
ABSTRACT
Many of the risk factors for violence against children are particularly prevalent in families and communities affected by HIV/AIDS. Yet, in sub-Saharan Africa, where HIV rates are high, efforts to prevent or address violence against children and its long-lasting effects are hampered by a lack of evidence. We assessed the relationship between violence exposure and mental health among HIV-affected children attending community-based organisations in South Africa (n = 834) and Malawi (n = 155, total sample n = 989) at baseline and 12–15-month follow-up. Exposure to violence in the home and in the community was high. HIV-negative children who lived with an HIV-positive person experienced most violence overall, followed by HIV-positive children. Children unaffected by HIV experienced least violence (all p < .05). Interpersonal violence in the home predicted child depression (β = 0.17, p < .001), trauma symptoms (β = 0.17, p < .001), lower self-esteem (β = −0.17, p < .001), and internalising and externalising behavioural problems (β = 0.07, p < .05), while exposure to community violence predicted trauma symptoms (β = 0.16, p < .001) and behavioural problems (β = 0.07, p < .05). Harsh physical discipline predicted lower self-esteem (β = −0.18, p < .001) and behavioural problems for children (β = 0.24, p < .001). Exposure to home (OR: 1.89, 95% CI: 1.23–2.85) and community violence predicted risk behaviour (OR: 2.39, 95% CI: 1.57–3.62). Over time, there was a decrease in depressed mood and problem behaviours, and an increase in self-esteem for children experiencing different types of violence at baseline. This may have been due to ongoing participation in the community-based programme. These data highlight the burden of violence in these communities and possibilities for programmes to include violence prevention to improve psychosocial well-being in HIV-affected children.
KEYWORDS:
Introduction
Freedom from experiencing and witnessing violence is fundamental to the rights of children. The 2006 UN Secretary-General's study on violence concluded that violence against children is pervasive, occurring in all countries, and in many cases entrenched in the cultural, economic, and social frameworks of societies (United Nations, Citation2006; World Health Organization, Citation2014). Children who are exposed to violence are more likely to engage in harmful use of substances, risky sexual behaviour, become HIV-infected (Dubowitz & Bennett, Citation2007; Mills et al., Citation2011; Mock, Peden, Hyder, Butchart, & Krug, Citation2008; Richter et al., Citation2014), bully other children (Chaux, Molano, & Podlesky, Citation2009; Fleming & Jacobsen, Citation2010), take part in rape and intimate partner violence later in life (Huesman, Citation2011; Mathews & Benevenuti, Citation2014), be abusive parents (Dubowitz & Bennett, Citation2007), and are also more at risk of abuse or victimisation as adults (Renner & Slack, Citation2006). Harsh physical abuse during childhood has been linked with increased rates of depression and attempted suicide (Norman et al., Citation2012).
Risk of exposure to violence for children is complex and driven by broader societal and cultural norms, as well as community factors, relationships with family and peers, and individual child characteristics (World Health Organization, Citation2002). Importantly, many of the risk factors for violence against children are particularly prevalent in families and communities affected by HIV/AIDS. For example, community risk factors for violence against children include gender inequality, alcohol use, and high levels of community violence (World Health Organization, Citation2006), all of which have also been identified as drivers of HIV transmission and are common in communities with high HIV/AIDS rates (Schneider, Chersich, Neuman, & Parry, Citation2012; Seeley et al., Citation2012). At a family level, HIV is associated with a range of factors that predict child violence, including intimate partner violence (Jewkes, Dunkle, Nduna, & Shai, Citation2010), risk behaviours such as substance use (Betancourt, Meyers-Ohki, Charrow, & Hansen, Citation2013), and HIV-related stigma and social isolation, which can impact others in close contact with someone infected with the virus (Boyes, Mason, & Cluver, Citation2013). On an individual level, factors such as gender and child temperament may place a child at risk of experiencing violence. Children who require higher levels of care, such as those with developmental disabilities (Devries et al., Citation2014) may be more likely to be victims of violence from their carers and others (World Health Organization, Citation2006).
