
Abstract
Currently, the world is facing a global pandemic of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), also known as COVID-19. So far, there are no clear recommendations regarding hospital discharge and aftercare for COVID-19. Here, we briefly discuss the current understanding of recommendations for discharge criteria, discharge treatment regimens, and follow-up.
According to the Centers for Disease Control and Prevention, stable patients with COVID-19 should be discharged from a health care facility based on their clinical condition and in consultation with the clinical care team and local or state public health departments. Although meeting criteria for discontinuation of transmission-based precautions (TBP) is not a prerequisite for discharge from a health care facility, understanding the criteria is a necessary part of the patient’s management after discharge. In patients discharged before discontinuation of TBP, isolation is required until they meet symptom-based strategy criteria for discontinuation of TBP.Citation1
In the symptom-based strategy, patients are stratified based on severity of illness into mild to moderate and severe to critical illness groups. Both groups must have respiratory symptom improvement and at least 24 hours of resolution of fever without the use of antipyretics. Patients with mild to moderate illness must have passed at least 10 days since the first symptoms appeared, while those with severe to critical illness must have passed at least 20 days since symptoms first appeared.Citation1
The test-based strategy for discontinuation of TBP is considered for severely immunocompromised patients in consultation with local infectious diseases experts. Patients are stratified into symptomatic and asymptomatic groups. Both groups must have at least two negative consecutive molecular viral assay tests to detect SARS-CoV-2 RNA respiratory specimens collected ≥24 hours apart. Symptomatic patients must meet two additional requirements: resolution of fever without the use of antipyretics and symptom improvement.Citation1
Patients with TBP discontinued during hospitalization can be discharged without restrictions. If TBP must be continued at home, their ability to adhere to home isolation and the home’s suitability should be considered. For nursing homes and other long-term care facilities, the receiving facility must be able to adhere to infection prevention and control recommendations.
DISCHARGE TREATMENT REGIMENS
Venous thromboembolism prophylaxis
Although the risk of venous thromboembolism (VTE) is markedly increased in COVID-19, the National Institutes of Health (NIH) does not recommend routine postdischarge VTE prophylaxis for patients with COVID-19 (level of evidence: AIII—strong, based on expert opinion).Citation2 However, based on benefits of postdischarge prophylaxis for certain high-risk patients without COVID-19, the Food and Drug Administration (FDA) approved two regimens of direct oral anticoagulants: rivaroxaban 10 mg daily for 31 to 39 days, and betrixaban 160 mg on day 1, followed by 80 mg once daily for 35 to 42 days.Citation2 The trials that studied these regimens required patients to meet one of the following inclusion criteria:
Modified IMPROVE-VTE score ≥4
Modified IMPROVE-VTE score ≥2 and D-dimer level >2 times the upper limit of normal
Age ≥75 years
Age >60 years and D-dimer level >2 times the upper limit of normal
Age 40 to 60 years, D-dimer level >2 times the upper limit of normal, and previous VTE event or cancer
The International Medical Prevention Registry on Venous Thromboembolism (IMPROVE) VTE risk score is a predictive score designed to assess the risk of VTE in hospitalized medical patients.Citation3
A non–FDA-approved regimen of 10 mg of rivaroxaban for 6 weeks can also be adopted.Citation4 The American Society of Hematology even proposed continuing COVID-19 VTE prophylaxis for up to 90 days after discharge.Citation5 Although aspirin has been studied in low-risk patients after hip or knee arthroplasty, it is not recommended in COVID-19 patients due to lack of data regarding its safety and efficacy.Citation6
At hospital discharge, patients must be educated on the signs and symptoms of VTE and advised to seek urgent medical attention should these develop. Postdischarge VTE prophylaxis decisions should be individualized, taking into consideration the patient’s risk factors, including reduced mobility, bleeding risks, and feasibility.
