
Abstract
Peculiar characteristics of cytotoxic endometrial cells’ response depending on the clinical aspects (frequency, gestational age, form of miscarriage, hysteroscopic pattern) have been studied. Patients with pregnancy loss in their past medical history demonstrate a decreased level of CD8 + lymphocytes, and the decrease is exacerbated as the incidence of miscarriages increases and in the presence of endometrial hypoplasia. The content of CD16 + lymphocytes increases in comparison with the control group, however, there is a reducing trend of this phenotype of killers as the incidence of miscarriages increases and in the presence of endometrial hypoplasia. Reduction of CD56 + lymphocytes progresses with repeated pregnancy loss and endometrial hyperplasia.
Introduction
Pregnancy loss is a multifactorial problem of reproductive medicine, the etiology of which in 50% of cases is not clearly specified [Citation1]. Various etiologies have been suggested, including chromosomal abnormalities, uterine abnormalities, endocrine diseases, autoimmune diseases, alloimmune anomalies, thrombophilia and an infectious factor [Citation2].
To date, scientific research has focused on genetic and epigenetic polymorphisms associated with the immune response and inflammatory mediators [Citation3]. It has been shown that unspecified causes of miscarriage may result from immune system imbalance caused by Th1/Th2/Th17 cytokines and Treg cells [Citation4]. A key role in the pathogenesis of miscarriage is attributed to natural endometrial killers, the severity of cytotoxic potential is associated with the luteal-phase defect, the presence of uterine fibroids, endometriosis, chronic endometritis, polycystic ovary syndrome, hyperandrogenia, hyperprolactinemia, thyroid dysfunction, diabetes and thrombophilia of various origin and karyotype anomalies [Citation5].
Clinically, it is of practical interest to study the peculiar characteristics of the response of cytotoxic cells depending on the frequency (single or recurrent miscarriage), the period of loss of pregnancy (ovular or late miscarriage), the form of miscarriage (spontaneous miscarriage or undeveloped pregnancy), and also on the state of hysteroscopic pattern (endometrial hyperplasia or hypoplasia).
Research objective: is the study of clinical and immunological parallels in patients with a history of pregnancy loss.
Materials and methods of research
The study included 50 women who came to the Scientific Center of Obstetrics, Gynecology and Perinatology in Almaty. The control group included of 20 patients with normal menstrual function and with no reproductive losses. All patients were divided into two study groups: the first group (main group) comprised 30 patients with a history of miscarriage, the second group (control group) – 20 patients with normal menstrual function and with no reproductive losses. Each woman was provided with an individual card, which included examination results with the study of complaints, medical and obstetric-gynecologic history, general and gynecological status data, conventional laboratory tests, and special examination methods, such as pelvic ultrasound, blood hormone levels, ELISA for infection, detection of lupus coagulant and anti-HCG in the blood, consultation of geneticist and karyotyping.
The average age of the women in the first group was 31.8 ± 2.4 years (23–52 years old), second group – 28.6 ± 2.6 years (21–44 years old), that is, the groups were comparable in age.
Characteristics of menstrual function have shown that the average age of onset of menarche in group 1 was 14.2 ± 1.6 years old while it was 12.7 ± 1.4 years old in the second group. When analyzing the reproductive function, the following was discovered. All patients in the first group had a history of one or more episodes of pregnancy loss. The reproductive function is significantly impacted by the woman’s past pregnancies and childbirths, as well as their outcome. When analyzing the number of pregnancies and childbirth in women, we noted that the majority (53.3%) of the patients in the main group had a history of 2–3 pregnancies, 26.7% had 4–5 pregnancies, and 3.3% had 8 pregnancies, while the outcomes of these pregnancies included spontaneous abortions of 23.3%, undeveloped pregnancy of 43.3% and a combination of miscarriage and undeveloped pregnancy – in 26.7% of cases.
Miscarriage was observed in all patients in group 1, where 43.3% of women suffered from habitual miscarriage. Premature births occurred in 18.5% of cases in the first group, and in one patient’s history premature birth resulted in a birth of a child with multiple congenital defects (there was an antenatal fetal death), two patients had repeated premature births with antenatal and early neonatal fetal death.
In the control group, 65% of women had repeated pregnancies: 1 pregnancy – in 35%, 2–3 pregnancies – in 60% of patients, 4–5 pregnancies – 5% of patients. Child birth only as a result of pregnancy was observed in 60%, a combination of childbirth and therapeutic abortions – in 30% of women.
Obstetric and gynecological history in the main group of patients was burdened in the overwhelming majority of women (76.7%). In the control group, obstetric and gynecologic history was burdened by therapeutic abortion in six patients (30%). Two women (10%) had an ectopic pregnancy in their history. Diseases of the female reproductive system were primarily detected in patients of the treatment group: cervical erosion (26.7%), adnexitis (33.3%), uterine fibroids (10%), ectopic pregnancy (3.3%). Among treatment group 10% of patients had ectopic pregnancy and infertility in their medical history, one patient had a bicornuate uterus. The study of hemostasiogram detected thrombophilia in 13.3% of cases. During karyotyping, normal karyotype was detected in all examined patients.
