
ABSTRACT
Suboptimal adherence to antiretroviral therapy (ART) remains common. Patient-centered tools are needed to comprehensively assess adherence barriers in HIV clinical practice. Thus, we conducted a research synthesis to produce a conceptual framework for a new patient-reported outcome measure (PRO) for use in routine HIV care in Canada and France. A PRO’s conceptual framework graphically represents the concepts to be measured and the potential relationships between them. Towards ensuring the framework’s relevance to the target populations’ concerns, qualitative studies with HIV-positive adults on barriers to ART adherence in developed countries were synthesized with thematic analysis, attending to the cross-study prevalence and interrelationships of barrier themes. In March 2016, searches within Medline, PsychINFO, and Embase produced 5,284 records. Two reviewers determined the final sample (n = 41). Analysis generated three levels of ART adherence barrier themes. Twenty Level 2 themes and their component subthemes (Level 3) were organized into 6 higher-order themes (Level 1): Cognitive and emotional aspects (100% of studies contributing content -prevalence), Lifestyle factors (95%), Social and material context (95%), Characteristics of ART (90%), Health experience and state (73%), and Healthcare services and system (66%). As to interrelationships, study authors articulated relationships between all higher-order themes (Level 3). Linkages between Level 2 barrier themes showed great variability, from 21% to 95%. Overall, this synthesis contributes an exceptionally detailed conceptual framework and report of ART adherence barriers, applicable to a wide range of PLHIV. It suggests that a key to understanding many barriers is through their interconnections. It also identifies gaps in barrier research. Concerning the new PRO’s development, comprehensiveness will need to be weighed against other concerns (e.g., respondent burden) and the provision of barrier-specific guidance for clinically addressing its scores seems essential.
Introduction
The individual and public health benefits of highly-active antiretroviral therapy (ART), the standard of HIV care since 1996, depend on assiduous and sustained adherence to this lifelong treatment by people living with HIV (PLHIV). While levels of adherence required for viral suppression may vary between regimens (Viswanathan et al., Citation2015), they are high and “strict” adherence is clinically recommended (U.S. Department of Health and Human Services [DHHS], Citation2016). Despite the arrival of simpler and more tolerable regimens (Truong, Schafer, & Short, Citation2015), suboptimal adherence remains common (Puskas et al., Citation2017; Viswanathan et al., Citation2015) and appears disproportionately elevated in some developed regions of the world (Mills et al., Citation2006; Ortego et al., Citation2011). Notably, a global meta-analysis of observational studies from 1999 to 2009 found among the lowest levels of ≥ 90% adherence in North America (59%) and Western Europe (61%) (Ortego et al., Citation2011). In HIV clinical practice, despite recommendations to identify potential barriers to adherence (DHHS, Citation2016) and indications of agreement between patients and providers about adherence as a priority area (Fredericksen et al., Citation2015), the visibility of PLHIV’s ART adherence challenges and capacity to address them may be limited. Reasons include reliance on viral load as an indicator of adherence (DHHS, Citation2016), some ART regimens being potentially more forgiving of missed doses (Viswanathan et al., Citation2015), and inadequate patient-provider communication about ART adherence (Laws et al., Citation2013; Wilson et al., Citation2010). For some, insufficient consideration of qualitative research and, consequently, of the complexity and context of patients’ lives in ART adherence guidelines also contributes to the persistence of adherence problems (Barroso, Leblanc, & Flores, Citation2017).
Barriers to ART adherence are widely acknowledged to be multiple, complex, dynamic and multi-level, from individual to structural (Shubber et al., Citation2016). Improving their detection in routine HIV care carries many potential advantages, including the opportunity to intervene before clinical markers deteriorate (Genberg, Lee, Rogers, & Wilson, Citation2015). Given the range of ART adherence barriers documented, it could also serve to improve overall care, notably, by helping to detect co-morbid conditions (e.g., mental illness), manage symptoms, monitor treatment impacts, improve patient-provider communication, and foster more patient-centered care, benefits accorded to the clinical use of patient-reported outcome measures (Fredericksen et al., Citation2012; Greenhalgh, Citation2009). Patient-centered care has become an aspiration for health care (Warsame & Halyard, Citation2017), including in HIV (World Health Organization, Citation2016), modeled, in part, on a view of patient and provider as collaborators. It depends on providers engaging with patients’ preferences, needs, values, views and experiences of their care (Barry & Edgman-Levitan, Citation2012). Systematically capturing patient-identified ART adherence barriers could help this process, providing important information to clinicians for effectively orienting patient-provider discussion and intervention.
There are few, if any, current, comprehensive and validated measures of patient-identified adherence barriers to ART (Engler, Lessard, & Lebouché, Citation2017) and reasons for ART non-adherence remain inadequately understood in current resource-rich settings (Siefried et al., Citation2017). Hence, our research team will be developing an electronically-administered patient-reported outcome measure (PRO) to assess ART adherence barriers in the context of adult HIV care in Canada and France.
