
ABSTRACT
Adolescents with attention-deficit/hyperactivity disorder (ADHD) are known to have stronger preferences for smaller immediate rewards over larger delayed rewards in delay discounting tasks than their peers, which has been argued to reflect delay aversion. Here, participants performed a delay discounting task with gains and losses. In this latter condition, participants were asked whether they were willing to wait in order to lose less money. Following the core assumption of the delay aversion model that individuals with ADHD have a general aversion to delay, one would predict adolescents with ADHD to avoid waiting in both conditions. Adolescents (12–17 years) with ADHD (n = 29) and controls (n = 28) made choices between smaller immediate and larger delayed gains, and between larger immediate and smaller delayed losses. All delays (5–25 s) and gains/losses (2–10 cents) were experienced. In addition to an area under the curve approach, a mixed-model analysis was conducted to disentangle the contributions of delay duration and immediate gain/delayed loss amount to choice. The ADHD group chose the immediate option more often than controls in the gain condition, but not in the loss condition. The contribution of delay duration to immediate choices was stronger for the ADHD group than the control group in the gain condition only. In addition, the ADHD group scored higher on self-reported delay aversion, and delay aversion was associated with delay sensitivity in the gain condition, but not in the loss condition. In sum, we found no clear evidence for a general aversion to delay in adolescents with ADHD.
The delay aversion model proposes that children with attention-deficit/hyperactivity disorder (ADHD) develop an aversion to delay due to negative emotions associated with waiting, as a result of disturbances in the brain’s reward circuits (Sonuga-Barke, Dalen, & Remington, Citation2003; Sonuga-Barke, Taylor, Sembi, & Smith, Citation1992). This can explain their impulsive behavior in daily life. In the laboratory, impulsive choice is often measured by the use of delay discounting tasks in which participants are repeatedly asked to choose between smaller immediate rewards (e.g., 5 dollars now) and larger delayed rewards (e.g., 10 dollars next week) (e.g., Scheres, de Water, & Mies, Citation2013). A reward loses its value if the delay to the reward increases, which is referred to as delay discounting. It is well known that children and adolescents with ADHD prefer, more often than controls, smaller immediate rewards over larger delayed rewards in these types of tasks. In other words, they show steeper discounting of delayed rewards (see for meta-analyses Jackson and MacKillop, Citation2016; Patros et al., Citation2016). Although the delay aversion account of ADHD is intuitively appealing, to date, evidence for the role of delay aversion in this impulsive choice behavior is limited. Only recently, neuroimaging studies have provided support for the idea that delay aversion contributes to this phenomenon, by showing increased involvement of emotional brain regions (i.e., amygdala and insula) in response to delay-related cues (Lemiere et al., Citation2012; Van Dessel et al., Citation2018; Wilbertz et al., Citation2013). It is important to gain insight into what drives impulsive choice in ADHD to be able to develop interventions to reduce this choice style and its associated negative outcomes.
Other factors than delay aversion might play a role in this form of impulsive choice. Steeper delay discounting in ADHD may also be due to reduced sensitivity to reward magnitude (e.g., Luman, Van Meel, Oosterlaan, Sergeant, & Geurts, Citation2009; Scheres, Tontsch, Thoeny, & Kaczkurkin, Citation2010). People who care less about the magnitude of the reward might not wait for a larger reward. Another factor that could explain steeper discounting in ADHD is a preference for reward immediacy: individuals with ADHD may be especially sensitive to sooner rewards when these can be obtained right now. When there is no immediate reward option available, but rather the choice is between a sooner (but still delayed) smaller reward and a later (even more delayed) larger reward, people are more likely to wait for larger rewards than if the sooner option were an immediately available reward. However, we found no support for such an exaggerated immediate reward preference in young adults with increased symptom levels of ADHD (Mies, De Water, & Scheres, Citation2016). Unpublished data from our group, on the other hand, showed that a small group of adolescents with a clinical diagnosis of ADHD did show an increased immediate reward preference compared to controls: When the choice was between receiving $100 after 2 years and a smaller reward (varying in size) after 1 year, the ADHD group was equally willing to wait for the larger amount as the control group was. When, however, the choice was between receiving $100 after 1 year and a smaller reward (varying in size) today, the ADHD group was less willing to wait for the larger reward than the control group was. This suggests that immediacy of the soon option is especially important for those with a clinical diagnosis of ADHD. Similarly, Tripp and Alsop (Citation2001) showed that children with ADHD are unusually sensitive to delays preceding rewards, rather than delays following rewards (postreward delays), suggesting that they have a “NOW” bias rather than being delay averse. In other studies that included such postreward delays, however, both sensitivity to reward immediacy and delay aversion appeared to contribute to a preference for immediate reward in older children/adolescents with ADHD (Marco et al., Citation2009; Scheres et al., Citation2006). In sum, these findings are mixed. A more thorough understanding of the role of delay aversion in impulsive choice behavior is thus needed.
In the present study, we took another approach to examine whether delay aversion contributes to discounting behavior in adolescents with ADHD: we examined not only discounting of rewards, but also of losses. The ADHD literature has focused mainly on sensitivity to reward and on reward discounting. To our knowledge, loss discounting has not been examined in ADHD yet. If ADHD is associated with a general aversion to delay, then steeper discounting should not be limited to gains, but should also apply to losses. Thus, in addition to asking participants to choose between smaller immediate and larger delayed gains, we asked them to choose between larger immediate losses and smaller delayed losses. That is, we asked them whether they were willing to wait in order to lose less money. We used an experiential design in which all gains and losses and all delays were experienced.
In contrast to the experiential design as applied in our study, previous loss discounting studies have used hypothetical designs (i.e., losses and delays are not actually experienced), in which participants were asked the opposite from what we asked, namely to choose between a smaller immediate loss (e.g., pay 10 dollars now) and a larger delayed loss (e.g., pay 100 dollars after 1 year). These studies have shown that people are inclined to choose larger delayed losses, that is, they discount losses (Estle, Green, Myerson, & Holt, Citation2006; Mies et al., Citation2016; Tanaka, Yamada, Yoneda, & Ohtake, Citation2014; Thaler, Citation1981). It should be noted, though, that losses are generally discounted less steeply than gains, which is known as the sign effect (e.g., Estle et al., Citation2006). Loss discounting occurs because losing money now is experienced as more aversive than losing money in a more distant future. In other words: people postpone losses. Thus, in contrast to gain discounting (i.e., preference for the immediate option), loss discounting reflects a preference for the delayed option in the case of a hypothetical design. In both cases, the larger amount of the two choice options – whether it is the larger delayed gain or the larger delayed loss – loses its value with increasing delay to that gain or loss. In the current study, however, we used an experiential design in which all delays were experienced. In such an experiential task, both waiting and losing money are thought to be aversive, and one would expect that no one would be willing to wait longer to lose more money in these circumstances, whereas in a hypothetical task “waiting” for a loss is appealing (putting it off). Therefore, as mentioned before, we reversed the questions: instead of asking participants whether they wanted to wait longer and lose more money, we asked them whether they were willing to wait in order to lose less money. In this case, loss discounting reflects a preference for the large immediate loss, that is, the large loss loses its (negative) value with increasing delay to the smaller loss.
