
ABSTRACT
Retention rates in antiretroviral treatment (ART) in low- and middle-income countries are suboptimal for meeting global "90-90-90" treatment targets. Interventions using routinely collected patient data to follow up with ART defaulters is recommended to improve retention; yet, little is documented on how these data are used in practice. This state of the evidence review summarizes how facilities and programmes use patient data to retain adults on ART in low- and middle-income countries, and what effect, if any, these interventions have on retention. The authors searched peer-reviewed and grey literature in PubMed, POPLINE, OVID, Google Scholar, and select webpages; screened publications for relevance; and applied eligibility criteria to select articles for inclusion. Over 4,000 records were found, of which 19 were eligible. Interventions assessed within the studies were sorted into three categories: patient tracing (18), data reviews (3), and improved data capture systems (9). Nine studies demonstrated increased retention or reduced lost to follow-up; however, the quality of evidence was weak. We recommend that future research investigates how various combinations of these interventions are being implemented and their effectiveness on ART retention across diverse country contexts, taking into account cultural, social and economic barriers and differences in countries' HIV epidemics and health information systems.
Introduction
The global HIV community released a series of ambitious goals and new treatment guidelines in the past few years that highlight the significance of starting people living with HIV (PLHIV) on treatment, and keeping them on treatment. The Joint United Nations Programme on HIV/AIDS (UNAIDS) introduced in October 2014 their “90-90-90” initiative, which calls for achievement of the following goals by 2020: 90% of PLHIV to be diagnosed; 90% of those diagnosed to be on antiretroviral treatment (ART); and 90% of those on ART to be virally suppressed (“UNAIDS”, Citation2014). The World Health Organization (WHO) released new treatment guidelines in September 2015, which recommend treating all PLHIV – at any age and at any CD4 count (“WHO”, Citation2015). Finally, the President’s Emergency Plan for AIDS Relief (PEPFAR) 3.0 plan is also seeking to aggressively increase treatment, with the goal of supporting 18.5 million women, men, and children on ART by 2017 (Vidanapathirana, Premadasa, Disanayake, Wijegoonewardene, & Mallikarachchi, Citation2016).
With this push to scale up ART, implementers and policymakers must think realistically about how to retain patients on treatment, especially in low- and middle-income countries where ART retention may be suboptimal. Definitions of ART retention vary, but retention indicators tend to measure the number or frequency of visits within a proscribed period of time. For instance, the U.S. Institute of Medicine defines retention as two attended visits separated by at least 90 days during a 12-month period (Mugavero et al., Citation2012). A systematic review of retention on ART in sub-Saharan Africa defined retention as the opposite of attrition; meaning anyone who has not died or has not been lost to follow-up (LTFU) is considered retained on treatment (Fox & Rosen, Citation2010).
Retention in ART is a great challenge for health systems, particularly in developing countries. Inadequate retention and adherence to ART results in poor health outcomes, including morbidity, mortality, drug resistance, and increased risk of transmission. It also results in the inefficient use of scarce available resources for treatment (Stricker et al., Citation2014). There are health-related, cultural and social factors which inhibit patients who initiate ART (or treatment for other infectious diseases, such as tuberculosis) in low resource settings from returning to a health facility for care. These include advanced illness and death, long distances and high associated costs of travelling to health facilities, stigma in receiving treatment, poor health service delivery (i.e., long waiting times; medicine stock outs; poor quality of care by health facility staff), a self-perceived improvement on treatment, alternative health beliefs and psychological factors including depression (“WHO”, Citation2011). There are also record-keeping-related constraints to patients’ retention in care. Specifically, after death, the most commonly cited reason for LTFU is transfer to another health facility (Dalal et al., Citation2008; Karcher, Omondi, Odera, Kunz, & Harms, Citation2007; Lawn et al., Citation2006; Yu et al., Citation2007).
