
ABSTRACT
Purpose: To describe the epidemiology of Microbial Keratitis (MK) in Uganda.
Methods: We prospectively recruited patients presenting with MK at two main eye units in Southern Uganda between December 2016 and March 2018. We collected information on clinical history and presentation, microbiology and 3-month outcomes. Poor vision was defined as vision < 6/60).
Results: 313 individuals were enrolled. Median age was 47 years (range 18–96) and 174 (56%) were male. Median presentation time was 17 days from onset (IQR 8–32). Trauma was reported by 29% and use of Traditional Eye Medicine by 60%. Majority presented with severe infections (median infiltrate size 5.2 mm); 47% were blind in the affected eye (vision < 3/60). Microbiology was available from 270 cases: 62% were fungal, 7% mixed (bacterial and fungal), 7% bacterial and 24% no organism detected. At 3 months, 30% of the participants were blind in the affected eye, while 9% had lost their eye from the infection. Delayed presentation (overall p = .007) and prior use of Traditional Eye Medicine (aOR 1.58 [95% CI 1.04–2.42], p = .033) were responsible for poor presentation. Predictors of poor vision at 3 months were: baseline vision (aOR 2.98 [95%CI 2.12–4.19], p < .0001), infiltrate size (aOR 1.19 [95%CI 1.03–1.36], p < .020) and perforation at presentation (aOR 9.93 [95% CI 3.70–26.6], p < .0001).
Conclusion: The most important outcome predictor was the state of the eye at presentation, facilitated by prior use of Traditional Eye Medicine and delayed presentation. In order to improve outcomes, we need effective early interventions.
Background
Microbial keratitis (MK) can be caused by a range of pathogens including, bacteria, viruses, protozoa, and fungi. It is characterized by acute or sub-acute onset of pain, conjunctival hyperemia, and corneal ulceration with a stromal inflammatory cell infiltrate.Citation1
MK has been described as a “silent epidemic”, which leads to substantial morbidity, related to blindness, pain, and stigma.Citation2 It is the leading cause of unilateral blindness after cataract in Tropical regions estimated at 2 million cases of monocular blindness per year.Citation3 In 2017, 1.3 million individuals were bilaterally blind from corneal opacity globally (excluding trachoma and vitamin A deficiency), accounting for 3.2% of the binocular blindness.Citation4 In Sub-Saharan Africa (SSA), MK is an important cause of binocular blindness and is responsible for about 15% of the monocular blindness (Nigeria National Survey).Citation5,Citation6 The only report of the incidence in SSA is from Malawi in 1994, which suggested a rate of around 180/100,000/year.Citation7 Rates in high-income settings are lower at 5–10/100,000.Citation8–Citation10
MK frequently leads to sight-loss from dense corneal scarring, or even loss of the eye, especially when the infection is severe and/or appropriate treatment is delayed. A good outcome depends on early appropriate treatment, supported by correct identification of the causative organism, and careful follow-up.Citation11,Citation12 In low and middle-income countries (LMIC), these resources are not readily available and outcomes tend to be poor.Citation13
Literature on MK in SSA is extremely sparse, only one audit from an LMIC setting (Tanzania) has previously reported outcomes of MK at discharge in SSA.Citation13 Here, in this large prospective cohort study from South-Western Uganda, we describe patient presentation, causative organisms, 3-month outcomes, and investigate their determinants.
Methods
Ethical statement
This study followed the tenets of the Declaration of Helsinki. It was approved by the London School of Hygiene & Tropical Medicine Ethics Committee (Ref 10647), Mbarara University Research Ethics Committee (Ref 10/04-16) and Uganda National Council for Science and Technology (Ref HS-2303). Written informed consent in the local language was obtained before enrolment. If the patient was unable to read, the information was read to them, and they were asked to indicate their consent by application of their thumbprint, which was independently witnessed.