The present study’s aim is to synthesize appropriate qualitative research with PLHIV to generate the measure’s conceptual framework. A PRO’s conceptual framework graphically represents the concepts measured and the potential relationships between them (DHHS Food and Drug Administration, Citation2009). However, a PRO’s content validity rests, in part, on the measure’s conceptual domains being relevant to the target patients’ concerns (Francis, McPheeters, Noud, Penson, & Feurer, Citation2016). As qualitative research emphasizes the meanings, experiences, and views of participants (Pope & Mays, Citation1995), it was favored to help identify barriers to ART adherence that are important to PLHIV and, in turn, to contribute to making the measure patient-centered, that is, one that PLHIV care about (Mayo, Citation2015). This is essential as a PRO’s adoption and utility in clinical care depend, in part, on its meaningfulness and relevance to end users (Ahmed et al., Citation2017). Given the above, this synthesis is guided by the following research question: Based on findings derived from qualitative methods of studies conducted in developed countries with HIV-positive adults, what factors are identified as barriers to taking ART as prescribed and how are they interrelated?
Methods
Design
Thematic analysis was used, a recognized methodology for qualitative synthesis (Bearman & Dawson, Citation2013), following Braun and Clarke’s (Citation2006) iterative 6-step approach (see ). It involves searching across a “data set” for recurring patterns of meaning. It was selected for its flexibility, allowing the inductive identification of semantic (or more explicit) themes (in the qualitative findings of included studies) to produce a detailed description of barriers to ART adherence useful for the foundation of our PRO’s conceptual framework.
Table 1. Iterative phases of the thematic analysis for the qualitative synthesis.
Search strategy
We searched three databases (Medline, PsychINFO, Embase) on March 10, 2016. Search queries were designed with a university librarian. They used a combination of index terms, words in the text, title, and abstract, and keyword headings and keyword heading words. Queries were adapted to each database, and targeted three concepts: (1) HIV; (2) ART adherence; (3) qualitative studies. Search queries are available upon request. The records obtained from these searches were de-duplicated, and screened based on their title and abstract for full-text examination. Twenty percent of both the de-duplicated records and the records marked for full-text examination were evaluated by another co-author to test interrater reliability with Cohen’s Kappa (McHugh, Citation2012).
Inclusion and exclusion criteria
We sought articles published from 1996, written in English or French, reporting studies conducted with PLHIV in a developed country (World Economic Situation and Prospects, Citation2012). Research from developed countries was selected to promote the relevance of the barriers identified to our PRO’s target populations (PLHIV in Canada and France) and the content validity of the conceptual framework generated. We included original qualitative studies, including mixed-methods and reviews of qualitative research, collecting the perspectives of ART-experienced adults living with HIV on barriers to ART adherence. Barriers to adherence referred here to any factor identified through the study’s qualitative analyses that is explicitly mentioned in the results or discussion as making it difficult to take ART or is directly linked with non-adherence.
Given variability in reporting on the participants’ ART-related experience, we included studies that explicitly stated that 90%–100% of participants had either received a prescription for, were currently on, or had experience taking ART, or if there was implicit evidence that all participants were ART-experienced (see Table 3 for examples in supplemental material). To ensure relevance, we included studies in which roughly half or more of the qualitative results were on adherence barriers and there was more than one evident analytical concept or theme on the issue.
We excluded conference abstracts and studies only concerned with barriers to adherence in correctional environments or in youth under 18 years old. Details on the included studies’ methodology were collected, but no formal quality appraisal was performed. There is debate on its place in qualitative synthesis (Atkins et al., Citation2008) and excluding studies on this basis comes with risks, including the potential conflation of study quality with the quality of study reporting (Campbell et al., Citation2011). Furthermore, evidence indicates that including poorer quality studies in a qualitative synthesis is unlikely to significantly distort the findings (Campbell et al., Citation2011; Vervoort, Borleffs, Hoepelman, & Grypdonck, Citation2007).
Data extraction
For descriptive purposes, we extracted the following aspects from each included study and organized them in table form: a short reference (first author, publication year); country (with details, as available, e.g., state/province); some of the qualitative participants’ sociodemographic characteristics; number of participants; ART regimen experience and criteria; study setting; data collection method; qualitative approach employed, and any theoretical framework guiding analysis.
Data synthesis
presents how the steps of the thematic analysis were operationalized. As prevalence is a consideration in theme development (Braun & Clarke, Citation2006) and may be useful input when deciding on the weight accorded to the PRO’s conceptual domains during measure specification (Crocker & Algina, Citation1986), the proportion of studies contributing data to each theme was recorded. Relationships articulated by study authors between themes (e.g., associations, interactions) were also documented.
