: 23%–48%) in third party- or proxy-reported studies across countries.
With the unprecedented pace of population aging, older adults in Asian countries have been a research focus over the past decades. There have been substantial studies conducted on elder mistreatment in the Asian context, especially among the Chinese, Korean, and Japanese populations of which the life expectancy is generally high (Yan et al., Citation2015). A recent review on 49 articles has observed considerable variations in prevalence of elder mistreatment across Asian countries, with figures ranging from 0.2% to 62% for overall mistreatment (Yan et al., Citation2015). Psychological abuse, verbal abuse, and neglect are the most commonly reported among community-dwelling older adults, whilst physical abuse and financial exploitation are more frequently observed in clinical samples.
Elder mistreatment in the caregiving context
Elder mistreatment can occur within and/or outside a caregiving context, but it is generally regarded as different from interpersonal violence unrelated to close relationships (WHO, Citation2015). Existing research has revealed that many elder mistreatment incidents happen within the informal caregiving setting where family caregivers are perpetrators (National Council of Aging, Citation2015). Family caregivers are self-identified individuals who provide informal or unpaid care for older people who are typically their spouse, parent, grandparent, or sibling (Kasper et al., Citation2015; U.S. Department of Health and Human Services, Citation2014). Informal caregiving encompasses a wide range of daily activities and supports to help an older person with limited self-care capacity (Colello, Citation2008). Caregivers may provide assistance with activities of daily living (such as bathing, eating, dressing, and walking). They may also assist their care recipient in achieving an independent life (such as preparing meals, doing laundry, and arranging medications for them). Despite the possibility of having positive and rewarding aspects of caregiving (Quinn & Toms, Citation2019), existing evidence points to the fact that family caregivers of older persons frequently experience a certain level of stress and burden (Hunt, Citation2003). Caregiver burden, which refers to the negative reaction to the influence of providing care on caregivers’ personal and social roles (Given et al., Citation1999; Liu et al., Citation2020), can be multidimensional: It can be related to physical, emotional, social, and financial stress. For example, objective burden may arise from the changes in household and work routine, family relationship, physical health, and leisure time; whilst subjective burden is the mental distress resulted from those changes (Reine et al., Citation2003). Chronic exposure to stress and burden in caregivers has been demonstrated to be associated with declining quality of life, deteriorated physical health, and increased psychiatric morbidity (Mahoney et al., Citation2005), which may in turn lead to a poorer quality of caregiving and even a heightened risk of elder mistreatment (Given et al., Citation1999).
In Asian societies, where filial piety is the fundamental social norm that guides family relationships, caregiver burden may be particularly great as taking care of older parents is often viewed as the primary responsibility of adult children (Yan et al., Citation2015). Adult children from Asia fear the social stigmatization of being branded as “abandoning parents” if they place their parents into an elderly home (Zhang et al., Citation2014); thus, they may need to take up the responsibility regardless of their own circumstances and difficulties. It can be expected that proximate intergenerational contact may give rise to family conflicts, due to the differences between generations in terms of role expectations, lifestyle, and social and financial activities (Arai, Citation2006). Over time, the initial satisfying caregiving experiences may become routine and impose stress and strain on the caregivers, leading to greater risks of elder mistreatment (Isac et al., Citation2021). In addition to the increasing burden and exhaustion, the intergenerational gaps in expectations on filial responsibilities resulted from modernization and westernization in recent decades. For example, younger generations in Hong Kong tend to view filial piety as repayment based on mutual affection instead of absolute obedience or a responsibility to provide direct care (Yan & Fang, Citation2017). Raised in Asian cultural tradition, older parents may view this as inadequate emotional attention, and it is unacceptable for adult children to violate the core cultural values by failing to provide sufficient support and care (Gao et al., Citation2019). As a result, intergenerational conflicts may arise, imposing older adults to greater risks of being mistreated.
Current theories of caregiver mistreatment
Concerning the specific context of family caregiving, the stress process model has frequently been applied to examine elder mistreatment. As highlighted in the previous section, informal caregivers are prone to long-term stress and burden in fulfilling their caregiving role (Hunt, Citation2003). The stress process model proposes that primary stressors, such as poor physical and cognitive functioning among care recipients, emerge directly from the caregiving situation (Pearlin et al., Citation1990); and the negative health consequences of exposure to stressors can be amplified by socioeconomic disadvantages through a compound of adversity (Aneshensel et al., Citation2016). Levels of stress or burden primarily depend on the levels of care demands and resources perceived by caregivers, and personal and social resources can intervene at multiple points along the stress process. Social support and the self-concept are two typical protective factors that have been demonstrated to mediate or moderate the negative impact of stressors (McLeod, Citation2012).
Although caregiver burden has often been suggested to be a significant risk factor for elder mistreatment in the literature (e.g., Given et al., Citation1999; Yan & Kwok, Citation2011), it is not feasible to use one single theory to account for all forms of elder mistreatment in the caregiving context. In fact, research-testing hypotheses generated by different theories on elder mistreatment have yielded mixed results, reflecting a possibly limited explanation power of any single theory. While some research on the caregiver stress theory has suggested that a greater burden perceived by caregivers is related to an increased risk of elder mistreatment perpetration (Garre-Olmo et al., Citation2009); others have demonstrated that caregiver burden should not be considered the sole cause of the phenomenon (Acierno et al., Citation2010; Fisher & Regan, Citation2006).
Social exchange theory takes into account the interactions and dependency between the caregiver and the victim. Elder mistreatment is expected in unbalanced relationships but not in balanced ones (Fundinho et al., Citation2021). When care recipients have increased needs and limited resources to provide, they will become dependent on their caregivers. In turn, caregivers may gain power over the relationship and manipulate the exchanges to maximize benefits or to vent negative emotions. In the caregiving context, manipulation of exchanges may take the form of taking monetary compensation (financial exploitation), denying necessary exchange (neglect), and inflicting pain or distress (physical and psychological abuse). To date, findings on social exchange theory in explaining elder mistreatment have been mixed. Most have portrayed elder victims as being dependent on abusers (Bergeron, Citation2001); whereas others have revealed perpetrators’ financial and emotional dependence on elder victims (Lachs & Pillemer, Citation2004; Lundy & Grossman, Citation2004).
Another major theory of elder mistreatment is social learning theory, which is also known as intergenerational transmission of violence and the cycle of violence theory. This theory states that children exposed to family violence are likely to internalize violent behavior as acceptable and use them during adulthood (Pillemer & Wolf, Citation1986). When child victims grow up and become caregivers of their parents, they may use violence as a way to resolve problems arising from caregiving. Like social exchange theory, studies testing the social learning theory hypotheses have also yielded contradictory results. On the one hand, some have shown that individuals exposed to family violence during childhood could be more likely to engage Corcoran (Citation2011) in elder mistreatment (Franklin & Kercher, Citation2012); on the other hand, a systematic review of 47 studies has described mixed support for the association between childhood traumatic experiences and subsequent family violence during adulthood (Thornberry et al., Citation2012).
Other theoriesin particular, the one focusing on psychopathology and intra-individual dynamics among perpetrators, have emphasized perpetrator characteristics as the primary cause of elder mistreatment. The caregiver psychopathology theory proposes that abusive caregivers are suffering from some mental health problems that hamper their ability to provide sufficient care or even make them prone to violence (Fulmer et al., Citation2004). Apart from mental health issues, such as depression and anxiety disorder, certain personality traits as well as alcohol or substance dependence can be closely related to the use of violent behavior against older persons (Choi & Mayer, Citation2000; Fang et al., Citation2021; WHO, Citation2006). Research has shown that caregivers high in neuroticism are prone to frustration and compulsive buying, posing them with a higher risk of neglect or financially exploit their care recipient (Fang et al., Citation2019).