There is very little research on community-based programming to prevent violence in low- and middle-income countries (LMIC) (Skeen, Tomlinson, Ward, Cluver, & Lachman, Citation2015 ; World Health Organization, Citation2014), particularly for vulnerable children such as those affected by HIV. In sub-Saharan Africa, efforts to prevent or address violence against children are hampered by this lack of evidence. In South Africa, rates of interpersonal violence are high (Seedat, Van Niekerk, Jewkes, Suffla, & Ratele, Citation2009), and physical abuse of children is common (Richter & Dawes, Citation2008). The national under-5 homicide rate is more than double that of other LMIC (Norman, Matzopoulos, Groenewald, & Bradshaw, Citation2007) and several times higher than high-income settings (UNICEF, Citation2014). The picture in Malawi is more mixed. The child homicide rate in Malawi is one of the lowest in the region, yet at least 21% of girls report that they have experienced physical violence (UNICEF, Citation2014) and violence against girls has been identified as a key barrier to attending and performing well in school (Bisika, Ntata, & Konyani, Citation2009; Sherr et al., Citation2016). In both Malawi and South Africa, there are high rates of gender-based intimate partner violence (Abrahams, Jewkes, Laubscher, & Hoffman, Citation2006; Rico, Fenn, Abramsky, & Watts, Citation2011). It is likely that children in these countries are also witnesses to violence in their homes and communities – in South Africa 45% of children have witnessed their mother being beaten (Seedat et al., Citation2009).
In addition, there is little research available investigating the relationship between violence exposure and other mental health outcomes of children in sub-Saharan Africa. Most of the research investigating the relationship between exposure to violence and child mental health outcomes in sub-Saharan Africa is focused on post-traumatic stress disorder (PTSD) in adolescents, with studies showing a positive relationship between the number of traumatic events and the severity of PTSD and depression (Suliman et al., Citation2009). Young children affected by HIV/AIDS are a vulnerable population, with those attending community organisations likely to be most at risk (Yakubovich et al., Citation2016), yet many of them are hard to reach and rarely included in research, meaning that we know little about their exposure to violence and its impact. The aim of this study was to assess the rates of child exposure to violence, the relationship with mental health status, and the mental health outcomes over time of children affected by HIV aged 4–13 years attending community-based programmes.
Method
This study reports baseline cross-sectional data from the Child Community Care Study and 12–15-month follow-up. This is a longitudinal study on children affected by HIV/AIDS enrolled at community-based programmes in South Africa and Malawi. The study has ethical approval from the ethics boards at University College London (reference number 1478/002) and Stellenbosch University (reference number N10/04/112).
Procedures
Project partners provided contacts of all supported community-based organisations (CBOs) programmes delivering services directly to children affected by HIV/AIDS aged 4–13 years. This yielded 588 CBOs in total (524 in South African and 64 in Malawi) which were stratified by partner and geographical location, and 28 organisations (24 in South Africa and 4 in Malawi) were randomly selected for study inclusion. At each CBO, the research team interviewed approximately 35 consecutive children attending the CBO and their primary caregiver. Primary caregivers received full information on the study and gave written consent to participate. Children were given information and provided written assent. Carer and child interviews were conducted by trained data collectors using mobile phones for data collection (Tomlinson et al., Citation2009). Participants were followed up 15 months after baseline data was acquired, with a follow-up rate of 86.3%.
Measures
The questionnaires included questions relating to gender, age, country, carer relationship, household employment, housing, and school enrolment. Child and carer HIV status, recent family illness and death were based on carer report.
Child depressed mood was measured using the ten item Children's Depression Inventory-Short Form (Kovacs, Citation1992), which has been used previously in South Africa (Boyes & Cluver, Citation2015; Cluver, Gardner, & Operario, Citation2007). Trauma symptomatology was assessed with the Trauma Symptom Checklist for Children (TSCC) (Briere, Citation1996) a self-report measure which has been used in a middle-income setting country before, but not in sub-Saharan Africa (Li et al., Citation2009). Self-esteem was assessed using the child report Rosenberg Self-Esteem Scale (Rosenberg, Citation1965), which has been used in over 50 countries (Schmitt & Allik, Citation2005) including South Africa (Mueller, Alie, Jonas, Brown, & Sherr, Citation2011). The Strengths and Difficulties Questionnaire (SDQ) (Goodman, Citation1997) was used to measure internalising problems (made up emotional and peer problems) and externalising problems (made up of conduct and hyperactivity-inattention). The SDQ has been extensively validated in both LMIC and high-income countries and has been used in South Africa (Cluver et al., Citation2007). Finally, adolescents (10–13 years) reported on their risk behaviours including substance abuse, delinquency and violence using three selected items from the Social and Health Assessment (SAHA) scales which has been used in South Africa (Mueller et al., Citation2011).