Results
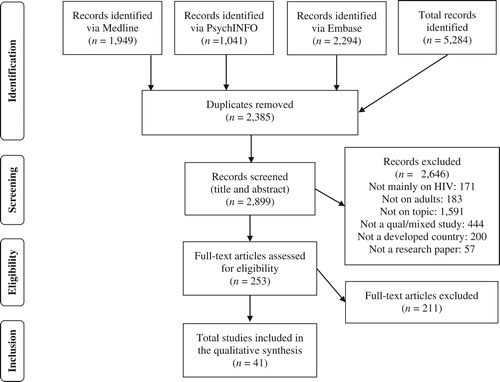
The search flow
presents the flow diagram (Moher, Liberati, Tetzlaff, Altman & The PRISMA Group, Citation2009) of the search strategy. The database search identified 5,284 records from which 2,385 duplicates were removed. The titles and abstracts of the remaining records were screened leading to the elimination of 2,646 records and the assessment of 253 full-texts for eligibility. Percent agreement for the 20% of de-duplicated records (n = 580) was 93% and Cohen’s Kappa was 0.63 (95% confidence interval (CI) = 0.52–0.73), considered a moderate level of interrater agreement (McHugh, Citation2012). Percent agreement for the 20% of full text articles (n = 51) was higher at 98%, as was Cohen’s Kappa at 0.94 (95%CI = 0.59–0.82), considered almost perfect. All rating differences were discussed and easily resolved. In total, 41 study articles were included in the synthesis.
Figure 1. Search flow diagram for the qualitative synthesis.
The study sample
Table 2 (see supplemental material) presents the studies’ details. Most were conducted in the United States (n = 35; 85%) while 3 were led in Europe (Switzerland, the Netherlands and Belgium) and 2 in Canada. A final study, a review, included only studies of “Western” origin. The study publication date range, extends from 1999 to 2015, with over half (54%) published from 2005 to 2015 (n = 22).
The remaining description excludes the review. The sources of recruitment for PLHIV were clinical contexts (e.g., HIV clinics, pharmacies) for over half of studies (n = 21), followed by a combination of clinical and community sources (e.g., AIDS service organizations (ASOs), advertisements) (n = 9). Five studies recruited through a research unit or existing study and 4 recruited from the community alone (e.g., ASOs, word of mouth, flyers). One study did not specify where participants were recruited. The number of HIV-positive qualitative study participants ranged from 14 to 113 per study, with an average of 37 (SD = 24).
The samples of PLHIV were composed only of women in 7 studies, including 2 among African American women and 1 among current or past alcohol- or substance-using women. Three studies were conducted exclusively with men, 2 of which were composed only of gay or bisexual men, including 1 study devoted to methamphetamine users. However, in 10 additional studies, three-quarters or more of the sample was male. Three studies required a mental illness diagnosis, with 1 focusing on methamphetamine use disorder and another on depressive disorder, while 6 studies had samples of only past or current substance users. Four studies were conducted only with Spanish-speakers, including one devoted to geographically mobile Dominicans and another to immigrant Latinos or Hispanics. A final study concerned previously incarcerated individuals.
Qualitative data collection proceeded with interviews alone in over half of studies (n = 22), followed by only focus groups (n = 13). Four studies combined interviews with another method (field observation, journal entries or focus groups). One study collected data with journal entries alone. Data were analyzed with a variety of methods, most commonly a form of content analysis (n = 9) or grounded theory analysis (n = 9). Less than a fifth of studies (n = 7) were guided by a framework (e.g., a theory, model, paradigm, existing taxonomy).
The synthesis
The analysis generated three levels of ART adherence barrier themes, presented in Table 3 (see supplemental material), which also informs on their prevalence and interrelationships. Below are definitions for each Level 2 theme, in order of prevalence as grouped within the higher-order Level 1 themes. Definitions reflect the data included within.
Cognitive and emotional aspects
“Affect” refers to negative emotions, including those arising from other barriers. “Beliefs” refer to beliefs about ART, adherence and HIV. “Acceptance” relates to non-acceptance, avoidance or denial of one’s HIV diagnosis and what it entails. “Motivation” concerns either a lack of motivation to adhere (e.g., motivation, desire, willingness, drive, want) or, conversely, a desire to assert control over one’s life, disease, and/or pill-taking. “Knowledge” pertains to having insufficient or incorrect knowledge of ART and adherence, including having unanswered questions, being faced with conflicting information and difficulty understanding.
Lifestyle factors
“Life demands and organizational issues” encompass barriers concerned with the structure, pace, multiplicity, nature or modification of one’s daily activities and responsibilities and one’s organization for adherence. “Substance use” refers to aspects of illicit drug use and alcohol consumption.
Social and material context
“Social interaction, support and relationships” relates to barriers concerned with the supportiveness, quality and presence of personal relationships and interactions with others. “HIV stigma and concealment” concerns barriers tied to HIV stigma and discrimination as well as not wanting others to know about one’s HIV status or to see one taking ART. “Material and structural challenges” are difficult material circumstances, such as financial constraints; unstable, inadequate or absent housing; lacking or insecure employment; and limited access to food or transportation. Challenges related to having a social status that carries disadvantages are also grouped here (e.g., gender, immigration status, marginalization, non-speaker of the official language(s), involvement in the criminal justice system).
Characteristics of ART
“Side effects” are adverse effects attributed to ART, whether anticipated (in the short or long-term), currently experienced or having occurred in the past. “Instructions” signify the demands of the ART regimen, particularly its complexity, dosing schedule, food and water requirements, magnitude, storage requirements, lifelong commitment, and provider changes to it. The “Physical features” of ART relate to its form (e.g., pill, liquid), size, smell, taste or route of administration (e.g., oral).