Typological analysis of caregivers
While caregiving is often perceived as a burden, not all stressed caregivers mistreat their elder care recipients. Thus, looking for typologies or groupings of caregivers may prove to be fruitful for professionals or stakeholders to understand what leads to violence and what protects individuals from victimization. Typological analysis is the grouping of cases or individuals on the basis of shared characteristics or background in order to serve different purposes, including concept building and refinement, case sorting, assessment development, case investigation, decision informing, and treatment or intervention planning (Burgess et al., Citation2007; Colier et al., Citation2012). There are various published descriptions of typologies concerning caregiving styles or caregivers of individuals with specific health conditions. Using a narrative qualitative analysis, Corcoran (Citation2011) has put forth a typology of four dementia family caregiving styles. The four styles, which include the “facilitating” style, the “balancing” style, the “advocating” style, and the “directing” style, are distinct from each other by the intended focus of care and the communications and interactions with the care recipients. With a similar approach, Davis et al. (Citation2014) have proposed a typology of three spouse caregivers of older persons with Alzheimer’s or Parkinson’s disease: “adapters,” “strugglers,” and “case managers.” The authors then suggested that caregiver burden might be more influenced by caregivers’ management styles than the actual demand of the care situation. Other narrative research using small samples (N = 9–23) have also identified different subgroups of caregivers based on caregivers’ levels of subjective burden, motivation of caregiving, expressed emotions, caregiving complexity, and resource availability. For example, Gehr et al. (Citation2021) have identified three types of caregiving spouses of geriatric patients without dementia: the “caring partner,” the “worried manager,” and the “desperate overburdened;” whilst Pepin et al. (Citation2013) have suggested five categories of caregivers: “high-distress,” “resourceful but at-risk,” “non-committal,” “high-functioning but static,” and “model caregivers.”
Noting the potential weaknesses of narrative research, recent studies on caregiver typologies have made attempts to identify subgroups of caregivers using cluster analyses or latent class analyses (LCA). Pristavec and Pruchno (Citation2019) have proposed a typology of five caregiving experiences based on caregivers’ primary stressors, primary appraisal in caregiving tasks, and socio-demographic background. The five types of caregivers include (a) the “intensive caregivers,” with high burden and moderate benefits; (b) the “balanced caregivers,” with moderate burden and high benefits; (c) the “dissatisfied caregivers,” with high burden and no benefits; (d) the “relationship caregivers,” with interpersonal burden and benefits; and (e) the “satisfied caregivers,” with no burden and high benefits. In contrast, in one of the first quantitative studies on the classification of elder mistreatment perpetrators, DeLiema et al. (Citation2018) have identified four other subgroups of perpetrators, namely the “caregiver,” the “temperamental,” the “dependent caregiver,” and the “dangerous,” in a sample of 336 victims or caseworker reports. The four subgroups were distinctive in their levels of aggression, financial dependency, irresponsibility, alcohol and substance use, emotional strain, and supportive behavior. Among all subgroups, “caregivers,” who exhibited the fewest negative behaviors and provided the greatest support were more likely to neglect their elder care recipients; whilst “dependent caregivers,” who were dependent on care recipient for money, were more likely to use financial abuse. The findings have shed light on the possibility of different patterns of elder mistreatment perpetration among different subtypes of caregivers and have warranted the need for future studies on the typology of elder mistreatment perpetrators in the caregiving context.
The present study
Although the diversity among caregiver characteristics and their risks of elder mistreatment has long been noted in the literature, relatively few studies have sought to identify specific caregiver profiles and their associations with different types of elder mistreatment. In this study, we aimed at filling the research gap by exploring the subgroups of caregivers of older people based on the risk and protective factors related to elder mistreatment. We also aimed to extend the use of typologies from sorting cases based only on the demographic background to providing preliminary insights on tailoring prevention and interventions for caregivers who were at risk of perpetrating elder mistreatment by including a series of variables in the classification model. Unlike past research having small sample size (e.g., fewer than 100) or using narrative approach to categorize caregivers, this study employed the latent profile analysis (LPA) to classify subgroups of caregivers by identifying latent profiles covering a wide range of risk and protective factors of elder mistreatment.
Based on existing theories on elder mistreatment in the caregiving context, this study included four aspects of key variables in the typological analysis, putting a special emphasis on the risk factors and protective factors related to elder mistreatment perpetration:
Caregiver stress and burden. According to the caregiver stress theory, the burden perceived by caregivers when fulfilling their caregiving role could increase the risk of elder mistreatment (Garre-Olmo et al., Citation2009; Pickering et al., Citation2018). Additionally, agitated behaviors exhibited by the care recipients were also considered a significant stressor that would increase caregivers’ risk of elder mistreatment (Yan, Citation2014).
Social support and resilience. The stress process theory suggests that protective factors such as personal resources, positive self-concepts, and social support may serve as buffers to the negative impact of stress (Ice, Sadruddin, Vagedes, Yogo, & Juma, 2012; Pearlin et al., Citation1990). As another protective factor, resilience has been demonstrated with significant buffering effects on the caregiver stress on elder mistreatment (Serra et al., Citation2018; Yan, Citation2020).
Neurotic personality and problematic health behavior. The caregiver psychopathology theory assumes that caregivers’ mental health problems are linked to greater risks of elder mistreatment. Caregivers with substance use problems are likely to be dependent on care recipients and have been shown to be more likely to use violent behavior against others (WHO, 2006). Caregiver neuroticism, among other major personality traits, has been consistently demonstrated as a risk factor that might lead to greater physical and psychological elder mistreatment (Fang et al., Citation2021; Li et al., Citation2020).
Childhood traumatic experiences. On the basis of the social learning theory, childhood traumatic experiencesin particular, the experiences of being abused by parents or other family members, is often suggested to transmit between generations, forming a “cycle of violence” that the child victim would result in perpetration of violence during childhood (Franklin & Kercher, Citation2012; Widom & Wilson, Citation2015).
It was hypothesized that (a) caregivers could be grouped into distinctive subgroups based on their profiles of risk and protective factors related to elder mistreatment; and (b) subgroups of caregivers would report significantly different patterns and/or severity of elder mistreatment toward elder care recipients.
Methods
Participants and sampling procedures
This study used a cross-sectional survey to explore the typology of family caregivers of older people in Hong Kong. Data were collected in 2017, and the target participants were family caregivers providing care to community-dwelling individuals aged 60 years or above. Family caregivers were defined as family members providing at least 10 hours of informal care per week in aspects including personal care needs (e.g., bathing, dressing, etc.) and activities necessary for independent living (e.g., meal preparation, shopping, etc.). All family caregivers who were 18 years of age or older, residing in Hong Kong during the study period, and providing at least 10 hours of care to an older family member were eligible to participate. On the other hand, paid or formal caregivers, such as domestic helpers and home support workers, were excluded from this study.
Caregivers were recruited from the local Neighbourhood Elderly Centres (NEC) and District Elderly Community Centers (DECC), which are government-funded organizations providing supportive services for older adults and their caregivers. To meet the criteria to be a minimum sample for the LPA analysis (Finch & Bronk, Citation2011; Peugh & Fan, Citation2015), our target sample size was 600. Invitations were sent to all 168 NECs and 41 DECCs in Hong Kong. Staff members of the participating NECs and DECCs were explained thoroughly by the research team about the study purpose and scope and were encouraged to refer family caregivers to participate in this study. Caregivers were chosen by the staff at the invited centers with the inclusion and exclusion criteria determined by the research team. Eligible participants were then contacted for a face-to-face interview with research assistants under close supervision of the research team. The research assistants, who held either a degree in counseling or gerontology, were trained in aspects related to elder mistreatment and crisis management. Interviews, which took approximately 30 to 40 minutes to complete, were conducted in a quiet corner at the NEC or DECC with the guidance of a research protocol and a structured questionnaire. Before the start of the interview, eligible caregivers were asked to provide written consent. They were reassured that they had the right to omit any question or terminate the interview without any effect on the services they were receiving. Upon the completion of the interview, each caregiver participant received a monetary incentive of HKD $100 (~ USD $12). Research ethical approval for this study was obtained from the institutional review board of the authors’ affiliated university.
Measures
Elder mistreatment
Elder mistreatment by caregivers was measured in six aspects, including verbal abuse, physical abuse, injury, potentially harmful behavior, financial exploitation, and neglect. The first three aspects were measured using the 8-item Verbal Aggression, 11-item Physical Assault, and 6-item Injury subscales of the Revised Conflict Tactics Scale, respectively (CTS-2, Straus et al., Citation1996). Potentially harmful behavior by caregivers was assessed with the 10-item instrument modified from the Conflict Tactics Scale (CTS), which listed different behaviors that caregivers employed when care recipients did not follow their instructions (Macneil et al., Citation2010). Financial exploitation was assessed using 14 items adapted from the Older Adult Financial Exploitation Measure (Conrad et al., Citation2009), and neglect was measured using the 20-item Unmet Needs Assessments (Katz, Citation1983). All items assessing elder mistreatment were rated by caregivers on a 7-point Likert scale according to how often they performed against the care recipient. Item scores ranged from 0 (never) to 6 (always). Mean scores were used to indicate the extent to which caregivers abused the care recipient, with a higher score reflecting more severe mistreatment.
