
Abstract
Although rural youth experience marked inequities in adolescent pregnancy, there is little guidance for implementing evidence-based programs (EBPs) in rural settings. When implementation occurs in rural communities, it frequently focuses on deficits, rather than strengths or capacity for growth. Using the consolidated framework for implementation research (CFIR), we describe a resiliency-focused implementation of two middle school EBPs in rural Midwestern communities, including the intervention, outer and inner settings, individuals, implementation processes and preliminary outcomes. Data included program staff interviews, feedback from local partners, community meetings notes, and participant surveys. Using the CFIR, we describe the engagement of rural communities themselves in a resilience-based implementation of adolescent pregnancy prevention EPBs. Communities self-described as rural, traditional and religious. They identified adolescent pregnancy, substance use, and academic success as priorities. To address infrastructure needs and build on local strengths, funds were used to hire local partners to implement the program. As small communities, stakeholders were closely networked and wanted to address local needs. Local partners selected the EBP based upon community values and priorities. Champions, including local partner organizations and schools were locally based and were well connected. Intensive training of local staff and piloting with adaptation assured fidelity and sustainability, while increasing community implementation skills and comfort. In Clinton County, enrollment was 1946 with students receiving the program in 6th, 7th, and/or 8th grades. In Southern Indiana, 7275 students received the program once in either 6th, 7th, or 8th. We conclude that the CFIR can facilitate the implementation of a community resilience-focused adolescent pregnancy prevention intervention in rural communities.
Introduction
Despite recent declines, the U.S. teen pregnancy rate remain high, with persistent geographic disparities. While concerted efforts over the past twenty years in developing new evidence-based programs (EBPs) have provided additional tools to reduce teen pregnancy, the vast majority of research consists of clinical trials in dense urban areas, rather than implementation studies across different contexts.Citation1 It is not clear whether and how these programs can be adapted to new settings, such as rural communities, and remain effective. Work is needed to develop implementation models for evidence-based teen pregnancy prevention across the range of cultural and community settings.Citation2 Using the Consolidated Framework for Implementation Research (CFIR), we describe how a resiliency focused implementation model can be used to implement teen pregnancy prevention programs for rural Midwestern middle school students.
Resilience can be thought of as the capacity to successfully adapt to an experience of stress or adversity.Citation3 Resilient communities are able to adapt to community-level adversity, maintaining or improving population functioning and wellbeing, reducing health disparities, and maintaining quality of life.Citation3 In public health, the concept of community resiliency comes from the field of disaster response and readiness, but has more recently been applied to chronic public health issues in child and adolescent health.Citation4
Community resilience-based approaches in public health identify and harness a community’s protective processes that guard against risk and support adaptive responses to hardships.Citation5 These approaches focus on community strengths and assets, rather than weaknesses. Community resiliency theory is built upon the idea that communities already possess the raw material (people, groups, organizations) necessary for resilience.Citation6,Citation7 These formal and informal networks aid in building capacity and social action.
Nationwide, adolescent birth rates in rural counties are persistently higher and have experienced fewer declines compared to urban and suburban counties.Citation8 Indiana, a state with 49 rural counties and another 20 counties with large rural census tracts,Citation9 ranks 39th nationally in adolescent pregnancies,Citation10 with an adolescent birth rate higher than the national average (22.8 vs. 18.8/1,000 girls age 15–19).Citation11 These geographic disparities are apparent on the county level in Indiana, with adolescent birth rates in the rural communities as much as twice as high as the state average.Citation12 Given these statistics, it is an easy trap to focus interventions on deficits; however, resilience theories posit that effective interventions will focus on community assets and capabilities.
Adolescent pregnancy is influenced by a series of community resilience-related risk and protective factors. Communities with stronger connections among adolescents, adults, and schools, that foster communication among adolescents, parents and partners, and with schools that provide sexual health education, have lower rates of adolescent sexual risk behaviors and adolescent pregnancy.Citation8,Citation13,Citation14 Substance use is a risk factor that operates on both a community level (e.g. in community disorganization) and an individual level, and is disproportionately high in rural communities.Citation15
Our programs focus on middle school (6th–8th grade, approximately 11–13 years of age) as an important age for pregnancy prevention. Middle school is a series of “firsts”—first attraction, first relationship, first kiss, first experimentation with substances.Citation16–18 Peer relationships and acceptance are important to middle-schoolers, and it is during middle school that adolescents develop healthy peer, romantic and sexual relationship skills, an appreciation for gender equity, respect for oneself and others, and communication skills.Citation18 From a community resiliency perspective, middle school is an ideal time for prevention because community strengths, such as adolescent connectedness to schools and communities, and community assets, such community organization, community safety, and opportunities, influence individual behavior and risk.Citation19–21
On a community level, factors such as the availability of developmentally appropriate, evidence-based sex education and access to sexual health services are associated with lower adolescent pregnancy rates.Citation22 Over the past 20 years, there has been a focus on the use of evidence to support sex education, with the US Department of Health and Human Services (HHS) Office of Adolescent Health and the Centers for Disease Control and Prevention maintaining lists of curricula shown to change sexual behavior (e.g. delay the onset of sex, increase condom use).Citation23 Here, rural communities are at a disadvantage. Despite higher pregnancy rates, there are few EBPs designed and evaluated for rural youth, few EBPs addressing shared risk and protective factors for pregnancy and substance use, and there is little guidance for implementing existing EBPs in rural settings.