Study design and setting
In this cohort, we prospectively enrolled patients with MK that presented to Ruharo Eye Centre (REC) and Mbarara University and Referral Hospital Eye Centre (MURHEC) from December 2016 to March 2018. MURHEC is a government-owned tertiary eye unit established in 2013. It provides mostly free services and sees about 6,000–10,000 patients/year. REC is a church-run fee-paying tertiary eye hospital founded in the 1960s. It sees about 20,000–25,000 patients/year. Both hospitals are located in Mbarara Municipality, South-Western Region, Uganda. In order to investigate the seasonal variation in the presentation of MK, we aimed to recruit all MK cases presenting during at least one year.Citation13
Study participants
MK was defined as loss of corneal epithelium (of at least 1-mm diameter) with underlying stromal infiltrate, associated with any or all signs of inflammation (conjunctival hyperemia, anterior chamber inflammatory cells, ± hypopyon).Citation14 We also included patients presenting with a deep corneal abscess (of at least 1 mm), defined as having all the features of MK, but without an epithelial defect. We excluded those not willing to participate, those not willing to return for follow-up, pregnant women, lactating mothers and those aged below 18 years.
Assessment
We documented basic demographic information and their ophthalmic history. This included the circumstances in which their eye became infected, predisposing factors, treatment received, and their “health care journey” before reaching the eye hospital. Presenting Log MAR (Logarithm of Minimum Angle of Resolution) visual acuity at 2 m in a dark room was measured using Peek Acuity software.Citation15 Participants were examined with a slit lamp to assess the anterior segment using a structured protocol, including eyelid assessment, corneal ulcer features, anterior chamber (flare, cells, hypopyon shape, and size) and perforation status. Infiltrate size was determined from the greatest diameter of the infiltrate (major axis) and the widest perpendicular diameter (minor axis).Citation14 The final infiltrate size was then derived as the geometric mean of these two diameters.Citation14 The same was repeated after fluorescein staining of the ulcer to determine epithelial defect sizes. High-resolution digital photographs with and without fluorescein staining were taken with a Nikon SLR 7200 digital camera with Macro lens.
Corneal scrape specimens were collected from the ulcer at a slit lamp or an operating microscope, using 21G needles after application of a proxymetacaine (minims) anesthetic eye drops. Samples underwent processing for the Gram stain, Potassium Hydroxide [KOH] stain, Calcofluor White [CFW] stain and direct inoculation on culture media (Sheep’s Blood Agar [BA], Chocolate Agar [HBA], Potato Dextrose Agar [PDA] and Brain Heart Infusion broth [BHI]). Two sterile corneal swab samples were taken for pan fungal gene sequencing. The number of corneal samples was dependent on how much material could be safely scraped from the cornea. The order was samples for microscopy, agar, broth, and finally corneal swabs.
In addition, a random blood sugar test and HIV counseling and testing were offered, as per the Uganda Ministry of Health HIV testing protocol. For those who were confirmed as HIV positive, a CD4 test was performed to determine the level of immune suppression and they were referred to the HIV care center, which is on the hospital site.
Microscopy, culture, and antimicrobial sensitivity work were done at the Mbarara University Department of Microbiology. The technician underwent initial training in ocular microbiology at the Aravind Eye Hospital System, department of ocular Microbiology in Madurai, India and had a site supervision visit by a mycologist from the London School of Hygiene & Tropical Medicine. Immediate CFW staining was also done in the side lab at MURHEC on a fluorescein microscope (Zeiss Primostar ILED) by the attending ophthalmologist. Agar plates and broths were incubated and read daily at 35–37°C for bacteria for up to 7 days and at 25°C for up to 21 days for fungi. Organism identification and sensitivity testing (MIC/zone of inhibition) were performed using standard microbiological techniques. We followed a previously described approach for reporting positive microbiology results.Citation16 Briefly, bacteria were identified using routine biochemical identification tests. Identification of fungi was according to the macroscopic appearance of cultures on potato dextrose and microscopic appearance of conidia and spore-bearing structures. Positive culture was growth at the site of inoculation or growth on one solid medium consistent with microscopy; or semiconfluent growth at the site of inoculation on one solid medium (if bacteria); or growth of the same organism on repeated scraping. If, by microscopy, hyphae were observed in corneal tissue, but failed to grow in culture, the causative organism was reported as fungal.
