
ABSTRACT
Purpose: To determine the prevalence of trachomatous inflammation – follicular (TF) and trichiasis in each of the 20 local government areas (LGAs) of Bauchi State, Nigeria.
Methods: We undertook a population-based prevalence survey in each LGA in Bauchi State, employing the Global Trachoma Mapping Project methodology. We used a 2-stage, systematic and quasi-random sampling strategy. Using probability proportional to size, we selected 25 clusters, in each of which 25 households were selected by random walk. All residents of selected households 1 year and older were examined for TF, trachomatous inflammation – intense, and trichiasis, using the World Health Organization simplified grading scheme.
Results: Only two LGAs in Bauchi State had TF prevalences in 1–9-year-olds over 5%, with none having TF prevalences of 10% or greater. Only one LGA had a trichiasis prevalence in adults below the elimination threshold; all the others had trichiasis at levels suggestive of public health significance. In all 20 LGAs, more than 60% of households were within 1 km of an improved source of water for hygiene.
Conclusion: Efforts need to be made in Bauchi State to provide trichiasis surgery in order to avert trachomatous blindness. Water supplies needs to be sustained and good personal hygiene practices assured so that elimination of trachoma as a public health problem will be achieved and sustained.
Introduction
In Nigeria, 84% of cases of blindness are avoidable, with trachoma responsible for 4% of blindness overall.Citation1 Trachoma is the leading infectious cause of blindness worldwide.Citation2 It can be prevented by implementing the SAFE strategy (surgery for trichiasis, antibiotics to clear infection, and promotion of facial cleanliness and environmental improvement to reduce transmission), as recommended by the World Health Organization (WHO).Citation3 A prerequisite for launching SAFE interventions is an understanding of the local prevalence of disease; specifically the district-level prevalences of trachomatous inflammation – follicular (TF) in children aged 1–9 years, and trachomatous trichiasis in adults aged 15 years and older. This helps to determine which aspects of the SAFE strategy need to be undertaken in each district.Citation4
Bauchi State is located in north-eastern Nigeria; the region with the highest burden of blindness in the country.Citation5 There has been no established trachoma control program and no comprehensive blindness prevention program in the State, in part due to lack of data. Surveys in neighboring Jigawa and Yobe States have indicated that trachoma is a public health problem in contiguous populations.Citation6,Citation7
Since Bauchi State is adjacent to known trachoma endemic areas, we sought to determine the district-level (local government area, LGA) prevalence of trachoma throughout Bauchi, in order to provide government and partners the necessary data required for the establishment of a trachoma control program, if required. This study was conducted as part of the Global Trachoma Mapping Project (GTMP).
Materials and methods
Sample size calculations, field team training and certification protocols, data collection procedures, data processing and analysis techniques all followed GTMP standards, which have been previously published.Citation8 Version 2 of the GTMP training system was used. As described elsewhere (in a companion paper on GTMP outputs for Kano StateCitation9), in Bauchi, for each LGA, we selected 25 households in each of 25 villages, chosen using a 2-stage, systematic and quasi-random sampling strategy. In each selected household, all residents aged 1 year and older were invited to be examined by GTMP-certifiedCitation10 graders for signs of TF, trachomatous inflammation – intense and trichiasis.Citation11 We also collected data on household-level access to water and sanitation, using a combination of questioning adult residents and direct observation.Citation8
Ethics
Following local-language explanation of survey goals and procedures, we obtained verbal consent for examination from this mostly illiterate population, and recorded it electronically in a smartphone application (LINKS system).Citation8,Citation12 Individuals aged over 15 years gave consent for their own participation, and for the participation of children in their care. We offered participants who had clinical evidence of active trachoma two tubes of 1% tetracycline ophthalmic ointment, and told them or a carer how to apply it. Participants with trichiasis were referred to the nearest trained trichiasis surgeon for free lid surgery. Protocols were approved by the Ethics Committee of the London School of Hygiene & Tropical Medicine (reference 6319), the National Health Research Ethics Committee of Nigeria (NHREC/01/01/2007), and the Bauchi State Health Research Ethics Committee (NREC/12/05/2013/4). Bauchi State Ministry of Health also gave administrative permission for the work to proceed.
Data analyses
As described previously,Citation8 data were checked and cleaned by the GTMP Data Manager (RW). To derive LGA-level prevalence estimates, we adjusted TF data for age of participants (in 1-year age bands), and number of participants per cluster, and trichiasis data for age of participants (in 5-year age bands), sex of participants, and number of participants per cluster. The trichiasis backlog in each LGA was calculated by multiplying the prevalence estimate in persons aged 15 years and older by 56% of the total population in the LGA (as determined in the most recent census), because 56% of the Nigerian population is 15 years and older.Citation13
Results
Fieldwork was undertaken from December 2013 to February 2014. In Bauchi State as a whole, a total of 75,843 residents were enumerated in selected households; 71,599 (94%) people were examined, 2841 (4%) were absent on the day that field teams visited, 1348 (2%) refused examination, and 55 (0.1%) could not be examined for various other reasons. The age range of persons enumerated ranged from 1 year to over 100 years. More females (38,888, 54.3%) were examined than males (32,711, 45.7%; ).