Fox & Rosen, Citation2010 paper reviewed articles published between 2007 and 2009 and estimated that in sub-Saharan Africa, 24-month retention was 70% (range: 66.7%–73.3%), while 36-month retention was just 64.6% (range: 57.5%–72.1%) (Fox & Rosen, Citation2010). Although these retention rates are higher than estimates from an earlier systematic review for the region (Rosen, Fox, & Gill, Citation2007), they indicate that substantial efforts must be made to reach the global targets on HIV treatment that will change the course of the epidemic – particularly ensuring that in the next three years 90% of those on ART are virally suppressed.
There are many studies that retrospectively analyse routinely collected data to assess retention at a particular health facility or at several health facilities. Based on a review of records for specific patient cohorts, these studies often recommend better record-keeping and tracing of patients who have defaulted (e.g., discontinued treatment) or been LTFU (e.g., not actively enrolled in care) (Dalal et al., Citation2008; Forster et al., Citation2008; McMahon et al., Citation2015; Scheibe et al., Citation2013).
For instance, Forster, et al. found a correlation between fewer missing data in electronic medical records and fewer losses to follow-up for ART, suggesting that better databases might contribute to ART retention (Forster et al., Citation2008). However, few studies examine how clinicians and community health workers actively use routinely-collected patient data to increase ART retention, and we have found no state of the evidence or systematic reviews to date on this topic (Fraser et al., Citation2007).
As such, the aim of this paper is to report the results of our state of the evidence review of published peer-reviewed and grey literature on how routinely collected patient data are used to retain adults on ART in low- and middle-income countries, with the objective of supporting policymakers and programme managers with documented, practical approaches, which they can adapt to their context and apply in low resource settings. We recognize that there are myriad other techniques to increasing ART retention through addressing the economic, social, behavioural and cultural factors that determine patient retention; however that is not the focus of this paper.
This study analyses adult patients who receive ART and default or who are lost to follow-up. We excluded articles focusing on pre-ART retention, because of the unique nature of retention at this stage in a patient’s treatment; as well as publications that focus exclusively on pregnant women and children, because the services they receive differ from those of other adults and therefore should also be examined separately.
Methods
Search strategy
In January and February of 2016, we systematically reviewed both peer-reviewed and grey literature. Four databases – PubMed, POPLINE, OVID, and Google Scholar – were used to search for this material. Additional grey literature was identified by searching 15 relevant websites, as well as abstracts from the International AIDS Conferences, starting in 2010. Following peer review, we identified literature published in 2017, after our initial search, to include in the study. We used Google Scholar and the same search strategy to identify these supplementary resources.
Key words for the searches were based on two general categories: routinely-collected patient data and ART retention. Synonyms, such as “records” or “files” in place of “data,” and similar concepts, such as “adherence” in place of “retention,” were used as key words. The investigators used Boolean operator syntax, including “and” and “or” commands, to conduct multiple key word searches in databases. Some targeted websites for grey literature searches did not have a key word search function; therefore, hand searches through relevant sections of the website were conducted. Search terms and search method, number of results reviewed, and number of results deemed relevant were recorded in an Excel spreadsheet. Database search results were stored in EndNote.
Study selection
Two investigators independently screened the titles and abstracts of all search results for relevance. All studies and texts, regardless of method used, were eligible for inclusion so as to collect the greatest number of items on the research topic. All texts deemed irrelevant by both investigators and all duplicates were removed. Full-text articles were retrieved for the remaining relevant abstracts. Two investigators independently reviewed the full text of each relevant article and assessed its eligibility based on the following criteria:
Publication must be in English;
Publication must be published in 2004 or later (2004 marked the start of ART delivery at scale in low- and middle-income countries) (Govindasamy et al., Citation2014);
Publication must have been conducted in a low- or middle-income country, as determined by World Bank income classifications;
Publication must examine adult (not prevention of mother-to-child transmission of HIV and non-pediatric) ART retention for patients already on ART (not pre-ART);
Publication must describe actual rather than hypothetical or recommended use of routinely collected patient data to improve adult ART retention.
The investigators discussed cases on which they disagreed and an ultimate determination of eligibility was made jointly. The investigators applied PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) to document all steps in the search and selection process and standardize the way that results were recorded.
