
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
The systems framework of resilience has suggested that resilient factors external to or within the individual and their interactions can contribute to positive adjustment in at-risk populations. However, the interplays of resilience resources at different levels have seldom been investigated in health psychology, particularly in people living with HIV/AIDS (PLWHA). This study aimed to examine the mediating role of individual resilience resources in the associations between marital and family relationships and well-being in PLWHA. A sample of 160 Chinese PLWHA were interviewed to complete measures on marital relationship, family relationship, individual resilience resources, and general, physical, and mental well-being. Results showed that better marital relationship and family relationship were associated with higher levels of individual resilience resources and well-being indicators. Mediation analysis with path analysis showed significant mediating effects of individual resilience resources between marital and family relationships and general, physical, and mental well-being. By highlighting marital and family relationships as external resources of resilience and their roles in increasing individual resilience factors which thereby contribute to the well-being of PLWHA, our findings support the systems framework of resilience. There are implications for resilience enhancement interventions with the aim of improving PLWHA’s well-being by including interpersonal strategies of strengthening the protective role of marital and family relationships, which will in turn facilitate the resilience process.
Introduction
Although the recent HIV transmission in China is driven by sexual contacts and intravenous use (NCAIDS, NCSTD, & China CDC, Citation2018), commercial blood donation constituted 19% of confirmed HIV/AIDS cases last decade (State Council AIDS Working Committee Office and UN Theme Group on AIDS in China, Citation2007). Nearly 40,000 people living with HIV/AIDS (PLWHA) were infected via commercial blood donation, with 79% residing in Henan province (Dou et al., Citation2010). This large population clustering in rural areas need public health and mental health care for well-being promotion as they confront various adversities. Most of them engaged in commercial blood donation to ease financial strain (Wu, Liu, & Detels, Citation1995) and were faced with public stigma and unfair health service (Yu, Zhang, & Chan, Citation2016). Therefore, PLWHA in rural China have been reported to have poor well-being (Jin et al., Citation2006; Lau et al., Citation2010; Yu et al., Citation2009). Resilience science has suggested that individuals could achieve positive adaptation despite adversities (Masten, Citation2011). The understanding of pathways leading to resilience in PLWHA in rural China may inform intervention strategies to facilitate better adaptation to contextual adversities in this population.
Resilience refers to the process and the capacity of overcoming adversities and adapting successfully (Luthar, Cicchetti, & Becker, Citation2000; Yates & Masten, Citation2004). Because the coping process involves constant interaction between individuals and their ecological contexts, resilience is distributed across interacting dynamic systems at different levels, including both external and individual levels (Masten, Citation2016). For individual resilience resources, Connor and Davidson (Citation2003) summarized previous findings about the personal characteristics of resilient people and subsequently developed the Connor-Davidson Scale of Resilience to provide a general measure of individual resilience resources, which covers resilient personal qualities such as self-efficacy and acceptance of change. These individual resilience resources have been found to be associated with better adjustment in various at-risk populations(Connor, Davidson, & Lee, Citation2003; Pietrzak, Johnson, Goldstein, Malley, & Southwick, Citation2009; Zhang, Yu, Zhou, & Zhang, Citation2017), including PLWHA in China (Yu, Chen, Ye, Li, & Lin, Citation2016; Yu, Zhang, Chow, Chan, & Chan, Citation2016; Zhang et al., Citation2015). Resilience resources are also external to individuals. Various external resilience factors have been identified, including good relationships, neighborhood characteristics, and institutional support (Fergus & Zimmerman, Citation2005; Masten, Citation2016).
Satisfying close relationships are one of the most important and well-documented external resilience resources. From childhood, close relationships compose the basic social context of life and shape the development of individuals’ adaptive systems, thereby playing an essential role in resilience outcomes under adversity (Masten & Shaffer, Citation2006; Orbuch, Parry, Chesler, Fritz, & Repetto, Citation2005). Mounting evidence has identified the positive link between higher quality close relationships (e.g., marital relationship, family relationship) and better well-being (e.g., fewer psychological symptoms, lower mortality) in at-risk populations (Proulx, Helms, & Buehler, Citation2007; Robles, Slatcher, Trombello, & McGinn, Citation2014), especially in people affected by chronic diseases (Fisher & Weihs, Citation2000; Pruchno, Wilson-Genderson, & Cartwright, Citation2009; Rohrbaugh, Shoham, & Coyne, Citation2006; Rottmann et al., Citation2015). For PLWHA, high-quality close relationships may be particularly important for resilience outcomes. This is because many of them suffer from reduced social connectedness and lack of social support due to the HIV stigma (Emlet, Citation2006; Ware, Wyatt, & Tugenberg, Citation2006), which can undermine their disease management (McDowell & Serovich, Citation2007). As major sources of social support, well-functioning close relationships may make up for the social isolation of PLWHA and facilitate the resilience process. Although close relationship includes various kinds of relationships (e.g., friendships, peer relationships, other social networks), marital relationship and family relationship are particularly significant as they are the major sources for support in rural Chinese families. Due to the strong family orientation in Chinese culture, the family usually undertakes the primary caregiving responsibility for chronic disease patients, including PLWHA (Li, Wu, et al., Citation2006; Parveen & Morrison, Citation2009). As PLWHA age, spouses become even more central in the daily supporting network because children need to establish their own nuclear family (Hoppmann & Gerstorf, Citation2009; Zhang et al., Citation2017). These factors could make high-quality marital and family relationships important external resilience resources for PLWHA in rural China. However, the influence of the quality of these two important close relationships for resilience outcomes in Chinese rural PLWHA have rarely been examined in previous studies.