Table 1. Age and sex distribution of participants, Global Trachoma Mapping Project, Bauchi State, Nigeria, 2013–2014.
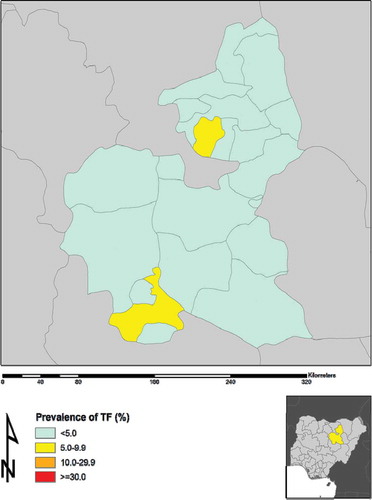
We examined a total of 23,626 children aged 1–9 years. Of these, 12,065 (51.1%) were male. The state-wide crude prevalence of TF in 1–9-year-old males was 1.5% (95% confidence interval, CI, 1.3–1.7%), which was also the prevalence in 1–9-year-old females (odds ratio 1.0, 95% CI 0.8–1.2; p = 1.0). The age-adjusted LGA-level prevalences of TF are shown in and .
Table 2. Local government area-level prevalences of trachomatous inflammation – follicular (TF) and trichiasis, Global Trachoma Mapping Project, Bauchi State, Nigeria, 2013–2014.
Figure 1. Prevalence of trachomatous inflammation – follicular (TF) in 1–9-year-old children, by local government area, Global Trachoma Mapping Project, Bauchi State, Nigeria, 2013–2014.
A total of 31,444 persons aged 15 years and older were examined. Of these, 12,835 (40.8%) were male. The state-wide crude prevalence of trichiasis was 1.9% (95% CI 1.8–2.1%). In males aged ≥15 years crude trichiasis prevalence was 1.4% (95% CI 1.2–1.6%), in females in the same age range it was 2.2% (95% CI 2.0–2.5%). This difference in trichiasis prevalence between adult females and adult males was statistically significant (odds ratio 1.6, 95% CI 1.3–1.9; p < 0.001). and show the LGA-level age- and sex-adjusted prevalences of trichiasis.
Figure 2. Prevalence of trichiasis in adults ≥15 years, by local government area, Global Trachoma Mapping Project, Bauchi State, Nigeria, 2013–2014.
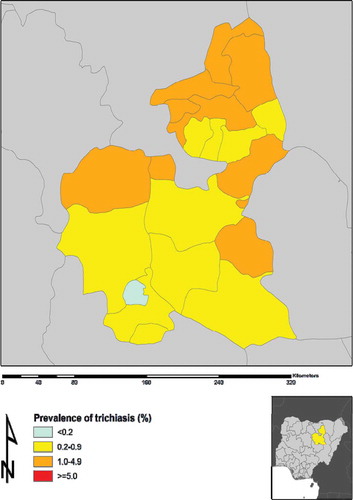
Two LGAs (Shira and Tafawa Balewa) had TF prevalences between 5% and 9.9%. No LGAs had TF prevalences ≥10%. Trichiasis prevalences ranged between 0.1% (Das) and 3.3% (Zaki).
With a population (according to the most recent censusCitation14) of over 4 million people, there is an estimated trichiasis surgery backlog of 28,559 people in Bauchi State, with at least 23,377 surgeries needing to be performed to reach the WHO target for the trichiasis component of “elimination of trachoma as a public health problem”Citation14 in each LGA of Bauchi State. Zaki has the greatest need for provision of trichiasis surgery amongst all Bauchi LGAs ().
Table 3. Local government area-level estimates of trichiasis surgery backlog, Global Trachoma Mapping Project, Bauchi State, Nigeria, 2013–2014.
Access to an improved source of water for hygiene purposes (defined as one which by nature of its construction and proper use adequately protects its contained water from outside contamination) is generally good in Bauchi State. In all 20 LGAs, >60% of households had access to an improved water source within 1 km, and in 15 LGAs (all except Bogoro, Gamawa, Itas-Gadau, Missau and Tafawa Balewa) this was true for >80% of households. Access to improved latrines defined as any latrine facility that hygienically separates human excreta from human contact ranged from approximately 3% in Bogoro to 99% in Missau LGA ().