Data extraction
From each article selected as eligible, the investigators extracted information on the study’s method and location, the intervention being assessed, and the relationship between an intervention and ART retention. During our analysis, we classified the types of interventions described into three main categories: patient tracing, data reviews, and improved data capture systems. These categories were determined after studies were selected for inclusion.
It is also important to note that there are publications related to patient tracing that were excluded from this systematic review due to insufficient information in the article on how routine data is used to inform patient tracing (Krebs et al., Citation2008; Yu et al., Citation2007).
Results
Our initial search strategy identified 4,682 records (). Database searches found 947 studies, while other grey literature searches yielded 3,735 records. Of the 4,682 records found, 651 were removed as duplicates, leaving 4,031 records to be screened for relevance. The investigators excluded 3,910 during the relevance screening, yielding 121 full-text articles to be assessed for eligibility. Of those assessed, 105 of those articles were excluded by the investigators because they did not meet all of the eligibility criteria (described above), leaving 16 publications eligible for the analysis. Following peer review, we identified an additional three publications that met the study’s eligibility criteria that were published in 2017. As a result, 19 publications were analysed in total. Five of these publications are peer-reviewed journal articles (Errol et al., Citation2012; Gilvydis et al., Citation2015; Nglazi, Kaplan, Wood, Bekker, & Lawn, Citation2010; Ramdas, Meyer, & Cameron, Citation2015; Tweya et al., Citation2010), six are abstracts and posters from an International AIDS Conference (Fox et al., Citation2017; Kitsao, Kimani, Muriuki, & Akolo, Citation2017; Mganga et al., Citation2014; Mugisa, Mugume, Odong, & Ndagire, Citation2014; Odhiambo et al., Citation2014; Wandina et al., Citation2011), four are reports (do Nascimento & Joao, Citation2013; do Nascimento et al., Citation2014; Vella, Govender, & Scelo, Citation2008; “South African National”, Citation2010), two are theses (Naidoo, Citation2006; Ncholo, Citation2010), one (Chantal, Citation2011) is a document recording an online discussion, and one is a blog post (Tjaronda, Mwinga, Kagoya, & Mazibuko, Citation2017) ().
Figure 1. Summary of articles eligible for and included in the systematic review.
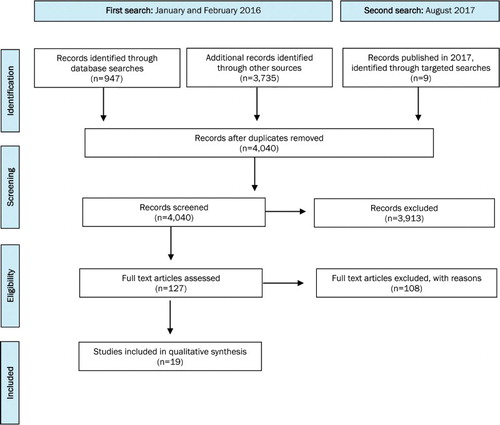
Table 1. Summary of body of evidence.
Most of the selected publications (17 of the 19) were published in 2010 or later. All but one of the 19 publications described interventions that took place in sub-Saharan Africa. The country featured most often was South Africa (eight publications), followed by Kenya (three publications) and Mozambique (two publications). The other studies described interventions in Tanzania, Rwanda, Uganda, Malawi, Namibia, and India.
The authors organized the publications in three non-mutually exclusive categories based on the approaches employed to improve patient retention described in each. The results presented below are divided into these three categories (patient tracing, data review, and improved data capture systems). Since many of the publications described strategies that used two or more of the intervention categories, they should not be seen as stand-alone approaches.
Improved data capture systems
Nine of the nineteen studies described ways in which health facilities improved current routine data collection systems to enhance retention in care – an intervention we call “improved data capture systems” (). For example, a report in South Africa explained that the introduction of a longitudinal ART patient record system enabled the clinical team to review patient records and easily follow up with patients, because all of the information required was located in one register with the “due back” date at the health facility clearly marked: “Every month at treatment collection date, a mark is entered in the correct month column (…). In this way, it is easy to get a quick monthly overview of the names of clients who have not collected treatment” (“South African National”, Citation2010).