Although previous studies have well differentiated resilience factors at external and individual levels, interplays among resources of different levels were seldom addressed (Fergus & Zimmerman, Citation2005; Masten, Citation2016), which may create barriers in promoting resilience. The systems framework of resilience argues that instead of contributing to resilience in an isolated way, resources at external and individual levels are interconnected and constantly interacting (Masten, Citation2011, Citation2016). Thus, the benefits of specific resilience factors may spread across levels via the interplays of different systems (Bonanno & Diminich, Citation2013; Masten, Citation2016). Such a cascading effect implicates the significance of including resilient factors in different systems and examining their interplays because a deepened understanding of spreading and interacting effects among these factors could inform cost-effective interventions (Masten, Citation2016). For example, if satisfying marital relationship is found beneficial in building individual resilience resources, interventions to improve marital relationship could be effective. This is because such interventions could not only facilitate individuals’ well-being by improving marital relationship, but also strengthen their internal protective factors and enhance their long-term coping capacity. Therefore, research that goes beyond identifying internal or external resilience factors and addresses how these factors interplay in the resilience process of PLWHA is still needed.
As an important external resilience resource, satisfying close relationships may facilitate the resilience process via building up individual resilience resources within PLWHA. For example, high-quality close relationships could foster a positive self-perception in PLWHA because the acceptance and positive regards entailed in good relationships (Bradbury, Fincham, & Beach, Citation2000) may cultivate a more positive view toward oneself (Swann, Chang-Schneider, & McClarty, Citation2007). Such positivity has been found to counteract stress brought by adversities and facilitate adaptive coping (Connor et al., Citation2003). Moreover, the sense of security brought by good relationships could have a calming effect on individuals’ emotional and physiological systems under stress (Kiecolt-Glaser & Newton, Citation2001), thereby helping to enhance one’s perception of received social support and tendency to quickly engage in effective coping (Uchino, Citation2009). In such a process, one’s efficacy and positive acceptance of challenges, as important individual resilience resources, can be built up (Fletcher & Sarkar, Citation2013). Thus, satisfying close relationships, such as good marital and family relationships, may serve as external factors to facilitate the resilience process in PLWHA in rural China via cultivating resilience factors within the individual.
Conceptual framework
The systems framework of resilience states that resilience builds on interconnected systems and is contingent upon ecological contexts. The resources contributing to the resilience process are distributed at internal and external levels and these resources interact with each other in facilitating the resilience process (Masten, Citation2016). A better understanding about the cross-level interplays would inform the path to resilient outcomes and the direction for intervention development (Masten, Citation2011, Citation2016). Despite acknowledging connectedness among systems in the systems framework of resilience, most existing resilience research in PLWHA investigated either resilience factors within (e.g., Yu, Chen, Ye, Li, & Lin, Citation2016; Zhang et al., Citation2015) or external to the individuals (e.g., McDowell & Serovich, Citation2007; Ware et al., Citation2006). Only a few exceptions included resilience resources at both levels, but examined their separate contributions to resilience process (e.g., Earnshaw, Lang, Lippitt, Jin, & Chaudoir, Citation2015; Yeji et al., Citation2014). These studies did not go beyond identifying specific resilience factors, leaving the cross-level interplays unclear. Thus, this study aimed to concurrently include important external resilience factors (marital relationship and family relationship) and individual resilience factors and examine their interplays in facilitating the resilience process.
We hypothesized that in Chinese rural PLWHA: (1) as external resilience resources, satisfying marital relationship and family relationship will be associated with better well-being; (2) individual resilience resources will be associated with better well-being; and (3) the protective effects of good marital and family relationships on well-being will be mediated by individual resilience resources.
Method
Participants
We randomly selected five villages from among 22 villages where the HIV prevalence is greater than 10% in Henan province, China. A total of 160 PLWHA were recruited in these villages to take part in this study. Inclusion criteria were: (1) being HIV positive and (2) being married for more than five years. The demographic and HIV-related characteristics of participants are displayed in . As shown, most participants were middle-aged with relatively low education and income levels.
Table 1. Demographic and HIV-related characteristics of participants.
Procedure
Due to the low education levels of the participants, local health care service providers with training on conducting psychological surveys interviewed participants with the questionnaires face to face. Participants provided written informed consent to participate in the study after the explanation of interviewers. They received compensation for their time spent on the survey (CNY30, approximately equivalent to USD5). Ethical approval was obtained from the City University of Hong Kong and the Institute of Psychology, Chinese Academy of Sciences.