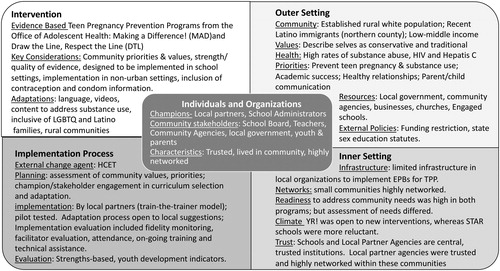
Although the field of implementation sciences has made progress toward developing models for implementing adolescent interventions in community settings, there is limited research that evaluates the extent that teen pregnancy prevention programs can be adapted and still maintain fidelity.Citation1 The question remains as to how far can an EBP be stretched and still considered an EBP? Use of an implementation sciences model, such as the CFIR, provides a comprehensive framework to study implementation.Citation24 Our purpose is to describe the use of the CFIR to implement community resiliency-focused teen pregnancy prevention programs for rural Midwestern middle school students. We map key implementation activities across the five domains of the CFIR: interventions, outer contexts, inner contexts, implementation, and individuals (see ).Citation25
Figure 1. Resilience-based implementation process for rural teen pregnancy prevention mapped onto the Consolidated Framework for Implementation Research (CFIR).
Methods
Evaluation overview
To better understand and replicate resilience-focused implementation of middle school sex education EBPs in rural counties, we completed a post-implementation formative evaluation.Citation26 This evaluation was conducted through a university-community partnership between the Indiana University School of Medicine and a community nonprofit serving the 5-state Midwest region, Health Care Education and Training, Inc. (HCET). Using qualitative and quantitative data, our evaluation determined the degree of goal achievement through analysis of inputs (funding/partners), outputs (curriculum, participants served), short term outcomes data (behavior, intention, attitudes), and barriers/facilitators to goal achievement (system and community level).Citation26 We mapped these mixed methods data onto the CFIR model (see ).
Data sources included: (1) community and local partner meetings notes from initial stakeholder meetings, site visits, collaborative partner meetings and monthly check-in calls; (2) program staff interviews (Clinton County only); (3) required online structured qualitative feedback from local partners during intervention delivery; and (4) participant pre- and post-program surveys. Community meeting notes were kept by HCET staff to document individuals attending and the content/outcomes of program planning meetings with local program partners, youth-serving community agencies, schools, and other key stakeholders. Local partner meeting notes were from periodic meetings with local partners about implementation issues. Program staff interviews were more formal qualitative, open-ended interviews done with HCET and local program staff after implementation to document successes and challenges in implementation. Example questions included, “Name some barriers that you faced,” and “how did you overcome those barriers.” Interviews were recorded and transcribed. Structured feedback was collected from local partners after each class as part of HCET routine to monitor curriculum fidelity and collect program-level federal performance measures. Facilitators access a web-based form on a secure server. The web-based form assessed attendance, lesson content, adaptations made and unexpected deviations from the lesson plan.
Because rates of pregnancies are low among middle school aged youth, middle school programs target intermediate outcomes, in particular, sexual behaviors. While sexuality is a core component of normal development when young adolescents (middle schoolers are typically 11–14 years of age) have sex, that sex is more likely to be coercive and the adolescents are less likely to use contraception or condoms, leading to high rates of pregnancy among those that are sexually active.Citation27 Pre- and post-program surveys of adolescent participants collected demographics (part of federal performance measures), knowledge, attitudes, and health behaviors. Items included sexual behaviors and intention, and resilience-focused risk and protective factors including community and school connectedness, and parent communication. Both projects were reviewed by the Indiana University Institutional Review Board, and determined to be exempt. With the exception of a condom demonstration (active parental permission required by the school board), both projects used an “opt out” approach to parental permission that is standard in Indiana schools for sex education programing. All parents were notified of the EBP and the survey. Parents were given an opportunity to review curricular materials and the surveys, ask questions, and ask that their child not participate in the program or survey.
Analytic approach
Qualitative data, including notes, interview data, and structured feedback, were analyzed using thematic analysis.Citation28 Quantitative data were analyzed using descriptive statistics and bivariate analyses using t-tests and chi-square (Statistical Package for the Social Sciences, version 24). All data were mapped onto the CFIR. The CFIR organizes implementation into five domains: (1) Interventions themselves; (2) Outer contexts which address broad community structure, resources and values; (3) Inner contexts which focus on characteristics of organizations and networks; (4) Processes of implementation; and (5) Individuals, including stakeholders and champions ().Citation25 Although conceptualized as distinct domains, there was overlap.
Program overview
HCET implements adolescent pregnancy prevention and positive youth development EBPs on a large scale. Two such funded project, HCET Clinton County Youth RISE! (Responsible, Involved, Supported, and Educated) and HCET STAR (Strong Teens Acting Responsibly) were implemented in middle schools in rural Indiana counties. describes characteristics of the middle school students in these two projects. YouthRISE! Focused on a single rural county, and the middle school program, which consisted of three linked curricula, one for 6th, one for 7th, and one for 8th graders, was one component of a multi-component community-wide intervention. Other components included high school, elementary school, and community-based programs in the same community. YouthRISE! implemented a comprehensive teen pregnancy prevention EBP, Draw the Line/Respect the Line (DTL)Citation29 in a single middle school. DTL has been demonstrated to delay sexual onset in boys and to change peer norms in both girls and boys in a randomized controlled trial.Citation30 The federal grant mechanism for YouthRISE!, a Tier 1 implementation project in the Teen Pregnancy Prevention Program, required strict fidelity to the EBP as written.Citation23,Citation31 As such, the community needed to select the EBP that best fit their needs.
Table 1. Reach of programs and characteristics of participants in rural middle-school pregnancy prevention programs.
