
ABSTRACT
Cognitive processes play an imperative role in children’s mathematics learning. Difficulties in cognitive functioning are a core feature of Attention Deficit Hyperactivity Disorder (ADHD) in children, who also tend to show lower levels of mathematics attainment than their typically developing peers. This review (registration number: CRD42020169708) sought to aggregate findings from studies assessing the relationship between cognition and mathematics in children with a clinical ADHD diagnosis aged 4–12 years. A total of 11,799 studies published between 1992 and August 2020 were screened for eligibility using various database (PsycINFO, PubMed, SCOPUS, EMBASE, ERIC, Web of Science, and additional sources), from which four studies met inclusion criteria. A narrative synthesis was conducted on the correlations between mathematics and cognitive domains, including an evaluation of the risk of bias within the studies. Across four studies meeting inclusion criteria, memory, inhibitory control, and processing speed were assessed. The results showed a positive association between cognition and mathematics performance in this population. The strength of associations across these studies varied as a function of the cognitive domain in question, means by which mathematics performance was assessed, as well as whether confounding factors such as age and IQ were controlled for. Collectively, this review demonstrates a lack of research in this area and points to various methodological considerations for identifying the association between cognition and mathematics performance in ADHD.
Attention Deficit Hyperactivity Disorder (ADHD) is one of the most common neurodevelopmental disorders with global prevalence rates of around 5% (G. Polanczyk et al., Citation2007; G. v. Polanczyk et al., Citation2014). Although ADHD was previously regarded as a childhood disorder, it is now recognized as a lifespan condition with difficulties persisting well into adulthood (Biederman et al., Citation2010; Döpfner et al., Citation2015; Faraone et al., Citation2006; Harpin, Citation2005). Long-term functional adversities are documented in behavioral, socioemotional, educational, and occupational domains (Klein et al., Citation2012; Kuriyan et al., Citation2013). Educational risks are of particular concern given their inherent contribution to future outcomes across the lifespan (Duncan et al., Citation2007; Klein et al., Citation2012). Core ADHD symptoms of inattention, impulsivity, and hyperactivity can have negative effects on children’s academic functioning, increasing susceptibility to a myriad of educational difficulties (Arnold et al., Citation2020; Daley & Birchwood, Citation2010; Loe & Feldman, Citation2007). Previous research indicates an ADHD diagnosis can have especially negative consequences on children’s level of mathematics attainment (Mayes et al., Citation2020; Silva et al., Citation2020). However, the precise mechanisms behind mathematics difficulties in ADHD remain contested.
Mathematics and ADHD
A previous review found that over 70% of studies in the field identified a negative association between ADHD symptoms and mathematics ability across all ages, even after controlling for a range of attenuating factors such as age, socioeconomic status, IQ, and psychostimulant medication (Tosto et al., Citation2015). Notably, symptoms of inattention showed stronger associations with mathematics than hyperactivity-impulsivity, implicating attentional processes as particularly important to mathematics ability. According to the clinical symptom model, difficulties in sustaining attention impede upon processes that promote successful learning and academic functioning, such as focusing on classroom activities, following instructions, and completing homework (Calub et al., Citation2019). This is supported by research linking diminished attention with lower mathematics performance as indexed by teacher ratings and standardized achievement tests (Breslau et al., Citation2009; Calub et al., Citation2019; Duncan et al., Citation2007). Nonetheless, pharmacological treatment aimed at alleviating clinical ADHD symptoms leads to only marginal and short-lived improvements in mathematics attainment, suggesting that factors other than behavioral inattention symptoms are involved (Baweja et al., Citation2015; DuPaul et al., Citation2016; Kortekaas-Rijlaarsdam et al., Citation2019; Molina et al., Citation2009).
Other research suggests that mathematics underachievement in ADHD may be due to generally lower levels of intellectual functioning (Calub et al., Citation2019; Duckworth et al., Citation2012; Frazier et al., Citation2004; Mayes et al., Citation2009). However, significant associations between IQ and mathematics performance are likely propelled by the large overlap between conventional IQ tests and higher order cognitive processes on which many children with ADHD struggle with (Antonini et al., Citation2016; Coghill et al., Citation2014; Dennis et al., Citation2009). Therefore, another plausible explanation is that higher order cognitive processes, responsible for regulating attention, modulate mathematics performance (L. M. Friedman et al., Citation2018; Rapport et al., Citation2008; Thorell, Citation2007).
The role of cognition in mathematics
Cognitive difficulties in children with ADHD are frequently documented in Executive Functions (EF), memory, processing speed, temporal processing, delay aversion, and motor control (Coghill et al., Citation2014; S. Rhodes et al., Citation2004; Rhodes et al., Citation2005, Citation2006; Sonuga-Barke et al., Citation2010). Of these, EF, memory, and processing speed have been implicated in children’s mathematics performance (Bellon et al., Citation2016; Bull & Lee, Citation2014; Cai et al., Citation2016; Cragg et al., Citation2017; Formoso et al., Citation2018; Geary, Citation2004; Gilmore et al., Citation2015; LeFevre et al., Citation2013; Sturm et al., Citation2018; Szucs et al., Citation2013; Verguts & Fias, Citation2005). Particular focus has been given to EF mechanisms due to their strong affiliations with attention regulation (Barkley, Citation1997; see reviews by Bull & Lee, Citation2014; Gilmore et al., Citation2018). EF are a set of higher-order cognitive processes responsible for managing goal-oriented behaviors and, typically, these include response inhibition, cognitive flexibility, working memory, and planning (Diamond, Citation2013; Miyake et al., Citation2000).
In the context of mathematics, inhibition can help suppress retrieval of related but incorrect solutions from memory (e.g., inhibit 8 when being asked to 4 × 4 = ? De Visscher & Noël, Citation2014) and curb automatically activated solution strategies in favor of more efficient ones (Lemaire & Lecacheur, Citation2011; Robinson & Dubé, Citation2013). Cognitive flexibility helps facilitate effortless shifting between different problem steps, operations (e.g., addition and subtraction), and notations (e.g., verbally presented digits and written Arabic symbols; Robinson & Dubé, Citation2013; Siegeler & Araya, Citation2005), although the evidence for its role is mixed (Bull & Scerif, Citation2001; Clark et al., Citation2010; Cragg et al., Citation2017). Working memory consistently emerges as one of the strongest predictors of children’s mathematics performance (Cragg et al., Citation2017; K. Lee et al., Citation2012; Monette et al., Citation2011). Working memory supports encoding and retrieval of arithmetic facts in long-term memory store through repeated practice (Cragg et al., Citation2017; Gremillion & Martel Citation2012) and regulating, manipulating, and updating verbally and spatially presented numerical information “online” (Cragg et al., Citation2017). The domain of planning has also been associated with children’s mathematics ability (Best et al., Citation2009; Lai et al., Citation2019; Sikora et al., Citation2002). Planning skills help organize knowledge and promote correct execution of a sequence of steps on more complex computations and its unique contribution has been demonstrated above and beyond working memory capacity (Cai et al., Citation2016; Davidson et al., Citation1994; Dowker, Citation2005; Rourke, Citation1993).
Considerable evidence suggests that EF task performance is compromised in children with ADHD when compared to their typically developing peers (Coghill et al., Citation2014; Kofler et al., Citation2018; Nigg et al., Citation2005; Willcutt et al., Citation2005). Moreover, ADHD-associated decrements in EF task performance are often accompanied by substantial group differences in mathematics attainment (Antonini et al., Citation2016; Biederman et al., Citation2004; Holmes et al., Citation2014; L. M. Friedman et al., Citation2018). However, in attempting to explore the cognitive mechanisms by which such group differences arise, studies focus on a select one or two EF components (e.g., Antonini et al., Citation2016; Gremillion & Martel, Citation2012). A global account of all domains is therefore necessary to help ascertain the relative principality of correlated EF processes.
Cognitive signatures of mathematics performance have also been extended to cognitive processes without substantial executive processing. This includes modality-specific verbal and visuospatial storage systems responsible for encoding and retrieval of information in short-term memory (short-term memory) in the absence of active processing (Baddeley & Hitch, Citation1974). Disruptions to visuospatial and linguistic information representation mechanisms hinder long-term memory (long-term memory) storage and retrieval of basic number facts (Cragg et al., Citation2017; Geary, Citation2004). Indeed, short-term memory, impaired in many children with ADHD (Rapport et al., Citation2008; Rhodes et al., Citation2005, Citation2012), is crucial for establishing networks for learned facts and retrieving these from long-term memory via linguistic and spatial codes (Dehaene & Cohen, Citation1995; Holmes & Adams, Citation2006). short-term memory has been identified as an important predictor of mathematics performance, although studies yield mixed results on the relative contributions of phonological and visuospatial storage domains (Bull et al., Citation2008; Gathercole et al., Citation2006; Passolunghi et al., Citation2014; Swanson & Kim, Citation2007). Phonological short-term memory appears to be crucial for encoding and processing verbal codes for numbers, fundamental to elementary aspects of mathematics learning such as counting and arithmetic fact retrieval from long-term memory (Andersson, Citation2010; Geary et al., Citation2008). Meanwhile, visuospatial memory becomes progressively more important with age as it taxes visualization and representation of quantities that support more advanced aspects of mathematics problem solving (Cragg et al., Citation2017; Holmes & Adams, Citation2006; Li et al., Citation2013). Thus, age and the type of mathematics assessment used can impact the relative engagement of phonological versus visuo-spatial storage domains.
Another important cognitive construct is processing speed – the efficiency with which relatively simple and automated cognitive tasks are executed (Shanahan et al., Citation2006). Children with ADHD generally show slower processing speed than their typically developing peers, although studies yield mixed results (Calhoun & Mayes, Citation2005; Goth-Owens et al., Citation2010; Jacobson et al., Citation2011; Nikolas & Nigg, Citation2013). This variability is proposed to stem from the broad range of measures used to index processing speed, including reaction time, perceptual speed, psychomotor speed, and decision speed (Kibby et al., Citation2019; Salthouse, Citation2000). There is evidence to suggest that processing speed affects mathematics achievement indirectly through its effects on EF (Cassidy et al., Citation2016; Rose et al., Citation2011). Processing speed facilitates the fluency with which children compute solutions during simple arithmetic by minimizing decay in working memory and by creating stronger associations for these in long-term memory (Bull & Johnston, Citation1997; Cirino et al., Citation2015; Fuchs et al., Citation2006, Citation2008, Citation2010). Nonetheless, the role of processing speed may vary as a function of the mathematics domain being assessed, with research showing direct associations when assessing basic arithmetic, and indirectly during more complex mathematics problem-solving tasks (Fuchs et al., Citation2006, Citation2008, Citation2010; Rose et al., Citation2011).
Methodological considerations
Exploring cognitive and mathematics performance in children with ADHD warrants consideration of various methodological issues. One issue relates to inclusion of children receiving medication at the time of assessment (e.g., DuPaul et al., Citation2004; Efron et al., Citation2014). Medication treatment is a confounding factor in ADHD research, which can underestimate the relationship between EF and mathematics due to documented benefits on neurocognitive and academic performance (e.g., Hawk et al., Citation2018; Kortekaas-Rijlaarsdam et al., Citation2019; Leo & Cohen, Citation2003; Powers et al., Citation2008). As such, the literature would benefit from a comprehensive assessment of these associations in the absence of active stimulant treatment. In doing so, the current review can help inform possible targets for intervention free from pharmacological effects and inform alternative remediation strategies.
Moreover, a range of approaches have been employed to assess mathematics performance including both individual and combined indices of arithmetic fluency, word problems, reasoning, and numerical operations (e.g., Antonini et al., Citation2016; Capodieci & Martinussen, Citation2017; Holmes et al., Citation2014; L. M. Friedman et al., Citation2018; Sabagh-Sabbagh & Pineda, Citation2010). The type of assessment used will influence the conclusions that can be drawn on the importance of cognitive domains for mathematics performance, and ultimately, their suitability as targets for intervention (Allen et al., Citation2019). As such, any review should consider more intricate aspects of numerical abilities, as well as broad attainment scores.
Lastly, children with ADHD present with highly heterogeneous cognitive profiles (Coghill et al., Citation2014; Luo et al., Citation2019; Nigg et al., Citation2005; Willcutt et al., Citation2005), and not all children with ADHD struggle with mathematics (Capano et al., Citation2008; Czamara et al., Citation2013; Mayes et al., Citation2020; Shalev et al., Citation1995). High rates of co-occurrences with other neurodevelopmental disorders such as Oppositional Defiant Disorder (ODD), Conduct Disorder (CD), Autism Spectrum Disorder, Developmental Coordination Disorder, and learning difficulties may exacerbate difficulties in mathematics performance (Liu et al., Citation2017; Capano et al., Citation2008; Czamara et al., Citation2013; Rasmussen & Gillberg, Citation2000; Zajic et al., Citation2018). It is therefore important to consider screening efforts across studies to explore the representativeness of the clinical ADHD population.