Measures
We collected participants’ demographic information (including gender, age, education level, duration of marriage, family size, and annual family income) and HIV-related characteristics (including duration of HIV diagnosis, self-reported treatment effect, and self-reported side effects of treatment).
Marital relationship was measured by participants’ rating on a ladder with steps numbered 0 through 10. Zero represents the worst possible relationship, and 10 represents the best possible relationship. Participants indicated which step their marital relationship was placed on (Cantril, Citation1965; Rottmann et al., Citation2015). Such a self-anchoring ladder measure has been previously used in a Chinese sample (Ku, McKenna, & Fox, Citation2007).
Family relationship was measured with the Brief Family Relationship Scale (Fok, Allen, Henry, & Team, Citation2014), which consists of cohesion (7 items, e.g., “In our family there is a feeling of togetherness”), expression (3 items, e.g., “In our family we sometimes tell each other about our personal problems”), and conflict (6 items, e.g., “In our family we argue a lot”) subscales. Participants were asked to indicate whether descriptions of the items were “True” or “False” to them. The items were adapted into Chinese following the translation and back-translation procedure. This measurement showed good internal consistency in this study (α = .85).
Individual resilience resources were measured with the Connor–Davidson Resilience Scale (CD-RISC; Connor & Davidson, Citation2003). The measurement includes 25 items (e.g., “I can deal with whatever comes”). Participants indicated the extent to which they agreed with the items on a 5-point Likert scale. Both the original (Connor & Davidson, Citation2003) and Chinese version (Yu & Zhang, Citation2007) of this measurement showed good psychometric properties. It has also previously been used in Chinese PLWHA (Yu et al., Citation2009). The internal consistency value of the CD-RISC in this study was .89.
General well-being was measured with the 5-item WHO Well-Being Index (WHO-5) (Topp, Østergaard, Søndergaard, & Bech, Citation2015). This measurement consists of five positively phrased items about well-being (e.g., “I have felt cheerful and in good spirits”). Participants were asked to rate how well the items applied to them on a 5-point Likert scale. The WHO-5 has been used in Chinese populations in previous studies (Ng et al., Citation2014). This measurement showed internal consistency in this study (α = .85).
Physical well-being and mental well-being were measured with two items from the Healthy Days Module (Centers for Disease Control and Prevention, Citation2000). Participants reported the number of recent days when their physical health and mental health, separately, was not good. The reported number of physically unhealthy days and mentally unhealthy days represented individuals’ physical well-being and mental well-being, respectively. Fewer unhealthy days indicated better well-being.
Data analysis
Correlation analysis was conducted. To further examine the mediation model, Structural Equation Modelling (SEM) was used as it allows the analyses for latent variables, which can account for measurement error and provide more accurate modeling estimates (Skrondal & Rabe-Hesketh, Citation2004). Due to the limited number of observations in this study, we used item parceling for general well-being, family relationship, and individual resilience resources to reduce the bias in parameters estimations (Hau & Marsh, Citation2004). As marital relationship, physically unhealthy days, and mentally unhealthy days were measured with single-item assessments, these three variables were included in the model as manifest variables instead of latent variables. All analyses were conducted with Mplus 7.0.
Results
Descriptive statistics and correlations of study variables are displayed in . As shown, both marital relationship (r = .26, p < .01) and family relationship (r = .23, p < .01) were significantly correlated with general well-being. A better marital relationship was associated with fewer physically unhealthy days (r = −.29, p < .01) and mentally unhealthy days (r = −.24, p < .01). Similarly, better family relationship was also related to fewer physically (r = −.30, p < .01) and mentally unhealthy days (r = −.27, p < .01). These associations support Hypothesis 1 and suggest direct effects of external resilience factors (marital relationship and family relationship) on well-being. Consistent with Hypothesis 2, individual resilience resources were significantly correlated with better general well-being (r = .40, p < .01), fewer physically unhealthy days (r = −.43, p < .01), and fewer mentally unhealthy days (r = −.31, p < .01). Therefore, we conducted subsequent mediation analysis with path analysis.
Table 2. Descriptive statistics and correlations of study variables.
Results of SEM are displayed in . Model indexes were acceptable, with = 1.95 (p < .05), RMSEA = .07, CFI = .96, TLI = .94, and SRMR = .06. When considering individual resilience resources in the model, the associations between marital relationship and the three well-being indicators were no longer significant. Both marital relationship (
= .35, p < .01) and family relationship (
= .27, p < .01) were associated with higher levels of individual resilience resources. Meanwhile, individual resilience resources were associated with better general well-being (
= .27, p < .05), fewer physically unhealthy days (
= −.25, p < .01), and fewer mentally unhealthy days (
= −.23, p < .05). We compared this model with an alternative model that the three outcome indicators were loaded on a single latent factor of well-being. It showed that this alternative model provided significantly worse fit to the data (
= 169.95,
, p < .01). Thus, we only reported mediation analysis results based on the original model with three separate outcomes.Footnote1
Figure 1. The mediation role of individual resilience resources on well-being.