In contrast, STAR, the southern Indiana program, focused exclusively on middle schools across 12 counties in southern Indiana with high rates of Hepatitis C and human immunodeficiency virus (HIV) infections. STAR implemented an abstinence-focused EBP, Making a Difference! (MAD).Citation32 MAD has demonstrated delayed sexual onset among sexually inexperienced adolescents,Citation33 and has been adapted and implemented across a range of settings. STAR’s federal funding, the Sexual Risk Avoidance Education Program,Citation34 allowed adaptations, with larger adaptations requiring consultation with the program officer. Developed in urban centers, HCET adapted the program for rural Indiana youth, including creating an adapted video set in a rural community.
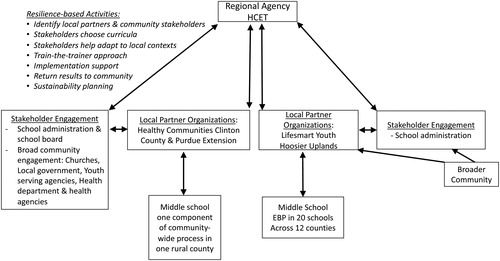
Interventions were delivered in middle schools as part of health education classes. To improve sustainability, HCET partnered with agencies already working in these communities to assess community priorities, create relationships with school administrations and community stakeholders, choose the EBP, receive training on the EBP, and deliver the EBP in their community (). HCET provides sub-awards to these local partner organization for implementation, training, technical assistance, oversite and ongoing quality assurance/quality improvement related to implementation of the EBP. Our local partners in Clinton County were Healthy Communities of Clinton County Coalition, Purdue Extension of Clinton County, and the Learning Network of Clinton County. Local partners for southern Indiana were LifeSmart Youth, Inc., Purdue Extension, and Hoosier Uplands. Facilitators from partner organizations and teachers delivered the curricula.
Figure 2. The process of implementing rural teen pregnancy prevention in rural communities using a community resilience process.
Results
Overview
HCET utilized a resilience-based approach, identifying, working collaboratively with, and building the capability of the individuals, organizations, and both formal and informal networks within communities. Examples of community-level risk factors identified included a lack of sexual health education and services for adolescents, a stagnating economy, high community rates of substance use, and low levels of communication on adolescent pregnancy risk. Examples of community protective factors included school districts willing to bring in new programs, health-focused community agencies with strong community linkages, and community leaders willing to address the issue of adolescent pregnancy. Using the CFIR, we identified the elements of the interventions, outer and inner contexts, processes and individuals that are specific to rural implementation and to a resilience-based approach to adolescent pregnancy prevention ().
Intervention
HCET utilized a resilience-based process of choosing an intervention. The funding mechanism required that interventions be EBPs identified by the HHS.Citation23 Rather than recommending a specific middle school EBP, community meeting notes and interviews with staff described how HCET worked collaboratively with local partner organizations and stakeholders to first identify community values and priorities, then identify key community capabilities, and finally to help local partners and stakeholders themselves select an EBP that was consistent with these values, and capabilities priorities. HCET and partners had a shared understanding that curricula must be evidence based, implemented with full fidelity and only use minor adaptation if essential (i.e. language, local data), have a close fit with the target community, be LGBTQ+ (lesbian, gay, bisexual, transgender, question and questioning) inclusive, culturally proficient, and medically accurate. All potential and final curricula and supporting materials were shared with implementation partners, schools, and upon request, to other stakeholders.
Key considerations for local partners and stakeholders in staff interviews and notes were the strength and quality of the evidence, space and time constraints, whether the program had been developed or implemented in non-urban settings, the presence of a youth development component, and the community’s willingness to accept a comprehensive program. A controversy in middle school sex education is whether to choose a program that teaches only abstinence, or also include information on contraceptives and condoms. While the vast majority of the programs which have shown any type of effectiveness are comprehensive (i.e. abstinence plus contraception), three out of 41 programs on the list of EBPs are abstinence-focused.Citation23 Complicating this issue is that sex education is often framed as a “values” question about whether communities should accept sexual behavior in teens, rather than as a public health issue about what is the most effective way to prevent adolescent pregnancy.
Clinton County local partners, schools, and community stakeholders chose DTL, a comprehensive multiyear program. Interviews and meeting notes identified this decision as based upon the following factors: (1) their beliefs that a program based upon youth development principles would fit their community well; (2) DTL had been implemented in non-urban settings; (3) DTL’s effectiveness in preventing pregnancy, an important public health and social issue in their community; and (4) DTL’s graded approach—the education would build across three years, starting with an abstinence-focused 6th grade curriculum and ended with a comprehensive 8th grade curriculum with a condom demonstration. When implemented with fidelity, DTL consisted of 19 × 45 minute-session spread across grades 6, 7 and 8 (4–6 hours/year). Passive parental permission was used for all of the curricula except for the 8th grade condom demonstration. Written active parental permission was requested because the school and other stakeholders wanted to be certain that parents were aware of the condom demonstration.
Local partners and schools in southern Indiana chose Making a Difference! (MAD), one of three abstinence programs that meet the rigorous U.S. HHS evidence criteria. This choice was based upon MAD’s focus on medically accurate HIV education, the fact that it has been adapted across multiple cultural and community settings, and its ability to be implemented in school settings. Local partners felt that a shorter, abstinence-focused program meeting Indiana’s HIV education requirement would be more acceptable across school districts in this region that self-described as rural and conservative. The use of MAD required multiple adaptations. Some were pragmatic, such as fitting one-hour lessons in a 40 minute class periods. Others reflected newer values, such as LGBTQ + inclusivity. The one major content adaptation was creating a new video. The original video featured two urban teens with typical urban language, dress, and scenarios. The new video featured two rural teens with language, dress and scenarios more likely to be found in the rural Midwest.
