
ABSTRACT
We use a socioecological model of health to define resilience, review the definition and study of resilience among persons living with human immunodeficiency virus (PLWH) in the existing peer-reviewed literature, and discuss the strengths and limitations of how resilience is defined and studied in HIV research. We conducted a review of resilience research for HIV-related behaviors/outcomes of antiretroviral therapy (ART) adherence, clinic attendance, CD4 cell count, viral load, viral suppression, and/or immune functioning among PLWH. We performed searches using PubMed, PsycINFO and Google Scholar databases. The initial search generated 14,296 articles across the three databases, but based on our screening of these articles and inclusion criteria, n = 54 articles were included for review. The majority of HIV resilience research defines resilience only at the individual (i.e., psychological) level or studies individual and limited interpersonal resilience (e.g., social support). Furthermore, the preponderance of HIV resilience research uses general measures of resilience; these measures have not been developed with or tailored to the needs of PLWH. Our review suggests that a socioecological model of health approach can more fully represent the construct of resilience. Furthermore, measures specific to PLWH that capture individual, interpersonal, and neighborhood resilience are needed.
Introduction
People living with human immunodeficiency virus (HIV) (PLWH) continue to face numerous adversities at the individual (e.g., trauma), interpersonal (e.g., stigma), and neighborhood (e.g., socioeconomic deprivation and violence) levels (Dale, Cohen, Weber, et al., Citation2014; Earnshaw, Bogart, Dovidio, & Williams, Citation2013; Fullilove, Citation2006; Latkin, German, Vlahov, & Galea, Citation2013; Nunn et al., Citation2014; Pellowski, Kalichman, Matthews, & Adler, Citation2013). These adversities have been linked to worse health behaviors (e.g., lower HIV medication adherence, poorer clinic attendance) and outcomes (e.g., less viral suppression) (Holtzman, Brady, & Yehia, Citation2015; Howe et al., Citation2014; Langebeek et al., Citation2014; Mugavero, Amico, Horn, & Thompson, Citation2013). Given the adversities faced by PLWH, resilience resources may facilitate good health behaviors and outcomes, potentially enabling PLWH to overcome the negative effects of adversities (De Santis, Florom-Smith, Vermeesch, Barroso, & DeLeon, Citation2013; Earnshaw et al., Citation2013).
While resilience refers to overcoming adversities, it has been defined in multiple ways and mostly as resources related to an individual’s personality characteristics (Bonanno, Citation2004; Connor & Davidson, Citation2003; Leipold & Greve, Citation2009; Luthar, Cicchetti, & Becker, Citation2000; Masten, Citation2001). However, the definition of resilience used in this paper incorporates recent insights from existing resilience literature (Fletcher & Sarkar, Citation2013) and a Socioecological Model of Health (SMH) (Baral, Logie, Grosso, Wirtz, & Beyrer, Citation2013). A SMH posits that health is influenced by factors at the individual, interpersonal, neighborhood, and societal/policy levels (Baral et al., Citation2013). Therefore, a SMH may be beneficial in framing resilience as a multi-component construct with direct relevance to the lives of PLWH.
Based on this SMH framework and previous resilience research, we define resilience resources as positive psychological, behavioral, and/or social adaptation in the face of stressors and adversities (Fletcher & Sarkar, Citation2013) that draws upon “an individual’s capacity, combined with families’ and communities’ resources to overcome serious threats to development and health” (Earnshaw et al., Citation2013; Unger, Citation2008). Resilience resources may protect the health of PLWH via promotion of positive health behaviors (e.g., engagement in care, antiretroviral therapy (ART) adherence) and buffering of adversities (e.g., trauma) on mental health, health behaviors, and physiological functioning (Dale, Cohen, Weber, et al., Citation2014; Emlet, Shiu, Kim, & Fredriksen-Goldsen, Citation2017; O’Leary, Jemmott, Stevens, Rutledge, & Icard, Citation2014; Sauceda, Wiebe, & Simoni, Citation2014; Spies & Seedat, Citation2014). Resilience resources are also viewed here as processes that buffer against and are potentially more malleable to intervention than some of the aforementioned adversities at the individual, interpersonal, and neighborhood levels (Dale, Grimes, Miller, Ursillo, & Drainoni, Citation2016; De Santis et al., Citation2013; Kent, Davis, Stark, & Stewart, Citation2011; Steinhardt & Dolbier, Citation2008).