Notes: *p < .05, **p < .01.
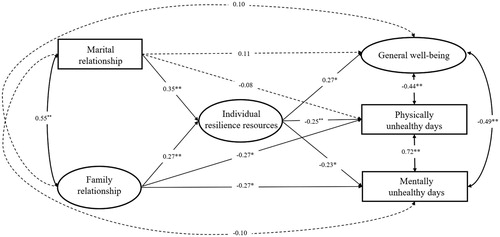
Further mediation analysis with Monte Carlo methods found significant indirect effects of individual resilience resources as the mediator between marital relationship and the three well-being indicators. Individual resilience resources mediated the association between family relationship and general well-being as well as physically unhealthy days significantly, while the mediation effect between individual resilience resources and mentally unhealthy days was marginally significant. The estimated mediation effects are shown in and support Hypothesis 3.
Table 3. Estimated mediation effects of individual resilience resources on well-being.
Discussion
Guided by the systems framework of resilience (Masten, Citation2016), this study aimed to identify resilience resources of PLWHA in rural China, both external to and within the individual, and to examine how they interplay to impact well-being outcomes. By concurrently investigating both external and individual resilience factors, this study managed to address the multi-systemic nature of the resilience process. This study revealed that both external resilience resources (high-quality marital and family relationships) and individual resilience resources were significantly associated with better general well-being, physical well-being, and mental well-being among PLWHA living in rural China. More importantly, the protective effects of marital and family relationships on well-being were mediated by individual resilience resources. Our findings indicate that as external resilience resources, satisfying marital relationship and family relationship benefit PLWHA’s well-being via enhancing individual resilience resources. Consistent with the assumption of the systems framework of resilience (Masten, Citation2011, Citation2016), this study found that both external and internal resilience factors contributed to better adjustment in at-risk populations, and resilience factors in different systems interact with each other in facilitating the resilience process. Our findings make a theoretical contribution to the field by providing evidence for the systems framework of resilience in a stressed Chinese population affected by HIV.
Our findings highlight the protective role of external resilience resources in PLWHA in a rural area of China. Although our study replicated the previous reports on the benefits of individual resilience resources in this population (Yu, Zhang, Chow, et al., Citation2016; Zhang et al., Citation2015), the roles of marital and family relationships as external resilience factors for Chinese PLWHA were neglected in previous studies because they are often described as an isolated population that brings stigma to their close family members (Cao, Sullivan, Xu, & Wu, Citation2006; Li et al., Citation2008). Resilience literature has suggested the importance of close relationships in the resilience process (Fergus & Zimmerman, Citation2005; Masten, Citation2016; Yates & Masten, Citation2004), which has been supported in people affected by non-stigmatized chronic diseases such as cancer and renal disease (Pruchno et al., Citation2009; Rosland & Piette, Citation2010; Rottmann et al., Citation2015). The role of satisfying close relationships as external resilience resources may be further magnified by the context of HIV infection and Chinese culture because they are assumed to provide essential caregiving to the patient in a rural area with limited health care and have the potential to counteract social isolation brought by HIV (Li, Wu, et al., Citation2006; Ware et al., Citation2006). However, because we only examined the role of marital and family relationships as external resilience factors in this study, future studies should consider expanding to investigate other external resources such as health care service accessibility (Coates, Richter, & Caceres, Citation2008) and supportive policies for PLWHA (Mugavero, Norton, & Saag, Citation2011).
In addition to identifying resilience factors in the internal and external systems of focal individuals, this study explored the interplay among resilience factors from different systems in the resilience process, which has seldom been addressed in previous studies. Consistent with our hypothesis, this study found that individual resilience resources mediated the benefits of satisfying marital and family relationships on well-being. Moreover, as demonstrated in footnote, moderation analyses showed that other kinds of interplays (external resources moderating the effects of individual resources on well-being; marital and family relationships interact with each other in building individual resources) were not supported by our data. These results extended our understanding of the resilience process in Chinese PLWHA by clarifying the pathway of how satisfying close relationships in the family context, as important external resilience resources (Masten, Citation2016; Rottmann et al., Citation2015), facilitate positive adaptation under adversity. Our mediation findings are in line with the cascading effects in developmental psychology, which suggest that interplays of different developmental systems can lead to spreading effects across levels (Masten & Cicchetti, Citation2010). Previous studies have identified cascading effects of external factors on internal outcomes (Bonell et al., Citation2014; Rogosch, Oshri, & Cicchetti, Citation2010). For example, better parent–child relationships have been found to contribute to a healthier self-schema and further suppress individuals’ vulnerability to depression (Shah & Waller, Citation2000). Moreover, the elucidation of cascading effects will inform the development of intervention and prevention programs (Bornstein, Hahn, & Haynes, Citation2010; Heckman, Citation2006). For instance, our findings suggest that programs aiming at improving close relationships of PLWHA may not only preserve external resilience resources but also create a positive cascade, improving personal competence to adjust to adversities. In addition, such cascading effects further support the malleability of resilience capacities (Yates & Masten, Citation2004; Yu et al., Citation2014). This suggests that efforts to improve external resilience resources may be translated into promoting individual resilience capacities.