Health experience and state
“Body monitoring” pertains to attending to how one feels (i.e., well or unwell) or interpreting what one’s body needs and adjusting adherence accordingly. “Comorbidity” relates to coexisting medical problems with HIV infection, including mental illness, and the challenges of comedication. “Manifestations of HIV disease and general health” includes barriers tied to HIV infection’s clinical signs (e.g., viral load, CD4 cell count), whether good or bad; symptoms, whether present or absent; and its impairments as well as general health.
Healthcare services and system
The “Patient-provider relationship” concerns barriers tied to one’s relationship and interactions with HIV healthcare providers, in terms of quality, trustworthiness, and accessibility. “HIV clinic and healthcare system issues” relate to the HIV clinic and its services (e.g., difficulty getting appointments) and the broader healthcare system (e.g., limit of a 1-month supply of medication). “Pharmacy issues” refer to problems with pharmacy staff (e.g., unprofessional, inadequate counsel) and access to HIV medication refills at the pharmacy level (e.g., stock outs, difficulty going to the pharmacy, limited pharmacy opening hours). “Health insurance” barriers concern the state, requirements, policies, practices and limitations of one’s health insurance and its coverage for HIV medications.
Theme prevalence and interrelationships
While prevalence was more variable for Level 2 themes, from 22% to 95% (see Table 3 in supplemental material), most studies (66%–100%) contributed content to the higher-order Level 1 themes (see ). Regarding interrelationships, Level 2 barrier themes were linked together from 21% to 95%. charts the cross-study frequency of associations drawn between Level 2 barriers in their impact on adherence. Almost two-thirds of these associations were mentioned by study authors in their analyses (117/190; 62%). However, at Level 1, as illustrated in , all themes were linked, although some considerably more so than others (see ). also portrays the working conceptual framework for the new PRO and indicates that within each Level 1 theme, there is at least one relationship between its component Level 2 themes.
Figure 2. Conceptual framework of barriers to antiretroviral therapy adherence derived from the thematic analysis.
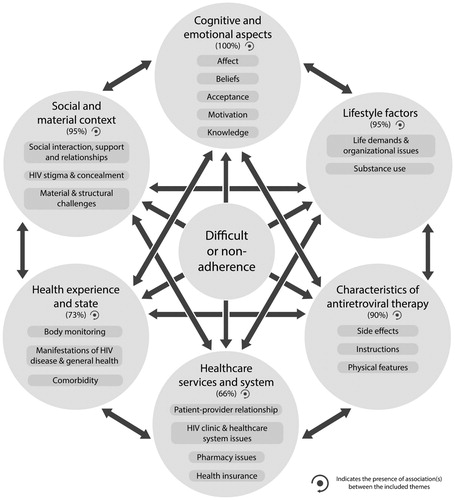
Table 2. Prevalence across studies (n = 41) of relationships articulated between antiretroviral therapy (ART) adherence barrier themes (Level 2 themes).
Discussion
Patient-centered tools are needed to routinely and comprehensively assess ART adherence barriers in HIV clinical practice. To design a new PRO measure for this purpose, we conducted a qualitative synthesis of research in developed countries to build its conceptual framework. It identified 3 levels of themes, including 20 classes of barriers (Level 2) organized into 6 higher order themes (Level 1) that are applicable to a range of populations. In their influence on adherence, barriers proved highly interconnected. Relative to other reviews of qualitative research on ART adherence barriers in developed countries (Bolsewicz, Debattista, Vallely, Whittaker, & Fitzgerald, Citation2015; Vervoort et al., Citation2007), this work not only contributes a graphic, synoptic view of barriers and their interrelationships but offers a high level of detail for more in-depth exploration (e.g., numerous subthemes, Level 2 barrier interrelations). Hence, it helps unpack the complexity of ART adherence barriers, if not, improve our understanding of reasons for non-adherence among PLHIV. By documenting theme prevalence across studies, it also underlines potential gaps in the research.
Implications for conceptualizing and studying ART adherence barriers
All or virtually all studies mentioned barriers relating to the themes of Cognitive and emotional aspects, Lifestyle factors, the Social and material context, and the Characteristics of ART. Decreased ART adherence has been statistically associated with patient-identified barriers within each of these themes (Genberg et al., Citation2015). Least commonly mentioned were barriers pertaining to the Healthcare services and system theme. This may be due to the inclusion criterion of ART experience, leading most participants in most studies reviewed to be on ART and, thus, to have healthcare ties. The barriers of ART experienced individuals with poor or irregular engagement in care may, therefore, be underrepresented and worth further investigating. Conversely, health service barriers may not be most prevalent (Shubber et al., Citation2016). In any case, current measures of patient-identified barriers or reasons for ART non-adherence with evidence of validity (Genberg et al., Citation2015; Schonnesson, Ross, & Williams, Citation2004; Walsh, Horne, Dalton, Burgess, & Gazzard, Citation2001) do not appear to address issues of the Healthcare services and system theme and several level 2 themes (e.g., Acceptance of HIV status, Comorbidity, Material and structural challenges), further illustrating the need for more encompassing measures.