Treatment and follow-up
Patients were treated empirically at presentation and the treatment choice was reviewed when the microbiology results became available. Patients with fungal keratitis were treated with Natamycin 5% eyedrops (Zonat Sunways India), those with bacterial keratitis were treated with Ofloxacin 0.3% eyedrops (Biomedica Remedies-India). Patients with fungal infection were treated hourly day and night for the first 3 days and then hourly while the patient was awake for 2 weeks. This was changed to 2-hourly for another 2 weeks and then tapered to 4 times a day until healed. For bacterial infections, patients were treated hourly day and night for the first 3 days and then reduced to 6 times a day for a further week. All patients with fungal MK were also given Ofloxacin 0.3% eye-drops four times a day as prophylaxis until all epithelial defects were healed. In addition, those in pain were treated with Atropine 1% eye-drops (locally formulated) and oral Paracetamol tablets. Raised intraocular pressure was treated with Timolol 0.5% eye-drops (locally formulated). Those with presumed viral keratitis were treated with Acyclovir 3% eye ointment (CIPLA India) five times a day for 3 weeks. Most patients were admitted during the first week.
After the initial assessment patients were seen on day 2, day 7, day 21, and day 90 (3 months). Additional assessments were conducted as clinically indicated. The main outcome measures were final best-corrected vision at 3 months, blindness (<3/60 in the affected eye) at 3 months, and loss of the eye at 3 months. Scar density was also graded as “no scar” (clear cornea), “mild scar” (anterior chamber structures clearly visible through the scar), “moderate scar” (anterior chamber structures vaguely visible through the scar) and “dense scar” (anterior chamber structures completely obscured by the scar).
Analysis
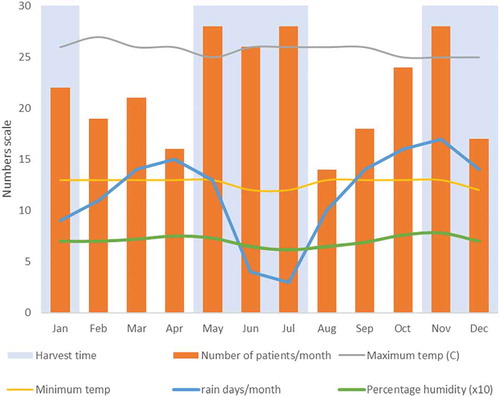
Data were analyzed in STATA v14. To describe the presentation of MK, summary frequency tables of demographics, presentation time, clinical history and clinical features were generated. Presentation time was classified as prompt (0–3 days), early (4–7 days), intermediate (8–14 days), late (15–30 days) and very late (more than 30 days).Citation17 In addition, a summary tally of patients that presented by month across one year (2017) was generated to describe the presentation pattern. This was compared to local rainfall, humidity and temperature patterns. Local weather data were obtained from the weather and climate repository.Citation18 For presentation purposes, Log MAR visual acuity measurements were converted to the Snellen scale and categorized according to the WHO classification system.Citation19
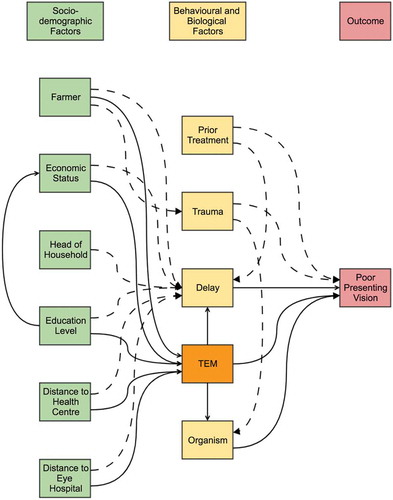
We used two different analytical approaches. We first took a causal modeling approach to explore the association of six risk factors of interest with visual acuity at presentation. These six factors were (Traditional Eye Medicine) TEM use, history of trauma, delayed presentation, distance from hospital, distance from nearest health center (HC), and organism type. In order to inform our modeling choices, we first drew Direct Acyclic Graphs (DAGs), using www.daggity.net v2.3 software, to identify relevant variables to adjust for in the multivariable logistic regression model.Citation20 A DAG is a representation of the hypothesized order of events from the exposure to the outcome. It allows the researcher to logically map out relationships between different variables and identify those to adjust for to determine the overall effect of the exposure on the outcome. A change in point estimate criteria was used to assess for confounding and multi-collinearity. Each main exposure was separately adjusted for confounding factors and final adjusted odds ratios (aOR) recorded.