Because of the high priority placed upon substance abuse prevention by southern Indiana communities, MAD was supplemented with a short evidence-informed substance abuse prevention program, Guiding Good Choices. Together, these two curricula were implemented in 9 sessions, through middle-schools health classes (either 6th, 7th, or 8th, depending upon the school). STAR schools used a similar opt-out parental permission approach, notifying parents, allowing time to respond and review materials, and to withdraw a student from the program.
Outer setting
Community
Clinton County is a rural community in north central Indiana with a primarily white and growing Latino population of recent immigrants. The Southern Indiana counties served by STAR were predominately white, with rates of child poverty higher than state or national averages.Citation35 For both projects, residents lived in small towns or in geographically dispersed locations throughout rural areas in the county. Because of geographic dispersal, schools were identified as central hubs, and interviews and notes of meetings with local partners and stakeholders felt that programs needed to be run in schools.
Shared values
In community resilience theory, people and connections among people are the most important assets of a community,Citation6 and shared values are an important way that people in a community connect. During interviews, stakeholders described their communities as traditional, rural, and religious felt that these shared values as important for community cohesion.
A challenge arising from a shared values approach was that there were concerns raised by community members that reproductive health for adolescents was considered to be a difficult, but not insurmountable, topic for their communities. This challenge was addressed by re-framing adolescent pregnancy as a health, rather than a values issue. The success of this approach was demonstrated when stakeholders themselves began to describe adolescent pregnancy as a serious public health issue, rather than a values and personal responsibility issue. This public health framing allowed community members with disparate values about adolescent sexuality work together on pregnancy prevention.
In interviews, both HCET and stakeholders placed high value in local input, respect for community values and priorities, and community involvement at all stages during the process. The important of local partner and stakeholder ownership of the project drove several key decisions, including local choice of curricula, incorporation of local preferences for parental notification and consent, and the hiring and training of individuals living and working in the community to be the primary implementation team.
Health indicators and access
The 2013 birth rate for teens age 15–19 in Clinton county, Indiana was 46.2/1,000 young women 15–19 years old, with higher rates for Latina teens.Citation36 Individual level data on adolescent sexual behaviors and contraceptive use were not available in the communities prior to program implementation. The local data supporting the grant applications used health department natality data and state-level behavioral data. Individual level data collected as part of these programs were used for a more detailed needs assessment for school districts and communities. These new data have been perceived as useful for program planning and funding.
Access-related risk factors for teen pregnancy included poverty, no family planning services in the county, and limited access to health services. Overall teen birth rates across southern Indiana counties were above the state and national average, ranging from 25.9/1,000 to 46.1/1,000.Citation36 These communities also had high rates of opioid and injection drug use, and this substance use epidemic was overlaid with a Hepatitis C and HIV epidemic.Citation37
Community priorities and resources
Because Clinton county was an intensive, single-community intervention, HCET was able to draw strongly on community resilience approaches, starting with facilitating a self-assessment of priorities and resources. This was done through a series of key stakeholder meetings in which participants were asked to set priorities, and to identify strengths and resources. Stakeholders included not just the partner agencies, but other community agencies serving youth and families, school administration and school board, church leaders, health resources (e.g. local pharmacy), the county health department, and county government officials, including the Mayor’s office. Clinton county participants prioritized teen pregnancy and graduation from high school. Substance use was a secondary concern. Community resources included a community health agency (Healthy Communities Clinton County) led by a local champion, highly engaged schools and a school board willing to consider a new approach to sex education, churches willing to participate in stakeholder meetings, and broad participation from stakeholders, including youth and parents.
In southern Indiana counties, assessing community preferences was more challenging from a resilience-based perspective. Rather than a single cohesive geographic area with existing networks and community groups, the target was an age group—middle school—that was spread across 12 different rural counties. As all programs were to be implemented only in middle schools as part of their health education curricula, HCET focused on school administrators and existing community health education agencies to set priorities and identification of strengths. These groups identified substance abuse as their prevention priority, but, given the recent high profile HIV and Hepatitis C outbreak linked to substance abuse and a rural HIV outbreak in one target community,Citation36,Citation38 recognized the connection between substance abuse and unintended pregnancy and HIV. For both programs, this process of assessing community priorities and preferences started prior to the grant application submission, so that the identified EPBs would be ones that the community selected as responsive to their needs.
External policies
Indiana Department of Education (IDOE) policies for human sexuality and HIV education caused considerable differences of opinion. IDOE requires that schools teach that “abstinence from sexual activity outside of marriage as the expected standard for all school children.”Citation39 The policy does not mention contraception, condom use, or risk reduction approaches. As a “local control” state, the rest of sex education is generally left to the school corporations.Citation26 As a result, some schools teach that abstinence is the only option, whereas others will teach an abstinence-focused curriculum that includes information on contraception and condom use. The philosophy of local control, which posits that communities are the best positioned to made decisions for their youth because they are the closest to the students and most invested in their success,Citation40 is consistent with resilience-based approaches. Clinton county embraced the concept of local control.
The two federal grants had different requirements for adaptation, which affected the planning and curricular selection and adaptation processes. Clinton County, funded through HHS’s Teen Pregnancy Prevention Initiative, required programs be selected off of a list of selected EBPs, be inclusive of sexual and gender minorities, and have strict fidelity to the program. The requirement for strict fidelity was somewhat at odds with a resilience-based approach, as it limited adaptation to community needs. The strict fidelity requirement necessitated intensive community participation at the front end of the process, at the point of curricula selection. In contrast, the funding for the southern Indiana project was through the Administration for Children and Families, had less stringent requirements for strict adherence to selected program models, and allowed more adaptation. This flexibility allowed HCET and local partners to take adapt the curriculum more specifically to community needs.