The interplays between external and internal resilience resources may be contingent upon the cultural and social economic context. In this study, with a sample of PLWHA in a rural area of China, we found that the protective effects of satisfying marital and family relationships in well-being were mediated by individual resilience resources, which may be attributed to the relatively strong interdependent self-construal in the Chinese population (Li, Zhang, Bhatt, & Yum, Citation2006; Markus & Kitayama, Citation1991), who tend to define themselves based on close relationships (Aron & Mclaughlin-Volpe, Citation2001). Such tendencies may strengthen the link between satisfying close relationships and personal resilience qualities such as efficacy and positive self-perception, as mentioned above. High-quality marital and family relationships may be particularly important for optimism and tolerance of stress among Chinese rural PLWHA whose perceived support from spouses and family members may be crucial for adversity adjustment due to their poor economic status and limited health service accessibility (Li, Wu, et al., Citation2006; Walsh, Citation2015). Therefore, the interplays between close relationship qualities and individual resilience resources may need validation in different cultural and social economic backgrounds.
There are several limitations to this study. Due to the cross-sectional research design, the associations presented in this study are correlational in nature. The resilience pathway found in this study needs to be confirmed with longitudinal or experimental design in future studies. In addition, because the role of marital relationship was examined, only PLWHA who were married were recruited in this study. The results have yet to be validated in single, bereaved, or divorced PLWHA. Moreover, PLWHA involved in this study were infected with HIV via commercial blood donation. Further studies are still needed to generalize the findings to other populations of PLWHA with different infection modes. Finally, this study relied on self-reported data, which are subject to potential biases, especially when most PLWHA in rural China have received relatively little education. Future studies can consider adopting more objective indicators such as CD4 counts to assess clinical outcomes in this population.
By concurrently including external resilience resources (marital and family relationships) and individual resilience resources, this study has confirmed their protective roles for PLWHA in rural China and indicated the across-level spreading effects of external resilience factors on internal systems. These findings support the systems framework of resilience and clarify the pathways of how close relationships facilitate the resilience process. The results of this study can inform future resilience research, implicating the importance of further examination of cross-level interplays among resilience resources at various levels. Our findings also inform that future intervention programs targeting PLWHA in rural China can use close relationship improvement as one of the intervention strategies to promote individual competence, thereby facilitating the resilience process in this population.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Nancy Xiaonan Yu http://orcid.org/0000-0002-6371-2684
Additional information
Funding
Notes
1 In addition to the mediating effects that close relationships facilitate well-being via enhancing personal resilience, questions remain regarding whether there are other possible interplays between external and individual resilience resources under the systems framework. One possibility is that external resilience resources may moderate with individual resilience resources to impact well-being. Another possibility is that marital relationship and family relationship may interact with each other in building individual resources.
In the first model, we tested that the associations between individual resilience resources and well-being outcomes were moderated by marital relationship and family relationship. Convergence problem occurred before reaching the maximum number of iterations, even after changing starting values. This indicated poor fit of the model and failure of generating estimation of model fit index (Muthén & Muthén, Citation2010). In the second model, we tested that marital relationship, family relationship, and the interaction term of these two variables were associated with individual resilience resources, which predicted well-being outcomes. SEM results of this model demonstrated poor fit index (χ2/df = 11.50 [p < .05], RMSEA = .26, CFI = .69, TLI = .57, and SRMR = .05). Therefore, these two moderation models did not fit the current data.
References
- Aron, A., & Mclaughlin-Volpe, T. (2001). Including others in the self. In Constantine Sedikides, & Marilynn B. Brewer (Eds.), Individual self, relational self, collective self (pp. 125–152). New York, NY: Psychology Press.
- Bonanno, G. A., & Diminich, E. D. (2013). Annual research review: Positive adjustment to adversity -trajectories of minimal-impact resilience and emergent resilience. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 54, 378–401. doi: 10.1111/jcpp.12021
- Bonell, C., Humphrey, N., Fletcher, A., Moore, L., Anderson, R., & Campbell, R. (2014). Why schools should promote students’ health and wellbeing. BMJ, 348, g3078. doi: 10.1136/bmj.g3078
- Bornstein, M. H., Hahn, C.-S., & Haynes, O. M. (2010). Social competence, externalizing, and internalizing behavioral adjustment from early childhood through early adolescence: Developmental cascades. Development and Psychopathology, 22, 717–735. doi: 10.1017/S0954579410000416
- Bradbury, T. N., Fincham, F. D., & Beach, S. R. (2000). Research on the nature and determinants of marital satisfaction: A decade in review. Journal of Marriage and Family, 62, 964–980. doi: 10.1111/j.1741-3737.2000.00964.x
- Cantril, H. (1965). Pattern of human concerns. New Brunswick: Rutgers University Press.