Exposure to interpersonal violence in the home was measured using scale items from a UNICEF survey tool for orphans and vulnerable children (Snider & Dawes, Citation2006) that enquired about children's exposure to violence in the household, both as a victim and as a witness. Harsh discipline practices that involved punishment or maltreatment in the household were reported by the carer using items adapted from the Parent-Child Conflict Tactics Scale (Straus, Hamby, Finkelhor, Moore, & Runyan, Citation1998) and from the International Society for the Prevention of Child Abuse and Neglect screening tools, relating to (a) use of physical violence and (b) use of psychological violence to discipline the child. Exposure to community violence was assessed using scale items from the UNICEF survey tool (Snider & Dawes, Citation2006) that enquired about child's exposure to different forms of violence within the community through witnessing and direct victimisation.
Data analysis
After descriptive analysis, we used t-tests and χ 2 tests to examine associations between exposure to violence and child functioning and mental health. We then used multivariate regression models to examine associations between exposure to violence and child mental health (depressive and trauma symptoms, self-esteem), emotional and behavioural functioning (assessed using SDQ), and risk behaviours (assessed using SAHA scales). Follow-up data were analysed using repeated measures analysis of variance (ANOVA) for continuous outcome variables and multiple logistic regression controlled for baseline for binary outcome variables. These were done to see whether violence exposure at baseline predicted change over time on mental health and behavioural variables. All multivariate analyses (regression and ANOVA) were adjusted for demographic factors (age, gender, and country) and child HIV status. Analyses were carried out using SPSS 20.0 (IBM Corp., Citation2012).
Results
Sample characteristics
In total, 28 CBOs participated, with further 4 being ineligible (insufficient participants (n = 1), closing (n = 2), and government service (n = 1). In total, 989 children participated with their carers; 834 in South Africa and 155 in Malawi. Refusal rate was low (under 1%). Just over half (n = 503, 51%) were female with ages ranging from 4 to 13 years, with a mean age of 8.9 years. At baseline, of the total, 19.4% (n = 185) carers reported being HIV positive and 13.7% (n = 135) reported that their child was HIV positive. Of the total, 21.9% (n = 217) of households reported having a household member sick for more than three months in the last year, while 28.6% (n = 283) reported the death of a household member in the past year. In 46.3% (n = 453) of households, there was no one employed.
At baseline, nearly half of the children had been exposed to interpersonal violence between adults in the home, and 42.5% exposed to violence in their community. Harsh discipline practices were common with 47.8% of carers reporting striking a child with an implement, or on the head or face and 45.4% of caregivers engaging in harsh psychological punishment. compares HIV-positive children, HIV-affected children (HIV negative but living in a household with someone who was HIV positive) and unaffected children. Exposure to violence varied significantly by group with higher rates in the HIV-affected group and lower rates in the unaffected group. Older children (10–13 years, n = 469) were asked about their engagement in risk behaviours, and over a third (34.8%) reported that they had beaten up someone (33.0%), been drunk or high (4.7%), or had been arrested (0.4%).
Figure 1. Rates of domestic and community violence and harsh psychological discipline as a function of child HIV burden. Chi-square difference test was performed for all three types of violence *p < .05, **p < .01.
Children lost to follow-up were more often from South Africa (92.9%) of those who were followed up (82.7%; χ2(1) = 10.42, p = .001). They also more often lived in a shack (25.3% vs. 13.8%; χ2(1) = 12.61, p < .001), and consequently less often lived in a comfortable home (50.7% versus 60.0%; χ2(1) = 4.47, p = .035). However, children lost to follow up were more often food secure (80.1% vs. 71.8%; χ2(1) = 4.65, p = .031). Children who were lost to follow-up and children who were followed up did not differ significantly on any of the violence measures at baseline, nor on mental health measures or any other demographic variables.
Violence exposure and mental health outcomes at baseline
presents associations between various types of violence exposure and child mental health outcomes. Interpersonal violence in the home was significantly associated with higher depression symptom score, higher trauma symptom score, higher behavioural and emotional problems (measured by the SDQ), and lowered self-esteem (all p ≤ .002). Community violence was not associated with depression scores, but was associated with higher trauma scores, and more behavioural and emotional problems (all p ≤ .01). Both harsh physical and psychological discipline measures were associated with lower self-esteem and more behavioural and emotional problems (all p ≤ .01). sets out the associations between exposure to violence and increased problematic risk behaviours, all of which were significant (all p ≤ .01).
Table 1. Associations between exposure to violence and child functioning and mental health.
Table 2. Associations between exposure to violence and risk behaviour among 10–13-year olds (n = 469).