The multilevel adversities faced by PLWH warrant a multi-component resilience definition and study (i.e., individual, interpersonal, and neighborhood components) to (1) fully understand resilience among PLWH and (2) intervene in a comprehensive manner to promote good health behaviors and outcomes for PLWH. Moreover, a synthesis of the evidence for how a multilevel resilience resource approach has been incorporated into HIV research is needed. Thus, the objectives of this paper are to (1) review the definition and study of resilience resources among PLWH as it relates to important health behaviors and outcomes (i.e., ART adherence, viral suppression, CD4 count, and clinic attendance); (2) identify gaps in the existing literature on resilience and HIV-related health behaviors and outcomes; and (3) provide recommendations for future research. Completing these objectives may inform the design and conduct of multilevel (including structural) interventions to enhance resilience and good behavioral/health outcomes among PLWH and thereby reduce HIV-related morbidity and mortality.
Methods
Search strategy
We performed searches using PubMed, PsycINFO and Google Scholar databases. While we completed unrestricted searches in PubMed and PsycINFO, we limited our examination of Google Scholar records to the first 300; this approach is consistent with best practice guidelines for using Google Scholar to conduct searches of the peer-reviewed literature (Haddaway, Collins, Coughlin, & Kirk, Citation2015). The two first authors (AJD and SKD) identified key search terms based upon expertise in resilience and HIV (Dale, Cohen, Weber, et al., Citation2014; Dale, Cohen, Kelso, et al., Citation2014; Dale et al., Citation2015). We also drew upon the work of Martin, Distelberg, Palmer, and Jeste (Citation2015) that constructed a multilevel resilience measure for low-income families and a multilevel resilience framework for HIV prevention proposed by Herrick, Stall, Goldhammer, Egan, and Mayer (Citation2014). We conducted a Boolean search using the 31 search terms that are listed in .
Table 1. Search terms used in PubMed, PsycINFO and Google scholar.
Inclusion and exclusion criteria
To be eligible for inclusion, the studies had to be published prior to January 1, 2018, in English in a peer-reviewed journal, and used the term “resilience” or included resilience-related key words. Additional inclusion criteria required that the specific HIV-related outcomes were ART adherence, clinic attendance, CD4 cell count, viral load, viral suppression, and/or immune functioning. We excluded studies that included children, did not focus solely on PLWH, focused on measure development, focused on mental health as an outcome, and were interventions and/or housing studies. While it can be argued that housing may represent a neighborhood resilience resource associated with favorable HIV outcomes, we excluded housing studies because a systematic review of housing status and HIV was published recently (see Aidala et al., Citation2016).
Study selection and data extraction
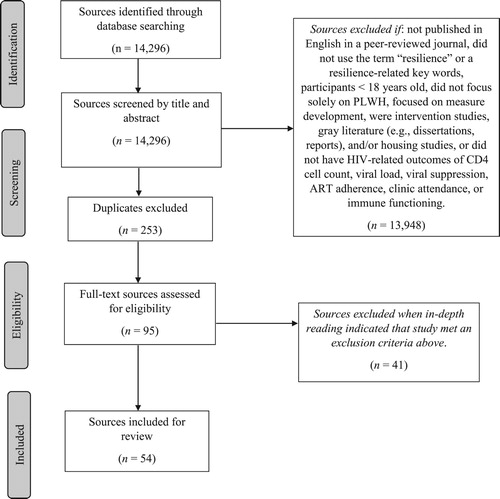
The two first authors and (seven) students/staff members performed initial database searches and selected articles for review. To depict the article selection process (see ), we used a modified PRISMA 2009 Flow Diagram (Moher, Liberati, Tetzlaff, Altman, & Prisma Group, Citation2009). The initial search generated 14,296 articles across the three databases. We then removed the article titles unrelated to HIV n = 13,948 and duplicates n = 253. This resulted in 95 articles eligible for full-text review. Based on our inclusion criteria, n = 54 articles were selected for inclusion and are summarized in Table S1.
