
ABSTRACT
Purpose: To complete the baseline trachoma map of Sudan by estimating the prevalence of trachoma and associated risk factors in the five Darfur States and Khartoum State.
Methods: Using a standardized methodology developed for the Global Trachoma Mapping Project, we undertook a cross sectional, community-based survey in each of 32 evaluation units (EUs) covering all accessible districts.
Results: We enumerated a total of 84,568 individuals, with 73,489 people (86.9%) examined from 20,242 households in 908 villages. The highest prevalence of trachomatous inflammation – follicular (TF) in children was found in El Fashir district (18.7%), and the lowest in El Malha district (0.0%). Five districts (El Fashir, Zalinji, Azoom, Maleet, and El Koma) were in the three EUs that had TF prevalences above the 10% threshold at which the World Health Organization recommends mass treatment with azithromycin, together with facial clean3liness and environmental improvement interventions, for at least 3 years. The highest trachomatous trichiasis prevalence in adults was found in the EU composed of Forbranga and Habillah (1.2%), and the lowest in the EU composed of As-salam and Belale districts in South Darfur (0.0%). TF in children was independently associated with younger age, unimproved sanitation in the household, having ≥5 children in the household, outside annual maximum temperatures <40°C, and living in an internally displaced persons camp.
Conclusion: We found a high prevalence of trachoma in some areas of Darfur, but in general the prevalence throughout Darfur and Khartoum was low.
Introduction
Trachoma is an ocular disease caused by infection with Chlamydia trachomatis, and is the major infectious cause of blindness worldwide. It is estimated to be responsible for 1.4% of global blindness.Citation1 Since 1993, the World Health Organization (WHO) has advocated the SAFE strategy (surgery, antibiotics, facial cleanliness and environmental improvement) for trachoma control and elimination.Citation2 Implementation of the SAFE strategy is undertaken at district level, with thresholds of disease prevalence used to determine which districts qualify for interventions. Population-based prevalence surveys are the gold standard for estimating prevalence of trachoma in populations and are therefore essential for program planning, implementation, monitoring and evaluation.Citation3
Trachoma has long been known to be prevalent in the Sudan. A report by MacCallan in 1934 documented trachoma among school pupils in Khartoum and Nubia (north of Wadi Halfa).Citation4 Surveys undertaken by WHO in Atbara Town and surrounding villages of Northern State between 1963 and 1964 revealed trachoma to be a serious public health problem.Citation5 In 1975, a retrospective review of Ministry of Health records dating from 1959 to 1969 found that the highest national incidence of active trachoma was in Northern State, with a decreasing incidence moving southwards through Sudan; there were 83 cases per 1000 total population in Northern State, decreasing to 0.23 per 1000 total population in Bahr El Gazal.Citation6 In addition, the 1975 study again surveyed children in the rural areas surrounding Atbara Town and found signs of trachoma in 71% of children aged 1–4 years.Citation6 While this illustrates the historical presence of trachoma in Sudan, the studies cited used diagnostic criteria which differ from the current WHO simplified trachoma grading system,Citation7 and reflect a pattern of disease that may no longer be relevant.
A survey of 14 villages in Wadi Halfa (Northern State) in 2000 that used the WHO simplified trachoma grading system estimated the prevalence of TF and/or trachomatous inflammation – intense to be 47% among children aged 1–10 years, while 4% of women aged over 40 years had trachomatous trichiasis (TT), confirming that trachoma continued to pose a serious public health problem.Citation8 A survey covering all states of Sudan, with the exception of Darfur and Khartoum, was conducted from 2006 to 2010. Published results showed the district-level prevalence of TF in children aged 1–9 years ranged from 0.0% to 19.8%.Citation9 TF prevalence was above 10% in three districts; two in Blue Nile State (Geissan and Kurmuk), and one in Gederaf State (El Galabat East). A total of 11 districts had TF prevalences between 5.0% and 9.9%, including Dongola in Northern State, Port Sudan and Sawaken in Red Sea State, El Fashga, El Rahd, Gedaref and Gorisha in Gedaref State, El Jabalian in White Nile State, Eldindir in Sinnar State, Baw in Blue Nile State, and Abu Jubaiyeh in South Kordufan State. The district-level prevalence of TT in adults aged 15 years and older ranged from 0.0% to 6.7%. TT prevalence was above 1% in 20 districts (which included the three districts with TF prevalence >10%).