Given the significant associations, the next step was to explore associations with child mental health and behaviour. presents linear regression models of the range of child mental health and behaviour outcomes. After controlling for demographic factors (country, age, gender, and HIV status), exposure to interpersonal violence in the home was found to be the only predictor of increased depressive symptoms (β = 0.17, p ≤ .001). Trauma symptoms were higher for children in Malawi (β = 0.23, p ≤ .001), for girls (β = 0.08, p = .03), and for children exposed to home violence (β = 0.17, p ≤ .001) and community violence (β = 0.16, p ≤ .001). Self-esteem was higher for older children (β = 0.12, p = .001), and for children in South Africa (β = 0.87, p = .02), and was negatively associated with exposure to domestic violence (β = −0.17, p ≤ .001) and harsh physical discipline practices (β = −0.18, p ≤ .001). Internalising and externalising behavioural problems were found to be greater in younger children (β = −0.14, p ≤ .001), and for those who were HIV positive (β = 0.08, p = .008). Exposure to violence in the home or in the community was positively associated with greater internalising and externalising behavioural problems, as was exposure to harsh discipline practices. Boys were more likely to engage in externalising behaviours than girls (β = 0.12, p ≤ .0001). Externalising behaviours were also greater in South Africa (β = 0.12, p = .001) and for children exposed to domestic violence (β = 0.06, p = .04).
Table 3. Linear regression models showing predictors of child outcomes.
We also ran a multivariate logistic regression model to test factors associated with risk behaviours among older children (10 years or above, n = 469) (). Country and exposure to home and community violence were found to be significantly and independently associated with delinquent behaviour. Children living in South Africa were three times more likely to engage in any type of delinquency than those in Malawi (39.4% vs. 17.3%, Adjusted OR: 3.03, 95% CI: 1.63–5.66, p < 0.0001). Children exposed to any type of domestic violence were also more likely to engage in delinquent behaviour (44.7% vs. 26.1%, Adjusted OR: 1.89, 95% CI: 1.23–2.85, p = 0.002), and so were those exposed to community violence (45% vs. 25.1%, Adjusted OR: 2.39, 95% CI: 1.57–3.62, p < 0.0001). Age, gender, HIV status, and exposure to harsh discipline practices were not significantly associated with delinquent behaviour ().
Table 4. Logistic regression model showing predictors of risk behaviour
Mental health outcomes at 15-month follow-up
At follow-up, we investigated changes in mental health outcomes over time and violence exposure. Repeated measures (see and ), controlling for the covariates country, gender, age, and HIV status, showed that there was a significantly larger decrease in depressive symptoms from baseline to follow-up for those children who were exposed to domestic violence at baseline (F(1, 815) = 5.08, p = .024). Trauma symptoms were stable over time for the children who were exposed to community violence at baseline, while they increased for those who were not (F(1, 828) = 6.47, p = .011). Children experiencing harsh physical discipline at baseline had a significantly larger increase in self-esteem (F(1, 701) = 4.73, p = .030) and a decrease in internalising behaviour where the non-exposed group experienced a slight increase (F(1, 821) = 7.86, p = .005). Finally, these children also had a decrease in externalising behaviour where the non-exposed group experienced an increase (F(1, 821) = 8.58, p = .003), an effect which was also found for exposure to domestic violence(F(1, 821) = 7.62, p = .006).
Figure 2. Change of child mental health measures over time according to exposure to domestic and community violence and harsh physical discipline. All differences between exposure and non-exposure to these three types of violence are significant (p < .05).
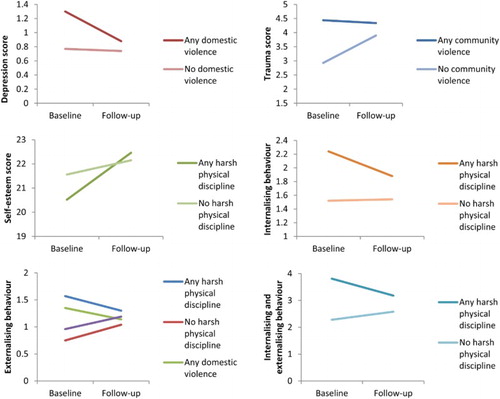
Table 5. Repeated measures ANOVAs showing effects of domestic violence, community violence, harsh physical and harsh psychological discipline on change over time of several psychosocial child outcomes.
Discussion
There are few studies from sub-Saharan countries that have examined the relationship between violence exposure and child mental health outcomes over time, and fewer still exploring very vulnerable populations of children affected by HIV. This study compared exposure to home and community violence and harsh discipline practices with a range of child mental health outcomes over a 15-month period. We found high rates of violence exposure, that children living with someone who was HIV positive were most affected, and that there are a range of negative mental health outcomes and problematic externalising behaviours associated with this exposure to violence.