Thus, in the present study, we used an experiential delay discounting task in order to examine the cost–benefit trade-off between waiting and losing money in adolescents with and without ADHD, in comparison with the more often examined cost–benefit trade-off between waiting and gaining money. By using an experiential instead of a hypothetical design, we are more likely to capture delay aversion, and are therefore better able to examine delay aversion as a mechanism contributing to steep discounting in ADHD.
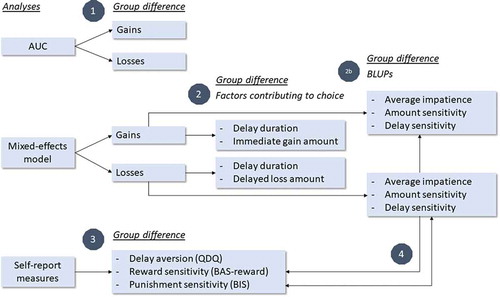
First, based on the delay aversion model, which proposes that individuals with ADHD have developed a general aversion to delay during childhood due to negative emotions associated with waiting, we predicted that individuals with ADHD would avoid waiting in both conditions, i.e., that they would show more discounting than controls in both the gain and loss condition. To this purpose, we compared the area under the discounting curves (AUCs) of both groups for gains and losses separately. Second, to gain more detailed insight into the different factors that may contribute to this discounting behavior, we used a mixed-model approach (Baayen, Citation2004). This approach enabled us to tease apart the contributions of delay duration and immediate gain amount to choices in the gain condition (see also de Water et al., Citation2017; Foerde et al., Citation2016) and delay duration and delayed loss amount in the loss condition. We examined whether adolescents with ADHD differed from controls in these contributions to choices. We expected that individuals with ADHD would be more sensitive than controls to delay, but not necessarily to amount, in both task conditions, in line with the delay aversion model. Third, we examined whether self-reported delay aversion in daily life and reward and punishment sensitivity differed between groups. Finally, we examined whether these self-report measures were associated with choices in the delay discounting task (i.e., with average impatience, sensitivity to delay and to amount; derived from the mixed-model analyses), in order to examine their convergent validity (see also Thorell, Sjöwall, Mies, & Scheres, Citation2017). We hypothesized that self-reported delay aversion would be associated with steeper discounting in general, i.e., with greater average impatience and delay sensitivity, and with less sensitivity to amount, in both the gain and loss conditions. We further hypothesized that self-reported reward sensitivity would be associated with sensitivity to amount in the gain condition specifically, and punishment sensitivity with sensitivity to amount in the loss discounting. See for an overview of the analyses corresponding to these research questions and hypotheses.
Figure 1. Overview of the analyses corresponding to the research questions. AUC = area under the (discounting) curve, BLUPs = best linear unbiased predictions (see mixed-effects model analyses), QDQ = quick delay questionnaire, BAS-reward = reward sensitivity subscale of the Behavioral Inhibition/Approach System Scales (BIS/BAS), BIS = Behavioral Inhibition subscale of the BIS/BAS. See Methods for further details.
Methods
Participants
For a larger study that also included an functional Magnetic Resonance Imaging (fMRI) session (see Mies, Ma, De Water, Buitelaar, & Scheres, Citation2018), we recruited 34 adolescents with ADHD (combined type) and 32 healthy controls between 12 and 17 years of age (see ). Participants and their parents gave written informed consent prior to participation, and the study was approved by the local medical ethics committee. Adolescents with ADHD were recruited via Karakter Child and Adolescent Psychiatry University Centre and advertisements in local newspapers. Control participants were recruited via advertisements and schools.
Table 1. Participant characteristics (means, standard deviations, and group differences).
All participants in the ADHD group were selected on the basis of a preexisting clinical diagnosis of ADHD of the combined type from a licensed child psychiatrist or psychologist. The “behavioral disorders” module of the Diagnostic Interview Schedule for Children (DISC-IV, parent version) was used to assess current validity of this diagnosis,Footnote1 and the “whole life” module was used to assess symptom criteria of other psychiatric disorders. Healthy volunteers were also screened for the same psychiatric disorders using the DISC-IV. Additionally, parents were asked to complete the Child Behavior Checklist (CBCL) (Achenbach and Rescorla, Citation2001) to assess emotional and behavioral problems and the Disruptive Behavior Disorders Rating Scale (DBDRS) (Oosterlaan, Scheres, Antrop, Roeyers, & Sergeant, Citation2000; Pelham, Gnagy, Greenslade, & Milich, Citation1992) to assess symptom severity of ADHD, oppositional defiant disorder (ODD), and conduct disorder (CD). These latter two questionnaires were used as descriptive instruments, and to help decide on whom to exclude from analyses in addition to the DISC-IV.
Exclusion criteria were neurological illness, brain trauma, any contraindication for having an MRI scan, the use of psychoactive medication that could not be discontinued (i.e., medication other than psychostimulants), and IQ < 70. Participants in the ADHD group were not allowed to have comorbid psychiatric disorders except for ODD (n = 2 according to DISC-IV) and CD (n = 2 according to DBDRS), while participants in the control group were not allowed to have any current psychiatric disorder on the basis of the DISC-IV, and not allowed to score within the clinical range of emotional or behavioral problems on the CBCL or DBDRS.
One control participant was excluded because of IQ < 70 (based on two subtests of the Wechsler Intelligence Scale for Children (WISC-III; Kort et al., Citation2002: vocabulary, block design), one because of an MRI contraindication, and another because she scored within the clinical range of internalizing problems on the CBCL. Three ADHD participants were excluded because of several comorbid disorders and/or the use of medication that could not be discontinued. Participants who used psychostimulants (n = 23) were asked to discontinue their medication at least 24 h prior to the experiment.Footnote2 Two participants (one ADHD and one control) did not perform the gain and loss discounting task, which always followed the scan session, because of fatigue or lack of motivation after the scan session. Another ADHD participant prematurely ended the study because of anxiety in the scanning environment, and therefore also did not participate in the gain and loss discounting task. Therefore, the data of 29 ADHD and 28 control participants () were used in the analyses of the gain and loss discounting task.