Bacterioscopic presentation typical for coleitis (the presence of an increased number of white blood cells per HPF in a smear in combination with a mixed and coccal microflora) was observed in 43.3% of the women in group 1. The majority (80%) of patients in group I had concurrent infections, mostly HSV and CMV infection – 17 cases (56.7%), chlamydia – 7 (23.3%), ureaplasma and mycoplasma – 3 cases each (10% each). According to hormone level tests, hyperprolactinemia was more common in the women from the first group – 4 patients (13.3%), hyperandrogenia – 7 patients (23.3%); in two cases, there was estrogen deficiency (6.7%) and in one case – its excess (3.3%).
Endoscopic examination of the uterine cavity was performed in 20 patients with a history of miscarriage, using a hysteroscope by Karl Storz Company (Germany). The most common hysteroscopic pattern, typical of chronic endometritis with endometrial hyperplasia and polyps – in 60% of cases. In endometrial hypoplasia, occurring in 40% of cases, a pale, dull-color whitish mucosal was found, irregular in thickness with a predominant thinned endometrium.
The material for immunology research were biopsy samples of the uterine endometrium, obtained in pipel-biopsy using Goldstein catheter. Isolation of immunocompetent cells from endometrial tissue was carried out using azymous method. Endometrial fragments were placed in a Medicon container (Becton Dickenson), added a phosphate buffer and grounded in a Medimachine tissue grinder (Becton Dickenson) for several minutes. The resulting cell-rich fluid was centrifuged for 30 min in a ficoll verografin velocity sedimentation gradient (d = 1.078). The content of cytotoxic CD8+, CD16+, CD56 + lymphocytes and the ratio between CD56 + and CD16 + cells, CD8 + and CD16 + cells was determined.
Research findings
The data characterizing peculiar characteristics of the population structure of endometrial cytotoxic lymphocytes in pregnancy loss (PL) in past medical history are shown in .
Figure 1. Content ratio of endometrial lymphocytes in patients with PL, %.
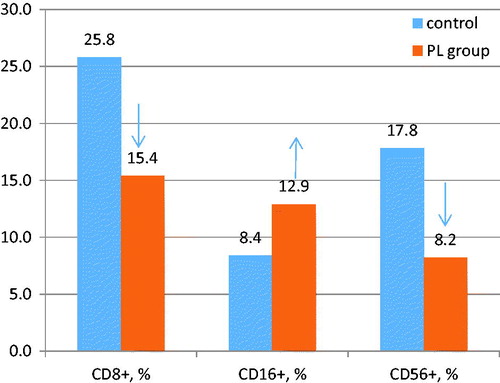
It was found that in patients with PL in the medical history, the level of CD8 + endometrial lymphocytes was lowered (p < .05), and in a third of patients, a decrease in the level was observed thrice. The average content of endometrial natural killers with the CD16 + phenotype in the main group exceeded the stated values (p <.05), while the content of CD56 + cells was suppressed (p < .05). A relevant (p < .05) decrease in the CD56+/CD16 + index to 0.7 and CD8+/CD16 + to 0.8 occurred in patients with PL.
It should be noted that in the medical history of women from the main group, there were repeated intrauterine interventions, which may result in the development of chronic endometritis, which in turn is associated with structural and functional changes aggravating not only the risk of sporadic pregnancy loss, but also the risk of recurrent pregnancy loss, that is, development of a set of habitual miscarriage symptoms. Each lost pregnancy adversely affects the condition of reproductive system.
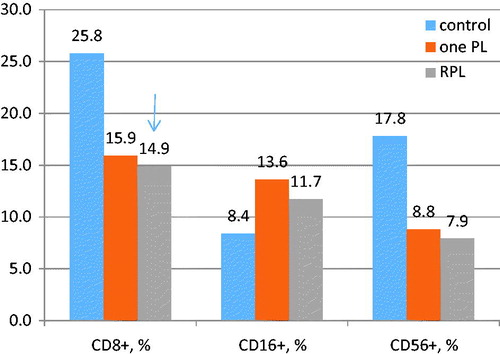
Therefore, we conducted further analysis of the levels of cytotoxic endometrial lymphocytes depending on the number of pregnancy losses. Patients were divided into two groups: one group with one pregnancy loss (one PL) – 17 patients and the other one – with recurrent pregnancy loss (RPL) – 13 patients. As can be seen in , with recurrent miscarriages, the percentage of endometrial CD8 + lymphocytes significantly decreased, and the level of CD56 + cells tended to decrease in comparison with the control group. However, the content of CD16 + cells tended to decrease compared to the group with a single miscarriage. This circumstance affected a significant (p < .05) decrease in the CD56+/CD16 + index to 0.8 and of CD8+/CD16 + index to 0.3 in patients with RPL.
Figure 2. The relative content of endometrial lymphocytes.