Other approaches included using a patient appointment tracking book (Mugisa et al., Citation2014), introduction of electronic patient monitoring systems that alert staff to patients who are LTFU (Chantal, Citation2011; Kitsao et al., Citation2017; Tjaronda et al., Citation2017; Tweya et al., Citation2010), and an electronic pharmacy tracking system that sends an alert when patients do not pick up their medicines within a predefined period (Nglazi et al., Citation2010). One study in South Africa also mapped the flow of data across all paper-based and electronic systems in 24 clinics to analyse how to improve efficiency in data capture, including how different systems interact with one another (Fox et al., Citation2017).
Data reviews
Data review is another approach cited in the literature as a means of increasing retention in care for ART patients. This approach involves reviewing health facility data on ART retention with clinic staff, community workers, and other appropriate parties with the goal of using the data to motivate improvements in ART retention rates using techniques already established or identifying new methods for reducing LTFU. Three of the nineteen studies cited data review as a means of improving retention, referring to it either as “data feedback” (Mganga et al., Citation2014) or “patient audit cycles” (Odhiambo et al., Citation2014; Wandina et al., Citation2011).
For example, Wandina, et al., describe the AIDSRelief programme in Kenya, which held patient care audit meetings with a multidisciplinary team at health facilities to identify areas of improvement in HIV care and strategize ways to close identified gaps. Based on these discussions, health facilities began ensuring that clinic diaries that tracked patient appointments were used and prompted follow-up for those who missed appointments in order to decrease LTFU (Wandina et al., Citation2011). Similarly, several years later the same programme published an abstract that documented processes in place for continuous review of patient care using the following quality improvement methods: review of chronic care support systems including clinic processes; assessment of patient outcomes; and strengthening the ability of health facilities to contact patients LTFU (Odhiambo et al., Citation2014).
Implementers in Tanzania used a similar method, in which summarized data on LTFU were presented in a table or figure format to local stakeholders to motivate improvements in patient retention (Mganga et al., Citation2014). The abstract did not document subsequent steps taken to improve retention.
Patient tracing
Every study except one discussed interventions pertaining to “patient tracing” to reduce LTFU (see ). Patient tracing is a strategy whereby health facility staff or community workers follow up with patients who do not appear at a health facility within a given timeframe and are therefore considered defaulted patients to determine why the patient is not reporting to the health facility as planned. Patient tracing is a common and recommended practice to identify patient outcomes (Geng et al., Citation2010). For patient tracing to be successful, patient registers must be of sufficient quality to show which patients need to be traced, and complete and up-to-date contact information is needed. Tracing modalities consisted of in-person visits to a patient’s home, phone calls, and short message service (SMS).
One example of patient tracing comes from Nhamatanda, Mozambique, where implementers made a concerted effort to better manage disorganized patient files at the health facility in order to ensure consistent and timely identification of defaulted patients. Patients who either missed pharmacy pick-ups or consultations were telephoned by the community worker or the community worker travelled to the patient’s neighbourhood and home to look for and counsel the patient to return to treatment – sometimes escorting them back to the health facility (do Nascimento & Joao, Citation2013; do Nascimento et al., Citation2014).
Effect on ART adherence
Nine of the nineteen studies provided some evidence that the interventions resulted in increased retention or reduced LTFU. However, the quality of the evidence was relatively weak. Seven of these studies compared retention or LTFU rates from before and after the intervention, but none of the studies accounted for other potential factors that could have contributed to changes in retention or LTFU rates. Further, all nine studies that described a relationship between the interventions and ART retention assessed pilot or small-scale programmes that were implemented in select facilities, resulting in small sample sizes. The effect of scaling up interventions nationwide on ART retention is unknown.