Inner setting
Organizational infrastructure
On the local level, there was limited infrastructure in community agencies or schools to implement EPBs for adolescent pregnancy prevention. Community agencies did not have the funding, staffing, or experience with key components of EBP implementation, such as facilitator training, fidelity monitoring, and evaluation. In contrast, HCET had 15 years of experience in implementing EBPs through federal, state, and regional adolescent pregnancy prevention projects, including grant writing, staff with experience in training and facilitation in teen pregnancy prevention, tools for site observations and fidelity monitoring, and evaluation. Building local community capacity through hiring, training, and close collaboration was a key component of the community resiliency-based approach.
Organizational networks
The communities were, however, highly networked, an important strength from a resilience perspective. Integrating into these networks was critical to accessing community strengths, understanding community priorities, and identifying local champions. To address this barrier, HCET partnered with local agencies with established programs in the community (local partner). In a small, rural community, the local partners were staffed by members of the community, and were closely networked to schools and other agencies. For example, three local partners offered other health, housing, and education programs in the same space. This co-location fostered both formal and informal communication among stakeholders. In Southern Indiana, Hoosier Uplands had established relationships with middle schools built upon trust that allowed the implementation of sex education content that otherwise might have been deemed too controversial.
Climate
In Clinton county, there was a clear community mandate to address teen pregnancy, with support of community leadership (agencies, school board, local government), and willingness to make changes in adolescent sex education. Framing was critical in creating a climate that could recognize and support community values, but would allow the implementation of comprehensive EBPs for adolescent pregnancy prevention. Leaders presented the programs as a part of a larger health and wellness initiative, and the use of local data on adolescent pregnancies and sexual behavior in community meetings further reinforced that adolescent pregnancy should be approached as a public health issue. The health framing additionally allowed the community to reconcile their stated values around adolescent sexuality and the implementation of a comprehensive sex education program. In Clinton county, the impetus to change the community’s approach to teen pregnancy prevention came initially from a local partner, rather than HCET, which likely contributed to a community climate that made the implementation of comprehensive sex education possible. In southern Indiana, local partners were similarly trusted and networked throughout their counties. However, in the absence of broad community mandates or prioritization of teen pregnancy as a health issue, school administration and local partners were reluctant to include aspects of middle school sex education considered more controversial, such as contraception information and condom demonstrations.
Individuals
All sources of data identified “local champions” as the most important element of successful implementation. Local champions included individuals and organizations that were respected and highly networked members of their communities. In Clinton county, implementation champions included the Executive Director and senior staff in a local partner and community educators at the other partners. Two partners, Purdue Extension and Learning Network of Clinton County, have deep roots in the Latino community in Clinton County. Other key individuals were the Assistant Superintendent, Principals, key teachers, and the School Board, whose support was evidenced through their willingness to allow time for teacher training and adapting the school schedules to fit the required lessons. During the implementation process, parents and youth played supportive roles through community and youth advisory boards, providing input and acting as informal spokespeople. In Southern Indiana, a multi-service health agency championed the project and was supported by school principals across multiple counties. Common characteristics of these champions were that they were rooted in the community (many since childhood), lived in the community, and were well connected and respected both personally and professionally.
Implementation process
External change agent
In both programs, HCET functioned as an external change agent bringing grant-writing and adolescent pregnancy prevention EBP implementation expertise. This funding and implementation expertise addressed the community infrastructure needs. HCET took a community capacity building approach, strengthening existing individual skills and organizational capacity. Funding was intentionally sub-awarded in higher amounts to a small number of local partners to support at least one full time staff person to manage the project. This allowed local partners to hire new staff, create new positions, and add a new service to their existing offerings. This approach built community capability for teen pregnancy prevention programing, and institutionalized the local partner as the trusted source for reproductive health education in their county.
Planning
As noted above, the early stages of planning included a community self-assessment of values and priorities, engagement of stakeholders in curriculum selection and adaptation, and creating of a project logic model sensitive to community goals and objectives. A key aspect was assessment of program “fit” to youth and families in the communities. Designated local partner program staff and key school personnel were co-decision-makers with HCET in the implementation of curriculum training, fidelity monitoring, and evaluation design.
HCET staff identified transparency as a priority in their collaborative relationships with communities. By transparency, we mean clear and frequent communication between the outside change agent (HCET) and community stakeholders. HCET and stakeholders both identified clear and frequent communication as critical to building trust, particularly at the start of the project. By intentional involvement of communities from the start, stakeholders and champions were more able to participate in key content decisions and enhance their ownership of the process. An example of transparency on the part of the change agent was that during the planning phase, HCET convened community and youth advisories, champions, and key stakeholders to talk through funding requirements, grant writing process, potential curricula and approach, staffing, committed and potential schools and budget requirements.
Implementation
The implementation approach built upon key aspects of community resilience, including developing skills in program facilitation and implementation to local partners and schools, involving local partner and stakeholder input into all facets of implementation, and focusing on on-going training with the ultimate goal of local sustainability. A key component of implementation was the use of a train-the-trainer approach to both train teachers and other facilitators for classrooms, and to train local partners in implementation skills. Having local trainers meant that individuals in the community could not only facilitate, but train a next generation of facilitators. Classroom trainers were trained on trauma informed program delivery, answering difficult questions, managing bullying, and content including sexual health information. Local partners were trained in survey collection, implementation evaluation tools, program reporting, fidelity monitoring, sub-awardee federal fund management, and research procedures. The regular site visits to assess fidelity and facilitator skills and to address any facilitator concerns or questions were collaborative, with both HCET and local partner participation advancing the goal of the local partner taking on the role in the future. The programs were pilot tested with an adaptation process open to local suggestions, and community stakeholders reviewed and adapted tools for fidelity monitoring and evaluation.