We carried out population-based prevalence surveys in all secure and accessible districts in Darfur (July 2014 to February 2015) and Khartoum State (May 2015; ) that had not previously been surveyed for trachoma, in order to complete the baseline trachoma map of Sudan. This paper presents the findings of those surveys and explores possible risk factors associated with trachoma in these states of Sudan.
Figure 1. States with baseline trachoma mapping, Global Trachoma Mapping Project, Sudan, 2014–2015.

Materials and methods
Survey design, training and implementation were carried out with standard Global Trachoma Mapping Project (GTMP) methodologies.Citation10 Surveys were carried out at the level of evaluation units (EUs), which comprised contiguous grouped districts of total population up to 200,000 inhabitants. Existing administrative boundaries were followed insofar as was possible. Insecurity and/or inaccessibility were exclusion criteria for districts and villages. Regular contact was maintained with local authorities as the security situation could change quickly. Villages were considered inaccessible if teams would have to walk more than half a day to reach them.
Trachoma graders and data recorders were required to attend a 4-day training course in Khartoum State, in which they were familiarized with the overall GTMP methodologyCitation10 and grading of trachoma using the WHO simplified trachoma grading system.Citation7,Citation11 Both graders and recorders were required to pass an examination to be considered for inclusion in field teams. Graders were Sudanese ophthalmology residents or ophthalmic medical assistants. Data recorders were all Sudanese public health officers. Version 3 of the GTMP training system was used.Citation10
Using a design effect of 2.65, the estimated sample size required to estimate a TF prevalence of 10% in children aged 1–9 years with a precision of ± 3% and 95% confidence, and an estimated non-response rate of 20%, 1222 children were required to be sampled.Citation10 The latest census data estimated that there were 2.1 children aged 1–9 years per household in Sudan. It was estimated that teams could survey 30 households per day, and would therefore see an average of 30 × 2.1 = 63 children per day. The number of villages required to be surveyed was therefore 1222/63 = 19.4, rounded up to 20 villages in total per EU.
A 2-stage sampling methodology was used, with villages used as the primary sampling unit. Villages were systematically selected from the latest available census list, with a probability proportional to their population size. To do this, all villages in the EU were listed in an arbitrary order with the village population and the cumulative population to that point. The sampling interval was calculated by dividing the total population by the number of villages to be selected. The first village was selected by generating a random number (n) in the range 0 < n ≤ 1, multiplying this by the sampling interval, and identifying the village in which this number fell. Subsequent villages were then selected by addition of the sampling interval to this first number, and identifying the corresponding village each time, until 20 villages had been selected.Citation12
On the day of the survey, villages were divided into quarters and one village quarter was selected by drawing lots. A total of 30 households were included. If not enough houses were found in the selected quarter, additional households were added from the next quarter until 30 households were approached. All households in the selected quarter were invited to participate in the survey.
Data collection
All data were collected using a custom-made application (LINKS, Taskforce for Global Health, Atlanta, GA, USA) on Android smartphones. Each participant was examined for the presence or absence of the clinical signs TF, trachomatous inflammation – intense and TT, using the WHO simplified trachoma grading system;Citation7,Citation11 TT was defined as trichiasis plus trachomatous conjunctival scarring in the same eye. Recorders were trained to collect household-level WASH (water, sanitation and hygiene) variablesCitation10 using direct observation and by focused interview with the household head. Global positioning system (GPS) coordinates were recorded at each household. Internally displaced person (IDP) camps in the Darfur States are generally established, long-term settlements recognized in local census lists, and were therefore included in the survey sampling frame. Each cluster was recorded as IDP or non-IDP at the time of sampling.