Discussion
Evidence from this review suggests that the use of routinely-collected patient data to increase ART retention has not been well-documented to date. Further, comparing the success of the three methods used to increase patient retention is difficult with the data currently available. Each study in our review used different measures and definitions (such as numbers on treatment, LTFU rates, or percentage of patients actively on treatment) to determine the success of an intervention. Standardizing definitions and measurements of ART retention and LTFU in future work documenting how routinely collected data are used to strengthen ART retention would improve our understanding of the effect of the interventions we discuss in this paper.
Additionally, more operations and quasi-experimental and experimental research in real world settings is needed to explore the effect of expanding interventions nationwide or combining multiple approaches to support ART retention. This larger pool of evidence could allow countries to experiment with and adapt evidence-informed retention techniques using routinely collected data to their contexts, and these could become part of national HIV/AIDS strategies and operational guidance, for instance on electronic patient monitoring systems, as discussed by Hochgesang et al., Citation2016. It should be coupled with approaches which address the unique cultural, social and economic barriers patients face to continue ART care, which, while not addressed in this paper, is key to reducing ART retention. Approaches should also be tailored to the type of HIV epidemic (generalized, concentrated, or mixed) that a country faces.
Several studies in our review indicate that routine patient data needs to be accurate and complete in order to effectively inform HIV retention interventions (e.g., do Nascimento & Joao, Citation2013; do Nascimento et al., Citation2014; Tjaronda et al., Citation2017). Improving the quality of data and data systems will be an important requirement to fully realize the potential of using available data to find and retain defaulted patients in treatment. This will require investments in human resources so that health facility staff and community health workers can effectively use data capture systems and newer technology, including electronic medical record systems and systems that link electronic databases and mobile phones (Hochgesang et al., Citation2016; Lambdin et al., Citation2012; “World Health”, Citation2006). It will also require improvements that are tailored to country health information system design – whether facility-based or patient-retained, stand-alone or integrated, paper-based or electronic, centralized or decentralized. Across these systems, the ability to link patients using unique patient identifiers will be critical to ensure patients are not LTFU when they transfer to a new health facility, and the data on retention is valid and reliable. Following a case based surveillance approach, an important component of the WHO’s HIV Second Generation Surveillance (WHO, Citation2013), would be a useful roadmap for implementers and ministries of health (see also Harklerode et al., Citation2017). Further, data collection systems should balance the need for monitoring multiple indicators with the labour intensity of collecting and recording that information (“World Health”, Citation2006), as well as consider the financial and other resource limitations that exist in low and middle income countries.
Conclusions
Despite the fact that the use of routinely-collected patient data to improve ART retention is a recommended best practice by the WHO to avoid mortality and other adverse outcomes (“World Health”, Citation2006), our state of the evidence review shows that there is limited evidence and research on this topic in low and middle income countries. Our review identified three types of interventions – improved data capture systems, data reviews and patient tracing – that use available data to improve ART retention. Going forward, we recommend the creation of a comprehensive research and policy agenda that investigates these interventions and various combinations of them across countries, recognizing the variations in social, cultural and economic factors at play across contexts, as well as the differences in health information system design and human resource capacity. Improving the quality of patient data and strengthening routine health information systems will continue to be essential to exploiting the full potential of facility data to increase ART retention.
Acknowledgements
We would like to thank Kay Wilson for her research support and Molly Cannon, Heidi Reynolds and Elizabeth Sutherland for their review of our paper.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Chantal, M. (2011). Data Use Net Discussion Series. UMUHOZA. Retrieved from http://www.cpc.unc.edu/measure/networks/datausenet/discussion-summary-facility-level-june-2011.doc
- Dalal, R. P., MacPhail, C., Mqhayi, M., Wing, J., Feldman, C., Cherisich, M. F., & Venter, W. D. (2008). Characteristics and outcomes of adult patients lost to follow-up at an antiretroviral treatment clinic in Johannesburg, South Africa. JAIDS Journal of Acquired Immune Deficiency Syndromes, 1, 101–107.
- do Nascimento, N., Cannon, M., Perales, N., Chariyeva, Z., Hagar, C., Kartzinel, H. … Schmid, C. (2014). Assessment of an mHealth initiative to improve patient retention. Information Development, 19(Suppl. 1), 1–8.