Agitated behavior by care recipients
Agitated behavior of care recipients was assessed using the Cohen-Mansfield Agitation Inventory (CMAI; Cohen-Mansfield et al., Citation1989). The 29-item CMAI was originally developed to measure the types and frequencies of agitated behaviors exhibited by older adults living in nursing homes. Caregivers were asked to rate their care recipients’ behavior, as a proxy, on a 7-point Likert scale ranging from 1 (never engages in) to 7 (manifests the behavior on an average of several times an hour). Item scores were summed to give a scale score (from 29 to 116); the higher the score, the greater the degree of agitation of the care recipient.
Caregiver burden
Caregivers’ perceived caregiver burden was assessed using the 22-item Zarit Burden Interview (ZBI, Zarit et al., Citation1985), which was designed to measure stresses experienced by family caregivers of older adults. Items were rated on a 5-point Likert scale from 0 (never) to 4 (nearly always), giving a scale score between 0 and 88. Higher scores indicate a greater burden perceived by the caregiver.
Social support
Caregivers’ informal support was assessed using a 15-item scale measuring emotional support (seven items) and instrumental support (eight items) (Wills, Citation1985). Caregivers rated the extent to which they received specific types of support on a 5-point Likert scale. Item scores were summed to give two subscale scores, namely emotional social support and instrumental social support, with higher scores indicating higher levels of informal support perceived by the caregivers.
Resilience
Caregiver resilience was assessed using the 10-item Connor Davidson Resilience Scale (CDRS, Connor & Davidson, Citation2003). Items were rated on a 5-point Likert scale from 0 (not true at all) to 4 (true nearly all of the time). Item scores were summed to give a scale score, and higher scores reflected a greater level of resilience.
Neurotic personality
Caregiver neurotic personality orientation was measured using the 12-item Neuroticism subscale of the NEO Five Factor Inventory (NEO-FFI, Costa & McCrae, Citation1992). Caregivers rated the degree to which they agreed with the statement on each item on a 5-point Likert scale ranging from 0 (strongly disagree) to 4 (strongly agree). A higher score indicated a higher level of neurotic personality of the caregiver.
Problematic gambling behavior
Caregiver gambling behaviors were assessed using the 20-item South Oaks Gambling Screen (SOGS, Lesieur & Blume, Citation1987). Each item was scored 0 or 1 according to the caregiver’s response. Item scores were summed to give a scale score from 0 to 20, with a higher score reflecting a greater degree of problematic gambling.
Childhood traumatic experiences
Caregivers’ experiences of abuse during childhood (i.e., before the age of 18) were measured using the Childhood Trauma Questionnaire-Short Form (CTQ-SF; Bernstein et al., Citation2003), which contains five subscales measuring three forms of abuse (emotional, physical, sexual) and two forms of neglect (emotional, physical). Each subscale contains five items to be rated on a 5-point Likert scale ranging from 1 (never true) to 5 (very often true). Item scores were summed to give subscale scores (from 5 to 25); higher scores indicated more childhood traumatic experiences.
Demographic background
Demographic characteristics of the caregivers and their care recipients were recorded. In this study, caregiver background included gender, age, highest education attainment, employment status, marital status, and family income. They were also asked to report whether they had any chronic health conditions, whether they needed long-term medications, and whether they had received any formal training in dementia care. In addition, caregivers were asked to provide basic information about the care recipient, including gender, age, mental health condition, chronic health condition, and long-term medication. Caregivers were also asked to rate their own health status and care recipients’ health status on an 11-point Likert scale, with higher scores indicating better health perceived by the caregivers.
Caregiving context
Variables including caregiver’s relationship with the care recipient, number of days co-residing with the care recipient per month, number of hours of care provided per week, number of fellow residents in the household, and the availability of domestic helpers to assist caregiving were recorded to give information about the caregiving context.
Data analysis
In order to identify distinguishable caregiver profiles, LPA was conducted using Mplus 8 (L. K. Muthén & Muthén, Citation2017), facilitated by the R package MplusAutomation (Hallquist & Wiley, Citation2018). LPA is a categorical latent variable modeling approach that helps identify latent subgroups within a population with a set of variables. It is based on the assumption that individuals can be typed or grouped into categories (subgroups) that bear different profiles of personal or environmental attributes (Collins & Lanza, Citation2013; Spurk et al., Citation2020). In this study, we used the 6-step approach proposed by Ferguson et al. (Citation2020) to perform LPA. The six steps included data inspection, iterative model evaluation, model fit and interpretability evaluation, profile patterns investigation, covariate analysis, and result presentation. In search of the best solution, a series of models was generated using stepwise addition procedures (Nylund-Gibson et al., Citation2019). Models were then compared on the basis of relevant statistical criteria including model fit statistics (e.g., log-likelihood, Bayesian information criterion, consistent Akaike information criterion, etc.), likelihood tests (e.g., Vuong-Lo-Mendell-Rubin adjusted likelihood ratio, bootstrapped likelihood ratio test, etc.), and diagnostic statistics (e.g., entropy). Low values of model-fit statistics, statistical significance in likelihood tests, and an entropy value greater than .80 indicated model fit (Weden & Zabin, Citation2005). In addition to these criteria, the class size of each profile in the models was also examined to ensure that it would be larger than 50 (B. O. Muthén & Muthén, Citation2000), or 5% of the total sample (Shanahan et al., Citation2013).
Indicators including agitated behavior exhibited by care recipients, caregiver burden, social support, resilience, neurotic personality, problematic gambling behavior, and childhood traumatic experiences were used to estimate latent profiles.
We then further conducted a distal outcome analysis, using the ML three-step approach (Bakk & Vermunt, Citation2016), to explore how variables differ across latent profiles and which profile(s) would predict different types of elder mistreatment (the distal outcomes). In the three-step approach, a model with various latent profiles was first built without the distal outcomes. The class memberships were then determined, and the associations between the class memberships and the distal outcomes were investigated in the final step. Demographic variables and caregiving contexts (including the gender and age of caregivers and their care recipients, the relationship between caregivers and care recipients, the presence of domestic helper, and the number of days of co-residence) were controlled.
In this study, missing data were handled by full information maximum likelihood (FIML) in Mplus. Robust estimators (MLR) were used to deal with non-normal data.
Results
Demographic background and caregiving context
A convenience quota sample of 600 family caregivers successfully completed the survey in this study. The mean age of the caregivers was 71.04 years (SD = 10.59). About 67.4% of the caregivers were female, 87.5% were married, 62.1% were retired, and 59.9% received secondary education or above. More than half of them had chronic health conditions (53.7%), or needed long-term medications (54.7%). A majority of the caregivers (70.4%) reported family income less than HKD $10,000 (~USD $1270) per month. Demographic backgound of family caregivers is presented in Appendix A.
Concerning the care recipients, male comprised 53.8% of the sample, and the mean age was 78.71 years (SD = 8.46). Approximately 78.7% had chronic health conditions, and 79.0% needed long-term medications. Most care recipients did not have any cognitive impairment or mental disorder (70.2%). On the other hand, about 12.3% had mild cognitive impairment, 15.8% were diagnosed with dementia, and 1.7% had mental disorders. Demographic backgound of care recipients is presented in Appendix B.
A majority of the caregiver-care recipient dyads were couples (77.9%), followed by older parents/adult children (19.3%) and siblings (2.4%). Caregivers reported that they spent an average of 26.41 days per month (SD = 10.13) living with the care recipients and 17.21 hours per week (SD = 24.57) to provide informal care. Only 6.0% of the caregivers had received formal training in dementia care, and 14.2% had domestic helper to provide assistance in household chores.
Detailed information about the demographic background of caregivers and care recipients as well as the caregiving contexts is presented in Appendices A and B.