Environmental risk factors
Climatic risk factor data were collected based on existing knowledge about the epidemiology of trachoma. Altitude was collected directly at the time of survey by GPS localization at each household. Climate variables derived from local meteorological stations were obtained from WorldClim BioClim variables (worldclim.org), at a resolution of 2.5 arc-minutes (~5 km).Citation13 Variables were chosen that were considered to be potentially relevant to ocular C. trachomatis transmission, including mean annual precipitation and maximum temperature in the hottest month. Point values were extracted using ArcGIS 10.3 from cluster-level mean-household GPS coordinates.
Statistical analysis
We used projected 2015 populations from the 2008 Sudan census report.Citation14 The cluster-level proportion of TF cases was adjusted in 1-year age groups. The cluster-level proportion of TT cases was adjusted for sex and age in 5-year age groups. The adjusted EU-level prevalence of each outcome was calculated as the mean of all adjusted cluster-level proportions. Proportions were adjusted using R 3.0.2 (2013, The R Foundation for Statistical Computing, Vienna, Austria). Confidence intervals (CIs) were calculated by bootstrapping the adjusted cluster-level proportions of each outcome and taking the 2.5th and 97.5th centiles of all ordered results.Citation15 Risk factor analysis was carried out in Stata 10.2 (Stata Corp, College Station, TX, USA). A 2-level hierarchical model was used with adjustment for clustering at village and household level. Univariable associations were considered for inclusion in the multivariable model if p ≤ 0.05 (Wald’s test).
Ethics approval
The survey protocol was approved by the Sudanese Federal Ministry of Health ethics committee as an amendment to an existing (2006) protocol in which trachoma prevalence surveys were approved throughout Sudan. The overall GTMP methodology was approved by the London School of Hygiene & Tropical Medicine Research Ethics Committee (references 6319 and 8355).
Verbal consent was obtained from all participants and recorded electronically. For those under 15 years of age, consent from a parent or guardian was required. Participants were free to withdraw consent at any time without consequence. All participants found to have clinical signs of active trachoma were offered either oral azithromycin or topical 1% tetracycline. All participants found to have TT or other significant ocular pathology were referred to the nearest ophthalmology center using a pre-agreed referral procedure.
Results
A total of 84,568 individuals were enumerated within 32 EUs covering 45 administrative districts. Overall, 37 districts (27 EUs) were in Darfur States, and six districts (5 EUs) were in Khartoum State. A total of 16,176 individuals were enumerated in Khartoum State, and 68,392 in Darfur State. Overall, 73,489 of those enumerated (86.9%) were present and consented to examination in 20,242 households of 676 villages and 43,761 of those examined were female (59.6%). A total of 34,181 children aged 1–9 years were examined, with a total of 1514 cases of TF identified (4.1%) whilst 33,316 participants over 14 years of age were examined and a total of 330 cases of TT identified (1.0%). The characteristics of those sampled are shown in .
Table 1. Characteristics of sample population, Global Trachoma Mapping Project, Sudan, 2014–2015.
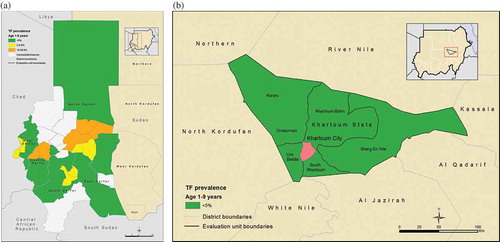
The mean adjusted TF prevalence in children aged 1–9 years over all EUs was 3.9% (95% CI 1.6–5.4%), with the highest prevalence found in El Fashir district of North Darfur (18.7%, 95% CI 13.1–26.5%), and the lowest found in El Malha district of North Darfur (0.0%, 95% CI 0.0–0.3%). Twenty five EUs had a TF prevalence below 5%, four EUs had a TF prevalence from 5–9.9%, and three EUs had a TF prevalence above 10%. The districts El Fashir, Zalinji, Azoom, Maleet and El Koma were all in EUs with TF above the 10% threshold at which WHO recommends mass treatment with azithromycin, plus implementation of the F and E components of SAFE, for three years or more before re-survey (, ).
Table 2. Trachomatous inflammation – follicular (TF) in children aged 1–9 years, Global Trachoma Mapping Project, Sudan, 2014–2015.