- do Nascimento, N., & Joao, F. D. (2013). Formative assessment of a future mHealth site in Nhamatanda Mozambique.
- Errol, L., Isaakidis, P., Zachariah, R., Ali, M., Pilankar, G., Maurya, S., … Reid, T. (2012). Tracing patients on antiretroviral treatment lost-to-follow-up in an urban slum in India. Journal of Advanced Nursing, 68(11), 2399–2409. doi: 10.1111/j.1365-2648.2011.05934.x
- Forster, M., Bailey, C., Brinkhof, M. W., Graber, C., Boulle, A., Spohr, M., … Egger, M. (2008). Electronic medical record systems, data quality and loss to follow-up: Survey of antiretroviral therapy programmes in resource-limited settings. Bulletin of the World Health Organization, 86(12), 939–947. doi: 10.2471/BLT.07.049908
- Fox, M., Pascoe, S., Huber, A., Murphy, J., Phokojoe, M., Gorgens, M., … Clouse, K. (2017, July). Implementation of interventions aimed at improving linkage, retention and adherence: Lessons learned from phase 1 of the roll out of the national adherence guidelines for chronic diseases in South Africa. Poster presented at the 9th IAS conference on HIV science, Paris, France.
- Fox, M. P., & Rosen, S. (2010). Patient retention in antiretroviral therapy programs up to three years on treatment in sub-Saharan Africa, 2007–2009: Systematic review. Tropical Medicine & International Health, 15(Suppl. 1), 1–15. doi: 10.1111/j.1365-3156.2010.02508.x
- Fraser, H., Allen, C., Bailey, C., Douglas, G., Shin, S., & Blaya, J. (2007). Information systems for patient follow-up and chronic management of HIV and tuberculosis: A life-saving technology in resource-poor areas. Journal of Medical Internet Research, 9(4), e29. doi: 10.2196/jmir.9.4.e29
- Geng, E. H., Nash, D., Kambugu, A., Zhang, Y., Braitstein, P., Christopoulos, K. A., … Martin, J. N. (2010). Retention in care among HIV-infected patients in resource-limited settings: Emerging insights and new directions. Current HIV/AIDS Reports, 7(4), 234–244. doi: 10.1007/s11904-010-0061-5
- Gilvydis, J. M., Steward, W. T., Saberi, P., Tumbo, J., Sumitani, J., Barnhart, S., & Lippman, S. A. (2015). Need for improvements in clinical practice to retain patients in pre-antiretroviral therapy care: Data from rural clinics in North West Province, South Africa. AIDS Care, 27(10), 1275–1278. doi: 10.1080/09540121.2015.1050985
- Govindasamy, D., Meghij, J., Negussi, E. K., Baggaley, R. C., Ford, N., & Kranzer, K. (2014). Interventions to improve or facilitate linkage to or retention in pre-ART (HIV) care and initiation of ART in low- and middle-income settings – a systematic review. Journal of the International AIDS Society, 17(1). doi: 10.7448/IAS.17.1.19032
- Harklerode, R., Schwarcz, S., Hargreaves, J., Boulle, A., Todd, J., Xueref, S., … Rice, B. (2017). Feasibility of establishing HIV case-based surveillance to measure progress along the health sector cascade: Situational assessments in Tanzania, South Africa, and Kenya. JMIR Public Health and Surveillance, 3(3), e44. doi: 10.2196/publichealth.7610
- Hochgesang, M., Zamudio-Haas, S., Moran, L., Nhampossa, L., Packel, L., Leslie, H., … Shade, S. B. (2016). Scaling-up health information systems to improve HIV treatment: Anassessment of initial patient monitoring systems in Mozambique. International Journal of Medical Informatics, 97, 322–330. doi: 10.1016/j.ijmedinf.2016.11.002
- Karcher, H., Omondi, A., Odera, J., Kunz, A., & Harms, G. (2007). Risk factors for treatment denial and loss to follow-up in an antiretroviral treatment cohort in Kenya. Tropical Medicine & International Health, 12, 687–694. doi: 10.1111/j.1365-3156.2007.01830.x
- Kitsao, R., Kimani, J., Muriuki, F., & Akolo, M. (2017, July). Effects of SMS reminders on key population appointment adherence and retention: Our success story. Poster presented at the 9th IAS conference on HIV science, Paris, France.