The high levels of domestic violence are likely to be linked to the fact that the sample was drawn from community organisations that serve children affected by HIV/AIDS, who are living in families in which risk for children may be particularly acute. Previous studies have also found high levels of negative behaviours, including violence, in households where someone is HIV positive, and its impact on children (Betancourt et al., Citation2013). There was also considerable exposure to community violence which was not associated with depressed mood, but with trauma symptoms and behavioural difficulties. Harsh physical violence was associated with low self-esteem and both harsh physical violence and psychological violence were associated with emotional and behavioural problems. Violence between adults in the home was the only independent factor associated with depressive symptoms, and also predicted poorer outcomes across other domains of mental health, including trauma symptoms, low self-esteem, and emotional and behavioural problems. This echoes findings from another recent South African school-based study in which home-based violence was the most significant risk factor for both internalising and externalising mental health problems in 12–15-year olds in an area of high community violence in Cape Town (Du Plessis, Kaminer, Hardy, & Benjamin, Citation2015).
In our findings, older children were more likely to have higher self-esteem scores and lower reported emotional and behavioural problems. This pattern has been noted in previous research, with a decrease in the severity of behavioural problems rated by parents in studies in high-income countries (Niclasen et al., Citation2012). In line with previous findings, boys were also more likely to present with externalising behaviour problems (Crijnen, Achenbach, & Verhulst, Citation2014). There were also country differences in these data. Unsurprisingly, given South Africa's turbulent political past and high levels of inequality (Seedat et al., Citation2009), violence exposure was higher among South African children, and related risk behaviours were three times more common. However, we noted higher trauma symptoms in children from Malawi. The reasons for these country differences are uncertain and it is difficult to draw conclusions about cross-country differences in the context of limited research about the relationship between violence exposure mental health in sub-Saharan African countries. However, a previous cross-country study, based in Kenyan and South African schools, also noted differences in trauma exposure and resultant trauma-related symptoms. In that study, the researchers found higher rates of exposure to violence among Kenyan adolescents, but significantly higher rates of PTSD in their South African counterparts (Seedat, Nyamai, Njenga, Vythilingum, & Stein, Citation2004). The authors suggest that these results may be due to cultural differences in the way in which trauma is understood and experienced, or due to trauma-related factors that were not measured as a part of the study, such as the severity and timing of traumatic events. Both these are potential reasons for this finding in the current study.
Over time, we saw a decrease in symptoms of depressed mood, internalising and externalising behaviours, and an increase in self-esteem score for children experiencing different types of violence exposure at baseline. We propose that this may have been due to ongoing participation in the community-based programme, and that participation in the programme may mitigate the mental health risks experienced by these children over time. Indeed, a previous study showed that attending the CBO reduced violence exposure over time (Sherr et al., Citationin press). This is in spite of the fact that most CBOs do not have a direct focus on violence prevention, but rather a more generalist focus of provision of different forms of psychosocial support, parenting interventions, nutrition, and basic health services in the context of HIV. These may alleviate stressors which trigger violence, or may train skills to allow for alternative discipline and parenting styles which may avoid behavioural problem triggers for violence in the first place. We suggest that CBOs are particularly well placed to work directly with families about issues relating to violence and that there is a potential to develop community-based programming that focuses on violence prevention. Such interventions would benefit from rigorous randomised controlled trial methodology to examine causal relationships and evaluate such input.
We have a growing understanding of the relationship between early negative experiences and brain development, and how chronic “toxic stress” may lead to difficulties in self-regulation, poor control of emotions, and aggressive behaviour in children (Bower & Dawes, Citation2014). However, there is little in the way of programming that is available for use in LMIC with a need to establish the efficacy of parenting programmes to prevent violence in LMIC (Skeen et al., Citation2015; World Health Organization, Citation2014) which are low cost, accessible, culturally appropriate (Ward et al., Citation2012) and delivered by community-level lay health workers (Mejia, Calam, & Sanders, Citation2012). Focusing on the role of CBOs and how they can integrate violence prevention into their work will would contribute to current global efforts to develop community-based parenting interventions.
Limitations
The design of this study is subject to some limitations. First, it is a cross-sectional study, and thus it is not possible to attribute causality of child mental health outcomes to exposure to different types of violence. In addition, while efforts were made to ensure systematic sampling of participants for enrolment in the study, participants were recruited on a consecutive basis from CBOs and thus generalizability of the findings may be limited beyond this population. There is no comparison group in this study and all participants were in receipt of a community-based programme. Finally, violence exposure measures were based on child and carer report. Previous studies from high-income settings have indicated that reporting of corporal punishment may vary according to informant (Schneider, Mackenzie, Waldfogel, & Brooks-Gunn, Citation2014).