Pregnancy loss in the early stages (up to 12 weeks) is manifested by activation of cytotoxic natural killers with CD16 + phenotype and express suppression of the endometrial type level of CD56 + cells, and in late stages (13–22 weeks of pregnancy) manifests a cellular deficiency, accompanied by a decrease in all cytotoxic lymphocytes – CD8+, and natural CD56 + and CD16 + killers [Citation6].
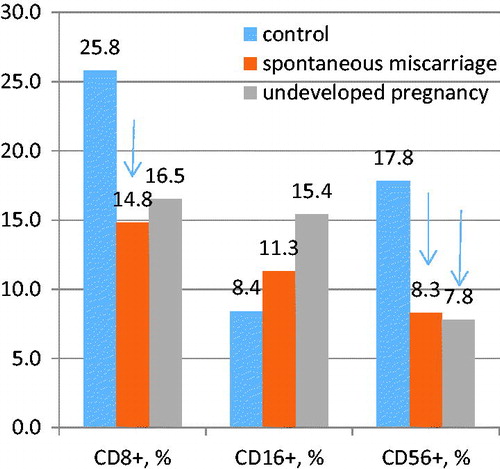
Analysis of endometrial cytotoxic lymphocytes levels depending on the form of pregnancy loss – spontaneous miscarriage and undeveloped pregnancy, with antenatal fetal death with its long delay in the uterine cavity. As can be seen from , in a spontaneous miscarriage, the percentage of endometrial CD8 + and CD56 + lymphocytes significantly decreased, while the level of CD16 + cells tended to increase. This impacted on a significant (p < .05) decrease in the CD56+/CD16 + index to 0.8 and CD8+/CD16 + index to 0.8. In an undeveloped pregnancy, a decrease in CD56 + lymphocytes and a downward trend of CD8 + lymphocytes was significant, while CD56+/CD16 + indices significantly decreased to 0.7 and CD8+/CD16+ - to 0.9.
Figure 3. Endometrial lymphocytes count.
We also noted the peculiar characteristics of cytotoxic responses depending on the presence of hyperplastic endometrial processes. The data characterizing the peculiarities of population structure of endometrial cytotoxic lymphocytes in endometrial hyper- and hypoplasia in patients with a history of miscarriage are shown in .
Figure 4. Endometrial lymphocytes count.

It was found that both in endometrial hyperplasia and endometrial hypoplasia, the level of endometrial CD8 + cytotoxic/suppressor lymphocytes was significantly lower in patients with miscarriage (p < .05), and in hypoplasia the decrease was more pronounced (2 times or more).
With endometrial hyperplasia, the average content of endometrial natural killers with CD16 + phenotype was significantly increased, while the content of CD56 + cells was reduced. This impacted a significant (p < .05) decrease in the CD56+/CD16 + and CD8+/CD16 + index as compared to that in the control group.
In endometrial hypoplasia, the average count of natural killers with CD16 + phenotype also tended to increase, while the content of CD56 + cells decreased. However, the CD56+/CD16 + index tended to decrease, but not significantly. At the same time, the CD8+/CD16 + index reduced significantly (p < .05).
Thus, in patients with the history of pregnancy loss, a decrease in the level of CD8 + lymphocytes is observed, and the decline is exacerbated with increasing frequency, the stage of miscarriage and the presence of endometrial hypoplasia. The CD16 + lymphocytes count increases in comparison with the control group, but there is a downward trend of this phenotype of killers as the number and stage of miscarriage increase and in the presence of endometrial hypoplasia. Reduction of CD56 + lymphocytes increases with repeated pregnancy loss, undeveloped pregnancy and endometrial hyperplasia.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Diejomaoh MF. Recurrent spontaneous miscarriage is still a challenging diagnostic and therapeutic quagmire. Med Princ Pract 2015;24:38–55.
- Mamedaliyeva NM, Kurmanova AM, Kurmanova GM. Immunopathogenetic aspects of recurrent miscarriage with infectious genesis. In book: Recurrent pregnancy loss. Prevalence, risk factors and outcomes. Ed. Lilliana R. Evans. New York: Nova Science Publishers; 2016:1–32.
- Tur-Torres MH, Garrido-Gimenez C, Alijotas-Reig J. Genetics of recurrent miscarriage and fetal loss. Best Pract Res Clin Obstet Gynaecol 2017;42:11–25. doi:10.1016/j.bpobgyn.2017.03.007
- Mamedaliyeva NM, Lokshin VN, Kurmanova AM. Comprehensive assessment of immunity and approaches to differentiated immunocorrection in recurrent miscarriage. Gynecol.Endocrinol 2015;31:55–7.
- Seshadri S, Sunkara SK. Natural killer cells in female infertility and recurrent miscarriage: a systematic review and meta-analysis. Hum Reprod Update 2014;20:429–38.
- Mamedaliyeva NM, Kurmanova AM, Moshkalova GN, Kim V. Local immunity status in patients with miscarriages and herpetic infection. Gynecol. Endocrinol 2016;32:45–6.