Latent profiles of caregivers
Mean scores, standard deviations, and internal consistencies of all variables were summarized in Appendix C.
Model selection
Findings from the LPA indicated three latent subgroups in the caregiver sample. shows the results of model-fit statistics, likelihood tests, and entropy test of six models in the LPA (from 1-profile to 6-profile). Although model-fit indices suggested a 6-profile model, the smallest profile size was too small (n = 3). Similarly, the smallest profile size in the 4-profile model and the 5-profile was not satisfactory (both n = 3). Therefore, these three models were excluded from further analyses. Among the remaining three models, the one with three profiles, which had satisfactory profile sizes and achieved good results in model-fit, likelihood, and entropy tests, was the most plausible.
Table 1. Model fit indices for the latent profile models.
Profile enumeration
Mean scores and standard deviations of the study variables across the three latent subgroups are presented in . Profiles were named according to their risks of perpetrating elder mistreatment estimated based on existing theories. Profile 1, which comprised 61.0% of the sample, described the characteristics of “low-risk caregivers.” In this study, low-risk caregivers reported lower levels of caregiver burden, neurotic personality orientation, problematic gambling, and childhood traumatic experiences, as well as higher levels of social support and resilience than the other two subgroups of caregivers. Profile 2, the “isolated, high-risk caregivers,” comprised 35.5% of the sample. Findings of the Wald’s tests showed that, compared with low-risk caregivers, isolated, high-risk caregivers (thereafter “isolated caregivers”) perceived significantly lower levels of emotional and instrumental support from others and showed lower levels of resilience (all p < .05). They also reported greater levels of agitated behavior by the care recipients, greater caregiver burden, greater orientation to neurotic personality, more problematic gambling behavior, and more severe childhood traumatic experiences than their low-risk counterparts (all p < .05). Profile 3, which consisted of 3.5% of the sample, described the subgroup of “traumatized, high-risk caregivers.” Traumatized, high-risk caregivers (thereafter traumatized caregivers) showed similar risk patterns as isolated caregivers when compared to those low-risk: They had greater caregiver burden, greater neurotic personality orientation, more problematic gambling behavior, more severe childhood traumatic experiences, lower social support, and lower resilience (all p < .05). What differed between the two high-risk subgroups was that traumatized caregivers reported significantly the highest levels of emotional, physical, and sexual abuse by family members during childhood among all caregivers (all p < .05). provides a visual depiction of the three profiles using the z-scores of each measure.
Figure 1. The three profiles of caregivers.
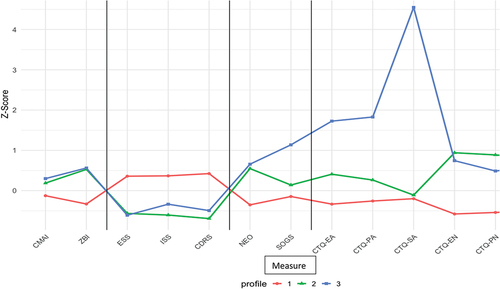
Table 2. Means and Standard Deviations (SD) of study variables across the three profiles.
Covariate analysis
presents the results of a multinomial regression analysis on caregiver and care recipient demographic background. The three subgroups differed significantly in caregiver age and care recipient gender. To be specific, low-risk caregivers and isolated caregivers were significantly older than traumatized caregivers; and care recipients of the former two subgroups were more likely to be male than those taken care by traumatized caregivers (all p < .05). Results from pairwise comparisons also indicated that care recipients of low-risk caregivers were younger and more likely to be the spouse than those taken care by isolated caregivers (all p < .05).
Table 3. Multinomial regression across three profiles, using profile 3 (Traumatised caregivers) as reference.
Distal outcome analysis
summarizes the findings of the distal outcome analysis of the LPA. As expected, the three profiles reported significantly different levels of elder mistreatment. Isolated caregivers in general reported greater levels of verbal abuse, physical abuse, potentially harmful behavior, financial exploitation, and neglect against their care recipients than low-risk caregivers did (all p < .05). Similarly, traumatized caregivers inflicted greater levels of verbal abuse, potentially harmful behavior, and financial exploitation against their care recipients than their low-risk counterparts (all p < .05). When comparing the two subgroups of high-risk caregivers, traumatized caregivers used significantly greater levels of potentially harmful behavior and financial exploitation than isolated caregivers (all p < .05). Finally, the three subgroups did not differ significantly in the injury levels of care recipients (p = .052) .
Figure 2. Latent profiles of caregivers and respective distal outcomes.
Table 4. Means and Standard Deviations (SD) of elder mistreatment against care recipients, the distal outcomes of the latent profile analysis.
Discussion
With the rapid growth of the elder population worldwide, the proportion of older people living at home with care needs will indisputably increase. To support the independent living among these community-dwelling older individuals, informal family caregiving has been expected to be the major source of assistance (Doty et al., Citation2010). The expanding population of older people and their family caregivers has warranted adequate and timely resources to support families in need (Lowenstein, Citation2010). Using a sample of 600 caregivers of community-dwelling older people in Hong Kong, this study is among the first to identify and characterize distinguishable subgroups of family caregivers using risk and protective factors related to elder mistreatment in an LPA model. Three different profiles of family caregivers are identified, and the severity levels of their perpetration of elder mistreatment differ significantly. The findings highlight the heterogeneity among caregiver characteristics and underpin the development of customized family intervention programmes by addressing the specific profile of each caregiver subgroup individually.
Variations across subgroups of caregivers
In line with previous studies on the typologies of caregivers (e.g., Corcoran, Citation2011; Davis et al., Citation2014; Gehr et al., Citation2021; Pepin et al., Citation2013), our findings show that caregiver subgroups might differ from each other with regard to their individual characteristics and caregiving contexts. Current findings provide support to a model of three subgroups, which were named according to their characteristics and their risks of perpetrating elder mistreatment: the low-risk caregivers, the isolated caregivers, and the traumatized caregivers. Low-risk caregivers had the lowest levels of caregiver stress and burden, lowest degrees of neurotic personality orientation, fewest problematic gambling behaviors, and lowest levels of childhood traumatic experiences. They perceived the highest degrees of emotional and instrumental support related to caregiving and exhibited high levels of resilience to caregiver stress. Based on the literature on various theories on caregiver mistreatment (e.g., Franklin & Kercher, Citation2012; Ice et al., Citation2012; Yan, Citation2014), caregivers with this profile were believed to have a relatively low risk of perpetrating elder mistreatment against their care recipient. Indeed, they reported the lowest levels of perpetration across all types of elder mistreatment in this study, reflecting the potential usefulness of the current typology in identifying and classifying healthy caregivers with low risks of elder mistreatment.
Contrasting with the profile of low-risk caregivers, the profiles of the two high-risk subgroups, including the isolated and the traumatized, comprise characteristics that are shared by many high-risk elder mistreatment perpetrators. In line with the caregiver stress theory, high levels of caregiver burden and agitated behavior by care recipients were commonly observed among the caregivers at-risk of perpetrating elder mistreatment. According to the caregiver stress theory, family stressors may lead to family crisis, and the effect of the stressor can be influenced by one’s appraisal of it (McCubbin & Patterson, Citation1983). In the case of caregiving for older persons with behavioral disturbance (i.e., the stressor), caregivers’ appraisal of the stressor or their perceived burden, can affect their likelihood of mistreating their care recipients (Yan & Kwok, Citation2011). When the objective level of agitated behavior by care recipient is high and the subjective burden is great, caregivers may be at high risk of using violence as a means of expressing emotions and resolving problems. Supporting the caregiver psychopathology theory, current findings showed that caregivers’ neurotic personality was one of the significant characteristics observed among high-risk caregivers. Caregiver personality traits have been suggested in recent research as a risk factor of elder mistreatment, and high neuroticism has been linked with increased risks of physical and psychological abuse (Fang et al., Citation2021), as well as greater odds of financial exploitation and neglect (Li et al., Citation2020). Besides, what make the situation even worse may be the low levels of social support perceived by stressed caregivers. Our study has revealed lower levels of social support among caregivers at-risk of elder mistreatment, providing some evidence supporting the stress process theory in explaining caregiver violence. Social isolation has often been linked with an increased risk of family elder mistreatment (e.g., Acierno et al., Citation2009). A study has even revealed that more than one-third of perpetrators did not have anyone to count on or to talk to when they were in need (Jackson & Hafemeister, Citation2011). Together with a low level of resilience, the ability to adapt to stress and an important buffer of the negative impact of caregiver burden on the use of violence (Yan, Citation2020), the risks of elder mistreatment among isolated, stressed caregivers may drastically escalate.