The second modeling approach was to build a predictive model for visual acuity outcomes at 3 months, using baseline clinical features. Patients without 3-month data were excluded from the analysis. Ordinal logistic regression analysis of the WHO Snellen visual acuity categories was used to identify factors associated with visual acuity at 3 months. Univariable regression was performed to generate crude odds ratios (cOR). Variables with a p-value less than 0.1 were initially included in the multivariable model. A backward stepwise approach was then used until only the variables with a p-value of less than 0.05 were retained. Adjusted ORs were reported for the final model.
Results
Participants
Patient enrolment is illustrated in . The baseline characteristics of the patients are shown in . Median age was 47 years (IQR 35–60, total range 18–96 years), and the majority (56%) were male. Over a quarter had never had any formal education. Most (70%) were married and most (70%) were the heads of households. Median distance from home to the eye hospital was 79 km (IQR 52–128, total range 0.2–378 km). Median distance from home to their nearest HC was 3 km (IQR 1–4, total range 0–45 km). The main occupation was farming (70%). The baseline characteristics of the patients who were lost to follow-up and those who completed 3 months were similar (Supplementary Table 1).
Table 1. Demographic characteristics of the study participants.
Figure 1. Flow diagram of participants who were enrolled in the cohort study.
Presentation pattern
illustrates the number presenting per month throughout 2017, compared to rainfall, temperature and humidity patterns. Patients presented throughout the year, with peaks in May to July and October to November, which corresponded with the harvest seasons. April and November had the greatest rainfall. Temperature and humidity were constant throughout the year.
Figure 2. Presentation of patients with MK, by month in 2017 (n = 261). Monthly average minimum and maximum temperatures, average humidity and the number of days with rain are overlaid. Humidity was in percentage but was scaled to tens (divided by 10) to fit on the plot scale.
Presenting history
The median time from onset of symptoms to presentation time at the eye unit was 17 days (IQR 8–32, total range 0–370 days), . Only 7% of the participants presented “promptly” (within 3 days). Only 29% of the participants reported a history of trauma, and most (74%) of these were classified as organic in nature. Many patients (60%) reported use of TEM.
Table 2. Clinical history.
Clinical features and microbiology
shows the clinical features at presentation, including detailed characteristics of the ulcers and microbiology results. Specimen for microbiology was collected in 270 patients. Due to limited amounts of sample material, it was not possible to perform all tests on all those sampled. Almost half of the participants (47%) had a visual acuity of less than 3/60 (blind) in the affected eye at presentation. Microbiology results were available in 270/313 (86.3%) participants. Corneal scrapping was not performed on 43 participants who either did not consent, had deep-seated infiltrates, or small infiltrates (less than 0.5 mm). Overall, most infections were fungal (62%), 7% were bacterial and 7% were mixed (fungal and bacterial). Fifty-seven (20%) of the corneal scrapping samples were negative on both microscopy and culture.
Table 3. Clinical features and diagnosis at presentation (n = 313).
Outcomes
shows the outcomes of the 260 participants seen at the 3-month follow-up. At 3 months, the visual acuity was better than baseline vision. Median final visual acuity (Log MAR) was 0.4 (IQR 0–1.5) compared to a baseline median of 1.3 (IQR 0.3–2.5). Visual acuity at 3 months improved in 139 participants, worsened in 66 participants and remained unchanged in 56 (sign rank test p < .0001). Visual acuity was categorized according to the WHO classification system and poor outcome was considered as vision < 6/60.Citation19 Thirty percent of the participants were blind in the affected eye (vision less than 3/60) and 9% had lost their eye to infection due to evisceration following endophthalmitis.
Table 4. Outcomes at 3 months.
