
ABSTRACT
A stubborn health challenge for learners in South African public schools concerns sexual and reproductive health and rights (SRHR). In 2015, the Department of Basic Education (DBE) proposed the provision of condoms and SRHR-services to learners in schools. This study aimed to contribute to the finalisation and implementation of DBE’s policy by exploring learners’ perspectives on the provision of condoms and SRHR-services in schools. Sixteen focus group discussions were conducted with learners (n = 116) from 33 public schools, to assess their attitudes, social influences, and needs and desires regarding condom provision and SRHR-services in schools. The majority of learners did not support condom provision in schools as they feared that it may increase sexual activity. Contrarily, they supported the provision of other SRHR-services as clinics fail to offer youth-friendly services. Learners’ sexual behaviour and access to SRHR-services are strongly determined by their social environment, including traditional norms and values, and social-pressure from peers and adults. Learners’ most pressing needs and desires to access condoms and SRHR-services in school concerned respect, privacy and confidentiality of such service provision. Implementation of DBE’s policy must be preceded by an evidence-informed advocacy campaign to debunk myths about the risk of increased sexual activity, to advocate for why such services are needed, to shift societal norms towards open discussion of adolescent SRHR and to grapple with the juxtaposition of being legally empowered but socially inhibited to protect oneself from HIV, STIs and early pregnancy. Provision of condoms and other SRHR-services in schools must be sensitive to learners’ privacy and confidentiality to minimise stigma and discrimination.
Introduction
A stubborn health-related challenge for learners in South African public schools remains sexual and reproductive health and rights (SRHR) (DBE, Citation2015a). Despite the introduction of sexuality education in schools 17 years ago, high levels of sexual risk behaviour are reported (Reddy et al., Citation2013). The Department of Basic Education’s (DBE) 2015 Draft National Policy on HIV, STIs and TB departs from the 1999 policy by proposing the provision of SRHR-services including condoms to learners in school (DBE, Citation2015b).
Announcement of the draft policy raised public concerns about increased sexual activity and early sexual debut (Han & Bennish, Citation2009), learners’ psychosocial wellbeing and conflicting personal, religious and cultural views (Gwandure, Ross, & Gardner, Citation2014; Alli, Maharaj, & Vawda, Citation2013; Francis & DePalma, Citation2014). This study aimed to inform the draft policy by exploring learners’ perspectives on SRHR-service provision in schools.
Methods
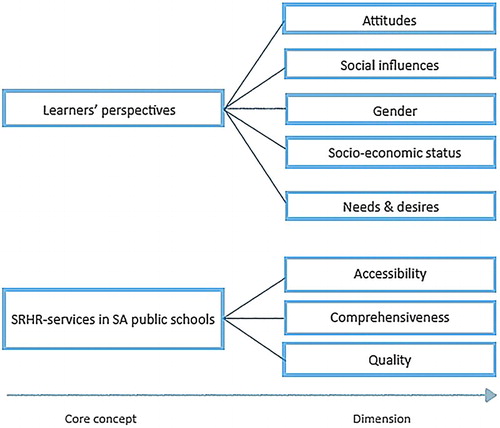
Focus group discussions (FGDs) were conducted with secondary school learners (aged ≥12 years) to explore their perspectives on access to condoms and other SRHR-services in schools based on the core concepts and dimensions of this study ().
Figure 1. Core concepts and dimensions used to conceptualize this study.
Schools and learners were recruited through UNICEF’s existing programmes from all nine provinces, both urban and rural areas and the five poverty quintiles (Q1-Q3: no-fee paying schools). Learner selection was stratified by sex due to the gender-sensitive nature of SRHR-topics (Bliesner, Rolleri, Moore, & Gavin, Citation2007).
Institutional approval was obtained in writing from district offices and schools. Written consent was obtained from all participants; they were not compensated for participation.
Discussions were conducted in English as the medium of instruction in secondary schools. All FGDs were recorded, transcribed verbatim, and thematically analysed using a coding-scheme as per . Codes were added as new themes emerged (e.g., abortion, social media and taboos). Search functions and visual aids of Nvivo software were used to analyse data, identify themes and structure the results. Saturation was reached by focus group eight, with the remaining focus groups confirming earlier findings.
Study limitations include that the sample cannot be considered representative given its qualitative nature; discussions were held on provision of condoms in general and not differentiated by male and female condoms; and learners were recruited at a UNICEF event, hence number of learners approached were not recorded.