Objectives
A previous review explored the association between ADHD symptoms of inattention, hyperactivity, and impulsivity, and mathematics performance (Tosto et al., Citation2015). However, cognition rather than behavioral symptoms appear to be more closely affiliated with children’s mathematics performance. To date, there has been now systematic exploration of the correlations between cognitive processes and mathematics performance in children with ADHD. The aim of this review was to explore the literature on the association between key cognitive processes and mathematics performance in children aged 4–12 years with a clinical diagnosis of ADHD. Specifically, this review examines the strength of association between objectively assessed performance on cognitive tasks and children’s mathematics performance. Specifically, previously implicated cognitive domains in ADHD were included: inhibitory control, cognitive flexibility, visuospatial and verbal working memory, planning, processing speed, as well as short- and long-term memory. Furthermore, this review was interested in both standardized attainment scores, as well as non-standardized indices of numerical skills. The key outcome of interest were the correlations between cognitive and mathematics scores. In doing so, the current review will help conceptualize the cognitive correlates of mathematics performance in children with ADHD and highlight potential avenues for early interventions aimed at improving mathematics skills. From an applied perspective, establishing the cognitive mechanisms which correlate with mathematics performance in ADHD can act as a steppingstone in formulating predictive models and help in educational developments of instructional design and practice.
Method
The protocol for this review was registered with the International Prospective Register of Systematic Reviews PROSPERO; registration number CRD42020169708 available from http://www.crd.york.ac.uk/prospero. To ensure clarity and transparency of search strategy and procedures reporting, the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist was used (Supplement File 1; Moher et al., Citation2015).
Eligibility criteria
The PICOTS (Population, Intervention (here we refer to this as Assessment), Comparison, Outcomes, Timeframe, and Study Design) framework was used to devise a study screening criterion. This review focused on papers published between 1992 (for ICD-10-based diagnoses) or 1994 (for DSM-IV-based diagnoses) to 2020 in peer-reviewed journals written in English for which full text was available.
Population
Aligning with UK-wide primary school years, studies with children aged between 4 and 12 years recruited through clinical, community, or population-based studies were included. Recommended guidelines for ADHD assessment and treatment typically begin at age four (Wolraich et al., Citation2019). Children aged over 12 were excluded as this review focuses on primary school years during which basic numerical skills are mastered. Studies where the data from different age groups were aggregated in a way in which data for those aged 4–12 could not be extracted were excluded. Studies had to report a clinical diagnosis of ADHD or hyperkinetic disorder using the DSM-IV/5 or ICD-10/11 which constitute the most widely established mental health classification systems (Stein et al., Citation2013). Studies using other diagnostic criteria were excluded. A clinical diagnosis of ADHD had to be reported by a parent or identified using ADHD-validated parent rating scales or parent interviews. Additionally, diagnosis had to be corroborated via teacher verification (e.g., questionnaire or interview). Studies failing to mention teacher verification were excluded under the assumption that there was no multi-setting corroboration of difficulties – a crucial aspect of obtaining an accurate ADHD diagnosis (American Psychological Association, Citation2013). The only exception for this was where no teacher corroboration was present, but another source of confirmation was present, such as confirmation of a diagnosis by a psychiatrist or use of ADHD-medication, to which teacher corroboration is inherent.
Participants had to either (1) be drug-naive, or (2) be asked to abstain taking medication ahead of their participation in the study. Studies where participants were actively on medication during testing were excluded due to confounding effects of pharmacological treatment on cognition and academic productivity (e.g., see Hawk et al., Citation2018; Kortekaas-Rijlaarsdam et al., Citation2019; Leo & Cohen, Citation2003; Powers et al., Citation2008). Where authors failed to report medication status, a contact attempt was made to clarify medication status and if there was no response from the author, the study was excluded under the assumption that some/all participants were not subject to wash-out requirements. Participants with ADHD and other co-occurring neurodevelopmental disorder and learning difficulties were included to accommodate for well-documented co-occurrences (Elia et al., Citation2008; Lange, Citation2018; Reale et al., Citation2017). Studies with individuals with parent-reported epilepsy, Down syndrome, brain injury, or chromosomal conditions were excluded due to their specific effects on neurocognitive functioning (S. E. Lee et al., Citation2016; Ekstein et al., Citation2011; Lo-Castro et al., Citation2011). Studies including children with IQ < 70 or intellectual disability were also excluded.
Assessment
Studies were included where either of the following mathematics assessments were administered: (1) standardized tests (e.g., Wechsler Objective Numerical Dimensions; WOND), (2) non-standardized tests (e.g., number fact fluency), and/or (3) state-wide or nation-wide school-based standardized tests. Studies using school-specific achievement tests or grades were excluded due to potential discrepancies in curriculum across schools (Tosto et al., Citation2015). Studies were only included if at least one of the cognitive domains of interest was objectively assessed. Studies relying on parent/teacher ratings of cognitive function (e.g., Behavior Rating Inventory of Executive Function) were excluded due to their subjectivity and small-modest associations with objective performance-based tests (Toplak et al., Citation2013).
Comparison
Studies comparing children with ADHD to any other group were included, so long as the authors reported on the relationship between cognition and mathematics in the ADHD group.
Outcomes
The main outcome of interest was the examination of correlations between mathematics and cognitive scores. Studies were included where effect sizes between mathematic and cognition for the ADHD group were reported (e.g., correlation coefficient, beta coefficients, p-values). In studies using multiple tasks to measure a single construct, all eligible effect sizes were included. Determination of effect sizes using conversion to a common metric (r) was explored (e.g., Allen et al., Citation2019). Following extensive examination of the literature, it became apparent that calculating an effect size (e.g., Cohen’s d or Hedge’s g) from the same group (i.e., single ADHD group) using two different variables measured at a single time point (i.e., cognition and mathematics) would not be possible without access to the raw data from each of the studies, which was beyond the scope of the present review (Borenstein et al., Citation2011; Field, Citation2001; Higgins et al., Citation2019).
Timeframe
The start point for the search was set at 1994 for DSM-IV-based diagnoses and 1992 for ICD-10-based diagnoses. Studies published before 1992 (for ICD-10 research) and 1994 (for DSM-IV research) were excluded. For DSM-IV, 1994 marks the important reconceptualization from a previously regarded unitary disorder to ADHD as we know it today, with the specification of three subtypes endorsed by factor analytic research (Biederman et al., Citation1997; Lahey et al., Citation1994). For ICD, 1992 marks the publication of the critical update from the more outdated ICD-9 (published in 1976) to ICD-10 aimed at integrating more recent research and thereby providing greater accuracy of diagnoses (Taylor & Hemsley, Citation1995).
Study design
Any quantitative research where data for the association between cognition and mathematics in children with ADHD were available, including (1) case–control studies comparing children with ADHD and any other group, (2) cross-sectional studies examining the cognition and mathematics in ADHD, (3) longitudinal/cohort studies that follow up children with ADHD and children are aged 12 or younger at the end of the follow-up, or where baseline data are available for children aged 12 or younger that are followed up longitudinally, and (4) intervention/experimental studies aimed at improving mathematics or cognitive performance with available baseline (i.e., pre-intervention) data. Studies solely using qualitative research methods were excluded (e.g., ethnography, action research, social observation, focus groups, case study research). Systematic reviews, conference proceedings and protocols were excluded.
Search strategy
Search methods for study identification
Searches were conducted between March 2020 and August 2020. The following electronic databases were searched: PsycINFO, PubMed, SCOPUS, EMBASE, ERIC, and Web of Science. The search strategy was first defined by identifying three key terms from the research question: “cognition,” “mathematics” and “Attention Deficit Hyperactivity Disorder.” Common terms for these key items were extracted or adapted from previous reviews on ADHD (e.g., Tosto et al., Citation2015; Willcutt et al., Citation2012) and mathematics in children (e.g., Simms et al., Citation2019), as well as previously implicated cognitive domains of interest to ADHD (e.g., Coghill et al., Citation2018; Kofler et al., Citation2018; Willcutt et al., Citation2005) and those which have previously been suggested as important for mathematics learning (e.g., Cragg et al., Citation2017; Gilmore et al., Citation2018). The final search string terms and search strategy combinations are summarized in . Following completion of the search strategy in each of the specified databases, citations were retrieved and uploaded onto Endnote where any duplicates were removed. The list of references of included studies were also screened to identify any additional papers that may have been missed. Additionally, the reference list from a previous review of mathematics and ADHD symptoms (Tosto et al., Citation2015) was also screened.
Table 1. Search strategy key words and combinations
Screening for inclusion
Searches generated a pool of studies to be screened. In the first step, these articles were screened one of the reviewers (MK) by title and abstract using a pre-defined screening checklist (Supplement File 2; adapted from Polanin et al., Citation2019). A 20% sample was then screened by a second reviewer (JO) with an interrater agreement rate of 97%, which is deemed as acceptable (Belur et al., Citation2021; Schlosser, Citation2007). Any conflicts were initially resolved through discussion. During the second step, papers were scrutinized for eligibility (MK) by applying full-text review screening criteria (Supplement File 3; adapted from Shvedko et al., Citation2018). A 20% sample from these was screened by an independent reviewer (JO), resulting in 100% agreement. Following full-text review, four studies were deemed as eligible for inclusion.
Study selection
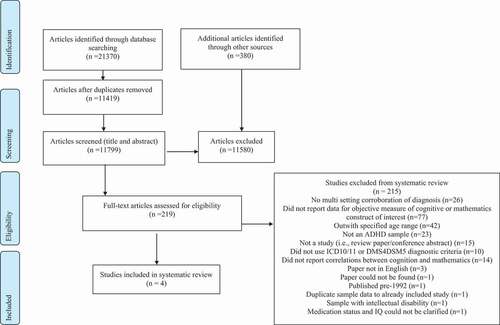
In total, 21,370 were generated from the electronic database and 380 additional studies were identified through screening reference lists. Following duplicate removal, 11,799 articles were screened by title and abstract. From these, 219 met eligibility criteria for full test screening. These were carefully sifted and reason(s) for exclusion were provided (see Supplement File 3). In total, four papers qualified to be included in the present review. A flow diagram detailing the study selection process is provided in (Moher et al., Citation2009).
Figure 1. Flow diagram of study selection process.
Data extraction
Data from the final articles included were independently and blindly extracted by two reviewers (MK & either EMC or JO) and any discrepancies were resolved through discussion. Data extraction items included information on (1) source of study (authors, publication year, country of study), (2) methods and population characteristics (study design, diagnostic criteria used, ADHD subtype, sample size, age range, mean age and SD, sex, IQ range and mean, medication status, ethnicity, SES, co-occurrences, drop outs/non completers), (3) outcome measures (mathematics assessment and domain, cognitive assessment and domain), and (4) results (r value and accountability for confounding factors). A correlation coefficients and confidence intervals were either directly extracted from each study or calculated using a freely available calculator (Lenhard & Lenhard, Citation2016; https://www.psychometrica.de/effect_size.html). For any data clarifications or missing data, corresponding authors were contacted by e-mail and a follow-up e-mail was sent after 4 weeks from initial contact date.Footnote1 Any finalized missing information is specified as “not reported” (NR).
Risk of bias
Risk of bias (RoB) was assessed using the Newcastle Ottawa Scale (NOS; Wells et al., Citation2012). The NOS is one of the most widely used tools for assessing the quality of observational research (Luchini et al., Citation2017). The NOS has been used extensively in previous systematic reviews including in ADHD populations (e.g., Cortese et al., Citation2016; Donzelli et al., Citation2020; Ruiz-Goikoetxea et al., Citation2017). Although the NOS was developed for quality assessment of case-control and cohort studies, it has previously been adapted for cross-sectional design studies (e.g., Stewart et al., Citation2017; Wang et al., Citation2017). In line with the Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Green, Citation2011), the criteria for items in the NOS were tailored to the present review by consolidating previous reviews (Donzelli et al., Citation2020; Stewart et al., Citation2017) and agreed upon by three of the reviewers (MK, SR & SMC). For case-control and cohort studies (max = 9 points) a score of ≥7 stars rendered low risk of bias, 4–6 stars qualified as medium risk of bias, and studies scoring ≤4 stars were high risk of bias. Cross-sectional studies (max = 7 points) scoring ≥5 stars were deemed as low risk of bias, 3–4 stars qualified as medium risk of bias, and studies scoring ≤3 stars were high risk of bias. Studies were not excluded based on a high RoB. Rather, this assessment was used to highlight important points for future research considerations. The RoB was completed by two independent reviewers (MK & EMC) with any discrepancies resolved through discussion.