- Krebs, D. W., Chi, B. H., Mulenga, Y., Morris, M., Cantrell, R. A., Mulenga, L., … Stringer, J. S. (2008). Community-based follow-up for late patients enrolled in a district wide programme for antiretroviral therapy in Lusaka, Zambia. AIDS Care, 20(3), 311–317. doi: 10.1080/09540120701594776
- Lambdin, B. H., Micek, M. A., Koepsell, T. D., Hughes, J. P., Sherr, K., Pfeiffer, J., … Stergachis, A. (2012). An assessment of the accuracy and availability of data in electronic patient tracking systems for patients receiving HIV treatment in central Mozambique. BMC Health Services Research, 12(1), S58. doi: 10.1186/1472-6963-12-30
- Lawn, S. D., Myer, L., Harling, G., Orrell, C., Bekker, L. G., & Wood, R. (2006). Determinants of mortality and nondeath losses from an antiretroviral treatment service in South Africa: Implications for program evaluation. Clinical Infectious Diseases, 43, 770–776. doi: 10.1086/507095
- McMahon, J. H., Moore, R., Eu, B., Tee, B. K., Chen, M., El-Hayek, C., … Paraskevis, D. (2015). Clinic network collaboration and patient tracing to maximize retention in HIV care. PloS One, 10(5), e0127726. doi: 10.1371/journal.pone.0127726
- Mganga, J., Zenda, P., Zephania, G., Msanja, J., Hasegawa, A., & Tanaka, A. (2014, July). Reducing patients’ lost to follow-up through data feedback – mkuranga practice in Tanzania. Poster presented at the 20th international AIDS conference, Melbourne, Australia.
- Mugavero, M. J., Westfall, A. O., Zinski, A., Davila, K., Drainoni, M. L., Gardner, L., … Measuring retention in HIV care. (2012). Measuring retention in HIV care: The elusive gold standard. JAIDS Journal of Acquired Immune Deficiency Syndromes, 61(5), 574–580. doi: 10.1097/QAI.0b013e318273762f
- Mugisa, A., Mugume, A., Odong, T., & Ndagire, H. (2014, July). Improving client retention in HIV care clinics using patient appointment books: A case of east central Uganda. Poster presented at the 20th international AIDS conference, Melbourne, Australia.
- Naidoo, N. P. (2006). Organisational Capacity of Public Sector ART Provision in Gauteng Province and its Impact on Adherence: Case Studies of Two Facilities (Doctoral dissertation). Retrieved from: http://wiredspace.wits.ac.za/bitstream/handle/10539/5804/NaidooNP_final%20research%20report.pdf?sequence=2.
- Ncholo, E. K. (2010). Review of patient follow up mechanisms in the two Ekurhuleni metropolitan hospitals providing antiretroviral treatment (Doctoral dissertation). Retrieved from: http://wiredspace.wits.ac.za/handle/10539/7654.
- Nglazi, M. D., Kaplan, R., Wood, R., Bekker, L. G., & Lawn, S. D. (2010). Identification of losses to follow-up in a community-based antiretroviral therapy clinic in South Africa using a computerized pharmacy tracking system. BMC Infectious Diseases, 10(1), 1897. doi: 10.1186/1471-2334-10-329
- Odhiambo, F., Wandina, D., Ojoo, S., Nganga, L., Mongare, J., Ngethe, R., … Refield, R. (2014, July). Sustainable response to loss to follow-up among HIV infected patients receiving ART: Impact of implementing continuous quality improvement mechanisms in a large ART program in Kenya. Poster presented at the 20th international AIDS conference, Melbourne, Australia.