Results
Sixteen FGDs were conducted amongst 116 learners (female n = 61; average age = 17 years) representing 33 schools (Q1-Q5) from all provinces. Although three FGDs comprised mixed gender groups, participants expressed comfort with the other gender’s presence.
Attitudes towards SRHR-services
The majority of learners reported a negative attitude towards condom provision in schools, due to fears that it would increase sexual activity and harm academic performance.
“Well with the condoms in schools, the teenagers will think about sex … Yes it is wrong, because they will do it every weekend, even in school they will do it, they won’t focus on schoolwork, they will focus on having sex.” – Male learner, Free State
Some learners shifted their opinion on condom provision during the discussion when they received additional information through the FGD. They also considered condoms important for other learners but not for themselves.
Attitudes towards provision of other SRHR-services (e.g., HIV testing and provision of contraceptives) in schools were positive, particularly amongst female learners, as SRHR-service providers are not easily accessible and are not youth-friendly. Many learners were concerned about gossip and privacy if SRHR-services would became available at school.
Social influences on accessing SRHR-services
Learners’ perspectives on accessing SRHR-services were strongly determined by their social environment. Learners clarified that parents, teachers and other adults maintain conservative norms and values whereas their generation is experiencing a shift towards more progressive and open-minded norms and values. They acknowledged that many adolescents are sexually active and accordingly have needs and rights.
Female learners argued that sexual activity amongst girls is frowned upon, but more socially acceptable and discussed openly amongst boys. Consequently, girls felt that boys can more easily obtain information on SRHR. Female learners also indicated that nurses disrespected them at clinics, and that they are punished or “kicked out of the house” when they are seen at SRHR-clinics.
Findings also revealed social modeling and -pressure regarding SRHR-services. Health seeking behaviour for both access to information and services, seems to be shaped by the behaviour and (perceived) expectations of significant others. Learners were concerned about what friends and classmates think:
“They think that you will take the condoms because you are going to use them. So they think you will have sex. Whereas maybe you are not going to, maybe you just take one because you might not know when that (i.e., sex) is going to happen” –Male learner, North West
Needs and desires regarding SRHR-services
The majority of participants expressed a desire for privacy regarding access to condoms. Some suggested that condoms should be made available in the toilets; others recommended controlled access via school staff. Learners repeatedly emphasised that condoms provided should not only be government-issued due to quality concerns (e.g., easy rupture), although this was based on the condoms’ poor image rather than personal experience.
Regarding SRHR-services, learners indicated that they desire respectful treatment, privacy and confidentiality. They recommended a comprehensive SRHR-service package including provision of contraceptives, HIV-, STI-, and pregnancy testing and treatment with counseling emphasised as the most important component:
“[ … ] If there is someone like a counsellor, who you can speak to, I think that will help a lot for many girls. Because there is not many kids who have a relationship with their parents that they talk about this. But when it is a stranger who is not going to judge you, and it is confidential and all, it will be easier to talk.” – Female learner, Northern Cape
Discussion and conclusion
On the one hand, learners rejected condom provision in schools because of fear that it might increase sexual activity. On the other, they supported the provision of other SRHR-services because clinics fail to offer youth-friendly services. As the FGDs ensued, some learners shifted their perspective on condom provision based on the lived reality of their peers.
Studies show that sexuality education (Paul-Ebhohimhen, Poobalan, & Van Teijlingen, Citation2008; Alford, Citation2012) and condom availability (Blake et al., Citation2003) in schools do not increase sexual activity. This is reflected in the SA Children’s Act of Citation2005 that foregrounds the right of children from 12 years of age to access and use contraceptives without parental consent. The introduction of condoms in schools must be preceded by a strong advocacy campaign that debunks myths about the availability of condoms in schools and offers the rationale for its provision; that locates condoms within the wider basket of SRHR-services (as opposed to a stand-alone intervention); and that contextualises individual needs and desires within a broader social context. These are inherent goals of DBE’s Draft Policy and the school curriculum but implementation remains sub-optimal.
Learners reported that access to SRHR-services are compromised by the continued value-laden judgements and stigmatisation by gatekeepers namely educators, health workers and parents, especially for girls (Alli et al., Citation2013; Francis & DePalma, Citation2014; Gwandure et al., Citation2014) and subsequently replicated by peers. Consequently, learners regarded respect, privacy and confidentiality as prerequisites for the provision of condoms and SRHR-services in schools. These needs and desires are important features of DBE’s Draft Policy.