- Cao, X., Sullivan, S. G., Xu, J., & Wu, Z. (2006). Understanding HIV–related stigma and discrimination in a “blameless” population. AIDS Education and Prevention, 18, 518–528. doi: 10.1521/aeap.2006.18.6.518
- Centers for Disease Control and Prevention (CDC). (2000). Measuring healthy days: Population assessment of health-related quality of life. Atlanta: CDC.
- Coates, T. J., Richter, L., & Caceres, C. (2008). Behavioural strategies to reduce HIV transmission: How to make them work better. The Lancet, 372, 669–684. doi: 10.1016/S0140-6736(08)60886-7
- Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depression and Anxiety, 18, 76–82. doi: 10.1002/da.10113
- Connor, K. M., Davidson, J. R., & Lee, L.-C. (2003). Spirituality, resilience, and anger in survivors of violent trauma: A community survey. Journal of Traumatic Stress, 16, 487–494. doi: 10.1023/A:1025762512279
- Dou, Z., Chen, R. Y., Wang, Z., Ji, G., Peng, G., Qiao, X., … Zhang, F. (2010). HIV-Infected former plasma donors in rural central China: From infection to survival outcomes, 1985–2008. PLOS ONE, 5, e13737. doi: 10.1371/journal.pone.0013737
- Earnshaw, V. A., Lang, S. M., Lippitt, M., Jin, H., & Chaudoir, S. R. (2015). HIV stigma and physical health symptoms: Do social support, adaptive coping, and/or identity centrality act as resilience resources? AIDS and Behavior, 19, 41–49. doi: 10.1007/s10461-014-0758-3
- Emlet, C. A. (2006). An examination of the social networks and social isolation in older and younger adults living with HIV/AIDS. Health & Social Work, 31, 299–308. doi: 10.1093/hsw/31.4.299
- Fergus, S., & Zimmerman, M. A. (2005). Adolescent resilience: A framework for understanding healthy development in the face of risk. Annual Review of Public Health, 26, 399–419. doi: 10.1146/annurev.publhealth.26.021304.144357
- Fisher, L., & Weihs, K. L. (2000). Can addressing family relationships improve outcomes in chronic disease? Journal of Family Practice, 49, 561–561.
- Fletcher, D., & Sarkar, M. (2013). Psychological resilience: A review and critique of definitions, concepts and theory. European Psychologist, 18, 12–23. doi: 10.1027/1016-9040/a000124
- Fok, C. C. T., Allen, J., Henry, D., & Team, P. A. (2014). The brief family relationship scale: A brief measure of the relationship dimension in family functioning. Assessment, 21, 67–72. doi: 10.1177/1073191111425856
- Hau, K. T., & Marsh, H. W. (2004). The use of item parcels in structural equation modelling: Non-normal data and small sample sizes. British Journal of Mathematical and Statistical Psychology, 57, 327–351. doi: 10.1111/j.2044-8317.2004.tb00142.x
- Heckman, J. J. (2006). Skill formation and the economics of investing in disadvantaged children. Science, 312, 1900–1902. doi: 10.1126/science.1128898
- Hoppmann, C., & Gerstorf, D. (2009). Spousal interrelations in old age–a mini-review. Gerontology, 55, 449–459. doi: 10.1159/000211948
- Jin, H., Hampton Atkinson, J., Yu, X., Heaton, R. K., Shi, C., Marcotte, T. P., … Grant, I. (2006). Depression and suicidality in HIV/AIDS in China. Journal of Affective Disorders, 94, 269–275. doi: 10.1016/j.jad.2006.04.013
- Kiecolt-Glaser, J. K., & Newton, T. L. (2001). Marriage and health: His and hers. Psychological Bulletin, 127, 472. doi: 10.1037/0033-2909.127.4.472
- Ku, P.-W., McKenna, J., & Fox, K. R. (2007). Dimensions of subjective well-being and effects of physical activity in Chinese older adults. Journal of Aging and Physical Activity, 15, 382–397. doi: 10.1123/japa.15.4.382
- Lau, J., Yu, X., Mak, W., Cheng, Y., Lv, Y., & Zhang, J. (2010). Suicidal ideation among HIV+ former blood and/or plasma donors in rural China. AIDS Care, 22, 946–954. doi: 10.1080/09540120903511016
- Li, L., Wu, Z., Wu, S., Jia, M., Lieber, E., & Lu, Y. (2008). Impacts of HIV/AIDS stigma on family identity and interactions in China. Families, Systems, & Health, 26, 431–442. doi: 10.1037/1091-7527.26.4.431
- Li, L., Wu, S., Wu, Z., Sun, S., Cui, H., & Jia, M. (2006). Understanding family support for people living with HIV/AIDS in Yunnan, China. AIDS and Behavior, 10, 509–517. doi: 10.1007/s10461-006-9071-0
- Li, H. Z., Zhang, Z., Bhatt, G., & Yum, Y.-O. (2006). Rethinking culture and self-construal: China as a middle land. The Journal of Social Psychology, 146, 591–610. doi: 10.3200/SOCP.146.5.591-610
- Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71, 543–562. doi: 10.1111/1467-8624.00164
- Markus, H. R., & Kitayama, S. (1991). Culture and the self: Implications for cognition, emotion, and motivation. Psychological Review, 98, 224–253. doi: 10.1037/0033-295X.98.2.224
- Masten, A. S. (2011). Resilience in children threatened by extreme adversity: Frameworks for research, practice, and translational synergy. Development and Psychopathology, 23, 493–506. doi: 10.1017/S0954579411000198
- Masten, A. S. (2016). Resilience in developing systems: The promise of integrated approaches. European Journal of Developmental Psychology, 13, 297–312. doi: 10.1080/17405629.2016.1147344
- Masten, A. S., & Cicchetti, D. (2010). Developmental cascades. Development and Psychopathology, 22, 491–495. doi: 10.1017/S0954579410000222
- Masten, A. S., & Shaffer, A. (2006). How families matter in child development: Reflections from research on risk and resilience. In Families count: Effects on child and adolescent development (pp. 5–25). New York, NY: Cambridge University Press.