Synthesis
The main aim of the present review was to examine the correlations between mathematics and cognitive scores in children with an ADHD diagnosis. The magnitudes of effect sizes were interpreted according to Cohen (Citation1988) as small (r = .10), medium (r = .30) or large (r = .50). The protocol set out to quantitatively synthesize the relationship between mathematics and cognition. However, only four of the included studies (Alloway, Citation2011; Friedman et al., Citation2018; Kim et al., Citation2020; Miranda-Casas et al., Citation2012) reported a statistic for the association between cognition and mathematics from which a common effect size could either be extracted or calculated. These studies assessed a wide range of cognitive constructs and mathematics domains – none of which could be combined according to meaningful commonalities in the measured characteristics. In line with previous arguments, it was decided that quantitatively synthesizing few studies with largely heterogeneous characteristics was unwarranted (Valentine et al., Citation2010). Thus, a narrative synthesis was provided.
Results
Study characteristics
Descriptive data relating to source, methods, and participants from included articles is summarized in .Footnote2 Across the four studies, there were 334 participants in total with sample sizes ranging between 24 and 224 children. Overall, 15% were girls, and participants’ ages ranged between 6 and 12 years (Age Median = 8.36 years). There were three case–control studies and one cross-sectional study. Further, three of the included studies included less than 50 participants. Included studies were also heterogeneous in terms of location comprising one study each from Spain, South Korea, UK, and USA.
Table 2. Source, methods, and population characteristics
All but one of the studies (Miranda-Casas et al., Citation2012) used standardized assessments of mathematics achievement. The descriptions of these assessments are provided in . Each assessment description was mapped onto one of three broad domains. The numerical operations domain included tasks that required children to conduct direct simple or complex arithmetic computations (Mazzocco et al., Citation2008). The numerical concepts domain included tasks that capitalized on children’s acquisition of basic numerical concepts such as counting digits or objects, reading numbers, and quantity judgments (Butterworth, Citation2005; Gallistel & Gelman, Citation1990; Gallister & Gelman, Citation1992). Lastly, applied problem solving required children to solve word problems orally and apply knowledge to real-life contexts (e.g., time, money, graphs; Swanson et al., Citation2015; Zheng et al., Citation2011). The nature of applied problem-solving tasks is such that performance inherently requires children to draw on a range of specific mathematics skills including numerical concepts and mental numerical operations. In terms of cognition, included studies assessed verbal and spatial aspects of short-term memory and working memory, inhibitory control, and processing speed. A detailed description of the tasks used to assess cognitive constructs can be found in .
Table 3. Description of mathematics assessment used by included studies
Table 4. Description of cognitive assessment used by included studies
Risk of bias
The RoB ratings of each study according to the NOS quality assessment tool are summarized in . It is important to note that the inclusion criteria used in the present review was such that these studies can be generally considered as high-quality studies. Indeed, all the studies scored either low or medium RoB across selection, comparability, and outcomes domains.
Selection
Three of the studies scored high RoB on the item relating to representativeness of the ADHD sample (L. M. Friedman et al., Citation2018; Kim et al., Citation2020; Miranda-Casas et al., Citation2012). This was mainly due to studies failing to report the socio-economic background of participants (Kim et al., Citation2020; Miranda-Casas et al., Citation2012) and the country in which the study was conducted (L. M. Friedman et al., Citation2018; Miranda-Casas et al., Citation2012). Three of the studies excluded children with a co-occurring Autism Spectrum Disorder diagnosis (Alloway, Citation2011; L. M. Friedman et al., Citation2018; Miranda-Casas et al., Citation2012), whilst another study specified excluding children showing a pervasive developmental disorder (Kim et al., Citation2020). Studies also screened the ADHD group for at least one other frequently co-occurring developmental disorders including DCD (Alloway, Citation2011) and ODD (Kim et al., Citation2020; L. M. Friedman et al., Citation2018). In relation to the definition of ADHD item, only one of the studies (Alloway, Citation2011) scored high RoB as it failed to report whether the ADHD diagnosis was corroborated by a teacher.Footnote3 It is also important to note that none of the studies reported inclusion of children with a reading disorder, and only one of the studies (L. M. Friedman et al., Citation2018) included children with a mathematics learning difficulty.
Comparability
A maximum of two points could be awarded to this item. For the first point, age and medication treatment were selected as the most important factors that, where relevant, should have been accounted for either in the design or addressed in the analysis. To obtain a second point, studies could control for any additional confounding factor (e.g., gender, IQFootnote4). All studies accounted for differences in age in either the design or analysis. However, in two studies (L. M. Friedman et al., Citation2018; Miranda-Casas et al., Citation2012) some children in the ADHD groups were subject to a 24–48 hr medication, which was not controlled for in the analysis. Nonetheless, these studies accounted for at least one other important factor in either the design or the analysis including IQ (L. M. Friedman et al., Citation2018; Miranda-Casas et al., Citation2012), gender (L. M. Friedman et al., Citation2018), and SES (L. M. Friedman et al., Citation2018). The study scoring low RoB on this comparability domain accounted for IQ and gender (Kim et al., Citation2020).
Outcome
Three studies scored a high RoB on the assessment of outcome item (Alloway, Citation2011; Kim et al., Citation2020; L. M. Friedman et al., Citation2018). Although all studies used objective and validated measures of both cognitive and mathematics performance, they failed to specify whether tasks were administered by a qualified clinician (i.e., clinical psychologist, psychiatrist) or a trained psychologist/researcher. In relation to the appropriateness of statistical test, two of the studies scored a high RoB due to failure to provide sufficient information in relation to all appropriate values (Miranda-Casas et al., Citation2012)Footnote5 and for not carrying out correction for multiple testing in their correlational analysis (Alloway, Citation2011). Additionally, three of the studies (Alloway, Citation2011; L. M. Friedman et al., Citation2018; Miranda-Casas et al., Citation2012) failed to report on how many children were initially recruited to the study and the proportion for whom data were available, thereby failing to acknowledge issues around missing or incomplete data.
Narrative synthesis
All studies reported a positive association between children’s cognitive and mathematics performance, albeit with different magnitudes of effect sizes and significance levels.Footnote6 Studies indexed children’s mathematics performance in a variety of ways. One of the studies presented mathematics achievement scores as composites combining various subtests together (Alloway, Citation2011), while others opted for providing individual composite scores for subtests (Kim et al., Citation2020; L. M. Friedman et al., Citation2018). Another study (Miranda-Casas et al., Citation2012) did not use a standardized achievement test and instead used tasks that reflected more specific aspects of mathematics skills. Cognitive domains assessed included verbal short-term memory, verbal working memory, visuospatial short-term memory, visuospatial working memory, inhibitory control, working memory central executive, and processing speed. Studies mainly included children with the ADHD-C subtype, except for one study (Kim et al., Citation2020) which, in addition to this, included children with the ADHD-I and ADHD-H subtypes.
Verbal short term memory
Three studies assessed the association between verbal short-term memory and mathematics in children with ADHD-C. Alloway (Citation2011) found a statistically significant, medium-sized, correlation between a standardized composite score of verbal short-term memory on the AWMA and children’s composite WOND scores mapping on to both numerical operations and applied problem solving (r = .45, 95% CI 0.20 to 0.65, p < .01). However, this association was no longer significant once age and IQ were considered (r = .20, 95% CI −0.08 to 0.45, p > .05). L. M. Friedman et al. (Citation2018) did not control for age and IQ but nonetheless found no significant association between a verbal short-term memory factor and KTEA-I/II applied problem-solving performance (r = .29, 95% CI −0.05 to 0.56, p = .093) nor numerical operations (r = .27, 95% CI −0.06 to 0.55, p = .112). Using a stepwise multiple linear regression, with IQ introduced in the first block, Miranda-Casas and colleagues (2012) did not find verbal short-term memory performance to be a statistically significant predictor of any of the mathematics tasks that mapped onto numerical concepts, operations, nor applied problem solving.
Verbal working memory
Two studies addressed the relationship between mathematics and verbal working memory (Alloway, Citation2011; Miranda-Casas et al., Citation2012). Alloway (Citation2011) found a statistically significant, large correlation between verbal working memory composite on the AWMA and WOND composite score (r = .55, 95% CI 0.32 to 0.72, p < .01). However, this association was no longer significant once age and IQ were partialled out (r = .22, 95% CI −0.06 to 0.47, p > .05). Introducing IQ in the first block of the regression analysis, Miranda-Casas and colleagues (2012) found that verbal working memory performance was a statistically significant predictor of children’s calculation procedures (Beta = .50 p = .014, calculated r = .55, 95% CI 0.18 to 0.788) and general calculation scale (Beta = .50 p = .014, calculated r = .55, 95% CI 0.11 to 0.75). The relationship between verbal working memory and all remaining mathematics task performance was not significant.
Visuospatial short term memory
Two studies reported on the relationship between visuospatial short-term memory and mathematics (Alloway, Citation2011; L. M. Friedman et al., Citation2018). Alloway (Citation2011) found a statistically significant large association between the visuospatial working memory composite on the AWMA and WOND composite score (r = .51, 95% CI 0.27 to 0.69, p < .01). This association remained significant even after age and IQ were controlled for (r = .28, 95% CI 0.002 to 0.52, p < .05). L. M. Friedman et al. (Citation2018) justified not accounting for IQ due to substantial overlap with working memory. Nonetheless, they did not find a strong association between a visuospatial short-term memory factor and KTEA-I/II applied problem-solving performance (r = .15, 95% CI −0.19 to 0.46, p = .380), nor numerical calculations (r = .22, 95% CI −0.12 to 0.51, p = .196).
Visuospatial working memory
Two studies reported on the relationship between mathematics and visuospatial working memory (Alloway, Citation2011; Miranda-Casas et al., Citation2012). Alloway (Citation2011) found a statistically significant, large association between the visuospatial working memory composite on the AWMA and the WOND composite mathematics scores (r = .59, 95% CI 0.37 to 0.75, p < .01). This association was no longer significant once age and IQ were accounted for (r = .25, 95% CI −0.03 to 0.49, p > .05). Introducing IQ in the first block of the regression analysis, Miranda-Casas and colleagues (Citation2012) did not find that visuospatial working memory performance significantly predicted children’s performance on a range of mathematics tasks, with the exception of numerical comprehension and production, which was one of four tasks that mapped onto numerical concepts (Beta = .45, p = .028, calculated r = .50, 95% CI 0.12 to 0.75).
Central executive
One study (L. M. Friedman et al., Citation2018) partialled out common variance between children’s performance on a verbal working memory and visuospatial working memory tasks to index a central executive performance factor. Results showed a moderate-sized correlation between the central executive and KTEA-I/II applied problem-solving performance (r = .41, 95% CI 0.09 to 0.65, p = .014) as well as children’s calculation achievement scores (r = .45, 95% CI 0.14 to 0.68, p = .006). Given the inherent role of numerical calculation skills in tasks that assess applied problem-solving abilities, it is difficult to derive conclusions on whether the central executive’s role extends to children’s numerical concepts.
Inhibitory control
Two studies assessed the association between inhibitory control and mathematics (Kim et al., Citation2020; Miranda-Casas et al., Citation2012). Controlling for gender and IQ, Kim et al. (Citation2020) found a significant association between WISC Arithmetic (applied problem solving) and commission errors on the auditory ATA task (r = −.25, 95% CI −0.37 to −0.12, p < 0.001), but not the visual variant of attention task (r = .02, 95% CI −0.15 to 0.11 p > .05). Miranda-Casas and colleagues (2012) only used a visual variant of the CPT task and found that commission errors significantly predicted children’s ability to read units and tens (Beta = −.46, p = .024, calculated r = −.51, 95% CI −0.76 to −0.13) – one of four tasks that mapped onto numerical concepts domain. Other mathematics outcome measures, including numerical calculation, concepts, and broader applied problem-solving skills, were not significantly predicted by the visual inhibitory control index.
Processing speed
Controlling for gender and IQ, Kim et al. (Citation2020)reported a weak, non-significant, correlation between WISC Arithmetic and response times on the auditory (r = .08, p > .05, 95% CI −0.05 to 0.21) and visual (r = .03, 95% CI −0.10 to 0.16, p > .05) variants of the ATA task.
Discussion
Summary of evidence
This review aimed to summarize findings on the associations between cognitive processes and mathematics performance in children diagnosed with ADHD. Broadly, cognition was positively related to children’s mathematics performance whereby better cognitive performance correlated with higher mathematics scores. Evidently, very few studies considered the relationship between cognition and mathematics in children with ADHD and, as such, implications of the present review should be interpreted with caution. A previous systematic review demonstrated a positive association between ADHD and mathematics ability across various age groups (Tosto et al., Citation2015). The current review extends this idea by highlighting cognitive mechanisms, frequently found to be impaired in children with ADHD, as potentially important targets for exploration in children’s mathematics performance. The present review also complements a shift in the conceptualization of learning difficulties in children by exploring these within the context of cognitive processes, rather than diagnostic categories (Astle et al., Citation2019).