Gain and loss discounting task
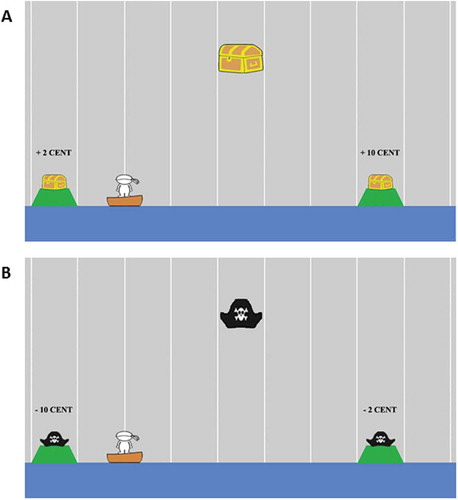
The task consisted of four blocks of 24 trials each. Blocks 1 and 3 were gain blocks, and blocks 2 and 4 were loss blocks. The order of blocks was thus: Gain–Loss–Gain–Loss. In the gain condition, a character in a boat was shown, representing the participant, and both on the left and the right side of this character, an island with a treasure chest with a monetary amount was shown (see ). Participants were instructed to choose to sail to one of the two islands, one island always being close to the participant and the other island being further away. Vertical lines indicated the level of delay corresponding to the islands. In the gain condition, the treasure chest close to the participant contained a small immediate gain (e.g., 2 cents in 1.5 s), and the treasure chest further away contained a larger delayed gain (e.g., 10 cents in 25 s). In the loss condition, participants were told that there were pirates on the islands instead of treasure chests and that they had to pay money to the pirates in order to be able to dock their boat. On the island close to the participant, they would lose 10 cents immediately (1.5 s), and on the island further away they would have to wait longer in order to lose less money (e.g., 2 cents in 25 s). In the gain condition, the reward associated with the delayed choice was 10 cents (fixed), and the rewards associated with the immediate option were 2, 4, 6, and 8 cents. This was opposite in the loss condition: the loss associated with the immediate option was −10 cents (fixed), and the losses associated with the delayed option were −2, −4, −6, and −8 cents. In both conditions, delays were 1.5 (immediate option), 5, 10, 15, 20, and 25 s. To prevent strategies to deal with delay, as well as possible group differences in initial delay perception influencing choice behavior, participants were not informed about the exact delay durations. Instead, participants were told that the delays were the same as the delays that were used in a delay and effort discounting task that they performed in the scanner. They had already experienced each delay before performing the task.
Figure 2. Task design showing an example of a choice presentation between (A) two islands with treasure chests (gain condition) and (B) two islands with pirate hats (loss condition). The character in the boat represented the participant. On the left and right side of this character, an island with either a treasure chest (gain) or pirate hat (loss) was shown. Participants were instructed to choose to sail to one of the two islands, one island always being close to the participant (no delay, 1.5 s) and the other island being further away. Vertical lines indicated the level of delay corresponding to the islands.
The stimulus sequence consisted of the following: (1) a cue stimulus with the two options (islands) to choose from, which was presented until a choice was made with a maximum of 6 s, (2) a confirmation of the participant’s choice (arrow pointing at island of choice), presented for 1 s, (3) a fixed thermometer that indicated the chosen delay, which was presented for the proposed and chosen delay period, (4) a feedback stimulus indicating the amount of money gained/lost on that trial, presented for 1 s, and (5) a fixation cross presented for 1 s.
All amounts that were won and lost were added so that participants actually lost money that they had just gained in the previous block. The net amount was paid in cash to the participant. In order to prevent that participants would worry that they might lose money in the end, we gave them 50 cents to start with and told them that they could use that amount to be able to pay in the loss condition. Despite this start amount, it was still possible to lose more money than the money gained; therefore, unbeknownst to participants, the minimum amount was set to 0 cents. None of the participants, however, lost more money than they gained.
In each block, all choice combinations for either gain or loss were presented once, leading to two presentations in total for each condition. In both conditions, 8 “catch” trials (4 per block) were included in which participants were asked to choose between the same amount (10 cents) at different delays (e.g., gain or lose 10 cents after 1.5 s or 10 cents after 25s), or different amounts for the same level of delay (e.g., gain or lose 2 cents after 1.5 s or 10 cents after 1.5 s). These catch trials served to check whether participants made choices as expected, i.e., whether they preferred to minimize delays and losses, and maximize gains, all else being equal (see supplemental data). Each block lasted between approximately 3 and 7 min, depending on the participant’s choices. On each trial, participants indicated their choice by pressing 1 (island on the left) or 2 (island on the right) on a keyboard. Participants were told that there was a fixed number of trials, and that there were no right or wrong answers, so that they should choose what they preferred.
Questionnaires
Participants completed several questionnaires. A self-developed questionnaire was used to assess health, including medication use and substance use. The Barratt Impulsiveness Scale (BIS-11) (Patton, Stanford, & Barratt, Citation1995) was used to compare groups on trait impulsivity (internal consistency in current study: α = .81), the Behavioral Inhibition/Approach System Scales (BIS/BAS) (Carver and White, Citation1994) to compare groups on reward sensitivity (subscale BAS reward sensitivity, α = .82), and on punishment sensitivity (subscale BIS, α = .66), the Snaith–Hamilton Pleasure Scale (SHAPS) (Snaith et al., Citation1995) to compare groups on anhedonia or the loss of pleasure (α = .88), and the Quick Delay Questionnaire (QDQ) (Clare, Helps, & Sonuga-Barke, Citation2010) to compare groups on self-reported delay aversion (α = .77) and delay discounting (α = .58).
Parents completed the CBCL and DBDRS to assess problem behaviors in their child (see also Participants section), as well as the Social Responsiveness Scale (SRS) (Constantino and Gruber, Citation2005; Roeyers, Thys, Druart, De Schryver, & Schittekatte, Citation2011) to screen for autism spectrum disorder (ASD) symptoms, since ASD and ADHD symptoms often co-occur (e.g., Hartman, Geurts, Franke, Buitelaar, & Rommelse, Citation2016). The SRS was used as a descriptive instrument. See for group comparisons on these questionnaires.
Procedure
During visit 1, participants completed the above-mentioned questionnaires, two subtests of the WISC-III (vocabulary, block design) to estimate IQ, and got acquainted with the scanning environment in a mock scanner. In the meantime, parents were interviewed (DISC-IV) and completed the CBCL, DBDRS, and SRS. During visit 2, participants first conducted a delay and effort discounting task (reported elsewhere) in the scanner. After scanning, participants conducted the gain and loss discounting task.
Participants were paid 25 euros for participation in the study and additionally earned between 8.80 and 17.60 euros during the scan session, and between 0 and 2.70 euros during the gain and loss discounting task.