Figure 2. (a) Prevalence of trachomatous inflammation – follicular (TF) in 1–9-year-olds by evaluation unit in selected Darfur districts, Global Trachoma Mapping Project, Sudan, 2014–2015. (b) Prevalence of trachomatous inflammation – follicular (TF) in 1–9-year-olds by evaluation unit in Khartoum, Global Trachoma Mapping Project, Sudan, 2014–2015.
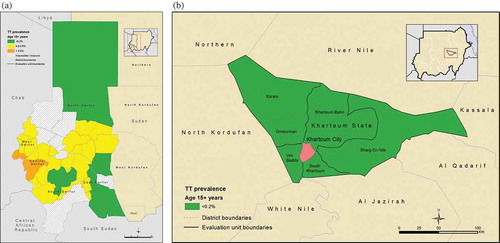
The mean adjusted TT prevalence over all EUs was 0.4% (95% CI 0.1–0.7%), with the highest prevalence found in the EU composed of Forbranga and Habillah (1.2%, 95% CI 0.8–1.7%), and the lowest prevalence found in the EU composed of As-salam and Belale districts in South Darfur, where no cases of TT were found among 997 adults examined (, ).
Table 3. Trachomatous trichiasis (TT) in those ≥15 years, Global Trachoma Mapping Project, Sudan, 2014–2015.
Figure 3. (a) Prevalence of trachomatous trichiasis (TT) in ≥15-year-olds by evaluation unit in selected Darfur districts, Global Trachoma Mapping Project, Sudan, 2014–2015. (b) Prevalence of trachomatous trichiasis (TT) in ≥15-year-olds by evaluation unit in Khartoum, Global Trachoma Mapping Project, Sudan, 2014–2015.
IDP camps made up 36 (5.3%) of the 676 clusters surveyed. This represented 4556 individuals and 1080 households from the total sampled in all EUs. These 36 camps were sampled as part of 10 EUs covering 13 districts; 7 camps were in North Darfur, 13 were in South Darfur, 3 were in East Darfur, and 10 were in West Darfur.
Factors associated with TF
Univariable associations with TF are shown in . In the final multivariable model, TF in children aged 1–9 years was independently associated with age being 1–4 years (odds ratio, OR, 1.8, 95% CI 1.6–2.1) compared to being 5–9 years of age, the use of an unimproved form of sanitation (OR 1.5, 95% CI 1.2–1.9), 5 or more children resident in the household (OR 1.2, 95% CI 1.0–1.4), and living in an IDP camp (OR 2.6, 95% CI 2.2–2.9). A protective effect was associated with living in an area where the maximum annual temperature was ≥40°C (OR 0.4, 95% CI 0.2–0.4). Full results are shown in .
Table 4. Univariable association with the outcome trachomatous inflammation – follicular (TF) in children aged 1–9 years, Global Trachoma Mapping Project, Sudan, 2014–2015.
Table 5. Univariable association with the outcome trachomatous trichiasis (TT) in those aged ≥15 years, Global Trachoma Mapping Project, Sudan, 2014–2015.
Table 6. Multilevel multivariable association with the outcome trachomatous inflammation – follicular in children aged 1–9 years, Global Trachoma Mapping Project, Sudan, 2014–2015.
Factors associated with TT
Univariable associations with TT are shown in . In the final multivariable model, TT in those aged 15 years and older was strongly associated with increasing age in years (OR 1.09, 95% CI 1.08–1.09; included as 10-year age bands in the final model), and female sex (OR 3.0, 95% CI 2.2–3.9)]. Living in an area where the maximum annual temperature was ≥40°C (OR 0.2, 95% CI 0.1–0.3)] had a protective association. Similarly, living in an area where the annual rainfall was <500 mm (the definition of a desert) was associated with a decreased odds of TT (OR 0.2, 95% CI 0.1–0.4). In contrast to the TF findings, there was no association between TT and living in an IDP camp (p = 0.27, likelihood ratio test on the final model). Full results are shown in .
Table 7. Multilevel multivariable association with the outcome trachomatous trichiasis in adults aged ≥15 years, Global Trachoma Mapping Project, Sudan, 2014–2015.