Because of limited funding and scarce resources in many of the rural communities served in this project, sustainability was built into program design. Use of train-the-trainer models anticipated needs for future turnover and implementation in neighboring communities.
Evaluation
The strengths-based evaluation mirrored the community resilience-approach of the program implementation. The process evaluation, which monitored fidelity to the curriculum and procedures, utilized self-reflection and real-time feedback. Local facilitators completed session reflections forms after each class in which they themselves identified successes, challenges, and adaptations to the curriculum. Site observations were conducted by both HCET and local partners, and feedback was given in real-time.
Student surveys were developed by external evaluators at Indiana University. These surveys captured required federal performance measures. They also measured key goals and objectives, developed by the community, and laid out in the logic model. In both locations, surveys measured not only sexual behaviors and intentions, but also constructs identified as important to the community, including adolescent attitudes and values around abstinence and pregnancy, adolescent communication with families about sex, and co-occurring substance use. Surveys additionally measured youth development indicators, such as decision-making skills. Local partners and schools provided initial and ongoing feedback on survey development, surveys were approved by schools and survey procedures were consistent with the federal education rights and privacy act (FERPA). Examples of changes included the elimination of questions on economic status, which were felt to be intrusive in this low to middle income community, and the decision to use a series of anonymous cross-sectional surveys for middle school, rather than tracking ID numbers, which communities felt would better protect the privacy of students and families. Local partners were trained in research ethics and data collection. Surveys were piloted the same time the interventions were piloted to identify any needed adaptations related to time, language, acceptability, and understandability. Plans were made to return results to the communities in a format that could be used for future funding applications.
Outcomes (see and )
Reach
The resilience-based process demonstrated adequate reach in terms of numbers of participants and the ability to reach youth at risk for unintended pregnancy. In Clinton County, 701 receive the program in 6th grade, 645 in 7th grade, and 588 in 8th grade for 1946 total enrollment across 3 years (). Participants were 12.4 +/−1.0 years, and were diverse ethnicities, reflecting the fact that the recent Latino immigration consists primarily of young people and families. Participants reported a mix of risk and protective factors. Sexual behavior was uncommon (4.3%). Although participants reported little parent communication on sexual topics (5.0 ± 4.7, Range 0–20), positive attitudes toward abstinence were high (16.0 ± 3.0 range 5–20). Substance use was a common risk factor, with 11% reporting tobacco use, 34% alcohol use, 8% marijuana use, and 7% prescription pill use.
In Southern Indiana, 7275 students received a single 2 week period of programing in either 6th, 7th, or 8th grades (). The grade that received programing was determined by the school schedule and school administration. Participants were 12.7 +/−0.9 years, most described themselves as white, and few described themselves as gender non-binary. Less than 6% had sex, less than 10% intended to have sex in the next 6 months and most (73%) intended to remain abstinent through high school. For parental communication, participants reported low frequency of communication and numbers of sexual topics (6.6 ± 5.2, Range 0–22). However, participants’ baseline knowledge of curriculum content was high (3.5/4 knowledge questions correct), baseline positive attitudes toward abstinence were high (15.6 ± 3.0, Range 5–20) and most (73%) intended to remain abstinent through high school. Substance use was again a common risk factor, with 16% reporting tobacco use, 33% reporting alcohol use, 7% marijuana use, and 3.9% prescription pill use.
Data driving program change ()
Data from surveys were used as a tool to improve program implementation. In many cases, our baseline surveys provided local schools with their first individual-level data on adolescent risk behaviors. An area of particular interest was program fit with the population. For example, when analyzing the Southern Indiana data by grade, we observed a marked increase in sexual behaviors, decrease in positive attitudes toward abstinence, and increase in substance use from 6th through 8th grade (). These findings suggested that an abstinence focused curriculum may not be appropriate for 8th graders, and that 8th graders may need a more comprehensive program that includes both contraception and substance use. These data led HCET to recommend to local community partners and schools currently implementing MAD in 8th grade health classes to instead implement it in 6th or 7th grade classes. HCET staff noted that local program partners and schools were more open to this type of change when it was based upon data from their own students.
Table 2. Characteristics of Southern Indiana middle school participants by grade.
Discussion
Use of a community resilience approach facilitated the successful implementation of two middle school sex education programs in rural Indiana counties. Our analysis, using the CFIR suggests that key components were the explicit attention to community priorities, use of local champions, partnering with local agencies, and use of a train-the-trainer approach in these rural communities. We identified program successes as uptake by school districts, high numbers of students participating, and implementation with fidelity. We credit these successes to rural community ownership of the processes and building upon the strength and capacity inherent in the individuals, organizations, and networks in rural communities. Transparency in process allowed trust and community ownership. The use of local data both during community mobilization and afterwards from participant surveys also facilitated community ownership of implementation and adaptation of programs.
Sex education, particularly for 12–14 year-olds (middle school age) is controversial in the United States, particularly in rural areas. The explicit use of a health framework, rather than a values framework, allowed local communities to align the programs with their values and priorities. The resilience-based approach also helped to limit controversy, as local stakeholders were engaged in priority setting, curriculum selection, implementation, and evaluation.