Generally, verbal short-term memory did not show significant associations with mathematics performance, and where it did, this relationship was no longer significant once IQ and age were considered. A previous study in a typically developing population suggests that verbal short-term memory is particularly important for older children’s solution of easier mental arithmetic sums, possibly due to proficiency of symbolic-linguistic processes or employment of more advanced strategies employing retrieval of verbal codes (Holmes & Adams, Citation2006). Based on the current review, the potential role of verbal short-term memory cannot be ruled out.
Findings in relation to visuospatial short-term memory were mixed. In one of the studies, visuospatial short-term memory maintained its large associations with achievement composite scores even after IQ and age were considered, whilst another study did not find evidence for the importance of this memory domain even in the absence of accountability for IQ scores in the statistical model. One possibility for these discrepant findings could be differences in approach used to measure visuospatial short-term memory performance. Whilst Alloway (Citation2011) used three different tasks to index composite visuospatial short-term memory performance, L. M. Friedman et al. (Citation2018) utilized a regression-based strategy to segregate this domain from working memory tasks.
Both verbal working memory and visuospatial working memory performance showed meaningful associations with children’s composite achievement scores. However, this association weakened once age and IQ were considered. One of the studies also addressed the role of the central executive component of working memory in children’s mathematics aptitude. Regressing common variance between components of working memory highlighted the central executive as the key component most strongly correlated with children’s mathematics attainment. This echoes previous findings in typically developing populations (Cragg et al., Citation2017) and may reflect associations between updating requirements of the central executive with that of intelligence tests (L. M. Friedman et al., Citation2018). In such a case, the findings across the studies uphold the importance of working memory, and in particular updating, to mathematics attainment (Cragg et al., 2014).
Importantly, when more specific calculation procedures were considered, verbal working memory showed a substantial association even after accounting for IQ, whilst visuospatial working memory emerged as important for children’s numerical comprehension. Collectively, these findings imply that whilst verbal working memory is related to numerical calculation skills, visuospatial working memory could be especially related with children’s conceptual understanding. Furthermore, this highlights challenges of indexing mathematics performance using composite achievement scores, which can obscure the relationship between cognitive processes and more specific mathematics skills, which contribute to broader underachievement (Cragg et al., 2014). Future research exploring mathematics in ADHD would therefore benefit from differentiating between conceptual and procedural performance when exploring cognitive signatures of mathematics performance.
The strength of association between inhibitory control and mathematics varied depending on the format of stimuli presentation. Inhibition of auditory information was associated with applied problem-solving skills, whilst inhibition of visually presented stimuli was related to a very specific conceptual skill of reading units and tens. These findings suggest that inhibition of irrelevant visual stimuli is related to a very specific aspect of children’s numerical concept comprehension (i.e., the ability to read units and tens). Contrary to this, suppression of irrelevant auditory stimuli is related to a broader range of numerical skills, which standardized applied problem-solving subtests tap in to. This further highlights the importance of disentangling broad achievement scores by exploring performance on more specific mathematics abilities. Doing so can help identify more informative pathways of impairment that would otherwise be concealed by standardized composites. Notably, the studies assessing inhibitory control diverge in the subtypes of ADHD that children were diagnosed with. Kim et al. (Citation2020) included children with all three ADHD subtypes, Miranda-Casas and colleagues (Citation2012) focused only on children with ADHD-C, a discrepancy which may have further contributed to the differences in findings.
Lastly, processing speed, addressed by one of the studies, showed a weak correlation with applied problem-solving performance. However, no conclusions can be made in relation to more specific numerical skills that such assessments tap into. It is important to note that other processes previously implicated in children’s mathematics performance, such as cognitive flexibility, planning, and delayed aspects of memory were not assessed (Bull & Lee, Citation2014; Cai et al., Citation2016; Cragg et al., Citation2017; Geary, Citation2004; LeFevre et al., Citation2013; Szucs et al., Citation2013). These domains have previously been identified as impaired in many children with ADHD, and thus their role in mathematics performance warrants an important target for further exploration.
All studies either excluded children with a co-occurring Autism Spectrum Disorder diagnosis and/or failed to screen for frequently co-occurring disorder symptoms. Although isolating ADHD from other diagnoses is useful for identifying difficulties specific to this population, ADHD seldom occurs in isolation. Rather, children with ADHD frequently meet criteria for at least one additional disorder. For example, while between 11% and 22% of children in the studies met diagnosis for ODD in two of the studies (Kim et al., Citation2020; L. M. Friedman et al., Citation2018), the other two studies failed to report on co-occurrences (Alloway, Citation2011; Miranda et al., Citation2012). This is particularly problematic for development and administration of interventions to a diverse group of children where underlying cognitive difficulties are incompatible with the targeted processes, thwarting potential for long-lasting improvements (Kadosh et al., Citation2013; Rapport et al., Citation2013). Addressing issues surrounding cognitive heterogeneity and co-occurrences will be crucial for navigating decisions around educational interventions. More recent research urges a shift toward a dimensional characterization of disorders, which are generally considered to be distinct (Gathercole et al., Citation2018; Sonuga-Barke & Coghill, Citation2014). Arguably, such an approach would be more compatible in reflecting the complex realities of cognitive and educational difficulties experienced by children with ADHD.
It is important to note that while some studies controlled for IQ in their statistical models (Alloway, Citation2011; Miranda Casas et al., 2012; Kim et al., Citation2020) others did not (L. M. Friedman et al., Citation2018). IQ scores are linked to both mathematics and cognitive performance in children with ADHD, with some studies rendering IQ as the best single predictor of academic achievement (Mahone et al., Citation2002; Mayes & Calhoun, Citation2007). As a result, researchers may be inclined to use IQ scores as a covariate when assessing cognitive and/or educational outcomes in ADHD. However, others argue against using IQ as a covariate in assessments of cognitive functioning ADHD (De Zeeuw et al., Citation2012; Dennis et al., Citation2009; O’Brien et al., Citation2010). Assessments of IQ frequently examine multiple intercorrelated cognitive abilities, and so controlling for IQ scores when assessing mathematics outcomes removes important variance that can be attributed to underlying cognitive processes affected in ADHD (Frazier et al., Citation2004). A previous meta-analysis found that medicated children with ADHD showed an average increase of 6–7 IQ points when compared to drug naive children (Jepsen et al., Citation2009). This implies that lower IQ scores could reflect difficulties in EF processes related to focusing/maintaining attention or difficulties in test taking behavior, rather than diminished intellectual functioning. In other words, IQ tests seldom represent independent aptitude abilities from other aspects of cognition that are impaired in ADHD – an important statistical pre-requisite in the use of covariates (Dennis et al., Citation2009). Future work should therefore carefully consider whether or not it is appropriate to control for IQ scores in their study design (see Dennis et al., Citation2009 for a comprehensive overview of this issue).
Limitations
Due to the wide range of cognitive processes assessed, and the different approaches used to measure and report mathematics performance scores, a quantitative synthesis was not possible. Additionally, the small number of studies that were identified for inclusion and their small sample sizes limits the conclusions that can be drawn with regard to the relationship between specific cognitive processes and mathematics performance in ADHD. The relatively small sample sizes reflect the realities of other clinical ADHD studies (e.g., Kaufmann & Nuerk, Citation2008; Passolunghi et al., Citation2005). Although larger sample sizes are reported elsewhere (e.g., Antonini et al., Citation2016; Gremillion & Martel, Citation2012; Roberts et al., Citation2017) these typically include community/school recruited samples and not a clinical ADHD sample. Clinical samples are notoriously difficult to recruit but nonetheless allow for rich disorder-specific data to be collected. Nonetheless, the small number of studies coupled with their relatively recent dates of publication likely reflects the inception of research in this area and echoes a similar novelty found in typically developing populations (Allen et al., Citation2019).
Another potential limitation relates to strict inclusion criteria of children with a clinically confirmed ADHD diagnosis according to stringent diagnostic criteria. Teacher corroboration of difficulties was one of the predetermined key inclusion criteria for this review. A diagnosis of ADHD requires that functional impairments are present in two contexts, typically at home and at school (APA, Citation2013). Thus, the gold-standard to diagnosing ADHD occurs via parent reports of the child’s behavior at home combined by teacher reports of the child’s behavior at school. Notably, community-oriented approaches using parent or teacher questionnaires are linked to high false positives of ADHD and may therefore not be representative the clinical realities of ADHD (Coghill & Seth, Citation2015; Sayal et al., Citation2018). Nonetheless, research shows that even children with high ADHD symptoms in the absence of a clinical diagnosis struggle with mathematics, implying that even subthreshold symptoms can put children at higher risk for mathematics difficulties (Czamara et al., Citation2013). Plausibly, exclusion of studies with children scoring high on ADHD symptoms may have resulted in loss of informative data on the association between cognitive and mathematics performance. Despite this, the present review was able to assemble findings of high-quality studies in which participants were truly representative of the diagnosed population in question. Another limitation relates to the limited representation of different ADHD subtypes. Studies in the present review predominantly included children with the ADHD-C subtype, except for one study (Kim et al., Citation2020) that, in addition to this, included children with the ADHD-I and ADHD-H subtypes. Thus, the findings of the present review are limited in their generalizability to all ADHD subtypes. Lastly, the present review only included peer reviewed studies that were published in English. As such, it is possible that important findings in other languages, or studies which had not been published, may have been missed.
Lastly, the current review used a 20% subsample for title/abstract and full-text screening by an independent researcher, consistent with other reviews (e.g., Stewart et al., Citation2017). A dual blind review of a 20% subsample for title/abstract screening is in line with previous recommendations for conducting systematic reviews (Nevis et al., Citation20155). To mitigate the possibility that important studies would be missed, the reference list of included papers was also screened for inclusion. Furthermore, due to resource constraints, it was only possible to apply 20% dual screening at full-text review and a reason for exclusion at full-test screening was provided for each excluded study to decrease the possibility that a study would be missed.
Conclusions and future directions
This review explored available research on the association between cognition and mathematics in children with ADHD. This review highlighted the importance of assessing the relationship between cognitive domains and mathematics in ADHD. However, the few studies available coupled by small sample sizes and substantial methodological heterogeneity make it difficult to draw solid conclusions. Overall, however, studies reviewed showed that better cognitive performance was associated with higher mathematics performance. This review highlights a strong need for further research on the identification of specific cognitive correlates of mathematics skill in children with ADHD. In particular, such research would benefit from dissecting specific numerical skills, rather than broad attainment scores, which risk masking the specific areas children with ADHD struggle with. Future research should also carefully consider whether or not it is appropriate to control for IQ when examining cognitive functioning and its relationship to mathematics in ADHD, as issues around shared variance may understate their association.
CNY-RA_21-72-File005.docx
Download MS Word (20.3 KB)CNY-RA_21-72-File004.xlsx
Download MS Excel (53.5 KB)CNY-RA_21-72-File003.docx
Download MS Word (26.2 KB)CNY-RA_21-72-File002.docx
Download MS Word (24.1 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed at https://doi.org/10.1080/09297049.2021.1985444
Additional information
Funding
Notes
1 One of the studies (Dahlin, Citation2013) was excluded as it did not report on children’s medication status (a key inclusion criteria) and attempts to clarify medication status with author via e-mail correspondence were unsuccessful.
2 Data includes information that was confirmed via e-mail correspondence with the author.
3 Diagnosis was conducted according to DSM-IV criteria by a pediatric psychiatrist/community pediatrician and all children were on ADHD medication. For purposes of inclusion, teacher corroboration was assumed due to its fundamental role in receiving a clinical diagnosis.
4 Based on previous arguments against using IQ as a covariate in assessments of neurocognitive function (Dennis et al., Citation2009), IQ was included here as an additional, rather than critical, confounding factor.
5 Means and SD’s included were provided by Miranda-Casas et al., Citation2012 via e-mail correspondence.
6 For table summarizing correlations between cognition and math please refer to Supplement File 4.
References
- Allen, K., Higgins, S., & Adams, J. (2019). The relationship between visuospatial working memory and mathematical performance in school-aged children: A systematic review. Educational Psychology Review, 31(3), 509–531. https://doi.org/https://doi.org/10.1007/s10648-019-09470-8
- Alloway, T. P. (2007). Automated working: Memory assessment: Manual. Pearson.