Statistical analyses
Area under the discounting curve
Delay discounting was examined using the classical AUC approach (Myerson, Green, & Warusawitharana, Citation2001). Subjective values (SVs), indicative of the amount at which an individual is indifferent between the delayed and immediate gain/loss, were calculated for the delayed gain and immediate loss (10 cents) for each level of delay preceding the larger gain or smaller loss, for each participant. SVs were calculated on the basis of the proportion of delayed choices (Boettiger et al., Citation2007; Eppinger, Nystrom, & Cohen, Citation2012). Subsequently, for each individual, the AUCs for gains and losses were calculated in accordance with the method described by Myerson et al. (Citation2001). AUC ranges from 0 to 1. Smaller AUCs reflect steeper discounting.
Two participants with ADHD had initially not understood task instructions: after the first gain block, they indicated that they thought that pirates would have incidentally taken away money during the gain block. This first gain block was therefore not taken into account in the SV and AUC calculation for these two participants, and was also excluded from the mixed-model analyses mentioned below. Another two participants with ADHD did not finish the last (loss) block of the task because they accidentally aborted the task by pressing the ESC key. For these latter two participants, all choices up to the point of task abortion were taken into account in the SV and AUC calculation, as well as in the mixed-model analyses.
Two independent-samples t tests were conducted in SPSS to examine group differences in the AUC for gains and for losses (see ).
Mixed-effects model analyses
In addition to the main AUC analyses, the different factors contributing to task choices () were analyzed with generalized linear mixed-effects models using the lme4 package (Bates, Mächler, Bolker, & Walker, Citation2015) in R (version 3.2.0; R Core Team, Citation2013). The dependent variable was choice (1 = immediate, 0 = delayed). See supplemental data for the formal notations of the fitted mixed-effects models.
The first model was estimated based on the gain condition. This model included a fixed intercept and the following fixed effects: (1) the delay preceding the larger gain, (2) the amount of the immediate gain, (3) group, (4) the interaction between group and delay, and (5) the interaction between group and amount. For each participant, random adjustments to the fixed intercept and to the slopes of the effects for delay and amount were included. All correlation terms among the random effects were estimated, resulting in a model “maximal with respect to the random effects” as suggested by Barr, Levy, Scheepers, and Tily (Citation2013), to avoid inflated Type 1 errors. Delay and amount were standardized (centered and scaled) and group was specified by a sum-to-zero contrast (1 = ADHD, −1 = controls).
The second model was estimated based on the loss condition. This model was similar to the previous model based on gains. In this case, however, the fixed effect of amount that was included in the model concerned the amount of the delayed loss instead of the immediate gain.
For the mixed-effects model analyses described above (see also ), the optimizer “bobyqa” was used, with a maximum number of 1 × 109 iterations. p-Values were determined using likelihood ratio tests as implemented in the mixed function of the afex package (Singmann, Bolker, & Westfall, Citation2015). All fixed and random effects estimate how a change in one of the predictors (e.g., the effect of amount on immediate gain choice) affects the dependent variable (e.g., immediate gain choice) when the other variables are held constant (Baayen, Citation2004).
In addition to examining the interactions between group and delay and group and amount, we also directly compared groups on their average preference for immediate gain/loss (i.e., average impatience), sensitivity to delay, and sensitivity to amount (see ), by extracting three so-called best linear unbiased predictions (BLUPs; the model’s best estimate for each participant’s intercept and regression coefficients) for each participant. These BLUPs were again estimated for the gain and loss condition separately: (1) Average impatience (random intercept). This reflects each participant’s likelihood to choose the immediate option for an average amount and delay. Higher values indicate a greater tendency to choose the immediate option. This BLUP is similar to the AUC in that it includes both the influence of delay and amount on choice. Consistent with this point, participants’ random intercept was highly correlated with their AUC for both the gain condition (rho = –.98, p < .001) and the loss condition (rho = –.90, p < .001); (2) Amount sensitivity (i.e., random amount slope), indexing the unique contribution of the immediate gain amount (for the gain condition) and delayed loss amount (for the loss condition) to choice. Higher values indicate a greater tendency to choose the immediate option when the immediate gain was high or the delayed loss was high; (3) Delay sensitivity (random delay slope), indexing the unique contribution of delay to the delayed option to choice. Higher values indicate a greater tendency to choose the immediate option when delays were longer. To examine group differences in average impatience, delay sensitivity, and amount sensitivity, we used independent-samples t tests (in SPSS) on these BLUPs (see ).
Group differences in self-report measures
Groups were compared on their self-reported delay aversion (QDQ), as well as on reward and punishment sensitivity (BAS reward scale, BIS scale) using independent-samples t tests (see ).
Correlations between self-report measures and discounting across groups
We computed Spearman rank-order (rho) correlationsFootnote3 between the different BLUPs – average impatience, amount sensitivity, and delay sensitivity – and (1) self-reported daily-life delay aversion (QDQ), (2) reward sensitivity (BAS reward scale), and (3) punishment sensitivity (BIS scale) (see also ).
Results
Area under the curve analysis
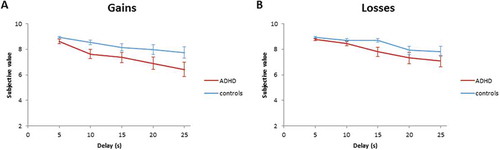
There was a significant effect of group on gain discounting (t(55) = 2.009, p = .050, d = 0.53), but not on loss discounting (t(55) = 1.67, p = .102, d = 0.44) (see ), suggesting that the ADHD group showed more discounting than controls in the gain task, but this effect did not reach statistical significance in the loss task.
Figure 3. Subjective values of (a) delayed gains (10 cents) and (b) immediate losses (−10 cents) as a function of delay for the ADHD and control group.
Mixed-effects model analyses
Group differences in contributions of delay duration and gain/loss amount to choice
Model 1 showed a main effect of group on immediate gain choice (B = 1.10, SE = 0.52, χ2(1) = 4.70, p = .03), indicating that adolescents with ADHD chose the immediate gain more often than controls, in line with the medium-sized group effect in the AUC analysis. No main effect of delay was found in this model, but the very high correlation between delay and intercept may have obscured such an effect. In a model in which this correlation was not explicitly estimated, we did find a main effect of delay on immediate gain choice (B = 1.08, SE = 0.16, χ2(1) = 24.79, p < .001), indicating that participants chose the immediate gain more frequently as the delay preceding the larger gain increased, i.e., gains were discounted. There was also a main effect of amount on immediate gain choice (B = 1.38, SE = 0.34, χ2(1) = 18.49, p < .001): participants chose the immediate gain more frequently as its amount increased. No significant interactions between group and delay (B = 0.25, SE = 0.22, χ2(1) = 1.43, p = .23) and group and amount (B = 0.01, SE = 0.19, χ2(1) = 2.48, p = .12) were found.