Conclusion
Many risk factors for violence against children are particularly prevalent in HIV/AIDS-affected families and communities. Violence in the home is associated with a range of negative mental health outcomes for children. It is possible that participation in community-based programmes mitigates the impact of violence exposure over time. Community-based organisations who are working to improve psychosocial outcomes for vulnerable children affected by HIV/AIDS should integrate violence prevention programming into their work.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Abrahams, N., Jewkes, R., Laubscher, R., & Hoffman, M. (2006). Intimate partner violence: Prevalence and risk factors for men in Cape Town, South Africa. Violence and Victims, 21(2), 247–264. doi: 10.1891/vivi.21.2.247
- Betancourt, T. S., Meyers-Ohki, S. E., Charrow, A., & Hansen, N. (2013). Annual research review: Mental health and resilience in HIV/AIDS-affected children – A review of the literature and recommendations for future research. Journal of Child Psychology and Psychiatry, 54, 423–444. doi: 10.1111/j.1469-7610.2012.02613.x
- Bisika, T., Ntata, P., & Konyani, S. (2009). Gender-violence and education in Malawi: A study of violence against girls as an obstruction to universal primary school education. Journal of Gender Studies, 18(3), 199–306. doi:10.1080/09589230903057183
- Bower, C., & Dawes, A. (2014). Young children: Preventing physical abuse and corporal punishment. In S. Mathews, L. Jamieson, L. Lake, & C. Smith (Eds.), South African Child Gauge 2014: End the cycle of violence (pp. 58–64). Cape Town: Children's Institute, University of Cape Town.
- Boyes, M. E., & Cluver, L. D. (2015). Relationships between familial HIV/AIDS and symptoms of anxiety and depression: The mediating effect of bullying victimization in a prospective sample of South African children and adolescents. Journal of Youth and Adolescence, 44, 847–859. doi: 10.1007/s10964-014-0146-3
- Boyes, M. E., Mason, S. J., & Cluver, L. D. (2013). Validation of a brief stigma-by-association scale for use with HIV/AIDS-affected youth in South Africa. AIDS Care, 25, 215–222. doi: 10.1080/09540121.2012.699668
- Briere, J. (1996). Professional manual for the Trauma Symptom Checklist for Children (TSCC). Odessa, FL: Psychological Assessment Resources.
- Chaux, E., Molano, A., & Podlesky, P. (2009). Socio-economic, socio-political and socio-emotional variables explaining school bullying: A country-wide multilevel analysis. Aggressive Behavior, 35, 520–529. doi: 10.1002/ab.20320
- Cluver, L., Gardner, F., & Operario, D. (2007). Psychological distress amongst AIDS-orphaned children in urban South Africa. Journal of Child Psychology and Psychiatry, 48(8), 755–763. doi: 10.1111/j.1469-7610.2007.01757.x
- Crijnen, A. A. M., Achenbach, T. M., & Verhulst, F. C. (2014). Problems reported by parents of children in multiple cultures: The Child Behavior Checklist syndrome constructs. American Journal of Psychiatry, 156(4), 569–574.
- Devries, K. M., Kyegombe, N., Zuurmond, M., Parkes, J., Child, J. C., Walakira, E. J., & Naker, D. (2014). Violence against primary school children with disabilities in Uganda: A cross-sectional study. BMC Public Health, 14, 1017. doi: 10.1186/1471-2458-14-1017
- Dubowitz, H., & Bennett, S. (2007). Physical abuse and neglect of children. Lancet, 369, 1891–1899. doi: 10.1016/S0140-6736(07)60856-3
- Du Plessis, B., Kaminer, D., Hardy, A., & Benjamin, A. (2015). The contribution of different forms of violence exposure to internalizing and externalizing symptoms among young South African adolescents. Child Abuse Neglect, 45, 80–89. doi: 10.1016/j.chiabu.2015.02.021
- Fleming, L. C., & Jacobsen, K. H. (2010). Bullying among middle-school students in low and middle income countries. Health Promotion International, 25(1), 73–84. doi: 10.1093/heapro/dap046
- Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x
- Huesman, L. R. (2011). The contagion of violence: The extent, the processes, and the outcomes. Washington, DC: National Academies of Sciences’ Institute of Medicine.
- IBM Corp. (2012). IBM SPSS statistics for windows (Version 20.0). Chicago, IL: Author.