- McDowell, T. L., & Serovich, J. (2007). The effect of perceived and actual social support on the mental health of HIV-positive persons. AIDS Care, 19, 1223–1229. doi: 10.1080/09540120701402830
- Mugavero, M. J., Norton, W. E., & Saag, M. S. (2011). Health care system and policy factors influencing engagement in HIV medical care: Piecing together the fragments of a fractured health care delivery system. Clinical Infectious Diseases, 52, S238–S246. doi: 10.1093/cid/ciq048
- Muthén, L. K., & Muthén, B. O. (2010). Mplus user’s guide, v. 6.1. Los Angeles, CA: Muthen and Muthen, UCLA.
- NCAIDS, NCSTD, & China CDC. (2018). Update on the AIDS/STD epidemic in China in the first quarter of 2018. Chinese Journal of AIDS/STD, 24, 431.
- Ng, S. S. W., Lo, A. W. Y., Leung, T. K. S., Chan, F. S. M., Wong, A. T. Y., Lam, R. W. T., & Tsang, D. K. Y. (2014). Translation and validation of the Chinese version of the short Warwick-Edinburgh mental well-being scale for patients with mental illness in Hong Kong. East Asian Archives of Psychiatry; Aberdeen, 24, 3–9.
- Orbuch, T. L., Parry, C., Chesler, M., Fritz, J., & Repetto, P. (2005). Parent-child relationships and quality of life: Resilience among childhood cancer survivors. Family Relations, 54, 171–183. doi: 10.1111/j.0197-6664.2005.00014.x
- Parveen, S., & Morrison, V. (2009). Predictors of familism in the caregiver role: A pilot study. Journal of Health Psychology, 14, 1135–1143. doi: 10.1177/1359105309343020
- Pietrzak, R. H., Johnson, D. C., Goldstein, M. B., Malley, J. C., & Southwick, S. M. (2009). Psychological resilience and postdeployment social support protect against traumatic stress and depressive symptoms in soldiers returning from operations enduring freedom and Iraqi freedom. Depression and Anxiety, 26, 745–751. doi: 10.1002/da.20558
- Proulx, C. M., Helms, H. M., & Buehler, C. (2007). Marital quality and personal well-being: A meta-analysis. Journal of Marriage and Family, 69, 576–593. doi: 10.1111/j.1741-3737.2007.00393.x
- Pruchno, R., Wilson-Genderson, M., & Cartwright, F. P. (2009). Depressive symptoms and marital satisfaction in the context of chronic disease: A longitudinal dyadic analysis. Journal of Family Psychology, 23, 573. doi: 10.1037/a0015878
- Robles, T. F., Slatcher, R. B., Trombello, J. M., & McGinn, M. M. (2014). Marital quality and health: A meta-analytic review. Psychological Bulletin, 140, 140. doi: 10.1037/a0031859
- Rogosch, F. A., Oshri, A., & Cicchetti, D. (2010). From child maltreatment to adolescent cannabis abuse and dependence: A developmental cascade model. Development and Psychopathology, 22, 883–897. doi: 10.1017/S0954579410000520
- Rohrbaugh, M. J., Shoham, V., & Coyne, J. C. (2006). Effect of marital quality on eight-year survival of patients with heart failure. The American Journal of Cardiology, 98, 1069–1072. doi: 10.1016/j.amjcard.2006.05.034
- Rosland, A.-M., & Piette, J. D. (2010). Emerging models for mobilizing family support for chronic disease management: A structured review. Chronic Illness, 6, 7–21. doi: 10.1177/1742395309352254
- Rottmann, N., Hansen, D. G. A., Larsen, P. V., Nicolaisen, A., Flyger, H., Johansen, C., & Hagedoorn, M. (2015). Dyadic coping within couples dealing with breast cancer: A longitudinal, population-based study. Health Psychology, 34, 486–495. doi: 10.1037/hea0000218
- Shah, R., & Waller, G. (2000). Parental style and vulnerability to depression: The role of core beliefs. The Journal of Nervous and Mental Disease, 188, 19–25. doi: 10.1097/00005053-200001000-00004
- Skrondal, A., & Rabe-Hesketh, S. (2004). Generalized Latent Variable Modeling. New York: Chapman and Hall/CRC.