In line with the AUC analysis, model 2 showed no significant effect of group on immediate loss choice (B = 0.72, SE = 0.50, χ2(1) = 2.04, p = .15). There was a main effect of delay on immediate loss choice (B = 1.25, SE = 0.16, χ2(1) = 25.51, p < .001), indicating that participants chose the larger immediate loss more often as the delay preceding the smaller loss increased, i.e., losses were discounted. The effect of amount on immediate loss choice did not reach significance (B = 0.75, SE = 0.39, χ2(1) = 3.50, p = .06). Again, no significant interactions between group and delay (B = 0.09, SE = 0.21, χ2(1) = 0.18, p = .68), or group and amount (B = 0.06, SE = 0.19, χ2(1) = 0.08, p = .77) were found.
Group differences in average impatience, delay sensitivity, and amount sensitivity
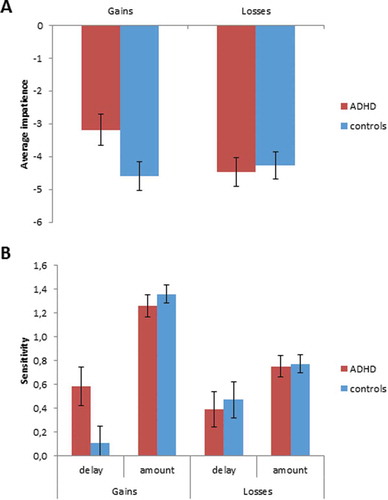
For gains, adolescents with ADHD showed a significantly higher average impatience (t = −2.10, p = .04, d = 0.56) and delay sensitivity (t = −2.07, p = .04, d = 0.55) than controls, but groups did not differ in their amount sensitivity (t = 0.86, p = .39, d = 0.23). For losses, there were no significant group differences in average impatience, or delay and amount sensitivity (all ps > .71) (see ).
Figure 4. Best linear unbiased predictions (BLUPs) for (a) average impatience and (b) sensitivity to delay and to amount of the immediate gain or delayed loss for the ADHD and control group. The ADHD group chose the immediate gain more often than the control group, and was more sensitive to delay than the control group in the gain condition, but not in the loss condition.
Group differences in self-report measures
Participants with ADHD reported to be more delay averse in daily life than those without ADHD. No group differences were found in self-reported reward (BAS-reward) and punishment sensitivity (BIS) (see ).
Correlations between Average Impatience, Delay Sensitivity, Amount Sensitivity and Self-report Measures across Groups
Participants’ self-reported delay aversion (QDQ) was positively correlated with their average impatience (rho = .38, p = .004) and delay sensitivity (rho = .35, p = .008) in the gain condition, but not in the loss condition (ps > .74) (). No significant associations were found between participants’ self-reported reward (BAS-reward) or punishment sensitivity (BIS) with their amount sensitivity in the gain and loss condition, respectively (ps > .36).
Figure 5. Relationship between sensitivity to delay and self-reported daily-life delay aversion measured with the Quick Delay Questionnaire (QDQ) for (a) gains and (b) losses. Individuals who reported to be more delay averse were more sensitive to delay in the gain condition, but not in the loss condition.
Discussion
This study examined the contribution of delay aversion to “impulsive” choice in ADHD by measuring both gain and loss discounting using an experiential delay discounting task in which all gains and losses, and all delays, were experienced. Importantly, in contrast to previous research, we included a condition in which participants had to choose between larger immediate and smaller delayed losses. On the basis of the delay aversion model, proposing that individuals with ADHD are delay averse, we predicted that adolescents with ADHD would be less willing to wait for both gains and losses. Our main AUC findings showed that groups differed from each other in their willingness to wait for larger gains, but not for smaller losses, although it should be noted that effect sizes for the gain and loss condition were both in the medium range (d = 0.53 and 0.44, respectively), comparable to a recent meta-analysis by Patros et al. (Citation2016) (d = 0.47). In other words, adolescents with ADHD appeared to be only slightly more willing to pay more money than controls in order to minimize waiting times. This suggests that delay aversion in ADHD seems to be context dependent. Furthermore, mixed-model analyses showed that the ADHD group was more sensitive to delay than the control group, but only in the gain condition. Finally, higher levels of self-reported delay aversion in daily life were associated with more immediate gain choices, but not with immediate loss choices. Together, these results are not fully supportive of the delay aversion model in a broader sense. To our knowledge, existing research on delay aversion in ADHD so far has focused exclusively on delays preceding gains. Our findings suggest that adolescents with ADHD might be especially averse to delays preceding gains and less to delays preceding losses, and may warrant further refinement of the delay aversion model of ADHD.
In addition to the group difference in delay discounting of gains, the ADHD group differed significantly from the control group on several other measures. As expected, the ADHD group scored higher on questionnaires that assess inattention and hyperactivity/impulsivity symptoms, but also on trait impulsivity, and delay discounting and delay aversion in daily life. In line with reaction time studies (Kofler et al., Citation2013), participants with ADHD were slower in responding during the discounting task and more variable in their response times than controls (see supplemental data). Our sample therefore appears to comprise a representative ADHD and control group.
Our AUC findings suggest that adolescents with ADHD are not willing to pay more money than controls to minimize waiting times. In addition to this classical AUC approach, the mixed-model analysis approach enabled us to examine the contributions of delay sensitivity and amount sensitivity to “impulsive” choice, thus giving more insight into the underlying processes involved. These analyses suggest that delay sensitivity plays an important role in the relatively strong preference for smaller immediate gains in individuals with ADHD compared to controls, while this was not the case for losses. In general, for gains, the relatively impatient participants (across groups) appear to be strongly driven by their sensitivity to delay, and less by their sensitivity to amount. The relatively patient participants, however, appear to be mostly driven by their sensitivity to amount. This is in line with findings from another study in our laboratory that examined delay discounting of gains in typically developing adolescents (de Water et al., Citation2017). It emphasizes the need to consider individual differences in choice behavior, as different factors appear to underlie choices for those individuals at the most patient versus those at the most impatient end of the spectrum. For losses, relatively impatient participants also appeared to be mainly driven by their sensitivity to delay. Interestingly, though, relatively patient participants were not driven by their sensitivity to the amount of the delayed loss, as was the case for gains. It should be noted, though, that the lack of an interaction between group and delay in model 1 (gains) seems inconsistent with these findings. This discrepancy may be due to the fact that testing moderation by including interaction terms is less powerful (i.e., increased Type II error) than using t tests to directly compare two groups (caused by larger standard errors of interaction terms). This has led some researchers to argue that t tests may be a more appropriate method to test for moderation of effects (Robinson, Tomek, & Schumacker, Citation2013).