Causal modeling for poor presentation
shows the overall model for several variables of interest that we considered in the causal analysis for poor presenting vision. The results are summarized in and their corresponding outputs from the DAGitty software in Supplementary Figures 1–5. Those who reported TEM were estimated to have overall 1.6 times the odds of being in a poorer vision category compared to those who did not use TEM (aOR 1.62 [95%CI 1.04–2.54], p = .033). It was considered plausible that some of this effect was mediated through delayed presentation and/or organism type, and after adjusting for these factors as well, the aOR was 1.47 [95%CI 0.91–2.38], p = .11. There was some evidence (p = .033) of an association between the category of presentation time and presenting vision, with the lowest odds of poorer vision being in those that present earliest and increasing odds as delay increases. No evidence (p = .609) was found of an association between trauma and presenting visual acuity, but strong evidence was found of an association between presenting visual acuity and both distance from the eye hospital (p < .001) and distance from the nearest HC (p = .007). Interestingly, even after adjusting for delayed presentation there remained strong evidence of an association (p < .0001 and p = .009).
Table 5. Causal modeling for poor presenting vision (n = 313).
Figure 3. A DAG framework showing the causal pathways for poor presenting vision. This diagram is adjusted to illustrate the role of TEM. The solid lines indicate hypothesized direct relationships and the dashed lines indicate hypothesized indirect relationships.
Predictors of outcome
In the final multivariable model, worse visual acuity outcome at 3 months was associated with baseline vision, size of the infiltrate and perforation status at presentation .
Table 6. Factors at presentation predictive of a poor final visual acuity (WHO snellen ordinal scale) at 3 months (n = 260).
Discussion
This study describes the clinical history, signs, microbiological etiology, causes, and outcomes of MK in Uganda. Most patients presented with poor vision. At 3 months, 30% had monocular blindness in the affected eye and 1 in 10 lost their eye to infection.
Delayed presentation was common. Very few (7%) presented within 3 days of symptom onset and this had a direct impact on outcomes, as previously reported.Citation13 In this study, delayed presentation after adjusting for being a farmer, distance, economic status, education status, trauma, TEM and previous use of other treatment was associated with poor presenting vision. Earlier studies indicate that prompt prophylactic antibiotic can prevent simple corneal abrasions developing into MK, leading to much better outcomes.Citation17,Citation21,Citation22 Most late presenters had advanced ulcers, where treatment could do little. We know from prior literature that once an ulcer is advanced, treatment does relatively little to change its course.Citation23 From previous studies, it is recommended that treatment of MK should be started as early as possible to achieve optimal outcomes.Citation17
Another important cause of poor vision at presentation was Traditional Eye Medicine use. In this study, 60% of the patients reported TEM use. TEM increased the odds of poor presentation by 60% after adjusting for age, sex, being a farmer, economic status, education level, and distance. In our model, some of the effects of TEM seemed to be mediated through delay and organism type. But after adjusting for these, there was still an estimated 40% increase in odds of poor presentation, although the evidence for this association was weak. Many people probably try TEM before attending hospital, as it can be easily obtained within or close to home. In Uganda, TEM is usually made from plant products. This is concerning, as such substances may be toxic or harbor infectious agents, such as fungal spores.Citation7,Citation24 Importantly, our patients were open in admitting use of TEM, a widely acceptable practice for treating MK.
Distance was an important cause of poor presenting vision. This included distance to the eye hospital and distance to the nearest HC. This highlighted a major underlying problem of access to health services: the further the HC, the lower the chances of promptly starting appropriate treatment. In our model, even after adjusting for delay, distance was still highly associated with poor presenting vision meaning that there were still other unexplained factors in this relationship.
As reported previously, severity of infection at presentation (vision, perforation status, and infiltrate size) was the strongest predictor of outcome.Citation23,Citation25,Citation26 Poor vision at presentation (WHO Snellen categories) was strongly associated with a worse visual outcome. Vision is an easily measurable and reliable prognostic measure that can support lower and mid-level cadres to make the right clinical decisions. A perforated eye at presentation had 10 times greater odds while an eye with an impending perforation had 3 times greater odds of a worse visual outcome compared to a non-perforated eye. This was not surprising because keratoplasty services are currently not available in Uganda. People who presented with threatened or full perforation underwent conjunctival flap or evisceration surgery depending on the extent of the perforation.