- Alloway, T. P. (2011). A comparison of working memory profiles in children with ADHD and DCD. Child Neuropsychology, 17(5), 483–494. https://doi.org/https://doi.org/10.1080/09297049.2011.553590
- American Psychological Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). https://doi.org/https://doi.org/10.1176/appi.books.9780890425596
- Andersson, U. (2010). Skill development in different components of arithmetic and basic cognitive functions: Findings from a 3-year longitudinal study of children with different types of learning difficulties. Journal of Educational Psychology, 102(1), 115–134. https://doi.org/https://doi.org/10.1037/a0016838
- Antonini, T. N., Kingery, K. M., Narad, M. E., Langberg, J. M., Tamm, L., & Epstein, J. N. (2016). Neurocognitive and behavioral predictors of math performance in children with and without ADHD. Journal of Attention Disorders, 20(2), 108–118. https://doi.org/https://doi.org/10.1177/1087054713504620
- Arnold, L. E., Hodgkins, P., Kahle, J., Madhoo, M., & Kewley, G. (2020). Long-term outcomes of ADHD: Academic achievement and performance. Journal of Attention Disorders, 24(1), 73–85. https://doi.org/https://doi.org/10.1177/1087054714566076
- Astle, D. E., Bathelt, J., Team, C., & Holmes, J. (2019). Remapping the cognitive and neural profiles of children who struggle at school. Developmental Science, 22(1), 1–18. https://doi.org/https://doi.org/10.1111/desc.12747
- Avila, C., & Parcet, M. A. (2001). Personality and inhibitory deficits in the stop-signal task: The mediating role of Gray’s anxiety and impulsivity. Personality and Individual Differences, 31(6), 975–986. https://doi.org/https://doi.org/10.1016/S0191-8869(00)00199-9
- Baddeley, A. D., & Hitch, G. (1974). Working memory. Psychology of Learning and Motivation, 8(1974), 47–89.
- Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121(1), 65–94. https://doi.org/https://doi.org/10.1037/0033-2909.121.1.65
- Baweja, R., Mattison, R. E., & Waxmonsky, J. G. (2015). Impact of attention-deficit hyperactivity disorder on school performance: What are the effects of medication? Pediatric Drugs, 17(6), 459–477. https://doi.org/https://doi.org/10.1007/s40272-015-0144-2
- Bellon, E., Fias, W., & De Smedt, B. (2016). Are individual differences in arithmetic fact retrieval in children related to inhibition? Frontiers in Psychology, 7, 825. https://doi.org/https://doi.org/10.3389/fpsyg.2016.00825
- Belur, J., Tompson, L., Thornton, A., & Simon, M. (2021). Interrater reliability in systematic review methodology: Exploring variation in coder decision-making. Sociological Methods & Research, 50(2), 837–865. https://doi.org/https://doi.org/10.1177/0049124118799372
- Best, J. R., Miller, P. H., & Jones, L. L. (2009). Executive functions after age 5: Changes and correlates. Developmental Review, 29(3), 180–200. https://doi.org/https://doi.org/10.1016/j.dr.2009.05.002
- Biederman, J., Faraone, S. V., Weber, W., Russell, R. L., Rater, M., & Park, K. S. (1997). Correspondence between DSM-III-R and DSM-IV attention-deficit/hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 36(12), 1682–1687. https://doi.org/https://doi.org/10.1097/00004583-199712000-00016
- Biederman, J., Monuteaux, M. C., Doyle, A. E., Seidman, L. J., Wilens, T. E., Ferrero, F., Morgan, C. L., & Faraone, S. V. (2004). Impact of executive function deficits and attention-deficit/hyperactivity disorder (ADHD) on academic outcomes in children. Journal of Consulting and Clinical Psychology, 72(5), 757–766. https://doi.org/https://doi.org/10.1037/0022-006X.72.5.757
- Biederman, J., Petty, C. R., Evans, M., Small, J., & Faraone, S. V. (2010). How persistent is ADHD? A controlled 10-year follow-up study of boys with ADHD. Psychiatry Research, 177(3), 299–304. https://doi.org/https://doi.org/10.1016/j.psychres.2009.12.010
- Borenstein, M., Hedges, L. V., Higgins, J. P., & Rothstein, H. R. (2011). Introduction to meta analysis. John Wiley & Sons.
- Breslau, J., Miller, E., Breslau, N., Bohnert, K., Lucia, V., & Schweitzer, J. (2009). The impact of early behavior disturbances on academic achievement in high school. Pediatrics, 123(6), 1472–1476. https://doi.org/https://doi.org/10.1542/peds.2008-1406
- Bull, R., Espy, K. A., & Wiebe, S. A. (2008). Short-term memory, working memory, and executive functioning in preschoolers: Longitudinal predictors of mathematical achievement at age 7 years. Developmental Neuropsychology, 33(3), 205–228. https://doi.org/https://doi.org/10.1080/87565640801982312
- Bull, R., & Johnston, R. S. (1997). Children’s arithmetical difficulties: Contributions from processing speed, item identification, and short-term memory. Journal of Experimental Child Psychology, 65(1), 1–24. https://doi.org/https://doi.org/10.1006/jecp.1996.2358
- Bull, R., & Lee, K. (2014). Executive functioning and maths achievement. Child Development Perspectives, 8(1), 36–41. https://doi.org/https://doi.org/10.1111/cdep.12059
- Bull, R., & Scerif, G. (2001). Executive functioning as a predictor of children’s maths ability: Inhibition, switching, and working memory. Developmental Neuropsychology, 19(3), 273–293. https://doi.org/https://doi.org/10.1207/S15326942DN1903_3
- Butterworth, B. (2005). The development of arithmetical abilities. Journal of Child Psychology and Psychiatry, 46(1), 3–18. https://doi.org/https://doi.org/10.1111/j.1469-7610.2004.00374.x
- Cai, D., Georgiou, G. K., Wen, M., & Das, J. (2016). The role of planning in different mathematical skills. Journal of Cognitive Psychology, 28(2), 234–241. https://doi.org/https://doi.org/10.1080/20445911.2015.1103742
- Calhoun, S. L., & Mayes, S. D. (2005). Processing speed in children with clinical disorders. Psychology in the Schools, 42(4), 333–343. https://doi.org/https://doi.org/10.1002/pits.20067
- Calub, C., Rapport, M., Friedman, L., & Eckrich, S. (2019). IQ and academic achievement in children with ADHD: The differential effects of specific cognitive functions. Journal of Psychopathology and Behavioral Assessment, 41(4), 639–651. https://doi.org/https://doi.org/10.1007/s10862-019-09728-z
- Capano, L., Minden, D., Chen, S. X., Schachar, R. J., & Ickowicz, A. (2008). Mathematical learning disorder in school-age children with attention-deficit hyperactivity disorder. The Canadian Journal of Psychiatry, 53(6), 392–399. https://doi.org/https://doi.org/10.1177/070674370805300609
- Capodieci, A., & Martinussen, R. (2017). Math error types and correlates in adolescents with and without attention deficit hyperactivity disorder. Frontiers in Psychology, 8, 1801. https://doi.org/https://doi.org/10.3389/fpsyg.2017.01801
- Cassidy, A. R., White, M. T., DeMaso, D. R., Newburger, J. W., & Bellinger, D. C. (2016). Processing speed, executive function, and academic achievement in children with dextro-transposition of the great arteries: Testing a longitudinal developmental cascade model. Neuropsychology, 30(7), 874. https://doi.org/https://doi.org/10.1037/neu0000289
- Cirino, P. T., Fuchs, L. S., Elias, J. T., Powell, S. R., & Schumacher, R. F. (2015). Cognitive and mathematical profiles for different forms of learning difficulties. Journal of Learning Disabilities, 48(2), 156–175. https://doi.org/https://doi.org/10.1177/0022219413494239
- Clark, C. A., Pritchard, V. E., & Woodward, L. J. (2010). Preschool executive functioning abilities predict early maths achievement. Developmental Psychology, 46(5), 1176. https://doi.org/https://doi.org/10.1037/a0019672
- Coghill, D., & Seth, S. (2015). Effective management of attention-deficit/hyperactivity disorder (ADHD) through structured re-assessment: the Dundee ADHD Clinical Care Pathway. Child and Adolescent Psychiatry and Mental Health, 9(1), 1–14. https://doi.org/https://doi.org/10.1186/s13034-015-0083-2
- Coghill, D. R., Banaschewski, T., Bliss, C., Robertson, B., & Zuddas, A. (2018). Cognitive function of children and adolescents with attention-deficit/hyperactivity disorder in a 2-year open-label study of lisdexamfetamine dimesylate. CNS Drugs, 32(1), 85–95. https://doi.org/https://doi.org/10.1007/s40263-017-0487-z.
- Coghill, D. R., Seth, S., & Matthews, K. (2014). A comprehensive assessment of memory, delay aversion, timing, inhibition, decision making and variability in attention deficit hyperactivity disorder: Advancing beyond the three-pathway models. Psychological Medicine, 44(9), 1989–2001. https://doi.org/https://doi.org/10.1017/S0033291713002547
- Cohen, J. (1988). Statistical power analysis Jbr the behavioral. Sciences, 18–74. Hillsdale (NJ): Lawrence Erlbaum Associates. https://doi.org/https://doi.org/10.4324/9780203771587
- Cortese, S., Moreira-Maia, C. R., St. Fleur, D., Morcillo-Peñalver, C., Rohde, L. A., & Faraone, S. V. (2016). Association between ADHD and obesity: A systematic review and meta-analysis. American Journal of Psychiatry, 173(1), 34–43. https://doi.org/https://doi.org/10.1176/appi.ajp.2015.15020266
- Cragg, L., Keeble, S., Richardson, S., Roome, H. E., & Gilmore, C. (2017). Direct and indirect influences of executive functions on maths achievement. Cognition, 162(C), 12–26. https://doi.org/https://doi.org/10.1016/j.cognition.2017.01.014
- Czamara, D., Tiesler, C. M., Kohlbock, G., Berdel, D., Hoffmann, B., Bauer, C. P., Heinrich, J., Lehmann, I., Herbarth, O., von Berg, A., Müller-Myhsok, B., Schulte-Körne, G., Heinrich, J., & Koletzko, S. (2013). Children with ADHD symptoms have a higher risk for reading, spelling and math difficulties in the GINIplus and LISAplus cohort studies. PLoS ONE, 8(5), e63859. https://doi.org/https://doi.org/10.1371/journal.pone.0063859
- Dahlin, K. I. (2013). Working memory training and the effect on mathematical achievement in children with attention deficits and special needs. Journal of Education and Learning, 2(1), 118–133. https://doi.org/https://doi.org/10.5539/jel.v2n1p118
- Daley, D., & Birchwood, J. (2010). ADHD and academic performance: Why does ADHD impact on academic performance and what can be done to support ADHD children in the classroom? Child: Care, Health and Development, 36(4), 455–464.
- Davidson, J. E., Deuser, R., & Sternberg, R. J. (1994). The role of metacognition in problem solving. Metacognition: Knowing About Knowing, 207–226.
- De Clercq, A., Desoete, A., & Roeyers, H. (2000). EPA2000: A multilingual, programmable computer assessment of off-line metacognition in children with mathematical-learning disabilities. Behavior Research Methods, Instruments and Computers, 32(2), 304–311. https://doi.org/https://doi.org/10.3758/BF03207799
- De Visscher, A., & Noël, M.-P. (2014). Arithmetic facts storage deficit: The hypersensitivity-to-interference in memory hypothesis. Developmental Science, 17(3), 434–442. https://doi.org/https://doi.org/10.1111/desc.12135
- De Zeeuw, P., Schnack, H. G., Van Belle, J., Weusten, J., Van Dijk, S., Langen, M., … & Durston, S. (2012). Differential brain development with low and high IQ in attention-deficit/hyperactivity disorder. PloS one, 7(4), e35770. https://doi.org/https://doi.org/10.1371/journal.pone.0035770
- Dehaene, S., & Cohen, L. (1995). Towards an anatomical and functional model of number processing. Mathematical Cognition, 1(1), 83–120.