Current findings support a further division of high-risk caregivers into two main subgroups, of which the traumatized group experienced significantly more severe physical, emotional, and sexual abuse than the isolated group during childhood. Although evidence observed by systematic reviews is mixed (e.g., Fundinho et al., Citation2021), childhood traumatic experiences, particularly the experiences of child abuse by parents or other family members, has been suggested in some research as a risk factor of various long-term negative consequences in adulthood, including interpersonal violence, hampered self-esteem, and psychopathology (Mullen et al., Citation1996). Current findings have partly supported the social learning theory in explaining elder mistreatment and indicated an intergenerational transmission of violence, where childhood violence victimization may predict later family violence (Heyman & Slep, Citation2002; Wang et al., Citation2015). According to Bandura’s social learning theory (1973), child abuse survivors may learn abusive behavior in response to conflicts or other stressful situations. The way they view and accept violent behavior may then affect how they interact with others in later stages and may possibly lead to a greater likelihood for them to use violence to resolve interpersonal problems. Concerning the influences on elder mistreatment, research has found that almost half of the elder mistreatment perpetrators had a history of childhood family violence (Jackson & Hafemeister, Citation2011) and that childhood abuse could be one of the strongest predictors of one’s proclivity to elder abuse during adulthood among all other risk factors (Yan & Tang, Citation2003). In the context of family caregiving, Dong’s et al. (Citation2017) has shown that caregivers who had experienced childhood trauma (e.g., being physically abused, threatened, insulted, or screamed at as a child) were more likely to perpetrate caregiver abuse. The authors also noted that, compared with physical childhood abuse, emotional childhood abuse, such as insult and threat, had stronger correlations with caregiver abuse, suggesting a possibility that different types of childhood abuse may have different influences on adulthood violence. Our findings provide support for this claim, and demonstrate that caregivers who experienced severe physical, emotional, and sexual abuse during childhood (i.e., the traumatized caregivers) perpetrated significantly more severe financial exploitation than the others.
The relationship between childhood traumatic experiences and the perpetration of financial exploitation in adulthood may be complex. As suggested in the literature, financial exploitation of older adults can be distinct from other types of elder mistreatment in terms of the perpetration motives and perpetrator and victim profiles (Dominguez et al., Citation2022). Our findings may provide some supportive evidence for the uniqueness of the profiles of perpetrators of financial exploitation: Caregivers who experienced childhood abuse may be at greater risk of financially abusing older parents in adulthood. Based on a literature review, Tueth (Citation2000) has described two types of financial abusers: (a) “passive or opportunistic exploiters” who are psychologically stressed and dysfunctional with low self-esteem and substance dependence problems and (b) “active or predatory exploiters” who actively manipulate vulnerable older persons with threats and intimidation. For childhood trauma survivors who grow up with hampered self-esteem and other psychopathy, they tend to have lower education, poorer socio-economic status, and higher risks of substance use or compulsive buying in adulthood (Khoury et al., Citation2010; Zielinski, Citation2009). Trapped in financial difficulties (Currie & Widom, Citation2010), traumatized caregivers may “passively exploit” their care recipient by being financially dependent on the latter. On the other hand, those who grow up with a distorted appraisal to abusive and violent behavior may end up “actively exploiting” care recipients by seeking vulnerable older people to manipulate using fear and threats. Yet, our findings on the associations between childhood trauma and financial elder mistreatment are preliminary, especially the number of caregivers in the traumatized subgroup was small when compared with the other two groups, and the underlying mechanisms of associations between the two clearly deserve further exploration in the future.
Findings from the multinomial regression analysis show that the three subgroups of caregivers differ in their demographic profiles and caregiving contexts. Low-risk caregivers were primarily older in age, and taking care of their husband at a younger age. Consistent with findings from various systematic reviews (e.g., Pillemer et al., Citation2016; Yan et al., Citation2015), older age and female gender of care recipients can be risk factors for elder mistreatment in the caregiving context. Surprisingly, caregiving contexts such as the presence of domestic helpers to share caregiving responsibilities and the time that caregivers lived with their care recipients, did not differ significantly between subgroups. This finding may shed light on the possibility that living arrangements or co-residence may serve as a protective factor in terms of space (i.e., the size of the living environment, whether all space is shared with care recipients, the presence of private rooms or space for relaxation, etc.) rather than time (i.e., number of days of co-residence).
Implications
The subgroups of caregivers identified in this study provide important empirical evidence to support the presence of and variations of abusive caregiver profiles and shed light on the differences in types of elder mistreatment perpetration between caregivers with different profiles. Our findings suggest that there is a need for customized interventions that address specific caregiver profiles.
Because traumatized caregivers are at the highest risk of mistreating care recipients financially, interventions may focus on managing the financial health of the caregiver/care recipient's dyads. Those who are heavily dependent on the care recipients they are mistreating should be identified at an early stage. To achieve early detection of financial mistreatment by traumatized caregivers, some researchers have suggested the use of “bystander intervention,” which emphasizes the importance of health and banking professionals to make direct observations of the signs of financial exploitation (Gilhooly et al., Citation2016). To assist with such observations, guidelines and protocols that describe the handling procedures when any sign of financial mistreatment is noticed can be developed to educate health and banking professionals. In addition to financial interventions, multi-disciplinary case management may also be effective in combating elder mistreatment among traumatized caregivers. The potential “cycle of violence” should be acknowledged, and it would be crucial to involve services (e.g., counseling and psychiatric services) to handle the negative health behaviors and outcomes among caregivers who survived childhood abuse (Dong et al., Citation2017).
In contrast, interventions for isolated caregivers may target at providing more supporting resources to the families in need. While formal support for caregiving, such as in-home services and subsidies for hiring formal caregivers, should be promoted to cover vulnerable families in order to reduce potential stressors; informal support that reduces perceived social isolation may also be useful to buffer the negative effects of caregiver burden. Findings from systematic reviews have proven that social support interventions with multiple components (e.g., support groups, social network interventions, befriending schemes, etc.) are most beneficial to isolated caregivers (Dam et al., Citation2016). Empirical evidence from longitudinal research has also suggested that social support from close family members or significant others may be the most useful dimension of support for caregivers of older people (Drentea et al., Citation2006). Receiving emotional support from close ones can help caregivers expand their care ability to cope with changes related to caregiving. With regard to this, professionals may consider putting an emphasis on the promotion of informal support and social connections from significant ones when developing caregiver interventions in the future.
Limitations
This study has several limitations. The first is concerned with the use of convenience sampling. Caregivers were recruited from local elderly community centers by referral, and the final sample might be disproportionate to healthy and capable caregivers. Caregivers who are less easy to communicate with might be excluded from the recruitment procedures. Besides, the convenience quota samples were recruited in Hong Kong only. All caregiver participants were Cantonese-speaking Chinese. These inevitably limit the extent to which current findings can be generalized to other populations. Also, related to selection bias is that the proportion of care recipients with dementia is relatively low in this study, and the profile of caregivers of dementia may require further studies. Furthermore, the selection of variables for creating caregiver profiles was not exhaustive. Other factors such as self-esteem, coping skills, violence appraisal, and the number of individuals they are taking care of may also have great influences on caregiver mistreatment. Another limitation exists in the self-report of elder mistreatment perpetration through face-to-face interviews. Social desirability may appear, and abusive caregivers may be reluctant to report their use of violent behavior against older people due to the fear of criminal consequence. The small number of caregivers (n = 21) in profile 3 (i.e., the traumatized caregivers) may be an issue. The low frequency might be due to the relatively small sample size in our study. Future research may consider recruiting a larger sample using a random sampling procedure. The nature of LPA that gives all factors the same weight in elder mistreatment vulnerability can be another problem. It has been suggested in the literature that some factors may have a greater impact on elder mistreatment than others. Unfortunately, it was not possible to give different weights on different factors in creating the caregiver profiles in this study. Finally, the retrospective nature of this study may lead to recall biases in the responses made by caregivers. Recall bias might be especially serious in items probing childhood traumatic experiences in a sample of caregivers with a mean age of 71 years. The accuracy of their responses about experiences several decades ago could be questionable.