Most of our patients presented with large infiltrate and epithelial defect sizes. Such median sizes would be considered severe ulcers in a high-income setting. The epithelial defect size was not included in the analysis because it was highly correlated to the infiltrate size. A large infiltrate size was associated with increased odds of a worse final visual outcome.Citation25,Citation26
Most of the affected patients were aged between 31 and 60 years, which are the prime years for economic productivity.Citation13 About 70% of the affected people were heads of households and sole breadwinners in their home. Prolonged morbidity due to MK meant that they could not provide for their dependents. In an ongoing study, we have been exploring how MK affects the quality of life and household incomes (unpublished). The prevalence of HIV among our cohort was almost double the national prevalence and diabetes was 4 times the reported prevalence.Citation27,Citation28 A high prevalence of HIV has been previously reported in people with MK.Citation13,Citation29 HIV and diabetes predispose to MK through immune suppression: we conducted a nested case-control to test for risk factors of MK including HIV and diabetes which have been reported separately.
Understanding the seasonal pattern of presentation is important to prepare a surveillance mechanism and for hospitals to have expectant management. We found that the presentation of MK tended to follow rainfall patterns linked to agricultural activity. This was not surprising since the majority (70%) of patients were farmers. There was little variation in humidity and temperature throughout the year. This region of Uganda has two planting and harvesting seasons, one in each half of the year following rains. Harvesting time is May–July and November–January. These were the periods when we recorded increased numbers of presentations. Farming (especially harvesting) has been linked to ocular trauma which predisposes to MK.Citation30 These corresponded with peak presentation to hospital. April has modest farming activity, as people are waiting for the harvesting season and it usually corresponds to Easter holiday. August usually has almost no farming activity since it comes at the end of the harvesting season before the rains come again in September. December had fewer patients presenting, possibly due to the Christmas season.
It remains unclear if this seasonal variation was related to trauma, as there were no clear seasonal differences in the pattern of presentation among patients who reported trauma and those who did not. We were surprised that relatively few patients (29%) reported trauma, although this is consistent with other studies from sub-Saharan Africa (SSA). In an older study from Ghana, 39% of the MK cases reported some form of eye injury prior to onset.Citation31 In two separate studies from Tanzania, 24% and 39% of the cases were associated with trauma.Citation13,Citation32 These levels are somewhat lower than those from South Asia, where around 75% are associated with an injury.Citation31,Citation33–Citation36 The reason for this difference is not apparent.
Ocular microbiology is not performed in many settings in SSA. As part of this study, we undertook to build the capacity of the hospital to provide this service. The overall microbiology yield was 80%. This was a composite of all the microscopy and culture results. Overall culture positive results were 55% similar to the expected yield reported in literature.Citation16,Citation31
Strengths/limitations
This is the first large prospective cohort study in SSA to describe outcomes of MK. Most of the reports have described etiology and presentation.Citation16,Citation29,Citation31,Citation32 Only one audit had attempted to describe outcomes.Citation13 The large number of patients gave sufficient power to analyze several factors associated with the main outcome measures. It was not possible to follow-up all the patients, with around 20% not having 3-month outcome data; however, no systematic differences were found between those with and without final follow-up data.
Conclusion
This study provides an understanding of MK epidemiology in Uganda. Majority of patients presented late after having traveled large distances to seek specialist care. Most patients presented with severe ulcers. The outcomes for many were poor, although around half had some improvement of vision with treatment. Predictive factors for these poor outcomes were the state of the eye at presentation. There is need to work on early interventions to prevent patients reaching such a stage where little can be done.
Conflict of interest
None of the authors have any proprietary interests or conflicts of interest related to this submission.
Submission statement
This submission has not been published anywhere previously and that it is not simultaneously being considered for any other publication.
Supplemental Material
Download MS Word (480 KB)Acknowledgments
The authors would like to appreciate Mr Gilbert Arinda, Ms Pauline Boonabaana, Mr Martin Bukenya, Mr Bernard Beinomugisha, Mr Martin Bukenya, and Ms Allen Asiimwe for helping in data collection.
Supplementary material
Supplemental data for this article can be accessed publisher’s website.
Additional information
Funding
Related Research Data
References
- Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases E-Book. Elsevier Health Sciences; 2014, New York, USA.