Table 4. Household access to washing water and improved latrines, by local government area, Global Trachoma Mapping Project, Bauchi State, Nigeria, 2013–2014.
Discussion
In Bauchi State, there is a high prevalence of trichiasis, the potentially blinding stage of trachoma. State-wide, we estimate there are more than 28,000 people with trichiasis; if left untreated, this could progress in each person to cause corneal damage and irreversible visual impairment or blindness. To prevent this number of people from potentially losing vision due to trachoma, urgent scale-up of the surgery component of the SAFE strategy is required. Particular attention should be directed to LGAs (such as Zaki, Katagum, Ningi, and Gamawa) where there are particularly large numbers of persons needing surgery. The trachoma program should trainCitation15 and deploy more trichiasis surgeons to these areas, while not neglecting the other LGAs, because the current contingent of 10 active trichiasis surgeons in Bauchi is inadequate for the size of the task at hand. Deliberate efforts to provide trichiasis surgery close to where people live,Citation16 and to encourage female trichiasis patients to present, are required. Women usually have worse access to trichiasis surgery services, are more afraid of surgery, and are less likely to have been offered surgery in the past.Citation17
Active trachoma is currently not at levels indicative of a public health problem in Bauchi State, with only two LGAs (Shira and Tafawa Balewa) having TF prevalences in 1–9-year-olds of 5% or higher; these two LGAs may benefit from a single round of azithromycin mass drug administration.Citation18 Given that access to improved water for hygiene purposes is high in this state, emphasis on the “E” component of the SAFE strategy here should include maintenance of existing water sources, while continuing to aim for 100% of households having proximate access to water in all communities. Given the low prevalence of TF, relatively high prevalence of TT, and absence of previous specific trachoma control interventions, it is possible that trachoma is already undergoing a secular trend towards elimination in Bauchi.
There is also a need to increase access to improved latrine facilities, with Kirfi, Bogoro and Zaki LGAs being high on the priority list in this regard. There were only two of 20 LGAs in which >80% of households had improved latrine access. These data call for collaboration with water and sanitation agencies to prioritize provision of latrines (or other means of safe disposal of human feces), as part of efforts to achieve United Nations sustainable development goals.Citation19 Latrine provision, in tandem with maintaining good access to water, should greatly assist in eliminating trachoma and other neglected tropical diseases in Bauchi.
Trachoma may be disappearing from Bauchi State, but there is an urgent need for provision of high volume, high quality, community-based trichiasis surgery, and maintenance or further suppression of the (presumed) current low transmission rate of ocular Chlamydia trachomatis infection. Elimination of trachoma as a public health problem here could provide a template for action in similar areas of Nigeria and beyond.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This study was principally funded by the Global Trachoma Mapping Project (GTMP) grant from the United Kingdom’s Department for International Development (ARIES: 203145) to Sightsavers, which led a consortium of non-governmental organizations and academic institutions to support ministries of health to complete baseline trachoma mapping worldwide. The GTMP was also funded by the United States Agency for International Development (USAID) through the ENVISION project implemented by RTI International under cooperative agreement number AID-OAA-A-11-00048, and the END in Asia project implemented by FHI360 under cooperative agreement number OAA-A-10-00051. A committee established in March 2012 to examine issues surrounding completion of global trachoma mapping was initially funded by a grant from Pfizer to the International Trachoma Initiative. AWS was a Wellcome Trust Intermediate Clinical Fellow (098521) at the London School of Hygiene & Tropical Medicine. None of the funders had any role in project design, in project implementation or analysis or interpretation of data, in the decisions on where, how or when to publish in the peer reviewed press, or in preparation of the manuscript.
Additional information
Funding
Related Research Data
References
- Abdull MM, Sivasubramaniam S, Murthy, et al. Causes of blindness and visual impairment in Nigeria: The Nigeria National Blindness and Visual impairment Survey. Inv Ophthalmol Vis Sci 2009;50:4114–4120.
- Bourne RR, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Glob Health 2013;1:e339–349.
- World Health Assembly. Global elimination of blinding trachoma. 51st World Health Assembly, Geneva, 16 May 1998, Resolution WHA51.11. Geneva: World Health Organization, 1998.
- Solomon AW, Zondervan M, Kuper H, et al. Trachoma control: a guide for program managers. Geneva: World Health Organization, 2006.
- Kyari F, Murthy GVS, Sivsubramaniam S, et al. Nigeria National Blindness and Visual impairment study group. Prevalence of blindness and visual impairment in Nigeria: The National Blindness and Visual Impairment Survey. Inv Ophthalmol Vis Sci 2009;50:2033–2039.
- Ramyil A, Wade P, Ogoshi C, et al. Prevalence of trachoma in Jigawa state, Northwestern Nigeria. Ophthalmic Epidemiol 2015;22:184–189.