- Jewkes, R. K., Dunkle, K., Nduna, M., & Shai, N. (2010). Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: A cohort study. The Lancet, 376, 41–48. doi: 10.1016/S0140-6736(10)60548-X
- Kovacs, M. (1992). Children's depression inventory. Niagara Falls, NY: Multi-Health Systems.
- Li, X., Fang, X., Stanton, B., Zhao, G., Lin, X., Zhao, J., … Chen, X. (2009). Psychometric evaluation of the Trauma Symptoms Checklist for Children (TSCC) among children affected by HIV/AIDS in China. AIDS Care, 21(3), 261–270. doi: 10.1080/09540120802195119
- Mathews, S., & Benevenuti, P. (2014). Violence against children in South Africa: Developing a prevention agenda. In S. Mathews, L. Jamieson, L. Lake, & C. Smith (Eds.), South African Child Gauge 2014: End the cycle of violence (pp. 26–34). Cape Town: Children's Institute, University of Cape Town.
- Mejia, A., Calam, R., & Sanders, M. R. (2012). A review of parenting programs in developing countries: Opportunities and challenges for preventing emotional and behavioral difficulties in children. Clinical Child and Family Psychology Review, 15, 163–175. doi: 10.1007/s10567-012-0116-9
- Mills, R., Alati, R., O'Callaghan, M., Najman, J. M., Williams, G. M., Bor, W., & Strathearn, L. (2011). Child abuse and neglect and cognitive function at 14 years of age: Findings from a birth cohort. Pediatrics, 127(1), 4–10. doi: 10.1542/peds.2009-3479
- Mock, C., Peden, M., Hyder, A. A., Butchart, A., & Krug, E. (2008). Child injuries and violence: The new challenge for child health. Bulletin of the World Health Organization, 2008, 420. doi: 10.2471/BLT.08.054767
- Mueller, J., Alie, C., Jonas, B., Brown, E., & Sherr, L. (2011). A quasi-experimental evaluation of a community-based art therapy intervention exploring the psychosocial health of children affected by HIV in South Africa. Tropical Medicine & International Health, 16, 57–66. doi: 10.1111/j.1365-3156.2010.02682.x
- Niclasen, J., Teasdale, T. W., Andersen, A. M., Skovgaard, A. M., Elberling, H., & Obel, C. (2012). Psychometric properties of the Danish strength and difficulties questionnaire: The SDQ assessed for more than 70,000 raters in four different cohorts. PLoS One, 7(2), e3205. doi: 10.1371/journal.pone.0032025
- Norman, R., Matzopoulos, R., Groenewald, P., & Bradshaw, D. (2007). The high burden of injuries in South Africa. Bulletin of the World Health Organization, 85(9), 649–732. doi: 10.2471/BLT.06.037184
- Norman, R. E., Byambaa, M., De, R., Butchart, A., Scott, J., & Vos, T. (2012). The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Med, 9(11), e1001349. doi: 10.1371/journal.pmed.1001349
- Renner, L. M., & Slack, K. S. (2006). Intimate partner violence and child maltreatment: Understanding intra- and intergenerational connections. Child Abuse Neglect, 30(6), 599–617. doi: 10.1016/j.chiabu.2005.12.005
- Richter, L., & Dawes, A. (2008). Child abuse in South Africa: Rights and wrongs. Child Abuse Review, 17, 79–93. doi: 10.1002/car.1004
- Richter, L., Komarek, A., Desmond, C., Celentano, D., Morin, S., Sweat, M., … Coates, T. (2014). Reported physical and sexual abuse in childhood and adult HIV risk behaviour in three African countries: Findings from Project Accept (HPTN-043). AIDS and Behavior, 18, 381–389. doi: 10.1007/s10461-013-0439-7
- Rico, E., Fenn, B., Abramsky, T., & Watts, C. (2011). Associations between maternal experiences of intimate partner violence and child nutrition and mortality: Findings from demographic and health surveys in Egypt, Honduras, Kenya, Malawi and Rwanda. Journal of Epidemiology and Community Health, 65(4), 360–367. doi: 10.1136/jech.2008.081810
- Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press.