A key component of a resilience-based approach is having communities take program ownership and to set program priorities. We recognize that key to our success were the communities themselves identifying teen pregnancy (Clinton county) and the substance abuse, HIV and Hepatitis C epidemic (southern Indiana) as important health priorities. Also critical to our success were the presence of local champions, in the form of individuals or organizations, that provided entre to the individuals, local organizations, and formal and informal networks that make communities resilient.Citation7
Planning for sustainability is an important aspect of public health funding. We found that sustainability was enhanced by our focus on building community capabilities. Our use of train-the-trainer approaches left local community partners and schools not just able to run the programs, but able to train subsequent generations of teachers and facilitators in the curriculum. Outside funding was critical to the initial implementation, as none of the schools were using evidence-based curricula prior to the implementation of these programs. Several used homegrown abstinence programs and others had single lessons to meet minimal state education requirements for HIV education. However, engagement with community stakeholders and the use of local champions at all levels of program implementation ensured that an invested member of the community would have the requisite skills in adolescent pregnancy prevention programing.
There was tension between fidelity and a resilience-based approach focused on a specific community’s unique needs, because maintaining strict program fidelity limits adaptation to local community contexts, values and preferences. This tension was not resolved. In one program, the community invested additional time and effort at the front end of the process to identifying a program with the best “fit”. This, however, required a high degree of flexibility and trust on the part of the community, and there were still unanticipated needs for adaptation during implementation. The second program required multiple adaptations for a rural setting. While efforts were done to make these best practices adaptations, differences existed between the curriculum as written and as implemented.
Conclusions
The use of a community resilience-based approach allowed our group to go beyond commonly held assumptions about rural counties. For example, many assume rural communities will only accept abstinence, or that they will not allow LGBTQ + inclusivity. Using a resilience-based approach, two LGBTQ + inclusive programs and one comprehensive sex education program were implemented with fidelity in rural Indiana counties. Future directions include prospectively testing a resilience-based approach to implementation of sex education in other rural areas of the state, or other grade levels in these counties. Next steps include the use of more quantitative measures to better prospectively describe implementation factors such as community climate, willingness to innovate, and champions. Our initial study of two implementations suggests that more intensive community engagement and ownership of the program may lead to more innovation. A possible association between “dose” of community engagement program success will also need to be further explored.
Data availability
The data that support the findings of this study are available on request from the corresponding author, M.O. The data are not publicly available due to confidentiality concerns (surveys cover sexual behavior, a sensitive topic, with minors).
Disclosure statement
None of the authors have a potential conflict of interest. Contents are solely the responsibility of the authors and do not necessarily represent the official views of the Department of Health and Human Services or the Office of Population Affairs.
Additional information
Funding
References
- Mueller T, Tevendale HD, Fuller TR, et al. Teen pregnancy prevention: implementation of a multicomponent, community-wide approach. J Adolesc Health. 2017;60(3):S9–s17. doi:10.1016/j.jadohealth.2016.11.002.
- Philliber S, Nolte K. Implementation science: promoting science-based approaches to prevent teen pregnancy. Prev Sci. 2008;9(3):166–177. doi:10.1007/s11121-008-0094-9.
- Norris FH, Stevens SP, Pfefferbaum B, Wyche KF, Pfefferbaum RL. Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. Am J Community Psychol. 2008;41(1–2):127–150. doi:10.1007/s10464-007-9156-6.
- Ellis WR, Dietz WH. A new framework for addressing adverse childhood and community experiences: the building community resilience model. Acad Pediatr. 2017;17(7):S86–S93. doi:10.1016/j.acap.2016.12.011.
- Mancini JA, Bowen GL. Community resilience: A social organization theory of action and change. In: Pathways of Human Development: Explorations of Change. USA: Lexington Books; 2009:245–265.
- Kretzmann J, McKnight J. Building Communities from the Inside Out: A Path toward Finding and Mobilizing a Community’s Assets. Chicago, IL: The Asset-Based Community Development Institute, Institute for Policy Research, Northwestern University; 1993.
- Morgan A, Ziglio E. Revitalising the evidence base for public health: an assets model. Promot Educ. 2007; 14(2_suppl):17–22. doi:10.1177/10253823070140020701x.
- Centers for Disease Control and Prevention. Social determinants and eliminating disparities in teen pregnancy. Department of Health and Human Services. https://www.cdc.gov/teenpregnancy/about/social-determinants-disparities-teen-pregnancy.htm. Published 2019. Accessed 1 August, 2019.
- Office of Rural Health Policy. List of rural counties and designated eligible census tracts in metropolitan counties. USDA. https://www.hrsa.gov/sites/default/files/ruralhealth/resources/forhpeligibleareas.pdf. Published 2016. Updated 31 December. Accessed 10 February, 2019.
- Power to Decide. Indiana Data 2019. The campaign to prevent unplanned pregnancy. https://powertodecide.org/what-we-do/information/national-state-data/indiana. Published 2019. Accessed 10 April, 2019.
- Power to Decide. National and State Data. The campaign to prevent unplanned pregnancy. https://powertodecide.org/what-we-do/information/national-state-data/national. Published 2019. Accessed 10 April, 2019.
- Indiana State Department of Health. Indiana Natality Report. https://www.in.gov/isdh/reports/natality/2017/tbl30_t.htm. Published 2019. Accessed 10 April, 2019.
- Centers for Disease Control and Prevention. Protective Factors. Department of Health and Human Services. https://www.cdc.gov/healthyyouth/protective/index.htm. Published 2018. Accessed 1 August, 2019.