- Whitcher JP, Srinivasan M. Corneal ulceration in the developing world–a silent epidemic. Br J Ophthalmol. 1997;81(8):622–623. doi:10.1136/bjo.81.8.622.
- Whitcher JP, Srinivasan M, Upadhyay MP. Corneal blindness: a global perspective. Bull World Health Organ. 2001;79:214–221.
- Flaxman SR, Bourne RR, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Global Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5.
- Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82(11):844–851. doi: /S0042-96862004001100009.
- Marmamula S, Khanna RC, Rao GN. Unilateral visual impairment in rural south India-Andhra Pradesh Eye Disease Study (APEDS). Int J Ophthalmol. 2016;9(5):763–767. doi:10.18240/ijo.2016.05.23.
- Courtright P, Lewallen S, Kanjaloti S, Divala DJ. Traditional eye medicine use among patients with corneal disease in rural Malawi. Br J Ophthalmol. 1994;78(11):810–812. doi:10.1136/bjo.78.11.810.
- Erie JC, Nevitt MP, Hodge DO, Ballard DJ. Incidence of ulcerative keratitis in a defined population from 1950 through 1988. Arch Ophthalmol. 1993;111(12):1665–1671. doi:10.1001/archopht.1993.01090120087027.
- Lam D, Houang E, Fan D, Lyon D, Seal D, Wong E. Incidence and risk factors for microbial keratitis in Hong Kong: comparison with Europe and North America. Eye. 2002;16(5):608. doi:10.1038/sj.eye.6700151.
- Ong HS, Fung SS, Macleod D, Dart JK, Tuft SJ, Burton MJ. Altered patterns of fungal keratitis at a London ophthalmic referral hospital: an eight-year retrospective observational study. Am J Ophthalmol. 2016;168:227–236. doi:10.1016/j.ajo.2016.05.021.
- Titiyal JS, Negi S, Anand A, Tandon R, Sharma N, Vajpayee RB. Risk factors for perforation in microbial corneal ulcers in north India. Br J Ophthalmol. 2006;90(6):686–689. doi:10.1136/bjo.2005.079533.
- Pharmakakis NM, Andrikopoulos GK, Papadopoulos GE, Petropoulos IK, Kolonitsiou FI, Koliopoulos JX. Does identification of the causal organism of corneal ulcers influence the outcome? Eur J Ophthalmol. 2003;13(1):11–17. doi:10.1177/112067210301300102.
- Burton MJ, Pithuwa J, Okello E, et al. Microbial keratitis in East Africa: why are the outcomes so poor? Ophthalmic Epidemiol. 2011;18(4):158–163. doi:10.3109/09286586.2011.595041.
- Prajna NVMD, Krishnan TMD, Mascarenhas JMD, et al. The mycotic ulcer treatment trial: a randomized trial comparing natamycin vs voriconazole. JAMA Ophthalmol. 2013;131(4):422–429. doi:10.1001/jamaophthalmol.2013.1497.
- Bastawrous A, Rono HK, Livingstone IA, et al. Development and validation of a smartphone-based visual acuity test (peek acuity) for clinical practice and community-based fieldwork. JAMA Ophthalmol. 2015;133(8):930–937. doi:10.1001/jamaophthalmol.2015.1468.
- Leck A, Thomas P, Hagan M, et al. Aetiology of suppurative corneal ulcers in Ghana and south India, and epidemiology of fungal keratitis. Br J Ophthalmol. 2002;86(11):1211–1215. doi:10.1136/bjo.86.11.1211.
- Getshen K, Srinivasan M, Upadhyay MP, Priyadarsini B, Mahalaksmi R, Whitcher JP. Corneal ulceration in South East Asia. I: a model for the prevention of bacterial ulcers at the village level in rural Bhutan. Br J Ophthalmol. 2006;90(3):276–278. doi:10.1136/bjo.2005.076083.
- Weather-and-climate.com. World weather and climate information. weather-and-climate.com. https://weather-and-climate.com/average-monthly-Rainfall-Temperature-Sunshine,Mbarara,Uganda. Published 2018. Accessed July 19, 2018.
- Organization WH. Change the definition of blindness. Disponível no endereço eletrônico. http://www who int/blindness/ChangetheDefinitionofBlindness pdf. 2008.