- Ramdas, N., Meyer, J. C., & Cameron, D. (2015). Factors associated with retention in HIV care at Sediba Hope Medical Centre. Southern African Journal of HIV Medicine, 16(1), 1–6. doi: 10.4102/sajhivmed.v16i1.347
- Rosen, S., Fox, M. P., & Gill, C. J. (2007). Patient retention in antiretroviral therapy programs in sub-Saharan Africa: A systematic review. PLoS Medicine, 4(10), e298. doi: 10.1371/journal.pmed.0040298
- Scheibe, F. J., Waiswa, P., Kadobera, D., Müller, O., Ekström, A. M., Sarker, M., & Neuhann, H. F. (2013). Effective coverage for antiretroviral therapy in a Ugandan district with a decentralized model of care. PloS One, 8(7), e69433. doi: 10.1371/journal.pone.0069433
- South African National Department of Health. (2010). Models for the scale up of HIV prevention, treatment and care from South Africa and beyond. Retrieved from http://www.ihi.org/resources/Documents/TriedandTested_ModelsforScaleUpHIVPrevention_Book.pdf
- Stricker, S. M., Fox, K. A., Baggaley, R., Negussie, E., de Pee, S., Grede, N., & Bloem, M. W. (2014). Retention in care and adherence to ART are critical elements of HIV care interventions. AIDS and Behavior, 18(5), 465–475. doi: 10.1007/s10461-013-0598-6
- Tjaronda, W., Mwinga, S., Kagoya, H., & Mazibuko, G. (2017, March). Using the electronic dispensing tool to retain patients on antiretroviral therapy in Namibia. Blog published on the SIAPS Program website. Retrieved from http://siapsprogram.org/2017/03/13/using-the-electronic-dispensing-tool-to-retain-patients-on-antiretroviral-therapy-in-namibia/
- Tweya, H., Gareta, D., Chagwera, F., Ben-Smith, A., Mwenyemasi, J., Chiputula, F., … Phiri, S. (2010). Early active follow-up of patients on antiretroviral therapy (ART) who are lost to follow-up: The “back-to-care” project in Lilongwe, Malawi. Tropical Medicine & International Health, 15(Suppl. 1), 82–89. doi: 10.1111/j.1365-3156.2010.02509.x
- UNAIDS. (2014). Fast-track: Ending the AIDS epidemic by 2030. Retrieved from http://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_en.pdf
- Vella, V., Govender, T., & Scelo, D. (2008). Evaluation of the antiretroviral therapy in KwaZulu-Natal, South Africa.
- Vidanapathirana, J., Premadasa, P., Disanayake, N., Wijegoonewardene, N., & Mallikarachchi, D. (2016). Let us know about HIV and AIDS: Achieving triple zeros: Handbook on HIV & AIDS for primary health care workers, national STD/AIDS control programme, United Nations population fund, Colombo, Sri Lanka.
- Wandina, D., Odhiambo, F., Ojoo, S., Mongare, J., Ogillo, G., Muriuki, J., … Ngethe, R. (2011, July). Strategies for reducing lost to follow-up rates in adult patients receiving antiretroviral treatment in rural services in Kenya. Poster presented at the 6th international AIDS society conference on HIV pathogenesis, treatment and prevention, Rome, Italy.
- WHO. (2006). Patient monitoring guidelines for HIV care and antiretroviral therapy. Retrieved from http://www.who.int/3by5/capacity/ptmonguidelinesfinalv1.PDF
- WHO. (2011, September). Retention in HIV Programmes: Defining the challenges and identifying solutions (Meeting report).
- WHO. (2015). Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. Retrieved from http://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/
- WHO & UNAIDS. (2013). Guidelines for second generation HIV surveillance. Retrieved from http://www.who.int/hiv/pub/surveillance/2013package/module1/en/surveillance/2013package/module1/en/
- Yu, J. K. L., Chen, S. C. C., Wang, K. Y., Chang, C. S., Makombe, S. D., Schouten, E. J., & Harries, A. D. (2007). True outcomes for patients on antiretroviral therapy who are lost to follow-up in malawi. Bulletin of the World Health Organization, 85(7), 550–554. doi: 10.2471/BLT.06.037739