- Mpyet C, Ogoshi C, Goyol M. Prevalence of trachoma in Yobe state, north eastern Nigeria. Ophthalmic Epidemiol 2008;15:303–307.
- Solomon AW, Pavluck A, Courtright P, et al. The Global Trachoma Mapping Project: methodology of a 34-country population-based study. Ophthalmic Epidemiol 2015;22:214–225.
- Mpyet C, Muhammad N, Adamu MD, et al. Prevalence of trachoma in Kano state, Nigeria: results of 44 local government area-level surveys. Ophthalmic Epidemiol. doi:10.1080/09286586.2016.1265657
- Courtright P, Gass K, Lewallen S, et al. Global trachoma mapping project: training for mapping of trachoma ( version 3), 2015. [ Available at: http://www.trachomacoalition.org/resources/global-trachoma-mapping-project-training-mapping-trachoma]. London: International Coalition for Trachoma Control.
- Thylefors B, Dawson CR, Jones BR, et al. A simple system for the assessment of trachoma and its complications. Bull World Health Organ 1987;65:477–483.
- Pavluck A, Chu B, Mann Flueckiger R, et al. Electronic data capture tools for global health programs: evolution of LINKS, an Android-, web-based system. PLoS Negl Trop Dis 2014;8:e2654.
- National Population Commission. 2006 population and housing census of the Federal Republic of Nigeria: national and state population and housing tables, priority tables (volume 1). Abuja: National Population Commission, 2009.
- World Health Organization. Report of the 3rd global scientific meeting on trachoma, Johns Hopkins University, Baltimore, MA, 19–20 July 2010. Geneva: World Health Organization, 2010.
- Merbs S, Resnikoff S, Kello AB, et al. Trichiasis surgery for trachoma (2nd ed). Geneva: World Health Organization, 2013.
- Bowman RJ, Soma OS, Alexander N, et al. Should trichiasis surgery be offered in the village? A community randomised trial of village vs. health centre-based surgery. Trop Med Int Health 2000;5:528–533.
- Rajak SN, Habtamu E, Weiss HA, et al. Why do people not attend for treatment for trachomatous trichiasis in Ethiopia? A study of barriers to surgery. PLoS Negl Trop Dis 2012;6(8):e1766.
- World Health Organization. Meeting Report: Technical Consultation on Trachoma Surveillance. Decatur, GA, USA. Geneva: World Health Organization, 2014.
- United Nations General Assembly. Resolution adopted by the General Assembly on 25 September 2015 ( A/70/L.1). Transforming our world: the 2030 agenda for sustainable development. New York: United Nations, 2015.
Appendix
The Global Trachoma Mapping Project Investigators are: Agatha Aboe (1,11), Liknaw Adamu (4), Wondu Alemayehu (4,5), Menbere Alemu (4), Neal D. E. Alexander (9), Berhanu Bero (4), Simon J. Brooker (1,6), Simon Bush (7,8), Brian K. Chu (2,9), Paul Courtright (1,3,4,7,11), Michael Dejene (3), Paul M. Emerson (1,6,7), Rebecca M. Flueckiger (2), Allen Foster (1,7), Solomon Gadisa (4), Katherine Gass (6,9), Teshome Gebre (4), Zelalem Habtamu (4), Danny Haddad (1,6,7,8), Erik Harvey (1,6,10), Dominic Haslam (8), Khumbo Kalua (5), Amir B. Kello (4,5), Jonathan D. King (6,10,11), Richard Le Mesurier (4,7), Susan Lewallen (4,11), Thomas M. Lietman (10), Chad MacArthur (6,11), Colin Macleod (3,9), Silvio P. Mariotti (7,11), Anna Massey (8), Els Mathieu (6,11), Siobhain McCullagh (8), Addis Mekasha (4), Tom Millar (4,8), Caleb Mpyet (3,5), Beatriz Muñoz (6,9), Jeremiah Ngondi (1,3,6,11), Stephanie Ogden (6), Alex Pavluck (2,4,10), Joseph Pearce (10), Serge Resnikoff (1), Virginia Sarah (4), Boubacar Sarr (5), Alemayehu Sisay (4), Jennifer L. Smith (11), Anthony W. Solomon (1,2,3,4,5,6,7,8,9,10,11), Jo Thomson (4); Sheila K. West (1,10,11), Rebecca Willis (2,9).
Key: (1) Advisory Committee, (2) Information Technology, Geographical Information Systems, and Data Processing, (3) Epidemiological Support, (4) Ethiopia Pilot Team, (5) Master Grader Trainers, (6) Methodologies Working Group, (7) Prioritisation Working Group, (8) Proposal Development, Finances and Logistics, (9) Statistics and Data Analysis, (10) Tools Working Group, (11) Training Working Group.