- Resnick MD, Bearman PS, Blum RW, et al. Protecting adolescents from harm. Findings from the National Longitudinal Study on adolescent health. Jama. 1997;278(10):823–832. doi:10.1001/jama.1997.03550100049038.
- Dombrowski K, Crawford D, Khan B, Tyler K. Current rural drug use in the US Midwest. Journal of Drug Abuse. 2016;2(3):22.
- Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance—United States, 2017. MMWR Surveill Summ. 2018;67(8):1–114. doi:10.15585/mmwr.ss6708a1.
- O’Sullivan LF, Cheng MM, Harris KM, Brooks-Gunn J. I wanna hold your hand: the progression of social, romantic and sexual events in adolescent relationships. Perspect Sexual Reprod Health. 2007;39(2):100–107. doi:10.1363/3910007.
- Giordano PC, Manning WD, Longmore MA. Affairs of the heart: qualities of adolescent romantic relationships and sexual behavior. J Res Adolesc. 2010;20(4):983–1013. doi:10.1111/j.1532-7795.2010.00661.x.
- Miller BC. Family influences on adolescent sexual and contraceptive behavior. J Sex Res. 2002;39(1):22–26. doi:10.1080/00224490209552115.
- Oman RF, Vesely SK, Aspy CB, et al. A longitudinal study of youth assets, neighborhood conditions, and youth sexual behaviors. J Adolesc Health. 2013;52(6):779–785. doi:10.1016/j.jadohealth.2012.12.005.
- Edwards LL, Hunt A, Cope-Barnes D, Hensel DJ, Ott MA. Parent-child sexual communication among middle school youth. J Pediatr. 2018;199:260–262. doi:10.1016/j.jpeds.2018.02.041.
- Yang Z, Gaydos LM. Reasons for and challenges of recent increases in teen birth rates: a study of family planning service policies and demographic changes at the state level. J Adolesc Health. 2010;46(6):517–524. doi:10.1016/j.jadohealth.2010.03.021.
- U.S. Department of Health & Human Services. Teen pregnancy prevention program. Office of Adolescent Health. https://www.hhs.gov/ash/oah/grant-programs/teen-pregnancy-prevention-program-tpp/about/index.html. Published 2019. Updated 7 May. Accessed 11 November, 2019.
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implementation Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50.
- CFIR Research Team-Center for Clinical Management Research. Consolidated Framework for Implementation Research. https://cfirguide.org. Published 2019. Accessed 25 January, 2019.
- CFIR Research Team-Center for Clinical Management Research. Consolidated Framework for Implementation Research—Evaluation design. https://cfirguide.org/evaluation-design/overview/. Published 2019. Accessed 29 July, 2019.
- Albert B, Brown S, Flanigan C. (eds.). 14 & Younger: The Sexual Behavior of Young Adolescents. Washington, D.C.: National Campaign to Prevent Teen Pregnancy; 2003.
- Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006; 3(2):77–101. doi:10.1191/1478088706qp063oa.
- ETR Program Success Center. Draw the line/respect the line! https://www.etr.org/ebi/programs/draw-the-line. Accessed 1 August, 2019.
- Coyle KK, Kirby DB, Marin BV, Gomez CA, Gregorich SE. Draw the line/respect the line: a randomized trial of a middle school intervention to reduce sexual risk behaviors. Am J Public Health. 2004;94(5):843–851. doi:10.2105/AJPH.94.5.843.
- U.S. Department of Health & Human Services. An overview of fidelity monitoring expectations. Office of Adolescent Health. New Grantee Orientation Meeting Web site. https://www.hhs.gov/ash/oah/sites/default/files/ash/oah/oah-initiatives/assets/tpp-grantee-orientation/fidelity_monitoring_expectations.pdf. Published 2015. Updated 16 November. Accessed 11 November, 2019.
- ETR Program Success Center. Making a difference! https://www.etr.org/ebi/programs/making-a-difference/. Accessed 1 August, 2019.
- Jemmott JB, III, Jemmott LS, Fong GT. Abstinence and safer sex HIV risk-reduction interventions for African American adolescents: a randomized controlled trial. Jama. 1998;279(19):1529–1536. doi:10.1001/jama.279.19.1529.
- U.S. Department of Health & Human Services. Sexual Risk Avoidance Education Program (SRAE). https://www.acf.hhs.gov/fysb/resource/srae-facts. Published 2017. Updated 17 February. Accessed 11 November, 2019.
- Index Mundi. Indiana poverty rate by county, 2009. 2013. https://www.indexmundi.com/facts/united-states/quick-facts/indiana/percent-of-people-of-all-ages-in-poverty#table. Accessed 12 December, 2019.
- Indiana State Department of Health. Indiana Natality Report—State and County Data 2013. http://www.in.gov/isdh/reports/natality/2013/index.htm. Published 2015. Accessed 15 March, 2015.
- Janowicz DM. HIV transmission and injection drug use: lessons from the Indiana outbreak. Topics in Antiviral Medicine. 2016;24(2):90.
- Peters PJ, Pontones P, Hoover KW, et al. HIV infection linked to injection use of Oxymorphone in Indiana, 2014–2015. N Engl J Med. 2016;375(3):229–239. doi:10.1056/NEJMoa1515195.
- Indiana State Department of Education. Health and Wellness: 20-30-5-13 Instruction on human sexuality or sexually transmitted diseases. https://www.doe.in.gov/standards/health-and-wellness. Published 2014. Accessed 1 August, 2019.
- The Glossary of Education Reform. Local Control. https://www.edglossary.org/local-control/. Published 2016. Accessed 1 August, 2019.