Our findings also suggest that many, if not, most barriers must be understood through their interrelationships versus conceiving them as singular, independent entities. This is perhaps most evident with the Affect theme (i.e., negative emotions), shown to potentially permeate almost all other Level 2 themes, and with substance use, most barriers of which were tied to other level 2 themes (see ). The notion of barriers as constellations -as composed of interconnected, evolving, and contextualized impediments to adherence- could be helpful for further reflection. Indeed, without understanding their context, barriers like “forgetting,” among the most frequently reported (Shubber et al., Citation2016), offer little clear direction for intervention. For example, in this synthesis, themes with which it was associated include (non)Acceptance of one’s HIV status (Witteveen & Van Ameijden, Citation2002), Substance use (Ryan & Wagner, Citation2003), Life demands (e.g., work (Adam, Maticka-Tyndale, & Cohen, Citation2003), caregiving (Roberts, Citation2000)) and organizational issues (e.g., routinization (Vervoort, Grypdonck, De Grauwe, Hoepelman, & Borleffs, Citation2009)), Stigma (e.g., hiding pills) (Taylor et al., Citation2014), Side effects of ART (Russell et al., Citation2003), as well as Social interaction (e.g., social life) (Vervoort et al., Citation2007), which may require different approaches.
Implications for clinical practice and the new PRO
These results suggest, as advanced in a recent quantitative review, that no single intervention can ensure the maintenance of high ART adherence (Shubber et al., Citation2016) and that efforts in this direction should accommodate multiple barrier types. Given their diversity, the clinical management of ART adherence barriers should be tailored to the individual patient. The conceptual framework generated or a simplified version of it (Engler, Lènàrt, Lessard, Toupin, & Lebouché, Citation2017) could serve as a visual aid to discuss barriers in clinical practice.
As for our PRO measure, the framework indicates that it will be multidimensional and possibly based on Level 2 themes. The quantity of barrier themes identified emphasizes that choices about the number of items composing the measure will need to weigh comprehensiveness against such factors as respondent burden and clinical relevance (Chang, Citation2007). Nevertheless, the PRO may still raise issues that do not typically fall within the purview of standard HIV care. Hence, its use could encounter noted challenges of PRO implementation in clinical practice such as provider uncertainty about how to respond to the scores produced (Locklear et al., Citationn.d.). In addition, patient-provider communication difficulties surrounding ART adherence may not be resolved with the introduction of this measure. Several studies have found that some PLHIV omit to share their adherence problems with providers (e.g., Golub, Indyk, & Wainberg, Citation2006; Laws, Wilson, Bowser, & Kerr, Citation2000). Similarly, investigators have argued that self-report measures, such as those on ART adherence barriers, are prone to under-reporting (Kalichman, Kalichman, & Cherry, Citation2017). However, relative to information collected during routine care, others suggest that electronically administered PROs can decrease social desirability bias, thus improving the quality of data captured on sensitive domains (Kozak et al., Citation2012). Nevertheless, how PRO data is used in clinical practice is critical and minimizing ART adherence barriers in care with a PRO is a complex challenge. Indeed, authors have stressed the need for disease management pathways or guidelines to address issues raised through PRO assessment in clinical care (Warsame & Halyard, Citation2017). One way forward is to develop intervention suggestions specific to each barrier theme (Level 2) that are customized to and accompany the PRO’s results. With provincial funding, we will develop such recommendations for use in HIV clinical practice in Montreal, Quebec, with mixed-methods and iterative rounds of patient and provider consultation. This approach, building on stakeholder engagement (Concannon et al., Citation2014), is consistent with arguments to incorporate patients’ perspectives in clinical guidelines (Légaré et al., Citation2011), more generally, and qualitative research in guidance for addressing ART adherence barriers in care, more specifically (Barroso et al., Citation2017). Furthermore, linking PRO scores with specific intervention paths to consider may improve chances of positively impacting patient care and outcomes (Snyder et al., Citation2012).
Limitations of the synthesis
This synthesis was shaped by pragmatic considerations (e.g., time/resource constraints, given the extensive PRO development study). Consequently, its study sample is potentially vulnerable to the disadvantages of linear sampling, the selected search databases’ coverage limitations, and journal publication biases (Suri, Citation2011). Nevertheless, the constituted sample is comparable in size to that of other qualitative syntheses on medication adherence (Munro et al., Citation2007; Pound et al., Citation2005) and allows for “data sufficiency,” arguably providing enough evidence for the synthesis’ main purpose (Suri, Citation2011). In addition, a sole person was mainly responsible for performing the thematic analysis which may raise concerns about trustworthiness (see author contributions). However, as described in , the extensive “paper trail” maintained, team member participation in evaluating each theme in relation to its study excerpts, and the final rechecking of all analyses, attest to the rigor with which this work was conducted.
This synthesis also has limitations as a foundation for the new PRO, which is intended to capture aspects of HIV-patients’ experience that they value. In synthesizing qualitative research, we recognize providing an interpretation (through our analyses) of an interpretation (by study authors) of an interpretation (by participants of their experience) (Ring, Ritchie, Mandava, & Jepson, Citation2010). Hence, there is a “distance” between our results and patients’ experience and priorities. However, our PRO development methodology incorporates several safeguards for the measure’s content validity, including comparison of the framework against semi-structured interviews with patients in each clinic and others described below.