Figure 1. PRISMA flow diagram of article review and inclusion.
In the included studies, resilience resources were examined as exposure variables only (n = 30), both exposure and mediator or moderator variables (n = 15), other variables (e.g., mediators, covariates) (n = 4), or as an outcome only (n = 5). Analysis of the included articles is guided by a SMH. For the resilience definition component, we indicate whether the definition is at the individual-, interpersonal-, or neighborhood/community-level only, or whether it is multilevel (i.e., two components or all three components of a SMH included in the definition). Please note that to be consistent with the methods and results from the included studies, we use neighborhood/community-level resilience resources to refer to geographic boundaries. We also used the abovementioned approach to summarize study results of the associations between resilience and the HIV-related outcomes described in the study inclusion criteria.
Study characteristics
The study design and characteristics are presented in Table S1; 31 studies were cross-sectional, 22 were longitudinal, and 1 was a retrospective case–control study. Thirty-two studies were conducted in the U.S. and/or a U.S. territory, 3 were multinational, 3 were from South Africa, 2 were from Kenya, 2 were from India, 2 were from Hong Kong, 1 study was published in Russia, Nepal, England, Mexico, Nigeria, Italy, Sweden, and Malawi, respectively and 2 studies did not report a location.
Results
Definition of resilience resources
Use of the term “resilience.” The majority of articles (50 out of 54; 92.5%) did not mention the construct, “resilience,” or provide a definition. These studies used related terms and constructs such as psychosocial factors, psychological factors, personal resources, protective factors, optimism, hardiness, self-efficacy, spirituality/religiousness, coping, personality state and trait characteristics, and/or social support. Two articles did not include the construct, “resilience,” but the authors provided definitions that aligned with resilience. Three articles mentioned “resilience” and two defined the construct.
Individual Level: Even though Solano et al. (Citation1993) did not mention resilience, they referred to personality characteristics (i.e., fighting spirit or positive mood) in the face of conflict or loss; this aligns with general definitions of trait resilience that have been presented by others (Connor & Davidson, Citation2003; Hu, Zhang, & Wang, Citation2015; Tugade, Fredrickson, & Barrett, Citation2004). O’Cleirigh, Ironson, Weiss, and Costa (Citation2007) mentioned resilience as a mechanism for the protective effects of conscientiousness on health outcomes. In their view, conscientiousness may protect individuals from engaging in health damaging behaviors via active coping and greater resilience to distress; the example of resilience was “less catastrophic disease-related stressor appraisals and lower levels of depressive symptomatology.” Dale, Cohen, Weber, et al. (Citation2014), defined resilience as “a combination of personality characteristics and successful coping that allows an individual to function adaptively in the face of or following adversity.” Pecoraro et al. (Citation2016) defined resilience as the “ability to resist negative psychological responses when confronted with stress or trauma.” Both Dale et al., and Pecoraro et al. (Dale, Cohen, Weber, et al., Citation2014; Pecoraro et al., Citation2016) supplemented their definitions by providing examples of resilience resources at the individual level.
No article included definitions of resilience at interpersonal-, neighborhood/community-, or multi-levels.
Associations between resilience resources and HIV-related outcomes
Individual Level: Ten of the articles examined resilience resources at the individual level. Four of these studies examined ART adherence only. These studies found that higher self-efficacy (Colbert, Sereika, & Erlen, Citation2013; Mo & Mak, Citation2009; Reif et al., Citation2013; Wolf et al., Citation2007) and lower avoidant coping scores (Mo & Mak, Citation2009) were associated positively with ART adherence. Tomakowsky, Lumley, Markowitz, and Frank (Citation2001) examined CD4 cell count as the outcome; they found that explanatory style optimism was predictive of a decline in CD4 cell count.