Age-specific TF prevalence
The age-specific TF prevalence in those aged 1–9 years is shown in . The prevalence of TF varied with age, with a peak at age 3 years of 6.3% (95% CI 5.7–7.1%), and a steep decrease to a minimum of 1.8% (95% CI 1.4–2.3%) at 8 years. This difference was highly statistically significant (χCitation2 test for difference in proportions p < 0.001). This relationship was maintained in the Darfur data when evaluated alone ( [lower left]; χCitation2 p < 0.01), but not in the data from Khartoum ( [lower right]) where there was no significant difference across the ages (χCitation2 p = 0.38).
Figure 4. Age-specific prevalence of trachomatous inflammation – follicular (TF) in 1–9-year-olds in 32 evaluation units (EUs) (upper panel). In 27 EUs, Darfur States only (lower, left); and in 5 EUs, Khartoum State only (lower, right), Global Trachoma Mapping Project, Sudan, 2014–2015.
Age and sex-specific TT prevalence
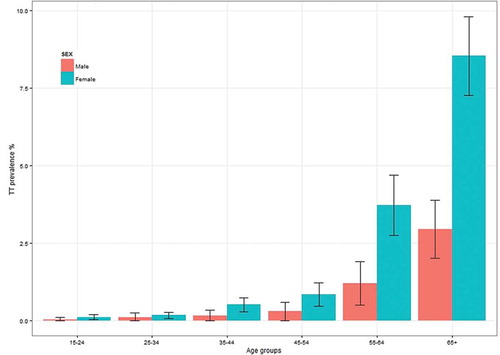
The age- and sex-specific TT prevalence in those aged 15 years and older is shown in . The prevalence of TT increased with age, with the highest prevalence in those aged 65 years and older. In all age groups, the prevalence of TT was higher in females than males, with a statistically significant difference at the p < 0.05 level in the age groups 55–64 years and ≥65 years (χCitation2 test for difference in proportions). In the ≥65 years age group, the prevalence of TT in females was 8.3% (95% CI 6.9–9.9%) and 2.3% in males (95% CI 1.5–3.8%).
Figure 5. Age- and sex-specific prevalence of trachomatous trichiasis (TT) in ≥15-year-olds in 32 evaluation units of Darfur and Khartoum states, Global Trachoma Mapping Project, Sudan, 2014–2015.
Discussion
We found a high prevalence of TF in children in some areas of Darfur, but in general, the prevalence throughout Darfur was low. In addition, the prevalence of TF in children in all areas surrounding Khartoum City was low. In contrast, the prevalence of TT was above the elimination threshold of 0.2% in those aged ≥15 years in the majority of areas surveyed, in both the Darfur States and Khartoum. In Darfur, the three EUs (five districts) in which TF prevalence in children was ≥10% were found in North Darfur and Central Darfur State. In these areas, WHO recommends mass drug administration (MDA) with azithromycin, together with implementation of the F and E components of SAFE, for 3 years before impact surveys are conducted. No districts in East Darfur, South Darfur, or West Darfur were above this 10% TF threshold. However, four districts had TF prevalences close to this level; Kalmando and Dar El Salam (9.3%), El Jinaina (8.8%), and Beda (9.9%), for which current guidelines recommend that these areas should have 1 year of MDA, in addition to F and E, before being re-surveyed to assess the impact. The decision to limit MDA to populations with a prevalence of TF ≥5% is based on consensus opinion that at lower prevalences, populations are unlikely to be at high risk of developing the permanent scarring associated with progression of trachomatous disease. This progression potential may be difficult to determine from a cross-sectional prevalence of TF, because it takes many years for trachomatous scarring to develop, and it is unknown if transmission here is in steady-state, increasing, or decreasing. Interestingly, despite the mean TT prevalence over all districts being 0.4%, the prevalence of TT in each of the districts close to the 10% TF threshold was 0.6%, 0.5%, and 1.0%, respectively. This supports the idea that the transmission of infection has decreased in recent years, perhaps as a result of an increased awareness about trachoma, improved personal hygiene, or because of general socioeconomic development.