An added limitation is that most studies reviewed were conducted in the USA which raises questions of the transferability of our synthesis to the clinics, across Canada and France, where we will seek to validate and pilot the PRO. Conversely, regarding Level 1 themes, with some nuances, these were later found to largely correspond to the dimensions of the World Health Organization’s model of adherence across chronic conditions, including HIV (WHO, Citation2003). In addition, our Montreal-based patient advisory committee, described elsewhere (Engler, Lessard, Toupin, Lènàrt, & Lebouché, Citation2017), gave feedback on the framework (September 2017). Evaluating the twenty Level 2 themes on relevance, the six members present rated half as high priority content areas for the PRO, while no theme was unanimously deemed irrelevant. Finally, Canadian HIV clinicians (n = 20) spontaneously mentioned barriers within 17/20 themes, in our research with providers (Toupin et al., Citation2018).
Conclusion
This qualitative synthesis offers an extensive portrait of ART adherence barriers and their interconnections in developed countries, particularly, in North America. One task at hand is to determine how these may be identified and addressed in HIV care in an effective and patient-centered way.
Supplemental Material
Download Zip (72.2 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
David Lessard http://orcid.org/0000-0002-1151-3763
Additional information
Funding
References
- Adam, B. D., Maticka-Tyndale, E., & Cohen, J. J. (2003). Adherence practices among people living with HIV. AIDS Care, 15(2), 263–274.
- Ahmed, S., Ware, P., Gardner, W., Witter, J., Bingham, C. O., Kairy, D., & Bartlett, S. J. (2017). Montreal Accord on Patient-Reported Outcomes (PROs) use series - Paper 8: Patient-reported outcomes in electronic health records can inform clinical and policy decisions. Journal of Clinical Epidemiology, 89, 160–167.
- Atkins, S., Lewin, S., Smith, H., Engel, M., Fretheim, A., & Volmink, J. (2008). Conducting a meta-ethnography of qualitative literature: Lessons learnt. BMC Medical Research Methodology, 8, 271.
- Barroso, J., Leblanc, N. M., & Flores, D. (2017). It’s not just the pills: A qualitative meta-synthesis of HIV antiretroviral adherence research. Journal of the Association of Nurses in AIDS Care, 28, 462–478.
- Barry, M. J., & Edgman-Levitan, S. (2012). Shared decision making -pinnacle of patient-centered care. New England Journal of Medicine, 366(9), 780–781.
- Bearman, M., & Dawson, P. (2013). Qualitative synthesis and systematic review in health professions education. Medical Education, 47, 252–260.
- Bolsewicz, K., Debattista, J., Vallely, A., Whittaker, A., & Fitzgerald, L. (2015). Factors associated with antiretroviral treatment uptake and adherence: A review. Perspectives from Australia, Canada, and the United Kingdom. AIDS Care, 27(12), 1429–1438.
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101.
- Campbell, R., Pound, P., Morgan, M., Daker-White, G., Britten, N., Pill, R., … Donovan, J. (2011). Evaluating meta-ethnography: Systematic analysis and synthesis of qualitative research. Health Technology Assessment, 15(43), 1–164.
- Chang, C. H. (2007). Patient-reported outcomes measurement and management with innovative methodologies and technologies. Quality of Life Research, 16(suppl.1), 157–166.
- Concannon, T. W., Fuster, M., Saunders, T., Patel, K., Wong, J. B., Leslie, L. K., & Lau, J. (2014). A systematic review of stakeholder engagement in comparative effectiveness and patient-centered outcomes research. Journal of General Internal Medicine, 29(12), 1692–1701.
- Crocker, L., & Algina, J. (1986). Introduction to classical & modern test theory. Belmont, CA: Wadsworth Group.
- Engler, K., Lènàrt, A., Lessard, D., Toupin, I., & Lebouché, B. (2017, June). A synthesis of qualitative research with adults living with HIV on barriers to ART adherence. Poster session presented at the 12th international conference on HIV treatment and prevention adherence, Miami, FL.
- Engler, K., Lessard, D., & Lebouché, B. (2017). A review of HIV-specific patient-reported outcome measures. The Patient - Patient-Centered Outcomes Research, 10(2), 187–202.
- Engler, K., Lessard, D., Toupin, I., Lènàrt, A., & Lebouché, B. (2017). Engaging stakeholders into an electronic patient-reported outcome development study: On making an HIV-specific e-PRO patient-centered. Health Policy and Technology, 6(1), 59–66.
- Francis, D. O., McPheeters, M. L., Noud, M., Penson, D. F., & Feurer, I. D. (2016). Checklist to operationalize measurement characteristics of patient-reported outcome measures. Systematic Reviews, 5, 50.
- Fredericksen, R., Crane, P. K., Tufano, J., Ralston, J., Schmidt, S., Brown, T., … Crane, H. M. (2012). Integrating a web-based, patient-administered assessment into primary care for HIV-infected adults. Journal of AIDS and HIV Research (Online), 4(2), 47–55.