Corticosteroid therapy
Based on data from the Randomized Evaluation of COVID-19 Therapy (RECOVERY) trial, NIH guidelines recommend using dexamethasone 6 mg per day for up to 10 days for the treatment of COVID-19 in patients who are mechanically ventilated (level of evidence: AI—strong, based on ≥1 randomized trial) and in patients who require supplemental oxygen but who are not mechanically ventilated (level of evidence: BI—moderate, based on ≥1 randomized trial). It is advised to continue a course of dexamethasone for 10 days even after discharge in recovered COVID-19 patients who required oxygen during hospital admission.Citation7 On the contrary, NIH guidelines recommend against the use of dexamethasone for COVID-19 cases not requiring supplemental oxygen due to lack of survival benefits and potential harmful effects (AI).Citation7
Oxygen therapy
Although there is no evidence about the beneficial use of oxygen therapy at home in discharged COVID-19 patients, short-term home oxygen therapy may be considered in hypoxemic patients at rest (oxygen saturation <88% on room air). Risks and benefits should be weighed before discharging patients on home oxygen.Citation8
Adjuvant therapies
Some vitamins and minerals such as vitamin C, vitamin D, and zinc have been proposed for use in COVID-19 due to their beneficial antioxidant immunomodulatory effect, but the NIH recommends against using them due to lack of safety and efficacy.Citation9
FOLLOW-UP AFTER DISCHARGE
Patients discharged after COVID hospitalization should follow-up with their primary care physician within 7 days. Face-to-face visits during the pandemic remain logistically difficult due to public safety recommendations and continued TBP. However, recent relaxation of previously cumbersome regulations surrounding telemedicine visits has improved primary care physicians’ opportunity to care for patients. The relaxed regulations allow for similar reimbursement on telephone visits, video visits, and face-to-face visits. We recommend utilizing transitional care management visits for selected Medicare patients. This gives the provider an opportunity to address hand-off between hospital and home while also giving the patient an opportunity to speak with a medical provider within 24 hours of discharge and have a follow-up visit within 7 to 14 days.Citation10 During follow-up, the physician should assess common late sequela of COVID-19 (neurologic, cardiac, VTE), explore the social effect of isolation, and consider the need for follow-up laboratory tests.Citation10
CONCLUSION
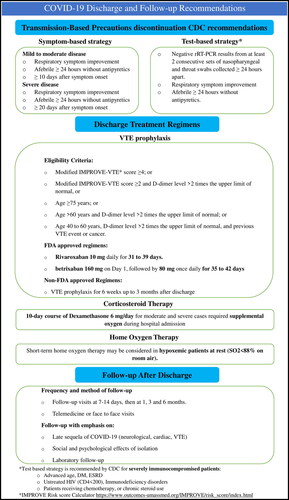
COVID-19 discharge and follow-up recommendations are lacking. As shown in , oxygen therapy is recommended for hypoxemic patients, and completion of a 10-day course of dexamethasone 6 mg and VTE prophylaxis with direct oral anticoagulants for up to 6 weeks are recommended in selected high-risk patients. Follow-up appointments should occur within 7 days and utilize telemedicine when appropriate, focusing on the late medical complications and psychological impact of COVID-19.
Figure 1. Summary of COVID-19 discharge and follow-up recommendations.
- Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19). Updated July 16, 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care.html.
- National Institutes of Health. Antithrombotic therapy in patients with COVID-19. Updated May 12, 2020. https://www.covid19treatmentguidelines.nih.gov/adjunctivetherapy/antithrombotic-therapy/.
- Spyropoulos A, Lipardi C, Xu J, et al. Modified IMPROVE VTE risk score and elevated D-dimer identify a high venous thromboembolism risk in acutely ill medical population for extended thromboprophylaxis. TH Open. 2020;4(1):e59–e65. doi:https://doi.org/10.1055/s-0040-1705137.
- Moores LK, Tritschler T, Brosnahan S, et al. Prevention, diagnosis, and treatment of VTE in patients with coronavirus disease 2019: Chest guideline and expert panel report. Chest. 2020;158(3):1143–1163. doi:https://doi.org/10.1016/j.chest.2020.05.559.
- American Society of Hematology. COVID-19 resources. Updated October 6, 2020. https://www.hematology.org/covid-19.
- Azboy I, Barrack R, Thomas A, et al. Aspirin and the prevention of venous thromboembolism following total joint arthroplasty: commonly asked questions. Bone Joint J. 2017;99-B(11):1420–1430. doi:https://doi.org/10.1302/0301-620X.99B11.BJJ-2017-0337.R2.
- RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in hospitalized patients with Covid-19—preliminary report. N Engl J Med. 2020; NEJMoa2021436. doi:https://doi.org/10.1056/NEJMoa2021436.
- Khor Y, Wong R, McDonald C. Post-hospitalization short-term oxygen therapy: use of a clinical management pathway and long-term follow-up. Respir Care. 2019;64(3):272–278. doi:https://doi.org/10.4187/respcare.06303.
- National Institutes of Health. Adjunctive therapy. Updated July 17, 2020. https://www.covid19treatmentguidelines.nih.gov/adjunctive-therapy/.
- Department of Health and Human Services. Notification of enforcement discretion for telehealth. HHS.gov. March 30, 2020. https://www.hhs.gov/hipaa/for-professionals/special-topics/emergency-preparedness/notification-enforcement-discretion-telehealth/index.html.