- Dennis, M., Francis, D. J., Cirino, P. T., Schachar, R., Barnes, M. A., & Fletcher, J. M. (2009). Why IQ is not a covariate in cognitive studies of neurodevelopmental disorders. Journal of the International Neuropsychological Society, 15(3), 331. https://doi.org/https://doi.org/10.1017/S1355617709090481
- Diamond, A. (2013). Executive functions. Annual Review of Psychology, 64(1), 135–168. https://doi.org/https://doi.org/10.1146/annurev-psych-113011-143750
- Donzelli, G., Llopis-Gonzalez, A., Llopis-Morales, A., Cioni, L., & Morales-Suárez-Varela, M. (2020). Particulate matter exposure and attention-deficit/hyperactivity disorder in children: A systematic review of epidemiological studies. International Journal of Environmental Research and Public Health, 17(1), 67. https://doi.org/https://doi.org/10.3390/ijerph17010067
- Döpfner, M., Hautmann, C., Görtz-Dorten, A., Klasen, F., & Ravens-Sieberer, U. (2015). Long-term course of ADHD symptoms from childhood to early adulthood in a community sample. European Child & Adolescent Psychiatry, 24(6), 665–673. https://doi.org/https://doi.org/10.1007/s00787-014-0634-8
- Dowker, A. (2005). Early identification and intervention for students with maths difficulties. Journal of Learning Disabilities, 38(4), 324–332. https://doi.org/https://doi.org/10.1177/00222194050380040801
- Dubois, B., Levy, R., Verin, M., Teixeira, C., Agid, Y., & Pillon, B. (1995). Experimental approach to prefrontal functions in humans. Annals of the New York Academy of Sciences, 769(1), 41–60. https://doi.org/https://doi.org/10.1111/j.1749-6632.1995.tb38130.x
- Duckworth, A. L., Quinn, P. D., & Tsukayama, E. (2012). What no child left behind leaves behind: The roles of IQ and self-control in predicting standardized achievement test scores and report card grades. Journal of Educational Psychology, 104(2), 439. https://doi.org/https://doi.org/10.1037/a0026280
- Duncan, G. J., Dowsett, C. J., Claessens, A., Magnuson, K., Huston, A. C., Klebanov, P., Pagani, L. S., Feinstein, L., Engel, M., Brooks-Gunn, J., Sexton, H., Duckworth, K., & Japel, C. (2007). School Readiness and Later Achievement. Developmental Psychology, 43(6), 1428–1446. https://doi.org/https://doi.org/10.1037/0012-1649.43.6.1428
- DuPaul, G. J., Morgan, P. L., Farkas, G., Hillemeier, M. M., & Maczuga, S. (2016). Academic and social functioning associated with attention-deficit/hyperactivity disorder: Latent class analyses of trajectories from kindergarten to fifth grade. Journal of Abnormal Child Psychology, 44(7), 1425–1438. https://doi.org/https://doi.org/10.1007/s10802-016-0126-z
- DuPaul, G. J., Volpe, R. J., Jitendra, A. K., Lutz, J. G., Lorah, K. S., & Gruber, R. (2004). Elementary school students with AD/HD: Predictors of academic achievement. Journal of School Psychology, 42(4), 285–301. https://doi.org/https://doi.org/10.1016/j.jsp.2004.05.001
- Efron, D., Sciberras, E., Anderson, V., Hazell, P., Ukoumunne, O. C., Jongeling, B., Schilpzand, E. J., Bisset, M., & Nicholson, J. M. (2014). Functional status in children with ADHD at age 6–8: A controlled community study. Pediatrics, 134(4), e992–e1000. https://doi.org/https://doi.org/10.1542/peds.2014-1027
- Ekstein, S., Glick, B., Weill, M., Kay, B., & Berger, I. (2011). Down syndrome and attention-deficit/hyperactivity disorder (ADHD). Journal of Child Neurology, 26(10), 1290–1295. https://doi.org/https://doi.org/10.1177/0883073811405201
- Elia, J., Ambrosini, P., & Berrettini, W. (2008). ADHD characteristics: I. Concurrent co-morbidity patterns in children & adolescents. Child and Adolescent Psychiatry and Mental Health, 2(1), 15. https://doi.org/https://doi.org/10.1186/1753-2000-2-15
- Faraone, S. V., Biederman, J., & Mick, E. (2006). The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychological Medicine, 36(2), 159–165. https://doi.org/https://doi.org/10.1017/S003329170500471X
- Field, A. P. (2001). Meta-analysis of correlation coefficients: A Monte Carlo comparison of fixed-and random-effects methods. Psychological Methods, 6(2), 161. https://doi.org/https://doi.org/10.1037/1082-989X.6.2.161
- Formoso, J., Injoque-Ricle, I., Barreyro, J.-P., Calero, A., Jacubovich, S., & Burín, D. I. (2018). Mathematical cognition, working memory, and processing speed in children. Cognition, Brain, Behavior. An Interdisciplinary Journal, 22(2), 59–84. https://doi.org/https://doi.org/10.24193/cbb.2018.22.05
- Frazier, T. W., Demaree, H. A., & Youngstrom, E. A. (2004). Meta-analysis of intellectual and neuropsychological test performance in attention-deficit/hyperactivity disorder. Neuropsychology, 18(3), 543. https://doi.org/https://doi.org/10.1037/0894-4105.18.3.543
- Friedman, L. M., Rapport, M. D., Orban, S. A., Eckrich, S. J., & Calub, C. A. (2018). Applied problem solving in children with ADHD: The mediating roles of working memory and mathematical calculation. Journal of Abnormal Child Psychology, 46(3), 491–504. https://doi.org/https://doi.org/10.1007/s10802-017-0312-7
- Fuchs, L. S., Fuchs, D., Compton, D. L., Powell, S. R., Seethaler, P. M., Capizzi, A. M., Schatschneider, C., & Fletcher, J. M. (2006). The cognitive correlates of third-grade skill in arithmetic, algorithmic computation, and arithmetic word problems. Journal of Educational Psychology, 98(1), 29. https://doi.org/https://doi.org/10.1037/0022-0663.98.1.29
- Fuchs, L. S., Fuchs, D., Stuebing, K., Fletcher, J. M., Hamlett, C. L., & Lambert, W. (2008). Problem solving and computational skill: Are they shared or distinct aspects of mathematical cognition? Journal of Educational Psychology, 100(1), 30. https://doi.org/https://doi.org/10.1037/0022-0663.100.1.30
- Fuchs, L. S., Geary, D. C., Compton, D. L., Fuchs, D., Hamlett, C. L., Seethaler, P. M., Bryant, J. D., & Schatschneider, C. (2010). Do different types of school maths development depend on different constellations of numerical versus general cognitive abilities? Developmental Psychology, 46(6), 1731–1746. https://doi.org/https://doi.org/10.1037/a0020662
- Gallistel, C. R., & Gelman, R. (1990). The what and how of counting. Cognition, 34(2), 197–200. https://doi.org/https://doi.org/10.1016/0010-0277(90)90043–j
- Gallistel, C. R., & Gelman, R. (1992). Preverbal and verbal counting and computation. Cognition, 44(1–2). 43–74. https://doi.org/https://doi.org/10.1016/0010-0277(92)90050–R
- Gathercole, S. E., Alloway, T. P., Willis, C., & Adams, A.-M. (2006). Working memory in children with reading disabilities. Journal of Experimental Child Psychology, 93(3), 265–281. https://doi.org/https://doi.org/10.1016/j.jecp.2005.08.003
- Gathercole, S. E., Astle, D. A., Manly, T., Holmes, J., & Team, C. (2018). Cognition and behaviour in learning difficulties and ADHD: A dimensional approach. bioRxiv, 260265. https://doi.org/https://doi.org/10.1101/260265
- Geary, D. C. (2004). Maths and Learning Disabilities. Journal of Learning Disabilities, 37(1), 4–15. https://doi.org/https://doi.org/10.1177/00222194040370010201
- Geary, D. C., Hoard, M. K., Nugent, L., & Byrd-Craven, J. (2008). Development of number line representations in children with mathematical learning disability. Developmental Neuropsychology, 33(3), 277–299. https://doi.org/https://doi.org/10.1080/87565640801982361
- Gilmore, C., Clayton, S., Cragg, L., McKeaveney, C., Simms, V., & Johnson, S. (2018). Understanding arithmetic concepts: The role of domain-specific and domain-general skills. PloS one, 13(9), e0201724. https://doi.org/https://doi.org/10.1371/journal.pone.0201724
- Gilmore, C., Keeble, S., Richardson, S., & Cragg, L. (2015). The role of cognitive inhibition in different components of arithmetic. ZDM: The International Journal on Maths Education, 47(5), 771–782. https://doi.org/https://doi.org/10.1007/s11858-014-0659-y
- Goth-Owens, T. L., Martinez-Torteya, C., Martel, M. M., & Nigg, J. T. (2010). Processing speed weakness in children and adolescents with non-hyperactive but inattentive ADHD (ADD). Child Neuropsychology, 16(6), 577–591. https://doi.org/https://doi.org/10.1080/09297049.2010.485126
- Gremillion, M. L., & Martel, M. M. (2012). Semantic language as a mechanism explaining the association between ADHD symptoms and reading and maths underachievement. Journal of Abnormal Child Psychology, 40(8), 1339–1349. https://doi.org/https://doi.org/10.1007/s10802-012-9650-7
- Harpin, V. A. (2005). The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Archives of Disease in Childhood, 90(suppl 1), i2–i7. https://doi.org/https://doi.org/10.1136/adc.2004.059006
- Hawk, L. W., Jr, Fosco, W. D., Colder, C. R., Waxmonsky, J. G., Pelham, W. E., Jr, & Rosch, K. S. (2018). How do stimulant treatments for ADHD work? Evidence for mediation by improved cognition. Journal of Child Psychology and Psychiatry, 59(12), 1271–1281. https://doi.org/https://doi.org/10.1111/jcpp.12917
- Higgins, J., & Green, S. (2011). 10.4. 3.1 recommendations on testing for funnel plot asymmetry. Cochrane Handbook for Systematic Reviews of Interventions, 5. https://handbook-5-1.cochrane.org/chapter_10/10_4_3_1_recommendations_on_testing_for_funnel_plot_asymmetry.htm
- Higgins, J. P., Li, T., & Deeks, J. J. (2019). Choosing effect measures and computing estimates of effect. Cochrane Handbook for Systematic Reviews of Interventions, 143–176. https://training.cochrane.org/handbook/current/chapter-06
- Holmes, J., & Adams, J. W. (2006). Working memory and children’s mathematical skills: Implications for mathematical development and maths curricula. Educational Psychology, 26(3), 339–366. https://doi.org/https://doi.org/10.1080/01443410500341056
- Holmes, J., Hilton, K. A., Place, M., Alloway, T. P., Elliott, J. G., & Gathercole, S. E. (2014). Children with low working memory and children with ADHD: Same or different? Frontiers in Human Neuroscience, 8(976), 1–13. https://doi.org/https://doi.org/10.3389/fnhum.2014.00976
- Hunter, J. E., & Schmidt, F. L. (2004). Methods of meta-analysis: Correcting error and bias in research findings. Sage.
- Jacobson, L. A., Ryan, M., Martin, R. B., Ewen, J., Mostofsky, S. H., Denckla, M. B., & Mahone, E. M. (2011). Working memory influences processing speed and reading fluency in ADHD. Child Neuropsychology, 17(3), 209–224. https://doi.org/https://doi.org/10.1080/09297049.2010.532204
- Jepsen, J. R. M., Fagerlund, B., & Mortensen, E. L. (2009). Do attention deficits influence IQ assessment in children and adolescents with ADHD? Journal of Attention Disorders, 12(6), 551–562.
- Kadosh, R. C., Dowker, A., Heine, A., Kaufmann, L., & Kucian, K. (2013). Interventions for improving numerical abilities: Present and future. Trends in Neuroscience and Education, 2(2), 85–93. https://doi.org/https://doi.org/10.1016/j.tine.2013.04.001
- Kaufman, A. (1998). Kaufman test of educational achievement–Normative update. American Guidance Service.
- Kaufman, A. S., & Kaufman, N. L. (2004). Kaufman test of educational achievement-comprehensive form. American Guidance Service.