- Fredericksen, R. J., Edwards, T. C., Merlin, J. S., Gibbons, L. E., Rao, D., Batey, D. S., … Patrick, D. L. (2015). Patient and provider priorities for self-reported domains of HIV clinical care. AIDS Care, 27(10), 1255–1264.
- Genberg, B. L., Lee, Y., Rogers, W. H., & Wilson, I. B. (2015). Four types of barriers to adherence of antiretroviral therapy are associated with decreased adherence over time. AIDS and Behavior, 19(1), 85–92.
- Golub, S. A., Indyk, D., & Wainberg, M. L. (2006). Reframing HIV adherence as part of the experience of illness. Social Work in Health Care, 42(3-4), 167–188.
- Greenhalgh, J. (2009). The applications of PROs in clinical practice: What are they, do they work, and why? Quality of Life Research, 18(1), 115–123.
- Kalichman, S. C., Kalichman, M. O., & Cherry, C. (2017). Forget about forgetting: Structural barriers and severe non-adherence to antiretroviral therapy. AIDS Care, 29(4), 418–422.
- Kozak, M. S., Mugavero, M. J., Ye, J., Aban, I., Lawrence, S. T., Nevin, C. R., … Willig, J. H. (2012). Patient reported outcomes in routine care: Advancing data capture for HIV cohort research. Clinical Infectious Diseases, 54(1), 141–147.
- Laws, M. B., Beach, M. C., Lee, Y., Rogers, W. H., Saha, S., Korthuis, P. T., … Wilson, I. B. (2013). Provider-patient adherence dialogue in HIV care: Results of a multisite study. AIDS and Behavior, 17(1), 148–159.
- Laws, M. B., Wilson, I. B., Bowser, D. M., & Kerr, S. E. (2000). Taking antiretroviral therapy for HIV infection: Learning from patients’ stories. Journal of General Internal Medicine, 15(12), 848–858.
- Légaré, F., Boivin, A., van der Weijden, T., Pakenham, C., Burgers, J., Légaré, J., … Gagnon, S. (2011). Patient and public involvement in clinical practice guidelines: A knowledge synthesis of existing programs. Medical Decision Making, 31(6), E45–E74.
- Locklear, T., Miriovsky, B. J., Willig, J. H., Staman, K., Bhavsar, N., Weinfurt, K., & Abernethy, A. (n.d.). Strategies for overcoming barriers to the implementation of patient-reported outcomes measures, NIH health care systems research collaboratory patient reported outcomes core white paper. Durham, NC: National Institutes of Health Research, Health Care Systems Collaboratory.
- Mayo, N. E. (2015). ISOQOL dictionary of quality of life and health outcomes measurement (1st ed.). Milwaukee, WI: International Society for Quality of Life Research.
- McHugh, M. L. (2012). Interrater reliability: The kappa statistic. Biochemia Medica, 22(3), 276–282.
- Mills, E. J., Nachega, J. B., Buchan, I., Orbinski, J., Attaran, A., Singh, S., … Bangsberg, D. R. (2006). Adherence to antiretroviral therapy in sub-Saharan frica and North America: A meta-analysis. Journal of the American Medical Association, 296(6), 679–690.
- Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097.
- Munro, S. A., Lewin, S. A., Smith, H. J., Engel, M. E., Fretheim, A., & Volmink, J. (2007). Patient adherence to tuberculosis treatment: A systematic review of qualitative research. Plos Medicine, 4(7), 1230–1245.
- Ortego, C., Huedo-Medina, T. B., Llorca, J., Sevilla, L., Santos, P., Rodríguez, E., … Vejo, J. (2011). Adherence to highly active antiretroviral therapy (HAART): a meta-analysis. AIDS and Behavior, 15(7), 1381–1396.
- Pope, C., & Mays, N. (1995). Qualitative research: Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ, 311(1), 42–45.
- Pound, P., Britten, N., Morgan, M., Yardley, L., Pope, C., Daker-White, G., & Campbell, R. (2005). Resisting medicines: A synthesis of qualitative studies of medicine taking. Social Science and Medicine, 61(1), 133–155.
- Puskas, C. M., Kaida, A., Miller, C. L., Zhang, W., Yip, B., Pick, N., … Hogg, R. S. (2017). The adherence gap: A longitudinal examination of men’s and women’s antiretroviral therapy adherence in British Columbia, 2000-2014. Aids (london, England), 31(6), 827–833.
- Ring, N., Ritchie, K., Mandava, L., & Jepson, R. (2010). A guide to synthesising qualitative research for researchers undertaking health technology assessments and systematic reviews. Retrieved from http://www.nhshealthquality.org/nhsqis/8837.html
- Roberts, K. J. (2000). Barriers to and facilitators of HIV-positive patients’ adherence to antiretroviral treatment regimens. AIDS Patient Care and STDs, 14(3), 155–168.
- Roberts, K. J., & Mann, T. (2003). Adherence to antiretroviral medications in HIV/AIDS care: A narrative exploration of one woman’s foray into intentional nonadherence. Health Care for Women International, 24(6), 552–564.