Conclusion
This study addresses an important gap in the literature by developing a typology of caregivers according to individual characteristics related to their risk and protective factors related to elder mistreatment perpetration. Using a sample of 600 caregivers of community-dwelling older people, caregivers were classified into three subgroups. The three subgroups of caregivers are distinct from each other with regard to their levels of caregiver stress and burden, social support, resilience, neurotic personality, gambling behavior, and childhood traumatic experiences. Using different caregiver profiles, the subgroups report different patterns of elder mistreatment. The findings provide valuable insights on the importance of early identification of caregiver types, and the development of empirically based interventions tailored for specific groups to combat elder mistreatment by caregivers.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study is available from the corresponding author, Elsie Yan, upon reasonable request.
Additional information
Funding
References
- Acierno, R., Hernandez, M., Amstader, A., Resnick, H., Steve, K., Muzzy, W., & Kilpatrick, D. (2010). Prevalence and correlates of emotional, physical, sexual, and financial abuse and potential neglect in the United States: The national elder mistreatment study. American Journal of Public Health, 100(2), 292–297. https://doi.org/10.2105/AJPH.2009.163089
- Acierno, R., Hernandez, M. A., Muzzy, W., & Steve, K. (2009). National elder mistreatment study. Retrieved from https://www.ncjrs.gov/pdffiles1/nij/grants/226456.pdf
- Aneshensel, C. S., Harig, F., & Wight, R. G. (2016). Aging, neighborhoods, and the built environment. In L. K. George & K. F. Ferraro (Eds.), Handbook of aging and the social sciences (pp. 315–335). Academic Press.
- Arai, M. (2006). Elder Abuse in Japan. Educational Gerontology, 32(1), 13–23. https://doi.org/10.1080/03601270500338567
- Bakk, Z., & Vermunt, J. K. (2016). Robustness of stepwise latent class modeling with continuous distal outcomes. Structural Equation Modeling, 23(1), 20–31. https://doi.org/10.1080/10705511.2014.955104
- Bergeron, L. R. (2001). An elder abuse case study: Caregiver stress of domestic violence? You decide. Journal of Gerontological Social Work, 34(4), 47–63. https://doi.org/10.1300/J083v34n04_05
- Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., Stokes, J., Handelsman, L., Medrano, M., Desmond, D., & Zule, W. (2003). Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse & Neglect, 27(2), 169–190. https://doi.org/10.1016/S0145-2134(02)00541-0
- Burgess, A. W., Commons, M. L., Safarik, M. E., Looper, R. R., & Ross, S. N. (2007). Sex offenders of the elderly: Classification by motive, typology, and predctors of severity of crime. Aggression and Violent Behavior, 12(5), 582–597. https://doi.org/10.1016/j.avb.2007.02.006
- Choi, N. G., & Mayer, J. (2000). Elder abuse, neglect, and exploitation: Risk factors and prevention strategies. Journal of Gerontological Social Work, 33(2), 5–25. https://doi.org/10.1300/J083v33n02_02
- Cohen-Mansfield, J., Marx, M., & Rosenthal, A. (1989). A description of agitation in a nursing home. Journals of Gerontology, 44(3), M77–84. https://doi.org/10.1093/geronj/44.3.M77
- Colello, K. J. (2008). Family caregiving to the older population: Background, federal programs, and issues for Congress. https://www.everycrsreport.com/files/20081024_RL34123_efcb25ce168e5ff3c57f92d159e07dd0b19f0bf6.pdf
- Colier, D., LaPorte, J., & Seawright, J. (2012). Putting typologies to work: Concept formation, measurement, and analytic rigor. Political Research Quarterly, 65(1), 217–232. https://doi.org/10.1177/1065912912437162
- Collins, L. M., & Lanza, S. T. (2013). Latent class and latent transition analysis: With applications in the social, behavioral, and health sciences. John Wiley & Sons, Inc.
- Connor, K. M., & Davidson, J. R. T. (2003). Development of a new resilience scale: The Connor-Davidson Resilience Scale (CDRISC). Depression and Anxiety, 18(2), 76–82. https://doi.org/10.1002/da.10113
- Conrad, K., Madelyn, I., & Ridings, J. (2009). Conceptualization and measuring financial exploitation and psychological abuse of elderly individuals. In Report to the national institute of justice, project #2006–MU–MU–0004 National Institute of Justice.
- Corcoran, M. A. (2011). Caregiving styles: A cognitive and behavioral typology associated with dementia family caregiving. The Gerontologist, 51(4), 463–472.
- Costa, P. T., & McCrae, R. R. (1992). Normal personality assessment in clinical practice: The NEO personality inventory. Psychological Assesssment, 4(1), 5–13. https://doi.org/10.1037/1040-3590.4.1.5
- Currie, J., & Widom, C. S. (2010). Long-term consequences of child abuse and neglect on adult economic well-being. Child Maltreatment, 15(2), 111–120. https://doi.org/10.1177/1077559509355316
- Dam, A. E. H., de Vugt, M. E., Klinkenberg, I. P. M., Verhey, F. R. J., & van Boxtel, M. P. J. (2016). A systematic review of social support internvetions for caregivers of people with dementia: Are they doing what they promise? Maturitas, 85, 117–130. https://doi.org/10.1016/j.maturitas.2015.12.008
- Davis, L. L., Chestnut, D., Molloy, M., Deshefy-Longhi, T., Shim, B., & Gilliss, C. L. (2014). Adapters, strugglers, and case managers: A typology of spouse caregivers. Qualitative Health Research, 24(11), 1492–1500. https://doi.org/10.1177/1049732314548879
- DeLiema, M., Yonashiro-Cho, J., Gassoumis, Z. D., Yon, Y., & Conrad, K. J. (2018). Using latent class analysis to identify profiles of elder abuse perpetrators. The Journals of Gerontology: Series B, Psychological Sciences and Social Sciences, 73(5), e49–58. https://doi.org/10.1093/geronb/gbx023
- Dominguez, S. F., Ozguler, B., Storey, J. E., & Rogers, M. (2022). Elder abuse vulnerability and risk factors: Is financial abuse different from other subtypes? Journal of Applied Gerontology, 41(4), 928–939. https://doi.org/10.1177/07334648211036402
- Dong, X., Li, G., & Simon, M. A. (2017). The association between childhood abuse and elder abuse among Chinese adult children in the United States. The Journals of Gerontology: Series A, Biological Sciences and Medical Sciences, 72(suppl_1), S69–75. https://doi.org/10.1093/gerona/glw205
- Doty, P., Mahoney, K. J., & Sciegaj, M. (2010). New state strategies to meet long-term care needs. Health Affairs, 29(1), 49–56. https://doi.org/10.1377/hlthaff.2009.0521
- Drentea, P., Clay, O. J., Roth, D. L., & Mittelman, M. S. (2006). Predictors of improvement in social support: Five-year effects of a structured intervention for caregivers of spouses with Alzheimer’s disease. Social Science & Medicine, 63(4), 957–967. https://doi.org/10.1016/j.socscimed.2006.02.020
- Fang, B., Yan, E., & Lai, D. W. L. (2019). Risk and protective factors associated with domestic abuse among older Chinese in the People’s Republic of China. Archives of Gerontology and Geriatrics, 82, 120–127. https://doi.org/10.1016/j.archger.2019.02.001
- Fang, B., Yan, E., Yang, X., & Pei, Y. (2021). Association between caregiver neurotic personality trait and elder abuse: Investigating the moderating role of change in the level of caregiver perceived burden. Gerontology, 67(2), 243–254. https://doi.org/10.1159/000512238