- State Council AIDS Working Committee Office and UN Theme Group on AIDS in China. (2007). A joint assessment of HIV/AIDS prevention, treatment and care in China. Presented at the State Council AIDS Working Committee Office and UN Theme Group on AIDS in China, Beijing, China.
- SwannJr, W. B., Chang-Schneider, C., & McClarty, K. (2007). Do people’s self-views matter? Self-concept and self-esteem in everyday life. American Psychologist, 62, 84–94. doi: 10.1037/0003-066X.62.2.84
- Topp, C. W., Østergaard, S. D., Søndergaard, S., & Bech, P. (2015). The WHO-5 well-being index: A systematic review of the literature. Psychotherapy and Psychosomatics, 84, 167–176. doi: 10.1159/000376585
- Uchino, B. N. (2009). Understanding the links between social support and physical health: A life-span perspective with emphasis on the separability of perceived and received support. Perspectives on Psychological Science, 4, 236–255. doi: 10.1111/j.1745-6924.2009.01122.x
- Walsh, F. (2015). Strengthening family resilience. New York, NY: Guilford Publications.
- Ware, N. C., Wyatt, M. A., & Tugenberg, T. (2006). Social relationships, stigma and adherence to antiretroviral therapy for HIV/AIDS. AIDS Care, 18, 904–910. doi: 10.1080/09540120500330554
- Wu, Z., Liu, Z., & Detels, R. (1995). HIV-1 infection in commercial plasma donors in China. The Lancet, 346, 61–62. doi: 10.1016/S0140-6736(95)92698-4
- Yates, T. M., & Masten, A. S. (2004). Fostering the future: Resilience theory and the practice of positive psychology. In P. Alex Linley, & Stephen Joseph (Eds.), Positive psychology in practice (pp. 521–539). New Jersey: John Wiley & Sons.
- Yeji, F., Klipstein-Grobusch, K., Newell, M. L., Hirschhorn, L. R., Hosegood, V., & Bärnighausen, T. (2014). Are social support and HIV coping strategies associated with lower depression in adults on antiretroviral treatment? Evidence from rural KwaZulu-Natal, South Africa. AIDS Care, 26, 1482–1489. doi: 10.1080/09540121.2014.931561
- Yu, N. X., Chen, L., Ye, Z., Li, X., & Lin, D. (2016). Impacts of making sense of adversity on depression, posttraumatic stress disorder, and posttraumatic growth among a sample of mainly newly diagnosed HIV-positive Chinese young homosexual men: The mediating role of resilience. AIDS Care, 29, 79–85. doi: 10.1080/09540121.2016.1210073
- Yu, N. X., Lau, J., Mak, W., Cheng, Y., Lv, Y., & Zhang, J. (2009). Risk and protective factors in association with mental health problems among people living with HIV who were former plasma/blood donors in rural China. AIDS Care, 21, 645–654. doi: 10.1080/09540120802459770
- Yu, N. X., Lau, J. T., Mak, W. W., Cheng, Y., Lv, Y., & Zhang, J. (2014). A pilot theory–based intervention to improve resilience, psychosocial well-being, and quality of life among people living with HIV in rural China. Journal of Sex & Marital Therapy, 40, 1–16. doi: 10.1080/0092623X.2012.668512
- Yu, N. X., & Zhang, J. (2007). Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Social Behavior and Personality: An International Journal, 35, 19–30. doi: 10.2224/sbp.2007.35.1.19
- Yu, N. X., Zhang, J., & Chan, C. L. (2016). Health care neglect, perceived discrimination, and dignity-related distress among Chinese patients with HIV. AIDS Education and Prevention, 28, 90–102. doi: 10.1521/aeap.2016.28.1.90
- Yu, N. X., Zhang, J., Chow, A. Y., Chan, C. H., & Chan, C. L. (2016). Fate control and well-being in Chinese rural people living with HIV: Mediation effect of resilience. AIDS Care, 29, 86–90. doi: 10.1080/09540121.2016.1198749
- Zhang, L., Li, X., Qiao, S., Zhou, Y., Shen, Z., Tang, Z., … Stanton, B. (2015). The mediating role of individual resilience resources in stigma-health relationship among people living with HIV in Guangxi, China. AIDS Care, 27, 1–9.
- Zhang, J., Yu, N. X., Zhou, M., & Zhang, J. (2017). Dyadic effects of resilience on well-being in Chinese older couples: Mediating role of spousal support. Journal of Family Psychology, 31, 273–281. doi: 10.1037/fam0000250