- Kaufmann, L., & Nuerk, H.-C. (2008). Basic Number Processing Deficits in ADHD: A Broad Examination of Elementary and Complex Number Processing Skills in 9- to 12- Year-Old Children with ADHD-C. Developmental Science, 11(5), 692–699. https://doi.org/https://doi.org/10.1111/j.1467-7687.2008.00718.x
- Kibby, M. Y., Vadnais, S. A., & Jagger-Rickels, A. C. (2019). Which components of processing speed are affected in ADHD subtypes? Child Neuropsychology, 25(7), 964–979. https://doi.org/https://doi.org/10.1080/09297049.2018.1556625
- Kim, Y., Koh, M. K., Park, K. J., Lee, H.-J., Yu, G. E., & Kim, H.-W. (2020). WISC-IV intellectual profiles in Korean children and adolescents with attention deficit/hyperactivity disorder. Psychiatry Investigation, 17(5), 444. https://doi.org/https://doi.org/10.30773/pi.2019.0312
- Klein, R. G., Mannuzza, S., Olazagasti, M. A. R., Roizen, E., Hutchison, J. A., Lashua, E. C., & Castellanos, F. X. (2012). Clinical and functional outcome of childhood attention-deficit/hyperactivity disorder 33 years later. Archives of General Psychiatry, 69(12), 1295–1303. https://doi.org/https://doi.org/10.1001/archgenpsychiatry.2012.271
- Kofler, M. J., Irwin, L. N., Soto, E. F., Groves, N. B., Harmon, S. L., & Sarver, D. E. (2018). Executive functioning heterogeneity in pediatric ADHD. Journal of Abnormal Child Psychology, 47(2), 273–286. https://doi.org/https://doi.org/10.1007/s10802-018-0438-2
- Koh, M., Noh, E.-A., & Kim, H.-W. (2015). Korean Wechsler intelligence scale for children-profiles in child and adolescent with attention-deficit hyperactivity disorder: Retrospective study. Journal of the Korean Academy of Child and Adolescent Psychiatry, 26(3), 183–189. https://doi.org/https://doi.org/10.5765/jkacap.2015.26.3.183
- Kortekaas-Rijlaarsdam, A. F., Luman, M., Sonuga-Barke, E., & Oosterlaan, J. (2019). Does methylphenidate improve academic performance? A systematic review and meta-analysis. European Child & Adolescent Psychiatry, 28(2), 155–164. https://doi.org/https://doi.org/10.1007/s00787-018-1106-3
- Kuriyan, A. B., Pelham, W. E., Jr., Molina, B. S. G., Waschbusch, D. A., Gnagy, E. M., Sibley, M. H., Babinski, D. E., Walther, C., Cheong, J., Yu, J., & Kent, K. M. (2013). Young adult educational and vocational outcomes of children diagnosed with ADHD. Journal of Abnormal Child Psychology, 41(1), 27–41. https://doi.org/https://doi.org/10.1007/s10802-012-9658-z
- Lahey, B. B., Applegate, B., McBurnett, K., Biederman, J., Greenhill, L., Hynd, G. W., … Richters, J. (1994). DMS-IV field trials for attention deficit hyperactivity disorder in children and adolescents. The American Journal of Psychiatry, 151(11), 1673–1685. https://doi.org/https://doi.org/10.1176/ajp.151.11.1673
- Lai, R. P., Ellefson, M. R., & Hughes, C. (2019). Executive Function and Metacognition Show Independent Associations with Academic Performance During Late Childhood and Early Adolescence. https://doi.org/https://doi.org/10.31234/osf.io/4jhnz
- Lange, S. M. (2018). ADHD and comorbid developmental coordination disorder: Implications and recommendations for school psychologists. Contemporary School Psychology, 22(1), 30–39. https://doi.org/https://doi.org/10.1007/s40688-017-0122-5
- Lee, K., Ng, S. F., Pe, M. L., Ang, S. Y., Hasshim, M. N. A. M., & Bull, R. (2012). The cognitive underpinnings of emerging mathematical skills: Executive functioning, patterns, numeracy, and arithmetic. British Journal of Educational Psychology, 82(1), 82–99. https://doi.org/https://doi.org/10.1111/j.2044-8279.2010.02016.x
- Lee, S. E., Kibby, M. Y., Cohen, M. J., Stanford, L., Park, Y., & Strickland, S. (2016). Differences in memory functioning between children with attention-deficit/hyperactivity disorder and/or focal epilepsy. Child Neuropsychology, 22(8), 979–1000. https://doi.org/https://doi.org/10.1080/09297049.2015.1060955
- LeFevre, J.-A., Berrigan, L., Vendetti, C., Kamawar, D., Bisanz, J., Skwarchuk, S.-L., & Smith-Chant, B. L. (2013). The role of executive attention in the acquisition of mathematical skills for children in grades 2 through 4. Journal of Experimental Child Psychology, 114(2), 243–261. https://doi.org/https://doi.org/10.1016/j.jecp.2012.10.005
- Lemaire, P., & Lecacheur, M. (2011). Age-related changes in children’s executive functions and strategy selection: A study in computational estimation. Cognitive Development, 26(3), 282–294. https://doi.org/https://doi.org/10.1016/j.cogdev.2011.01.002
- Lenhard, W., & Lenhard, A. (2016). Calculation of effect sizes. Psychometrica. https://www.psychometrica.de/effect_size.html
- Leo, J., & Cohen, D. (2003). Broken brains or flawed studies? A critical review of ADHD neuroimaging research. The Journal of Mind and Behavior, 29–55.
- Li, Y., Geary, D. C., & Paterson, K. (2013). Developmental gains in visuospatial memory predict gains in maths achievement. PLoS ONE, 8(7), e70160. https://doi.org/https://doi.org/10.1371/journal.pone.0070160
- Liu, C.-Y., Huang, W.-L., Kao, W.-C., & Gau, S. S.-F. (2017). Influence of disruptive behavior disorders on academic performance and school functions of youths with attention-deficit/hyperactivity disorder. Child Psychiatry and Human Development, 48(6), 870–880. https://doi.org/https://doi.org/10.1007/s10578-017-0710-7
- Lo-Castro, A., D’Agati, E., & Curatolo, P. (2011). ADHD and genetic syndromes. Brain & Development, 33(6), 456–461. https://doi.org/https://doi.org/10.1016/j.braindev.2010.05.011
- Loe, I. M., & Feldman, H. M. (2007). Academic and educational outcomes of children with ADHD. Journal of Pediatric Psychology, 32(6), 643–654. https://doi.org/https://doi.org/10.1093/jpepsy/jsl054
- Luchini, C., Stubbs, B., Solmi, M., & Veronese, N. (2017). Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World Journal of Meta-Analysis, 5(4), 80–84.https://doi.org/http://doi.org/10.13105/wjma.v5.i4.80
- Luo, Y., Weibman, D., Halperin, J., & Li, X. (2019). A review of heterogeneity in Attention Deficit/Hyperactivity Disorder (ADHD). Frontiers in Human Neuroscience, 13, 42. https://doi.org/https://doi.org/10.3389/fnhum.2019.00042
- Mahone, E. M., Hagelthorn, K. M., Cutting, L. E., Schuerholz, L. J., Pelletier, S. F., Rawlins, C., Singer, H. S., & Denckla, M. B. (2002). Effects of IQ on executive function measures in children with ADHD. Child Neuropsychology, 8(1), 52–65. https://doi.org/https://doi.org/10.1076/chin.8.1.52.8719
- Mayes, S. D., & Calhoun, S. L. (2007). Wechsler intelligence scale for children-third and -fourth edition: Predictors of academic achievement in children with attention-deficit/hyperactivity disorder. School Psychology Quarterly, 22(2), 234–249. https://doi.org/https://doi.org/10.1037/1045-3830.22.2.234
- Mayes, S. D., Calhoun, S. L., Bixler, E. O., & Zimmerman, D. N. (2009). IQ and neuropsychological predictors of academic achievement. Learning and Individual Differences, 19(2), 238–241. https://doi.org/https://doi.org/10.1016/j.lindif.2008.09.001
- Mayes, S. D., Waschbusch, D. A., Calhoun, S. L., & Mattison, R. E. (2020). Correlates of academic overachievement, nondiscrepant achievement, and learning disability in ADHD, autism, and general population samples. Exceptionality, 28(1), 60–75. https://doi.org/https://doi.org/10.1080/09362835.2020.1727324
- Mazzocco, M. M., Devlin, K. T., & McKenney, S. J. (2008). Is it a fact? Timed arithmetic performance of children with mathematical learning disabilities (MLD) varies as a function of how MLD is defined. Developmental Neuropsychology, 33(3), 318–344. https://doi.org/https://doi.org/10.1080/87565640801982403
- Miranda-Casas, A., Colomer, C., Fernández, I., & Presentación, M.-J. (2012). Executive functioning and motivation of children with attention deficit hyperactivity disorder (ADHD) on problem solving and calculation tasks. Revista De Psicodidactica, 17(1), 51–71. https://www.redalyc.org/articulo.oa?id=17523162007
- Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cognitive Psychology, 41(1), 49–100. https://doi.org/https://doi.org/10.1006/cogp.1999.0734
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269. https://doi.org/https://doi.org/10.7326/0003-4819-151-4-200908180-00135
- Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., Shekelle, P., & Stewart, L. A. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews, 4(1), 1–9. https://doi.org/https://doi.org/10.1186/2046-4053-4-1
- Molina, B. S., Hinshaw, S. P., Swanson, J. M., Arnold, L. E., Vitiello, B., Jensen, P. S., Abikoff, H. B., Hechtman, L., Abikoff, H. B., Elliott, G. R., Greenhill, L. L., Newcorn, J. H., Wells, K. C., Wigal, T., Gibbons, R. D., Hur, K., Houck, P. R., & Epstein, J. N. (2009). The MTA at 8 years: Prospective follow-up of children treated for combined-type ADHD in a multisite study. Journal of the American Academy of Child and Adolescent Psychiatry, 48(5), 484–500. https://doi.org/https://doi.org/10.1097/CHI.0b013e31819c23d0
- Monette, S., Bigras, M., & Guay, M.-C. (2011). The role of the executive functions in school achievement at the end of Grade 1. Journal of Experimental Child Psychology, 109(2), 158–173. https://doi.org/https://doi.org/10.1016/j.jecp.2011.01.008
- Nevis, I., Sikich, N., Ye, C., & Kabali, C. (2015). Quality control tool for screening titles and abstracts by second reviewer: QCTSTAR. Journal of Biom Biostat, 6(230), 2. https://doi.org/https://doi.org/10.4172/2155-6180.1000230
- Nigg, J. T., Stavro, G., Ettenhofer, M., Hambrick, D. Z., Miller, T., & Henderson, J. M. (2005). Executive functions and ADHD in adults: Evidence for selective effects on ADHD symptom domains. Journal of Abnormal Psychology, 114(4), 706. https://doi.org/https://doi.org/10.1037/0021-843X.114.3.706
- Nikolas, M. A., & Nigg, J. T. (2013). Neuropsychological performance and attention-deficit hyperactivity disorder subtypes and symptom dimensions. Neuropsychology, 27(1), 107. https://doi.org/https://doi.org/10.1037/a0030685
- O'Brien, J. W., Dowell, L. R., Mostofsky, S. H., Denckla, M. B., & Mahone, E. M. (2010). Neuropsychological profile of executive function in girls with attention[1]deficit/hyperactivity disorder. Archives of Clinical Neuropsychology, 25(7), 656–670. https://doi.org/https://doi.org/10.1093/arclin/acq050
- Passolunghi, M. C., Cargnelutti, E., & Pastore, M. (2014). The contribution of general cognitive abilities and approximate number system to early maths. British Journal of Educational Psychology, 84(4), 631–649. https://doi.org/https://doi.org/10.1111/bjep.12054
- Passolunghi, M. C., Marzocchi, G. M., & Fiorillo, F. (2005). Selective effect of inhibition of literal or numerical irrelevant information in children with attention deficit hyperactivity disorder (ADHD) or arithmetic learning disorder (ALD). Developmental Neuropsychology, 28(3), 731–753. https://doi.org/https://doi.org/10.1207/s15326942dn2803_1
- Polanczyk, G., De Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The worldwide prevalence of ADHD: A systematic review and metaregression analysis. American Journal of Psychiatry, 164(6), 942–948. https://doi.org/https://doi.org/10.1176/ajp.2007.164.6.942
- Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C., & Rohde, L. A. (2014). ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2), 434–442. https://doi.org/https://doi.org/10.1093/ije/dyt261
- Polanin, J. R., Pigott, T. D., Espelage, D. L., & Grotpeter, J. K. (2019). Best practice guidelines for abstract screening large‐evidence systematic reviews and meta‐analyses. Research Synthesis Methods, 10(3), 330–342. https://doi.org/https://doi.org/10.1002/jrsm.1354
- Powers, R. L., Marks, D. J., Miller, C. J., Newcorn, J. H., & Halperin, J. M. (2008). Stimulant treatment in children with attention-deficit/hyperactivity disorder moderates adolescent academic outcome. Journal of Child and Adolescent Psychopharmacology, 18(5), 449–459. https://doi.org/https://doi.org/10.1089/cap.2008.021
- Rapport, M. D., Alderson, R. M., Kofler, M. J., Sarver, D. E., Bolden, J., & Sims, V. (2008). Working memory deficits in boys with attention-deficit/hyperactivity disorder (ADHD): The contribution of central executive and subsystem processes. Journal of Abnormal Child Psychology, 36(6), 825–837. https://doi.org/https://doi.org/10.1007/s10802-008-9215-y