In Khartoum State, all five mapped EUs had TF prevalences in children <5%. In fact, four out of five EUs had TF prevalences <2%, and all had TT prevalences <0.2% in those aged 15 years and older. Together, this information suggests that blinding trachoma is unlikely to be a public health problem in Khartoum State.
Consistent with data from elsewhere, we found higher odds of TF in younger children.Citation16–Citation20 No association was found between sex and TF, although such an association is occasionally reported.Citation18,Citation21,Citation22 We included sex in the risk factor analysis a priori. At the household level, the use of an unimproved source of sanitation was independently associated with TF but not TT. Poor sanitation has been linked to trachoma in the literature.Citation23–Citation25 The eye-seeking Musca sorbens flies that can passively transmit C. trachomatis preferentially breed on human feces deposited on the ground, and even basic pit latrines are thought to limit their breeding potential.Citation26,Citation27 However, reported open defecation by household adults was not independently associated with TF or TT. This may be explained by more subtle cultural practices related to hygiene. As ocular C. trachomatis is also spread by direct contact between humans, the frequency of such interactions is likely to play a role in levels of endemicity.
Living in an area where the maximum temperature annually exceeds 40°C was protective for both TF and TT. Living in a household in a desert area was protective for TT (but not TF). High temperatures and higher rainfall have previously been associated with reduced prevalence,Citation28 thought to be mediated through decreased fly breeding potential. Temperatures above 40°C have previously been shown to limit the ability of M. sorbens flies to breed.Citation29
After accounting for other risk factors, we found independently higher odds of TF in children who lived in IDP camps. In and of itself, this may not be surprising, as conflict-related settlements have previously been associated with an increased risk of infectious disease such as measles, hepatitis A, cholera, meningococcal meningitis and polio.Citation30–Citation32 The association here persisted after accounting for proximity to water, the use of surface water as a washing source, household use of unimproved latrines, temperature and yearly rainfall, and so the reason for this additional risk is unclear. It might be that there are hygiene or cultural practices for which we have not accounted, or that surrogates for low socioeconomic status (such as a low levels of education in general) play a part. It’s also possible that the overall density of households in such camps is higher and so C. trachomatis transmission is more readily facilitated, but we did not account for this in our analysis.
In contrast, there was no association between TT in adults and living in an IDP camp. The mean age of those examined in IDP camps was not different from that of non-IDP subjects. It is possible that individuals with TT might not have been able to travel during the displacement. Alternatively, the number of resultant cases of TT might be higher in IDPs, but the life expectancy of those cases markedly reduced, so that fewer are found overall than might be expected from the high proportions of TF seen in children. However, although the absolute numbers were small (17 IDP TT cases, 317 non-IDP TT cases), the mean age of IDP TT cases was not significantly different from non-IDP TT cases (67.6 years, 95% CI 56.1–79.2 years vs 63.4 years 95% CI 61.4–65.3 years); IDP TT cases were (non-significantly) older overall. The association between trachoma and IDP camps warrants further investigation. We note that a limitation in each of our models, which were intended as exploratory analyses, is that we have not adjusted for multiple comparisons.
Although our surveys were based on clinical examination alone and did not include a laboratory component to look for evidence of C. trachomatis,Citation33 the data conform with WHO recommendationsCitation12 for guiding programs and partners to plan interventions against trachoma. These data represent a significant step forwards towards pursuing the elimination of trachoma from Sudan.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This study was principally funded by the Global Trachoma Mapping Project (GTMP) grant from the United Kingdom’s Department for International Development (ARIES: 203145) to Sightsavers, which led a consortium of non-governmental organizations and academic institutions to support ministries of health to complete baseline trachoma mapping worldwide. The GTMP was also funded by the United States Agency for International Development (USAID), through the ENVISION project implemented by RTI International under cooperative agreement number AID-OAA-A-11-00048, and the END in Asia project implemented by FHI360 under cooperative agreement number OAA-A-10-00051. A committee established in March 2012 to examine issues surrounding completion of global trachoma mapping was initially funded by a grant from Pfizer to the International Trachoma Initiative. AWS was a Wellcome Trust Intermediate Clinical Fellow (098521) at the London School of Hygiene & Tropical Medicine, and is now an employee of the World Health Organization (WHO); the views expressed in this article are the views of the authors alone and do not necessarily reflect the views or policy of WHO. None of the funders had any role in project design, in project implementation or analysis or interpretation of data, in the decisions on where, how or when to publish in the peer-reviewed press, or in preparation of the manuscript.