- Schmitt, D. P., & Allik, J. (2005). Simultaneous administration of the Rosenberg Self-Esteem Scale in 53 nations: Exploring the universal and culture-specific features of global self-esteem. Journal of Personality and Social Psychology, 89(4), 623–642. doi: 10.1037/0022-3514.89.4.623
- Schneider, M., Chersich, M., Neuman, M., & Parry, C. (2012). Alcohol consumption and HIV/AIDS: The neglected interface. Addiction, 107, 1369–1371. doi: 10.1111/j.1360-0443.2012.03824.x
- Schneider, W., Mackenzie, M., Waldfogel, J., & Brooks-Gunn, J. (2014). Parent and child reporting of corporal punishment: New evidence from the fragile families and child wellbeing study. Child Indicators Research, 8(2), 347–358. doi: 10.1007/s12187-014-9258-2
- Seedat, M., Van Niekerk, A., Jewkes, R., Suffla, S., & Ratele, K. (2009). Violence and injuries in South Africa: Prioritising an agenda for prevention. The Lancet, 374, 1011–1022. doi: 10.1016/S0140-6736(09)60948-X
- Seedat, S., Nyamai, C., Njenga, F., Vythilingum, B., & Stein, D. J. (2004). Trauma exposure and post-traumatic stress symptoms in urban African schools. The British Journal of Psychiatry, 184(2), 169–175. doi: 10.1192/bjp.184.2.169
- Seeley, J., Watts, C. H., Kippax, S., Russell, S., Heise, L., & Whiteside, A. (2012). Addressing the structural drivers of HIV: A luxury or necessity for programmes? Journal of the International AIDS Society, 15(Supp1 l), 1–4.
- Sherr, L., Hensels, I. S., Skeen, S., Tomlinson, M., Roberts, K. J., & Macedo, A. (2016). Exposure to violence predicts poor educational outcomes in young children in South Africa and Malawi. International Health, 8(1), 36–43. doi:10.1093/inthealth/ihv070
- Sherr, L., Yakubovich, A. R., Skeen, S., Cluver, L. D., Hensels, I. S., Macedo, A., & Tomlinson, M. (in press). How effective is help on the doorstep? A longitudinal evaluation of community-based organisation support. PLoS One. doi:10.1371/journal.pone.0151305
- Skeen, S., Tomlinson, M., Ward, C. L., Cluver, L., & Lachman, J. M. (2015). Early intervention: A foundation for lifelong violence prevention. South African Crime Quarterly, 51, 5–8. doi: 10.4314/sacq.v51i0.1
- Snider, L. M., & Dawes, A. (2006). Psychosocial vulnerability and resilience measures for national-level monitoring of orphans and other vulnerable children: Recommendations for revision of the UNICEF psychological indicator. Retrieved from http://www.childinfo.org/files/PsychosocialMeasures_Final06.pdf
- Straus, M., Hamby, S. L., Finkelhor, D., Moore, D. W., Runyan, D. (1998). Identification of child maltreatment with the parent-child conflict tactics scales: Development and psychometric data for a national sample of American parents. Child Abuse & Neglect, 22(4), 249–270. doi: 10.1016/S0145-2134(97)00174-9
- Suliman, S., Mkabile, S. G., Fincham, D. S., Ahmed, R., Stein, D. J., & Seedat, S. (2009). Cumulative effect of multiple trauma on symptoms of posttraumatic stress disorder, anxiety, and depression in adolescents. Comprehensive Psychiatry, 50(1), 121–127. doi: 10.1016/j.comppsych.2008.06.006
- Tomlinson, M., Solomon, W., Singh, Y., Doherty, T., Chopra, M., Ijumba, P., … Jackson, D. (2009). The use of mobile phones as a data collection tool: A report from a household survey in South Africa. BMC Medical Informatics and Decision Making, 9, 51. doi: 10.1186/1472-6947-9-51
- UNICEF. (2014). Hidden in plain sight: A statistical analysis of violence against children. New York, NY: Author.
- United Nations. (2006). United Nations Secretary-General's study on violence against children. New York, NY: Author.
- Ward, C. L., Artz, L., Berg, J., Boonzaier, F., Crawford-Browne, S., Dawes, A., … Van Der Spuy, E. (2012). Violence, violence prevention, and safety: A research agenda for South Africa. South African Medical Journal, 102, 215–218.
- World Health Organization. (2002). World report on violence and health. Geneva: Author.
- World Health Organization. (2006). Preventing child maltreatment: A guide to taking action and generating evidence. Geneva: Author.
- World Health Organization. (2014). Global status report on violence prevention 2014. Geneva: Author.
- Yakubovich, A. R., Sherr, L., Cluver, L. D., Skeen, S., Hensels, I. S., Macedo, A., & Tomlinson, M. (2016). Community-based organisations for vulnerable children in South Africa: Reach, psychosocial correlates, and potential mechanisms. Children and Youth Services Review, 62, 58–64. doi: 10.1016/j.childyouth.2016.01.016