- Shrier I, Platt RW. Reducing bias through directed acyclic graphs. BMC Med Res Methodol. 2008;8(1):70. doi:10.1186/1471-2288-8-70.
- Maung N, Thant CC, Srinivasan M, et al. Corneal ulceration in South East Asia. II: A strategy for the prevention of fungal keratitis at the village level in Burma. Br J Ophthalmol. 2006;90(8):968–970. doi:10.1136/bjo.2006.094706.
- Srinivasan M, Upadhyay MP, Priyadarsini B, Mahalakshmi R, Whitcher JP. Corneal ulceration in south-east Asia III: prevention of fungal keratitis at the village level in south India using topical antibiotics. Br J Ophthalmol. 2006;90(12):1472–1475. doi:10.1136/bjo.2006.103028.
- Prajna NV, Krishnan T, Mascarenhas J, et al. Predictors of outcome in fungal keratitis. Eye (Lond). 2012;26(9):1226–1231. doi:10.1038/eye.2012.99.
- Yorston D, Foster A. Traditional eye medicines and corneal ulceration in Tanzania. J Trop Med Hyg. 1994;97(4):211–214.
- Chidambaram JD, Venkatesh Prajna N, Srikanthi P, et al. Epidemiology, risk factors, and clinical outcomes in severe microbial keratitis in South India. Ophthalmic Epidemiol. 2018;25(4):297–305. doi:10.1080/09286586.2018.1454964.
- Tananuvat N, Punyakhum O, Ausayakhun S, Chaidaroon W. Etiology and clinical outcomes of microbial keratitis at a tertiary eye-care center in northern Thailand. J Med Assoc Thai. 2012;95:S8–17.
- International. UMoHaI. 2011 Uganda AIDS indicator survey: key findings. In: MOH, ed. Calverton, Maryland: MOH and ICF International; 2012.
- Bahendeka S, Wesonga R, Mutungi G, Muwonge J, Neema S, Guwatudde D. Prevalence and correlates of diabetes mellitus in Uganda: a population‐based national survey. Trop Med Int Health. 2016;21(3):405–416. doi:10.1111/tmi.2016.21.issue-3.
- Mselle J. Fungal keratitis as an indicator of HIV infection in Africa. Trop Doct. 1999;29(3):133–135. doi:10.1177/004947559902900303.
- Bharathi MJ, Ramakrishnan R, Meenakshi R, Shivakumar C, Raj DL. Analysis of the risk factors predisposing to fungal, bacterial & Acanthamoeba keratitis in south India. Indian J Med Res. 2009;130:749–757.
- Hagan M, Wright E, Newman M, Dolin P, Johnson G. Causes of suppurative keratitis in Ghana. Br J Ophthalmol. 1995;79(11):1024–1028. doi:10.1136/bjo.79.11.1024.
- Poole TR, Hunter DL, Maliwa EM, Ramsay AR. Aetiology of microbial keratitis in northern Tanzania. Br J Ophthalmol. 2002;86(8):941–942. doi:10.1136/bjo.86.8.941.
- Bharathi MJ, Ramakrishnan R, Meenakshi R, Padmavathy S, Shivakumar C, Srinivasan M. Microbial keratitis in South India: influence of risk factors, climate, and geographical variation. Ophthalmic Epidemiol. 2007;14(2):61–69. doi:10.1080/09286580601001347.
- Upadhyay M, Karmacharya P, Koirala S, et al. The Bhaktapur eye study: ocular trauma and antibiotic prophylaxis for the prevention of corneal ulceration in Nepal. Br J Ophthalmol. 2001;85(4):388–392. doi:10.1136/bjo.85.4.388.
- Upadhyay MP, Karmacharya PC, Koirala S, et al. Epidemiologic characteristics, predisposing factors, and etiologic diagnosis of corneal ulceration in Nepal. Am J Ophthalmol. 1991;111(1):92–99. doi:10.1016/S0002-9394(14)76903-X.
- Srinivasan M, Gonzales CA, George C, et al. Epidemiology and aetiological diagnosis of corneal ulceration in Madurai, south India. Br J Ophthalmol. 1997;81(11):965–971. doi:10.1136/bjo.81.11.965.