Despite the finding that delay sensitivity appears to underlie choices for larger immediate losses, our other findings, such as a lack of association between delay aversion measured with the QDQ and loss discounting behavior, suggest that delay aversion does not appear to be driving “impulsive” choice in our loss discounting task. Thus, it seems that delay aversion is especially related to gains, and does not extend to losses to the same degree. We should, however, be careful when interpreting these results, as there were many participants who did not show any loss discounting at all (14 ADHD and 17 control participants; 9 ADHD and 16 control participants did not show any gain discounting). This may have resulted in a ceiling effect and reduced power to find significant effects. Results could perhaps have been different if the delays involved would have been longer and/or the amounts at stake higher. Future studies are, therefore, needed to see whether loss discounting truly differs from gain discounting.
Our findings suggest that the context in which waiting occurs is important. Waiting for gains appears to be more difficult for adolescents with ADHD than for controls when an immediate gain option is available. Aversion to a relatively large loss, on the other hand, seems to outweigh aversion to delay in most individuals. The items of the QDQ that target delay aversion in daily life (Clare et al., Citation2010) do not include this type of context. For example, “I am usually calm when I have to wait in queues” and “Having to wait for things makes me feel stressed and tense” do not imply whether the waiting is related to something rewarding or punishing. Delay aversion scores, however, were only significantly correlated with delay sensitivity in the gain condition. Perhaps, in the case of (monetary) loss, individuals with ADHD are able to overrule their aversion to delay in order to choose economically. Scheres, Tontsch, and Thoeny (Citation2013) showed that youth with ADHD were more likely to act upon their (negative) feelings in a typical delay discounting task with gains only, i.e., they were less likely to wait for larger gains than controls, even though they rated waiting as equally difficult. While controls might be able to overrule their negative feelings associated with waiting for both larger gains and smaller losses, adolescents with ADHD might only be able to overrule these when losses are involved. This implies that adolescents with ADHD are equally sensitive or even more sensitive to (monetary) loss than controls, which argues against the idea that ADHD is associated with decreased sensitivity to punishment (Luman, Tripp, & Scheres, Citation2010; van Meel, Oosterlaan, Heslenfeld, & Sergeant, Citation2005). A recent questionnaire study by Luman, van Meel, Oosterlaan, and Geurts (Citation2012) also lacked support for decreased punishment sensitivity in ADHD, and in our current sample, we also found no significant group difference on the BIS subscale of the BIS/BAS (). An earlier study by Luman, Oosterlaan, Knol, and Sergeant (Citation2008) showed that children with ADHD were, unlike controls, blind to the magnitude of a loss, but they were just as sensitive to its frequency. If the magnitude of a loss does not matter to them, then steeper discounting (preferring the sooner larger loss) in our loss condition would have been expected, but this was not the case. Most studies to date, however, have focused on reward sensitivity in ADHD, and less on punishment sensitivity. More research is needed on the latter topic in order to understand loss-based decision-making in ADHD.
According to the delay aversion model, delay aversion develops due to negative experiences with delay, which is thought to be related to disturbances in the brain’s reward circuit. Neuroimaging studies in ADHD have rather consistently shown decreased activation in the ventral striatum (VS) in adults with ADHD while anticipating (delayed) reward (for an overview see Plichta and Scheres, Citation2014). Functional MRI studies specifically examining delay aversion in ADHD suggest an important role for the amygdala. Increased amygdala activation has been found in individuals with ADHD compared to controls in response to cues of impending delay (Lemiere et al., Citation2012; Van Dessel et al., Citation2018), as well as with increasing length of anticipated (Wilbertz et al., Citation2013) and experienced (Mies et al., Citation2018) delay. This suggests that delays carry a stronger emotional value or salience for individuals with ADHD than for others. Since loss discounting appears to be less strongly related to delay aversion than gain discounting, it is possible that the associated neural responses differ too. Future studies should thus examine the underlying neural mechanisms of loss-based decision-making as compared to reward-based decision making in ADHD.
Several limitations of this study are worth mentioning. We found less discounting than expected in both the gain and loss task, and especially the loss condition appeared to suffer from a ceiling effect (but there was a main effect of delay in both conditions (results not shown), providing support for discounting, see also ). It should be noted that the same group of participants performed a delay and effort discounting (DD-ED) task (reported elsewhere) just prior to the gains and losses task, in which also a small – but statistically significant – group difference emerged in discounting of gains. It is possible that extensive experience with this type of task led to less discounting in the current task. Waiting resulted in more monetary gain in the DD-ED task, and since participants received this money just before starting the gain and loss task, this may have made waiting in this second task more appealing for participants. Future studies may want to experiment with longer delay durations in order to diminish ceiling effects in discounting behavior. Alternatively, it is possible that participants were mentally fatigued after having performed for some time already, leaving limited resources for self-control (e.g., Baumeister, Vohs, & Tice, Citation2007), which is thought to lead to more discounting instead. Finally, the sample size did not allow us to control for group differences in ODD, CD, internalizing problems (depression, anxiety), and ASD symptoms in the analyses. We also could not reliably rule out potential effects from (long-term) stimulant use in our ADHD sample. We can thus not rule out the possibility that our findings may be driven by other factors which are (inherently) associated with ADHD.
In conclusion, we found no clear evidence for a general aversion to delay in adolescents with ADHD. Together, the AUC and mixed-model findings suggest that adolescents with ADHD have a stronger preference for smaller immediate gains over larger delayed gains than controls, but that this does not extend to the same degree to losses. Hence, the findings suggest that delay aversion in ADHD is stronger for gains than losses.
Supplemental data
Download PDF (385.6 KB)Acknowledgments
This study was supported by a VIDI-grant (016.105.363) from the Netherlands Organisation for Scientific Research (NWO) awarded to Dr. Scheres. We thank all participants and their parents. We thank Maria Lojowska and Marjolein van Donkelaar for designing and programming the task, Ili Ma, Marjolein van Donkelaar and Jana Kruppa for their help in data collection, Jennifer Dicker for her help in data entry, and Karakter Child and Adolescent Psychiatry University Centre and the Ambulatorium for their help in recruiting participants.
Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
Notes
1 Four participants were in partial remission on the basis of the DISC-IV, CBCL, and DBDRS.
2 All participants used methylphenidate except for one who used dexamphetamine. This latter participant reported last intake 23 h prior to participation.