In 2016, the Council of Education Ministers adopted the DBE National Policy on HIV, STIs and TB. As the Department plans for implementation, cognisance must be given to the fact that SRHR-services in schools remains a highly emotive issue that clashes with religious, cultural and traditional norms and values entrenched in society (Han & Bennish, Citation2009). To gain social traction for the provision of such services to youth, a systematic campaign is required to shifts societal norms on adolescent sexuality, in particular for girls, and that tackles the juxtaposition of being legally empowered but socially inhibited to protect oneself against HIV, STIs and early pregnancy.
The provision of SRHR-services in schools is ground-breaking, not only in so far as it reduces negative reproductive health and education outcomes for SA learners, but also for youth across the region. Although sexuality education is featured across the region (Paul-Ebhohimhen et al., Citation2008), none of these countries include the provision of condoms or SRHR-services on the school premises. Success of the intervention in SA could pave the way for more progressive SRHR for young people across the region.
Acknowledgement
We would like to thank UNICEF South Africa for funding this research, as well as all learners who participated in the focus group discussions.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Alford, S. (2012). Sex education and other programs that work to prevent teen pregnancy, HIV, and sexually transmitted infections science and successes (Vol. 3). Washington: Advocates for Youth. Retrieved from http://www.advocatesforyouth.org/storage/advfy/documents/sciencesuccess.pdf
- Alli, F., Maharaj, P., & Vawda, M. Y. (2013). Interpersonal relations between health care workers and young clients: Barriers to accessing sexual and reproductive health care. Journal of Community Health, 38(1), 150–155. doi: 10.1007/s10900-012-9595-3
- Blake, S. M., Ledsky, R., Goodenow, C., Sawyer, R., Lohrmann, D., & Windsor, R. (2003). Condom availability programs in Massachusetts high schools: Relationships with condom use and sexual behavior. American Journal of Public Health, 93(6), 955–962. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1447877/pdf/0930955.pdf. doi: 10.2105/AJPH.93.6.955
- Bliesner, M. L., Rolleri, L. A., Moore, C., & Gavin, L. (2007). Collecting qualitative data on youth perceptions regarding teen pregnancy and HIV prevention: A focus group guide. Scotts Valley, CA. Retrieved from http://www.massteenpregnancy.org/sites/default/files/providers/etr-focus-group-guide.pdf
- DBE. (2015a). Action plan to 2019: Towards the realisation of schooling 2030. Pretoria: Department of Basic Education. Retrieved from http://www.education.gov.za/Portals/0/Documents/Publications/Action%20Plan%202019.pdf?ver=2015-11-11-162424-417
- DBE. (2015b). Draft department of basic education national policy on HIV, STIs and TB (pp. Government gazette 395). Pretoria: Author. Retrieved from http://www.education.gov.za/Portals/0/Documents/Legislation/Call%20for%20Comments/DBE%20General%20Notice%20HIV%20Policy%205%20May%202015.pdf?ver=2015-05-11-090105-123
- Francis, D., & DePalma, R. (2014). Teacher perspectives on abstinence and safe sex education in South Africa. Sex Education, 14, 81–94. doi: 10.1080/14681811.2013.833091
- Gwandure, R., Ross, E., & Gardner, J. (2014). Parents’ perceptions of HIV counselling and testing in schools: Ethical, legal and social implications. Southern African Medical Journal, 104, 40–42. doi: 10.7196/samj.6645
- Han, J., & Bennish, M. L. (2009). Condom access in South African schools: Law, policy, and practice. PLoS Medicine, 6, e1000006. doi: 10.1371/journal.pmed.1000006
- Paul-Ebhohimhen, V. A., Poobalan, A., & Van Teijlingen, E. R. (2008). A systematic review of school-based sexual health interventions to prevent STI/HIV in Sub-saharan Africa. BMC Public Health, 8(1), 105. doi: 10.1186/1471-2458-8-4
- Reddy, P., James, S., Sifunda, R. S., Ellahebokus, A., Kambaran, N. S., & Omardien, R. G. (2013). Umthente uhlaba usamila - The 3rd South African national youth risk behaviour survey 2011. Cape Town: Human Sciences Research Council.
- SA Children’s Act. (2005). Children’s Act 38 S.134 (pp. Government gazette). Pretoria: The parliament of the Republic of South Africa. Retrieved from http://www.justice.gov.za/legislation/acts/2005-038%20childrensact.pdf