Additional information
Funding
References
- Bourne RRA, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Glob Heal 2013;1:e339–49.
- Francis V, Turner V. Achieving community support for trachoma control (WHO/PBL/93.36). Geneva: World Health Organization, 1993.
- Smith JL, Sturrock HJW, Olives C, et al. Comparing the performance of cluster random sampling and integrated threshold mapping for targeting trachoma control, using computer simulation. PLoS Negl Trop Dis 2013;7:e2389.
- MacCallan AF. Trachoma in the British Colonial Empire – its relation to blindness, the existing means of relief, means of prophylaxis. Br J Ophthalmol 1934;18:625–645.
- Majcuk JF. A study of trachoma and associated infections in the Sudan. Bull World Health Organ 1966;35:262–272.
- Salim AR, Sheikh HA. Trachoma in the Sudan. An epidemiological study. Br J Ophthalmol 1975;59:600–604.
- Thylefors B, Dawson CR, Jones BR, et al. A simple system for the assessment of trachoma and its complications. Bull World Health Organ 1987;65:477–483.
- World Health Organization (WHO). Report of the 5th meeting of the WHO alliance for the global elimination of blinding trachoma: Geneva, 5–7 December, 2000.
- Hassan A, Ngondi JM, King JD, et al. The prevalence of blinding trachoma in northern states of Sudan. PLoS Negl Trop Dis 2011;5.
- Solomon AW, Pavluck A, Courtright P, et al. The Global Trachoma Mapping Project: methodology of a 34-country population-based study. Ophthalmic Epidemiol 2015;22:214–225.
- Solomon AW, Peeling RW, Foster A, et al. Diagnosis and assessment of trachoma. Clin Microbiol. Rev 2004;17:982–1011, table of contents.
- Solomon A, Zondervan M, Kuper H, et al. Trachoma control: a guide for programme managers. Geneva: World Health Organization, 2006.
- Hijmans RJ, Cameron SE, Parra JL, et al. Very high resolution interpolated climate surfaces for global land areas. Int J Climatol 2005;25:1965–1978.
- Central Bureau of Statistics. Sudan Census Report 2008 – Total population expected to States for the period 2009–2018; 2013.
- Carpenter J, Bithell J. Bootstrap confidence intervals: when, which, what? A practical guide for medical statisticians. Stat Med 2000;19:1141–1164.
- Abdou A, Nassirou B, Kadri B, et al. Prevalence and risk factors for trachoma and ocular Chlamydia trachomatis infection in Niger. Br J Ophthalmol 2007;91:13–17.
- Cajas-Monson LC, Mkocha H, Muñoz B, et al. Risk factors for ocular infection with Chlamydia trachomatis in children 6 months following mass treatment in Tanzania. PLoS Negl Trop Dis 2011;5.
- Harding-Esch EM, Edwards T, Sillah A, et al. Risk factors for active trachoma in The Gambia. Trans R Soc Trop Med Hyg 2008;102.
- Kalua K, Chirwa T, Kalilani L, et al. Prevalence and risk factors for trachoma in central and southern Malawi. PLoS One 2010;5.
- Ketema K, Tiruneh M, Woldeyohannes D, et al. Active trachoma and associated risk factors among children in Baso Liben District of East Gojjam, Ethiopia. BMC Public Health 2012;12.
- Golovaty I, Jones L, Gelaye B, et al. Access to water source, latrine facilities and other risk factors of active trachoma in Ankober, Ethiopia. PLoS One 2009;4.
- Yalew KN, Mekonnen MG, Jemaneh AA. Trachoma and its determinants in Mojo and Lume districts of Ethiopia. Pan Afr Med J 2012;13:1–8.