- Ferguson, S. L., Moore, G. E. W., & Hull, D. M. (2020). Finding latent groups in observed data: A primer on latent profile analysis in Mplus for applied researchers. International Journal of Behavioral Development, 44(5), 458–468. https://doi.org/10.1177/0165025419881721
- Finch, W. H., & Bronk, K. C. (2011). Conducting confirmatory latent class analysis using Mplus. Structural Equation Modeling, 18(1), 132–151. https://doi.org/10.1080/10705511.2011.532732
- Fisher, B. S., & Regan, S. L. (2006). The extent and frequency of abuse in the lives of older women and their relationship with health outcomes. The Gerontologist, 46(2), 200–209. https://doi.org/10.1093/geront/46.2.200
- Franklin, C. A., & Kercher, G. A. (2012). The intergenerational transmission of intimate partner violence: Differentiating correlates in a random community sample. Journal of Family Violence, 27(3), 187–199. https://doi.org/10.1007/s10896-012-9419-3
- Fulmer, T., Guadagno, L., Dyer, C. B., & Connolly, M. T. (2004). Progress in elder abuse screening and assessment instruments. Journal of the American Geriatrics Society, 52(2), 297–304. https://doi.org/10.1111/j.1532-5415.2004.52074.x
- Fundinho, J. F., Pereira, D. C., & Ferreira-Alves, J. (2021). Theoretical approaches to elder abuse: A systematic review of the empirical evidence. Journal of Adult Protection, 23(6), 370–383. https://doi.org/10.1108/JAP-04-2021-0014
- Gao, X., Sun, F., & Hodge, D. R. (2019). Elder mistreatment among Chinese American families: Do acculturation and traditionalism matter? Journal of Gerontology: Social Sciences, 74(3), 465–473. https://doi.org/10.1093/geronb/gbw154
- Garre-Olmo, J., Planas-Pujol, X., López-Pousa, S., Juvinya, D., Vilà, A., & Vilalta-Franch, J. (2009). Prevalence and risk factors of suspected elder abuse subtypes in people aged 75 and older. Journal of the American Geriatrics Society, 57(5), 815–822. https://doi.org/10.1111/j.1532-5415.2009.02221.x
- Gehr, T. J., Freiberger, E., Sieber, C. C., & Engel, S. A. (2021). A typology of caregiving spouses of geriatric patients without dementia: Caring, worried, desperate. BMC Geriatrics, 21(1), 483. https://doi.org/10.1186/s12877-021-02425-1
- Gilhooly, M. M., Dalley, G., Gilhooly, K. J., Sullivan, M. P., Harries, P., Levi, M., Kinnear, D. C., & Davies, M. S. (2016). Financial elder abuse through the lens of the bystander intervention model: Table 1. Public Policy & Aging Report, 26(1), 5–11. https://doi.org/10.1093/ppar/prv028
- Given, C. W., Given, B. A., Stommel, V., & Azouz, F. (1999). The impact of new demands for assistance on caregiver depression Tests using an inception cohort. The Gerontologist, 39(1), 76–85. https://doi.org/10.1093/geront/39.1.76
- Hallquist, M. N., & Wiley, J. F. (2018). MplusAutomation: An R package for facilitating large-scale latent variable analyses in M plus. Structural Equation Modeling: A Multidisciplinary Journal, 25(4), 621–638. https://doi.org/10.1080/10705511.2017.1402334
- Heyman, R. E., & Slep, A. M. S. (2002). Do child abuse and interpersonal violence lead to adulthood family violence? Journal of Marriage and Family, 64(4), 864–870. https://doi.org/10.1111/j.1741-3737.2002.00864.x
- Ho, C. S. H., Wong, S. Y., Chiu, M. M., & Ho, R. C. M. (2017). Global prevalence of elder abuse: A meta-analysis and meta-regression. East Asian Archives of Psychiatry, 27(2), 43–55.
- Hunt, C. H. (2003). Concepts in caregiver research. Journal of Nursing Scholarship, 35(1), 27–32. https://doi.org/10.1111/j.1547-5069.2003.00027.x
- Ice, G. H., Sadruddin, A. F. A., Vegedes, A., Yogo, J., & Juma, E. (2012). Stress associated with caregiving: An examination of the stress process model among Kenyan Luo elders. Social Science & Medicine, 74(12), 2020–2027. https://doi.org/10.1016/j.socscimed.2012.02.018
- Isac, C., Lee, P., & Arulappan, J. (2021). Older adults with chronic illness – Caregiver burden in the Asian context: A systematic review. Patient Education and Counseling, 104(12), 2912–2921. https://doi.org/10.1016/j.pec.2021.04.021
- Jackson, S. L., & Hafemeister, T. L. (2011). Risk factors associated with elder abuse: The importance of differentiating by type of elder mistreatment. Violence and Victims, 26(6), 738–757. https://doi.org/10.1891/0886-6708.26.6.738
- Kasper, J. D., Freedman, V. A., Spillman, B. C., & Wolff, J. L. (2015). The disproportionate impact of dementia on family and unpaid caregiving to older adults. Health Affairs, 34(10), 1642–1649. https://doi.org/10.1377/hlthaff.2015.0536
- Katz, S. (1983). Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. Journal of American Geriatric Society, 31(12), 721–727. https://doi.org/10.1111/j.1532-5415.1983.tb03391.x
- Khoury, L., Tang, Y. L., Bradley, B., Cubells, J. F., & Ressler, K. J. (2010). Substance use, childhood traumatic experience, and posttraumatic stress disorder in an urban civilian population. Depression and Anxiety, 27(12), 1077–1086. https://doi.org/10.1002/da.20751
- Lachs, M. S., & Pillemer, K. (2004). Elder abuse. The Lancet, 364(9441), 1263–1272. https://doi.org/10.1016/S0140-6736(04)17144-4
- Lesieur, H. R., & Blume, S. B. (1987). The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. The American Journal of Psychiatry, 144(9), 1184–1188.
- Li, M., Kong, D., Chao, Y. Y., & Dong, X. (2020). Association between personality traits and elder abuse in a community-dwelling Chinese population: Findings from the PINE study. Journal of Elder Abuse & Neglect, 32(4), 317–333. https://doi.org/10.1080/08946566.2020.1782300
- Liu, Z., Heffenan, C., & Tan, J. (2020). Caregiver burden: A concept analysis. International Journal of Nursing Sciences, 7(4), 438–445. https://doi.org/10.1016/j.ijnss.2020.07.012
- Lowenstein, A. (2010). Caregiving and Elder Abuse and Neglect—Developing a new conceptual perspective. Ageing International, 35(3), 215–227. https://doi.org/10.1007/s12126-010-9068-x
- Lundy, M., & Grossman, S. F. (2004). Elder abuse: Spouse/intimate partner abuse and family violence among elders. Journal of Elder Abuse & Neglect, 16(1), 85–102. https://doi.org/10.1300/J084v16n01_05
- Macneil, G., Kosberg, J. I., Durkin, D. W., Dooley, W. K., Decoster, J., & Williamson, G. M. (2010). Caregiver mental health and potentially harmful caregiving behavior: The central role of caregiver anger. The Gerontologist, 50(1), 76–86. https://doi.org/10.1093/geront/gnp099
- Mahoney, R., Regan, C., Katona, C., & Livingston, G. (2005). Anxiety and depression in family caregivers of people with Alzheimer’s disease: The LASER-AD study. The American Journal of Geriatric Psychiatry, 13(9), 795–801. https://doi.org/10.1097/00019442-200509000-00008
- McCubbin, H. I., & Patterson, J. M. (1983). Family stress and adaptation to crises: A double ABC model of family behavior. In D. H. Olson & B. C. Miller (Eds.), Family studies review yearbook (pp. 87–107). Sage.
- McLeod, J. D. (2012). The meanings of stress: Expanding the stress process model. Society and Mental Health, 2(3), 172–186. https://doi.org/10.1177/2156869312452877
- Mullen, P. E., Martin, J. L., Anderson, J. C., Romans, S. E., & Herbison, G. P. (1996). The long-term impact of the physical, emotional, and sexual abuse of children: A community study. Child Abuse & Neglect, 20(1), 7–21. https://doi.org/10.1016/0145-2134(95)00112-3
- Muthén, B. O., & Muthén, L. K. (2000). Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcoholism: Clinical & Experimental Research, 24(6), 882–891. https://doi.org/10.1111/j.1530-0277.2000.tb02070.x
- Muthén, L. K., & Muthén, B. O. (2017). Mplus user’s guide (8th ed.). Muthén & Muthén.