3 Shapiro–Wilk tests indicated that none of the BLUPs were normally distributed; all ps< .001.
References
- Achenbach, T. M., and Rescorla, L. A. (2001). Manual for the ASEBA school-age forms & profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
- Baayen, R. H. (2004). Statistics in psycholinguistics: A critique of some current gold standards. Mental Lexicon Working Papers in Psycholinguistics, 1, 1–45.
- Barr, D. J., Levy, R., Scheepers, C., and Tily, H. J. (2013). Random effects structure for confirmatory hypothesis testing: Keep it maximal. Journal of Memory and Language, 68(3), 255–278. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3881361/
- Bates, D., Mächler, M., Bolker, B., and Walker, S. (2015). Fitting linear mixed-effects models using lme4. Sparse Matrix Methods; Linear Mixed Models; Penalized Least Squares; Cholesky Decomposition, 67(1), 48. Retrieved from https://www.jstatsoft.org/index.php/jss/article/view/v067i01
- Baumeister, R. F., Vohs, K. D., and Tice, D. M. (2007). The strength model of self-control. Current Directions in Psychological Science, 16(6), 351–355.
- Boettiger, C. A., Mitchell, J. M., Tavares, V. C., Robertson, M., Joslyn, G., D’Esposito, M., and Fields, H. L. (2007). Immediate reward bias in humans: Fronto-parietal networks and a role for the catechol-O-methyltransferase 158(Val/Val) genotype. Journal of Neuroscience, 27(52), 14383–14391. [Research Support, Non-U.S. Gov’t Research Support, U.S. Gov’t, Non-P.H.S.]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/18160646
- Carver, C. S., and White, T. L. (1994). Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS scales. Journal of Personality and Social Psychology, 67, 319–333.
- Clare, S., Helps, S., and Sonuga-Barke, E. J. (2010). The quick delay questionnaire: A measure of delay aversion and discounting in adults. Attention Deficit and Hyperactivity Disorders, 2(1), 43–48. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/21432589
- Constantino, J. N., and Gruber, C. P. (2005). Social responsiveness scale (SRS). Los Angeles, CA: Western Psychological Services.
- de Water, E., Mies, G. W., Figner, B., Yoncheva, Y., van den Bos, W., Castellanos, F. X., … Scheres, A. (2017). Neural mechanisms of individual differences in temporal discounting of monetary and primary rewards in adolescents. Neuroimage, 153, 198–210.
- Eppinger, B., Nystrom, L. E., and Cohen, J. D. (2012). Reduced sensitivity to immediate reward during decision-making in older than younger adults. PLoS One, 7(5), e36953. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3359996/
- Estle, S. J., Green, L., Myerson, J., and Holt, D. D. (2006). Differential effects of amount on temporal and probability discounting of gains and losses. Memory and Cognition, 34(4), 914–928. [Research Support, N.I.H., Extramural]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/17063921
- Foerde, K., Figner, B., Doll, B. B., Woyke, I. C., Braun, E. K., Weber, E. U., and Shohamy, D. (2016). Dopamine modulation of intertemporal decision-making: Evidence from Parkinson disease. Journal of Cognitive Neuroscience, 28(5), 657–667.
- Hartman, C. A., Geurts, H. M., Franke, B., Buitelaar, J. K., and Rommelse, N. N. J. (2016). Changing ASD-ADHD symptom co-occurrence across the lifespan with adolescence as crucial time window: Illustrating the need to go beyond childhood. Neuroscience & Biobehavioral Reviews, 71, 529–541. Retrieved from http://www.sciencedirect.com/science/article/pii/S0149763416301166
- Jackson, J. N. S., and MacKillop, J. (2016). Attention-deficit/hyperactivity disorder and monetary delay discounting: A meta-analysis of case-control studies. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 1(4), 316–325. Retrieved from http://www.sciencedirect.com/science/article/pii/S2451902216000914
- Kofler, M. J., Rapport, M. D., Sarver, D. E., Raiker, J. S., Orban, S. A., Friedman, L. M., and Kolomeyer, E. G. (2013). Reaction time variability in ADHD: A meta-analytic review of 319 studies. Clinical Psychology Review, 33(6), 795–811. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/23872284
- Kort, W., Schittekatte, M., Compaan, E. L., Bosmans, M., Bleichrodt, N., Vermeir, G., … Verhaeghe, P. (2002). WISC-III NL. Handleiding. London: The Psychological Corporation.
- Lemiere, J., Danckaerts, M., Van Hecke, W., Mehta, M. A., Peeters, R., Sunaert, S., and Sonuga-Barke, E. (2012). Brain activation to cues predicting inescapable delay in adolescent attention deficit/hyperactivity disorder: An fMRI pilot study. Brain Research, 1450, 57–66. [Research Support, Non-U.S. Gov’t]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22406068
- Luman, M., Oosterlaan, J., Knol, D. L., and Sergeant, J. A. (2008). Decision-making in ADHD: Sensitive to frequency but blind to the magnitude of penalty? Journal of Child Psychology and Psychiatry, and Allied Disciplines, 49(7), 712–722. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/18422549
- Luman, M., Tripp, G., and Scheres, A. (2010). Identifying the neurobiology of altered reinforcement sensitivity in ADHD: A review and research agenda. Neuroscience and Biobehavioral Reviews, 34(5), 744–754. [Review]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19944715
- Luman, M., van Meel, C. S., Oosterlaan, J., and Geurts, H. M. (2012). Reward and punishment sensitivity in children with ADHD: Validating the sensitivity to punishment and sensitivity to reward questionnaire for children (SPSRQ-C). Journal of Abnormal Child Psychology, 40(1), 145–157. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/21789519
- Luman, M., Van Meel, C. S., Oosterlaan, J., Sergeant, J. A., and Geurts, H. M. (2009). Does reward frequency or magnitude drive reinforcement-learning in attention-deficit/hyperactivity disorder? Psychiatry Research, 168(3), 222–229. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19545907
- Marco, R., Miranda, A., Schlotz, W., Melia, A., Mulligan, A., Müller, U., … Sonuga-Barke, E. J. S. (2009). Delay and reward choice in ADHD: An experimental test of the role of delay aversion. Neuropsychology, 23(3), 367–380.