- Emerson PM, Lindsay SW, Alexander N, et al. Role of flies and provision of latrines in trachoma control: cluster-randomised controlled trial. Lancet 2004;363:1093–1098.
- Prüss A, Mariotti SP. Preventing trachoma through environmental sanitation: a review of the evidence base. Bull World Health Organ 2000;78:258–266.
- Stocks ME, Ogden S, Haddad D, et al. Effect of water, sanitation, and hygiene on the prevention of trachoma: a systematic review and meta-analysis. PLoS Med 2014;11.
- Emerson PM, Bailey RL. Trachoma and fly control. Community Eye Heal J 1999;12:57.
- Emerson PM, Simms VM, Makalo P, et al. Household pit latrines as a potential source of the fly Musca sorbens – a one year longitudinal study from The Gambia. Trop Med Int Health 2005;10:706–709.
- Ramesh A, Kovats S, Haslam D, et al. The impact of climatic risk factors on the prevalence, distribution, and severity of acute and chronic trachoma. PLoS Negl Trop Dis 2013;7.
- Hägi M, Schémann J-F, Mauny F, et al. Active trachoma among children in Mali: clustering and environmental risk factors. PLoS Negl Trop Dis 2010;4.
- Lam E, McCarthy A, Brennan M. Vaccine-preventable diseases in humanitarian emergencies among refugee and internally-displaced populations. Hum Vaccin Immunother 2015;11:2627–2636.
- Oral cholera vaccine campaign among internally displaced persons in South Sudan. Wkly Epidemiol Rec 2014;89:214–220.
- Sharma S, Carballo M, Feld JJ, et al. Immigration and viral hepatitis. J Hepatol 2015;63:515–522.
- Solomon AW, Foster A, Mabey DCW. Clinical examination versus Chlamydia trachomatis assays to guide antibiotic use in trachoma control programmes. Lancet Infect Dis 2006;6:5–8.
Appendix
The Global Trachoma Mapping Project Investigators are: Agatha Aboe (1,11), Liknaw Adamu (4), Wondu Alemayehu (4,5), Menbere Alemu (4), Neal D. E. Alexander (9), Berhanu Bero (4), Simon J. Brooker (1,6), Simon Bush (7,8), Brian K. Chu (2,9), Paul Courtright (1,3,4,7,11), Michael Dejene (3), Paul M. Emerson (1,6,7), Rebecca M. Flueckiger (2), Allen Foster (1,7), Solomon Gadisa (4), Katherine Gass (6,9), Teshome Gebre (4), Zelalem Habtamu (4), Danny Haddad (1,6,7,8), Erik Harvey (1,6,10), Dominic Haslam (8), Khumbo Kalua (5), Amir B. Kello (4,5), Jonathan D. King (6,10,11), Richard Le Mesurier (4,7), Susan Lewallen (4,11), Thomas M. Lietman (10), Chad MacArthur (6,11), Colin Macleod (3,9), Silvio P. Mariotti (7,11), Anna Massey (8), Els Mathieu (6,11), Siobhain McCullagh (8), Addis Mekasha (4), Tom Millar (4,8), Caleb Mpyet (3,5), Beatriz Muñoz (6,9), Jeremiah Ngondi (1,3,6,11), Stephanie Ogden (6), Alex Pavluck (2,4,10), Joseph Pearce (10), Serge Resnikoff (1), Virginia Sarah (4), Boubacar Sarr (5), Alemayehu Sisay (4), Jennifer L. Smith (11), Anthony W. Solomon (1,2,3,4,5,6,7,8,9,10,11), Jo Thomson (4), Sheila K. West (1,10,11), Rebecca Willis (2,9).
Key: (1) Advisory Committee, (2) Information Technology, Geographical Information Systems, and Data Processing, (3) Epidemiological Support, (4) Ethiopia Pilot Team, (5) Master Grader Trainers, (6) Methodologies Working Group, (7) Prioritisation Working Group, (8) Proposal Development, Finances and Logistics, (9) Statistics and Data Analysis, (10) Tools Working Group, (11) Training Working Group.