- National Council of Aging. (2015). Elder abuse facts. Retrieved from https://www.ncoa.org/public-policy-action/elder-justice/elder-abuse-facts/
- Nylund-Gibson, K., Grimm, R. P., & Masyn, K. E. (2019). Prediction from latent classes: A demonstration of different approaches to include distal outcomes in mixture models. Structural Equation Modeling: A Multidisciplinary Journal, 26(6), 967–985. https://doi.org/10.1080/10705511.2019.1590146
- Pearlin, L. I., Mullan, J. T., Semple, S. J., & Skaff, M. M. (1990). Caregiving and the stress process: An overview of concepts and their measures. The Gerontologist, 30(5), 583–594. https://doi.org/10.1093/geront/30.5.583
- Pepin, R., Williams, A. A., Anderson, L. N., & Qualls, S. H. (2013). A preliminary typology of caregivers and effects on service utulization of caregiver counselling. Aging & Mental Health, 17(4), 495–507. https://doi.org/10.1080/13607863.2012.758232
- Peugh, J., & Fan, X. (2015). Enumeration index performance in generalized growth mixture models: a monte carlo test of Muthén’s (2003) Hypothesis. Structural Equation Modeling, 22(1), 115–131. https://doi.org/10.1080/10705511.2014.919823
- Pickering, M., Yefimova, M., & Maxwell, C. (2018). Caregiver stress theory may explain elder abuse and neglect in dementia family caregiving. Innovation in Aging, 2(suppl_1), 851. https://doi.org/10.1093/geroni/igy023.3173
- Pillemer, K., Burnes, D., Riffin, C., & Lachs, M. S. (2016). Elder abuse: Global situation, risk factors, and prevention strategies. The Gerontologist, 56(Suppl 2), S194–205. https://doi.org/10.1093/geront/gnw004
- Pillemer, K., & Wolf, R. S. (1986). Elder abuse: Conflict in the family. Auburn House Publishing Co.
- Pristavec, T., & Pruchno, R. (2019). The burden and benefits of caregiving: A latent class analysis. The Gerontologists, 59(6), 1078–1091. https://doi.org/10.1093/geront/gny022
- Quinn, C., & Toms, G. (2019). Influence of positive aspects of dementia caregiving and well-being: A systematic review. The Gerontologist, 59, e584–596. https://doi.org/10.1093/geront/gny168
- Reine, G., Lancon, C., Simeon, M. C., Duplan, S., & Auquier, P. (2003). [Caregiver burden in relatives of persons with schizophrenia: An overview of measure instruments]. L’Encéphale, 29(2), 137–147.
- Santo, A. J., Nunes, B., Kislaya, I., Gil, A. P., & Ribeiro, O. (2019). Elder abuse victimization patterns: Latent class analysis using perpetrators and abusive behaviours. BMC Geriatrics, 19(1), 117. https://doi.org/10.1186/s12877-019-1111-5
- Serra, L., Contador, I., Fernández-Calvo, B., Ruisoto, P., Jenaro, C., Flores, N., Ramos, F., & Rivera-Navarro, J. (2018). Resilience and social support as protective factors against abuse of patients with dementia: A study on family caregivers. International Journal of Geriatric Psychiatry, 33(8), 1132–1138. https://doi.org/10.1002/gps.4905
- Shanahan, L., Copeland, W. E., Worthman, C. M., Erkanli, A., Angold, A., & Costello, E. J. (2013). Sex-differentiated changes in C-reactive protein from ages 9 to 21: The contributions of BMI and physical/sexual maturation. Psychoneuroendocrinology, 38(10), 2209–2217. https://doi.org/10.1016/j.psyneuen.2013.04.010
- Spurk, D., Hirschi, A., Wang, M., Valero, D., & Kauffeld, S. (2020). Latent profile analysis: A review and “how to” guide of its application within vocational behavior research. Journal of Vocational Behavior, 120, 103445. https://doi.org/10.1016/j.jvb.2020.103445
- Straus, M. A., Hamby, S. L., Boney McCoy, S., & Sugarman, D. B. (1996). The Revised Conflict Tactics. Scales (CTS2): Development and preliminary psychometric data. Journal of Family Issues, 17(3), 283–316. https://doi.org/10.1177/019251396017003001
- Thornberry, T. P., Knight, K. E., & Lovegrove, P. J. (2012). Does maltreatment beget maltreatment? A systematic review of the intergenerational literature. Trauma, Violence & Abuse, 13(3), 135–152. https://doi.org/10.1177/1524838012447697
- Tueth, M. J. (2000). Exposing financial exploitation of impaired elderly persons. The American Journal of Geriatric Psychiatry, 8(2), 104–111. https://doi.org/10.1097/00019442-200005000-00004
- United Nations, Department of Economic and Social Affair, Division for Social Policy and Development. (2015). Global ageing and the data revolution – the way forward in the post-2015 environment: Report of the expert group meeting. United Nations.
- U.S. Department of Health and Human Services. (2014). Informal caregiving for older Americans: An analysis of the 2011 National Study of Caregiving. Department of Health and Human Services. Retrieved from https://aspe.hhs.gov/reports/informal-caregiving-older-americans-analysis-2011-national-study-caregiving
- Wang, M. S., Kang, S. W., & Schiamberg, L. B. (2015). Ecological factors associated with elder abuse in Taiwan: A systematic review. Asia Pacific Journal of Social Work and Development, 25(1), 13–28. https://doi.org/10.1080/02185385.2014.943276
- Weden, M. M., & Zabin, L. S. (2005). Gender and ethnic differences in the co-occurrence of adolescent risk behaviors. Ethnicity & Health, 10(3), 213–234. https://doi.org/10.1080/13557850500115744
- Widom, C. S., & Wilson, H. W. (2015). Intergenerational transmission of violence. (J. Lindert & I. Levav, Eds.). Springer Science and Business Media.
- Wills, T. A. (1985). Supportive functions of interpersonal relationships. In S. Cohen & S. L. Syme (Eds.), Social support and health (pp. 61–82). Academic Press.
- World Health Organization. (2006). Elder abuse and alcohol factsheet. World Health Organization.
- World Health Organization. (2015). World report on ageing and health.
- Yan, E. (2014). Abuse of older persons with dementia by family caregivers: Results of a 6-month prospective study in Hong Kong. International Journal of Geriatric Psychiatry, 29(10), 1017–1027. https://doi.org/10.1002/gps.4092
- Yan, E. (2020). Caregiver resilience as a protective factor for elder abuse. Innovation in Aging, 4(suppl. Supplement_1), 46. https://doi.org/10.1093/geroni/igaa057.149
- Yan, E., Chan, K. L., & Tiwari, A. (2015). A systematic review of prevalence and risk factors for elder abuse in Asia. Trauma, Violence, & Abuse, 16(2), 199–219. https://doi.org/10.1177/1524838014555033
- Yan, E., & Fang, G. (2017). Elder abuse and neglect in Asia. In X. Dong (Ed.), Elder Abuse (pp. 477–494). Springer International Publishing.
- Yan, E., & Kwok, T. (2011). Abuse of older Chinese with dementia by family caregivers: An inquiry to the role of caregiver burden. International Journal of Geriatric Psychiatry, 26(5), 527–535. https://doi.org/10.1002/gps.2561
- Yan, E., & Tang, C. S. K. (2003). Proclivity to elder abuse: A community study on Hong Kong Chinese. Journal of Interpersonal Violence, 18(9), 999–1017. https://doi.org/10.1177/0886260503254461
- Zarit, S. H., Orr, N. I. C., & Zarit, J. M. (1985). The hidden victims of Alzheimer’s disease. New York University Press.
- Zhang, Z., Gu, D., & Luo, Y. (2014). Co-residence with elderly parents in contemporary China: The role of filial piety, reciprocity, socioeconomic resources, and parental needs. Journal of Cross-Cultural Gerontology, 29(3), 259–276. https://doi.org/10.1007/s10823-014-9239-4
- Zielinski, D. S. (2009). Child maltreatment and adult socioeconomic well-being. Child Abuse & Neglect, 33(10), 666–678. https://doi.org/10.1016/j.chiabu.2009.09.001
Appendix A
Demographic Background of the Caregivers (N = 600)
Table
Appendix B
Demographic Background of Care recipients (N = 600)
Table
Appendix C
Mean, Standard Deviations (SD), and Internal Consistencies of the Study Variables