- Mies, G. W., De Water, E., and Scheres, A. (2016). Planning to make economic decisions in the future, but choosing impulsively now: Are preference reversals related to symptoms of ADHD and depression? International Journal of Methods in Psychiatric Research, 25(3), 178–189. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/27199170
- Mies, G. W., Ma, I., De Water, E., Buitelaar, J. K., and Scheres, A. (2018). Waiting and working for rewards: Attention-deficit/hyperactivity disorder is associated with steeper delay discounting linked to amygdala activation, but not with steeper effort discounting. Cortex, 106, 164-173. Retrieved from https://www.sciencedirect.com/science/article/pii/S0010945218301746
- Myerson, J., Green, L., and Warusawitharana, M. (2001). Area under the curve as a measure of discounting. Journal of the Experimental Analysis of Behavior, 76(2), 235–243. [Research Support, Non-U.S. Gov’t Research Support, U.S. Gov’t, P.H.S.]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11599641
- Oosterlaan, J., Scheres, A., Antrop, I., Roeyers, H., and Sergeant, J. A. (2000). Vragenlijst voor Gedragsproblemen bij Kinderen (VvGK). Nederlandse bewerking van de Disruptive Behavior Disorders Rating Scale [Dutch translation of the disruptive behavior disorders rating scale]. Lisse: Swets Test Publishers.
- Patros, C. H. G., Alderson, R. M., Kasper, L. J., Tarle, S. J., Lea, S. E., and Hudec, K. L. (2016). Choice-impulsivity in children and adolescents with attention-deficit/hyperactivity disorder (ADHD): A meta-analytic review. Clinical Psychology Review, 43, 162–174. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/26602954
- Patton, J. H., Stanford, M. S., and Barratt, E. S. (1995). Factor structure of the Barratt impulsiveness scale. [Research Support, Non-U.S. Gov’t]. Journal of Clinical Psychology, 51(6), 768–774. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8778124
- Pelham, W. E., Jr., Gnagy, E. M., Greenslade, K. E., and Milich, R. (1992). Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 31(2), 210–218. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1564021
- Plichta, M. M., and Scheres, A. (2014). Ventral-striatal responsiveness during reward anticipation in ADHD and its relation to trait impulsivity in the healthy population: A meta-analytic review of the fMRI literature. [Peer Reviewed]. Neuroscience and Biobehavioral Reviews, 38, 125–134.
- R Core Team, 2013. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, URL: http://www.R-project.org/.
- Robinson, C. D., Tomek, S., and Schumacker, R. E. (2013). Tests of moderation effects: Difference in simple slopes versus the interaction term. Multiple Linear Regression Viewpoints, 39(1), 16–24.
- Roeyers, H., Thys, M., Druart, C., De Schryver, M., and Schittekatte, M. (2011). SRS Screeningslijst voor Autismespectrumstoornissen. Amsterdam: Hogrefe Uitgevers.
- Scheres, A., de Water, E., and Mies, G. W. (2013). The neural correlates of temporal reward discounting. Wiley Interdisciplinary Reviews. Cognitive Science, 4(5), 523–545. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/26304244
- Scheres, A., Dijkstra, M., Ainslie, E., Balkan, J., Reynolds, B., Sonuga-Barke, E., and Castellanos, F. X. (2006). Temporal and probabilistic discounting of rewards in children and adolescents: Effects of age and ADHD symptoms. Neuropsychologia, 44(11), 2092–2103. [Clinical Trial Research Support, N.I.H., Extramural]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/16303152
- Scheres, A., Tontsch, C., and Thoeny, A. L. (2013). Steep temporal reward discounting in ADHD-Combined type: Acting upon feelings. Psychiatry Research, 209(2), 207–213. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/23347551
- Scheres, A., Tontsch, C., Thoeny, A. L., and Kaczkurkin, A. (2010). Temporal reward discounting in attention-deficit/hyperactivity disorder: The contribution of symptom domains, reward magnitude, and session length. Biological Psychiatry, 67(7), 641–648. [Research Support, N.I.H., Extramural]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/20034616
- Singmann, H., Bolker, B., and Westfall, J. (2015). afex: Analysis of factorial experiments (R package version 0.13-145).
- Snaith, R. P., Hamilton, M., Morley, S., Humayan, A., Hargreaves, D., and Trigwell, P. (1995). A scale for the assessment of hedonic tone the Snaith-Hamilton pleasure scale. The British Journal of Psychiatry : The Journal of Mental Science, 167(1), 99–103. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=7551619
- Sonuga-Barke, E. J., Dalen, L., and Remington, B. (2003). Do executive deficits and delay aversion make independent contributions to preschool attention-deficit/hyperactivity disorder symptoms? Journal of the American Academy of Child and Adolescent Psychiatry, 42(11), 1335–1342. [Research Support, Non-U.S. Gov’t]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/14566171
- Sonuga-Barke, E. J., Taylor, E., Sembi, S., and Smith, J. (1992). Hyperactivity and delay aversion–I. The effect of delay on choice. [Research Support, Non-U.S. Gov’t]. Journal of Child Psychology and Psychiatry and Allied Disciplines, 33(2), 387–398. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1564081
- Tanaka, S. C., Yamada, K., Yoneda, H., and Ohtake, F. (2014). Neural mechanisms of gain-loss asymmetry in temporal discounting. The Journal of Neuroscience, 34(16), 5595–5602. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/24741049
- Thaler, R. (1981). Some empirical evidence on dynamic inconsistency. Economics Letters, 8(3), 201–207. Retrieved from http://EconPapers.repec.org/RePEc:eee:ecolet:v:8:y:1981:i:3:p:201-207
- Thorell, L. B., Sjöwall, D., Mies, G. W., and Scheres, A. (2017). Quick delay questionnaire: Reliability, validity, and relations to functional impairments in adults with attention-deficit/hyperactivity disorder (ADHD). Psychological Assessment, 29(10), 1261–1272. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/27991822
- Tripp, G., and Alsop, B. (2001). Sensitivity to reward delay in children with attention deficit hyperactivity disorder (ADHD). Journal of Child Psychology and Psychiatry and Allied Disciplines, 42(5), 691–698. [Research Support, Non-U.S. Gov’t]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11464973
- Van Dessel, J., Sonuga-Barke, E., Mies, G., Lemiere, J., Van der Oord, S., Morsink, S., and Danckaerts, M. (2018). Delay aversion in attention deficit/hyperactivity disorder is mediated by amygdala and prefrontal cortex hyper-activation. Journal of Child Psychology and Psychiatry, 59, 888–899.
- van Meel, C. S., Oosterlaan, J., Heslenfeld, D. J., and Sergeant, J. A. (2005). Telling good from bad news: ADHD differentially affects processing of positive and negative feedback during guessing. [Controlled Clinical Trial]. Neuropsychologia, 43(13), 1946–1954. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15878183
- Wilbertz, G., Trueg, A., Sonuga-Barke, E. J., Blechert, J., Philipsen, A., and Tebartz van Elst, L. (2013). Neural and psychophysiological markers of delay aversion in attention-deficit hyperactivity disorder. Journal of Abnormal Psychology, 122(2), 566–572. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/23713509