- Rapport, M. D., Orban, S. A., Kofler, M. J., & Friedman, L. M. (2013). Do programs designed to train working memory, other executive functions, and attention benefit children with ADHD? A meta-analytic review of cognitive, academic, and behavioral outcomes. Clinical Psychology Review, 33(8), 1237–1252. https://doi.org/https://doi.org/10.1016/j.cpr.2013.08.005
- Rasmussen, P., & Gillberg, C. (2000). Natural outcome of ADHD with developmental coordination disorder at age 22 years: a controlled, longitudinal, community-based study. Journal of the American Academy of Child & Adolescent Psychiatry, 39(11), 1424–1431. https://doi.org/https://doi.org/10.1097/00004583-200011000-00017
- Reale, L., Bartoli, B., Cartabia, M., Zanetti, M., Costantino, M. A., Canevini, M. P., Rossi, G., & Termine, C. (2017). Comorbidity prevalence and treatment outcome in children and adolescents with ADHD. European Child & Adolescent Psychiatry, 26(12), 1443–1457. https://doi.org/https://doi.org/10.1007/s00787-017-1005-z
- Rhodes, S., Coghill, D., & Matthews, K. (2004). Methylphenidate restores visual memory, but not working memory function in attention deficit-hyperkinetic disorder. Psychopharmacology, 175(3), 319–330. https://doi.org/https://doi.org/10.1007/s00213-004-1833-7
- Rhodes, S. M., Coghill, D. R., & Matthews, K. (2005). Neuropsychological functioning in stimulant-naive boys with hyperkinetic disorder. Psychological Medicine, 35(8), 1109–1120. https://doi.org/https://doi.org/10.1017/S0033291705004599
- Rhodes, S. M., Coghill, D. R., & Matthews, K. (2006). Acute neuropsychological effects of methylphenidate in stimulant drug‐naïve boys with ADHD II–broader executive and non‐executive domains. Journal of Child Psychology and Psychiatry, 47(11), 1184–1194. https://doi.org/http://dx.doi.org/10.1111/j.1469-7610.2006.01633.x
- Rhodes, S. M., Park, J., Seth, S., & Coghill, D. R. (2012). A comprehensive investigation of memory impairment in attention deficit hyperactivity disorder and oppositional defiant disorder. Journal of Child Psychology and Psychiatry, 53(2), 128–137. https://doi.org/https://doi.org/10.1111/j.1469-7610.2011.02436.x
- Roberts, B. A., Martel, M. M., & Nigg, J. T. (2017). Are there executive dysfunction subtypes within ADHD? Journal of Attention Disorders, 21(4), 284–293. https://doi.org/https://doi.org/10.1177/1087054713510349
- Robinson, K. M., & Dubé, A. K. (2013). Children’s additive concepts: Promoting understanding and the role of inhibition. Learning and Individual Differences, 23, 101–107. https://doi.org/https://doi.org/10.1016/j.lindif.2012.07.016
- Rose, S. A., Feldman, J. F., & Jankowski, J. J. (2011). Modeling a cascade of effects: The role of speed and executive functioning in preterm/full‐term differences in academic achievement. Developmental Science, 14(5), 1161–1175. https://doi.org/https://doi.org/10.1111/j.1467-7687.2011.01068.x
- Rourke, B. P. (1993). Arithmetic disabilities, specific and otherwise: A neuropsychological perspective. Journal of Learning Disabilities, 26(4), 214–226. https://doi.org/https://doi.org/10.1177/002221949302600402
- Ruiz-Goikoetxea, M., Cortese, S., Aznarez-Sanado, M., Magallon, S., Luis, E. O., Zallo, N. A., Castro-Manglano, P. D., Soutullo, C., & Arrondo, G. (2017). Risk of unintentional injuries in children and adolescents with ADHD and the impact of ADHD medications: Protocol for a systematic review and meta-analysis. BMJ Open, 7(9), e018027. https://doi.org/https://doi.org/10.1136/bmjopen-2017-018027
- Sabagh-Sabbagh, S., & Pineda, D. A. (2010). Cognitive inhibitory control and arithmetic word problem solving in children with attention deficit/hyperactivity disorder: A pilot study. Universitas Psychologica, 9(3), 761–772. https://doi.org/https://doi.org/10.11144/Javeriana.upsy9-3.cica
- Salthouse, T. A. (2000). Aging and measures of processing speed. Biological Psychology, 54(1–3), 35–54. https://doi.org/https://doi.org/10.1016/S0301-0511(00)00052-1
- Sayal, K., Prasad, V., Daley, D., Ford, T., & Coghill, D. (2018). ADHD in children and young people: prevalence, care pathways, and service provision. The Lancet Psychiatry, 5(2), 175–186.https://doi.org/https://doi.org/10.1016/S2215-0366(17)30167-0
- Schlosser, R. W. (2007). Appraising the quality of systematic reviews. Focus, 17, 1–8. https://ktdrr.org/ktlibrary/articles_pubs/ncddrwork/focus/focus17/Focus17.pdf
- Shalev, R. S., Auerbach, J., & Gross‐Tsur, V. (1995). Developmental dyscalculia behavioral and attentional aspects: A research note. Journal of Child Psychology and Psychiatry, 36(7), 1261–1268. https://doi.org/https://doi.org/10.1111/j.1469-7610.1995.tb01369.x
- Shanahan, M. A., Pennington, B. F., Yerys, B. E., Scott, A., Boada, R., Willcutt, E. G., Olson, R. K., & DeFries, J. C. (2006). Processing speed deficits in attention deficit/hyperactivity disorder and reading disability. Journal of Abnormal Child Psychology, 34(5), 584. https://doi.org/https://doi.org/10.1007/s10802-006-9037-8
- Shin M.S., Cho S.C., Chun S.Y., Hong K.E. (2000). A study of the development and standardization of ADHD diagnostic system. Journal of Korean Academy of Child and Adolescent Psychiatry, 11, 91–99. https://www.koreascience.or.kr/article/JAKO200036036137518.page
- Shvedko, A., Whittaker, A. C., Thompson, J. L., & Greig, C. A. (2018). Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults: A systematic review and meta-analysis of randomised controlled trials. Psychology of Sport and Exercise, 34, 128–137. https://doi.org/https://doi.org/10.1016/j.psychsport.2017.10.003
- Siegler, R., & Araya, R. (2005). A computational model of conscious and unconscious strategy discovery. Advances In Child Development And Behavior, 33, 1–42. https://doi.org/https://doi.org/10.1016/S0065-2407(05)80003-5
- Sikora, D. M., Haley, P., Edwards, J., & Butler, R. W. (2002). Tower of London test performance in children with poor arithmetic skills. Developmental Neuropsychology, 21(3), 243–254. https://doi.org/https://doi.org/10.1207/S15326942DN2103_2
- Silva, D., Colvin, L., Glauert, R., Stanley, F., Srinivas Jois, R., & Bower, C. (2020). Literacy and numeracy underachievement in boys and girls with ADHD. Journal of Attention Disorders, 24(10), 1392–1402. https://doi.org/https://doi.org/10.1177/1087054715613438
- Simms, V., McKeaveney, C., Sloan, S., & Gilmore, C. (2019). Interventions to improve mathematical achievement in primary school-aged children. Ulster University. https://www.nuffieldfoundation.org/wp-content/uploads/2019/11/web-00553-05_UU_A4_Report_v7.pdf
- Sonuga-Barke EJ, Coghill D. (2014). The foundations of next generation attention-deficit/hyperactivity disorder neuropsychology: building on progress during the last 30 years. Journal of Child Psychological Psychiatry 55(12):e1–5. https://doi.org/https://doi.org/10.1111/jcpp.12360
- Sonuga-Barke, E., Bitsakou, P., & Thompson, M. (2010). Beyond the dual pathway model: Evidence for the dissociation of timing, inhibitory, and delay-related impairments in attention-deficit/hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 49(4), 345–355. https://doi.org/https://doi.org/10.1016/j.jaac.2009.12.018
- Stein, D. J., Lund, C., & Nesse, R. M. (2013). Classification systems in psychiatry: Diagnosis and global mental health in the era of DSM-5 and ICD-11. Current Opinion in Psychiatry, 26(5), 493. https://doi.org/https://doi.org/10.1097/YCO.0b013e3283642dfd
- Stewart, T. M., Hunter, S. C., & Rhodes, S. M. (2017). A narrative synthesis of the applicability of the CaR–FA–X model in child and adolescent populations: A systematic review. Memory, 25(9), 1161–1190. https://doi.org/https://doi.org/10.1080/09658211.2016.1275699
- Sturm, A., Rozenman, M., Piacentini, J. C., McGough, J. J., Loo, S. K., & McCracken, J. T. (2018). The effect of neurocognitive function on math computation in pediatric ADHD: Moderating influences of anxious perfectionism and gender. Child Psychiatry and Human Development, 49(5), 822–832. https://doi.org/https://doi.org/10.1007/s10578-018-0798-4
- Swanson, H. L., Lussier, C. M., & Orosco, M. J. (2015). Cognitive strategies, working memory, and growth in word problem solving in children with math difficulties. Journal of Learning Disabilities, 48(4), 339–358. https://doi.org/https://doi.org/10.1177/0022219413498771
- Swanson, L., & Kim, K. (2007). Working memory, short-term memory, and naming speed as predictors of children’s mathematical performance. Intelligence, 35(2), 151–168. https://doi.org/https://doi.org/10.1016/j.intell.2006.07.001
- Szucs, D., Devine, A., Soltesz, F., Nobes, A., & Gabriel, F. (2013). Developmental dyscalculia is related to visuo-spatial memory and inhibition impairment. Cortex, 49(10), 2674–2688. https://doi.org/https://doi.org/10.1016/j.cortex.2013.06.007
- Taylor, E., & Hemsley, R. (1995). Treating hyperkinetic disorders in childhood. British Medical Journal Publishing Group.
- Thorell, L. B. (2007). Do delay aversion and executive function deficits make distinct contributions to the functional impact of ADHD symptoms? A study of early academic skill deficits. Journal of Child Psychology and Psychiatry, 48(11), 1061–1070. https://doi.org/https://doi.org/10.1111/j.1469-7610.2007.01777.x
- Toplak, M. E., West, R. F., & Stanovich, K. E. (2013). Practitioner review: Do performance‐based measures and ratings of executive function assess the same construct? Journal of Child Psychology and Psychiatry, 54(2), 131–143. https://doi.org/https://doi.org/10.1111/jcpp.12001
- Tosto, M. G., Momi, S., Asherson, P., & Malki, K. (2015). A systematic review of attention deficit hyperactivity disorder (ADHD) and mathematical ability: Current findings and future implications. BMC Medicine, 13(1). https://doi.org/https://doi.org/10.1186/s12916-015-0414-4
- Valentine, J. C., Pigott, T. D., & Rothstein, H. R. (2010). How many studies do you need? A primer on statistical power for meta-analysis. Journal of Educational and Behavioral Statistics, 35(2), 215–247. https://doi.org/http://doi.org/10.3102/1076998609346961
- Verguts, T., & Fias, W. (2005). Interacting neighbors: A connectionist model of retrieval in single-digit multiplication. Memory & Cognition, 33(1), 1–16. https://doi.org/https://doi.org/10.3758/BF03195293
- Wang, B.-Q., Yao, N.-Q., Zhou, X., Liu, J., & Lv, Z.-T. (2017). The association between attention deficit/hyperactivity disorder and internet addiction: A systematic review and meta-analysis. BMC Psychiatry, 17(1), 260. https://doi.org/https://doi.org/10.1186/s12888-017-1408-x
- Wechsler, D. (1980). Escala de Inteligencia para niños de Wechsler Revisada (WISC-R). TEA Ediciones.
- Wechsler, D. (1996). Wechsler objective numerical dimensions. Psychological Corporation.
- Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. (2012). The Newcastle-Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm
- Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biological Psychiatry, 57(11), 1336–1346. https://doi.org/https://doi.org/10.1016/j.biopsych.2005.02.006
- Willcutt, E. G., Nigg, J. T., Pennington, B. F., Solanto, M. V., Rohde, L. A., Tannock, R., Loo, S. K., Carlson, C. L., McBurnett, K., & Lahey, B. B. (2012). Validity of DSM-IV attention deficit/hyperactivity disorder symptom dimensions and subtypes. Journal of Abnormal Psychology, 121(4), 991. https://doi.org/https://doi.org/10.1037/a0027347
- Wolraich, M. L., Hagan, J. F., Allan, C., Chan, E., Davison, D., Earls, M., Frost, J., Froehlich, T., Frost, J., Holbrook, J. R., Lehmann, C. U., Lessin, H. R., Okechukwu, K., Pierce, K. L., Winner, J. D., Zurhellen, W., & Evans, S. W. (2019). Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics, 144(4), e20192528. https://doi.org/https://doi.org/10.1542/peds.2019-2528
- Zajic, M. C., McIntyre, N., Swain-Lerro, L., Novotny, S., Oswald, T., & Mundy, P. (2018). Attention and written expression in school-age, high-functioning children with autism spectrum disorders. Autism, 22(3), 245–258. https://doi.org/https://doi.org/10.1177/1362361316675121
- Zheng, X., Swanson, H. L., & Marcoulides, G. A. (2011). Working memory components as predictors of children’s mathematical word problem solving. Journal of Experimental Child Psychology, 110(4), 481–498. https://doi.org/https://doi.org/10.1016/j.jecp.2011.06.001