- Russell, C. K., Bunting, S. M., Graney, M., Hartig, M. T., Kisner, P., & Brown, B. (2003). Factors that influence the medication decision making of persons with HIV/AIDS: A taxonomic exploration. Journal of the Association of Nurses in AIDS Care, 14(4), 46–60.
- Ryan, G. W., & Wagner, G. J. (2003). Pill taking “routinization”: a critical factor to understanding episodic medication adherence. AIDS Care, 15(6), 795–806.
- Schonnesson, L. N., Ross, M. W., & Williams, M. (2004). The HIV medication self-reported nonadherence reasons (SNAR) index and its underlying psychological dimensions. AIDS and Behavior, 8(3), 293–301.
- Shubber, Z., Mills, E. J., Nachega, J. B., Vreeman, R., Freitas, M., Bock, P., … Ford, N. (2016). Patient-reported barriers to adherence to antiretroviral therapy: A systematic review and meta-analysis. PLoS Medicine, 13(11), e1002183.
- Siefried, K. J., Mao, L., Kerr, S., Cysique, L. A., Gates, T. M., McAllister, J., … PAART study investigators. (2017). Socioeconomic factors explain suboptimal adherence to antiretroviral therapy among HIV-infected Australian adults with viral suppression. Plos One, 12(4), e0174613.
- Snyder, C. F., Aaronson, N. K., Choucair, A. K., Elliott, T. E., Greenhalgh, J., Halyard, M. Y., … Santana, M. (2012). Implementing patient-reported outcomes assessment in clinical practice: A review of the options and considerations. Quality of Life Research, 21(8), 1305–1314.
- Suri, H. (2011). Purposeful sampling in qualitative research synthesis. Qualitative Research Journal, 11(2), 63–75.
- Taylor, B. S., Reyes, E., Levine, E. A., Khan, S. Z., Garduno, L. S., Donastorg, Y., … Hirsch, J. S. (2014). Patterns of geographic mobility predict barriers to engagement in HIV care and antiretroviral treatment adherence. AIDS Patient Care and STDs, 28(6), 284–295.
- Toupin, I., Engler, K., Lessard, D., Wong, L., Lènàrt, A., Vicente, S., … Lebouché, B. (2018, April). Canadian HIV clinicians’ perception of barriers to antiretroviral therapy (ART) adherence faced by people living with HIV: A qualitative study. Paper presented at the Canadian association for HIV research conference, Vancouver, BC.
- Truong, W. R., Schafer, J. J., & Short, W. R. (2015). Once-daily, single-tablet regimens for the treatment of HIV-1 infection. Pharmacy and Therapeutics, 40(1), 44–55.
- U.S. Department of Health and Human Services, Food and Drug Administration Center for Drug Evaluation and Research. (2009). Guidance for industry. Patient-reported outcome measures: use in medical product development to support labeling claims.
- U.S. Department of Health and Human Services, Panel on Antiretroviral Guidelines for Adults and Adolescents. (2016). Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Retrieved from http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf
- Vervoort, S. C., Borleffs, J. C., Hoepelman, A. I., & Grypdonck, M. H. (2007). Adherence in antiretroviral therapy: A review of qualitative studies. AIDS, 21(3), 271–281.
- Vervoort, S. C. J. M., Grypdonck, M. H. F., De Grauwe, A., Hoepelman, A. I. M., & Borleffs, J. C. C. (2009). Adherence to HAART: Processes explaining adherence behavior in acceptors and non-acceptors. AIDS Care, 21(4), 431–438.
- Viswanathan, S., Detels, R., Mehta, S. H., Macatangay, B. J. C., Kirk, G. D., & Jacobson, L. P. (2015). Level of adherence and HIV RNA suppression in the current era of highly active antiretroviral therapy (HAART). AIDS and Behavior, 19(4), 601–611.
- Walsh, J. C., Horne, R., Dalton, M., Burgess, A. P., & Gazzard, B. G. (2001). Reasons for non-adherence to antiretroviral therapy: Patients’ perspectives provide evidence of multiple causes. AIDS Care, 13(6), 709–720.
- Warsame, R., & Halyard, M. Y. (2017). Patient-reported outcome measurement in clinical practice: Overcoming challenges to continue progress. Journal of Clinical Pathways, 3(1), 43–46.
- Wilson, I. B., Laws, M. B., Safren, S. A., Lee, Y., Lu, M., Coady, W., … Rogers, W. H. (2010). Provider-focused intervention increases adherence-related dialogue but does not improve antiretroviral therapy adherence in persons with HIV. Journal of Acquired Immune Deficiency Syndromes, 53(3), 338–347.
- Witteveen, E., & Van Ameijden, E. J. C. (2002). Drug users and HIV-combination therapy (HAART): factors which impede or facilitate adherence. Substance Use and Misuse, 37(14), 1905–1925.
- World Economic Situation and Prospects. (2012). Country classification. Retrieved from http://www.un.org/en/development/desa/policy/wesp/wesp_current/2012country_class.pdf
- World Health Organization. (2003). Adherence to long-term therapies: Evidence for action. Geneva: Author.
- World Health Organization. (2016). Global health sector strategy on HIV, 2016-2021. Towards ending AIDS. Geneva: Author.