Five U.S.-based studies examined multiple HIV-related outcomes. These studies found significant relationships between individual-level resilience resources (e.g., patient activation, optimism, conscientiousness) with ART adherence (Marshall et al., Citation2013; Milam, Richardson, Marks, Kemper, & McCutchan, Citation2004), CD4 cell count (Ironson et al., Citation2005; Marshall et al., Citation2013; Milam et al., Citation2004; O’Cleirigh et al., Citation2007); and viral suppression (Ironson et al., Citation2005; Marshall et al., Citation2013; O’Cleirigh et al., Citation2007). Higher Connor-Davidson Resilience Scale scores were associated positively with higher levels of ART adherence and with increased odds of having an undetectable viral load in work by Dale, Cohen, Weber, et al. (Citation2014); these relationships were moderated by histories of abuse.
Interpersonal Level: Fourteen articles examined interpersonal level resilience resources. Six studies examined ART medication adherence as the outcome variable. All of these studies examined social support. General social support was associated positively with ART adherence in the Poudel, Buchanan, Amiya, and Poudel-Tandukar (Citation2015), Afolabi, Afolabi, Afolabi, Odewale, and Olowookere (Citation2013), Huynh, Kinsler, Cunningham, and Sayles (Citation2013), Murphy, Marelich, Hoffman, and Steers (Citation2004), and Power et al. (Citation2003) studies. However, Sodergard et al. (Citation2006) did not find significant associations of social support for medication taking with ART adherence. Additionally, Afolabi et al. (Citation2013) found that those adherent to ART had normal family functioning while Murphy et al. (Citation2004) found that social attachment and reassurance of worth were associated with ART adherence.
The remaining studies examined outcomes such as clinic attendance, viral load, and/or disease progression. In some of these studies, social support was associated with clinic attendance (Waldrop-Valverde, Guo, Ownby, Rodriguez, & Jones, Citation2014) and delayed time to care (McCoy et al., Citation2009). In other studies, there were no significant relationships of social support with ART adherence (Sagarduy, Lopez, Remirez, & Davila, Citation2017), entry into care (Williams, Shahryarinejad, Andrews, & Alcabes, Citation1997), viral load or ART adherence (Attonito, Devieux, Lerner, Hospital, & Rosenberg, Citation2014; Safren et al., Citation2014). However, in the Friedman et al. (Citation2017) study, social support was associated negatively with viral load and in the work of Leserman et al. (Citation2002), less social support predicted HIV disease progression.
Neighborhood/Community-Level: One study examined these resilience resources. Zachariah et al. (Citation2007) found that PLWH who received neighborhood/community-level resilience resources (e.g., community centers, a community health worker) were more likely to be alive and on ART than those residing in communities without these resources.
Multi-level: Twenty-seven articles examined resilience resources at multiple levels.
Individual and Interpersonal Level: Twenty-three studies examined resilience resources at the individual and interpersonal levels; of these, 12 articles examined ART adherence as the only outcome. Some study findings indicated that trait-level control beliefs (Cook, Schmiege, Bradley-Springer, Starr, & Carrington, Citation2017), social support (Catz, Kelly, Bogart, Benotsch, & McAuliffe, Citation2000; Peltzer, Friend-du Preez, Ramlagan, & Anderson, Citation2010), coping self-efficacy (Kamau, Olson, Zipp, & Clark, Citation2011), and treatment self-efficacy (Catz et al., Citation2000; Simoni, Frick, Lockhart, & Liebovitz, Citation2002) were associated positively with medication adherence or time adherence for medication taking. Simoni et al. (Citation2002) also found that treatment self-efficacy mediated the relationship between need for social support and nonadherence to ART. However, Peltzer et al. (Citation2010) found that spirituality exhibited an inverse relationship with ART. The Cha, Erlen, Kim, Sereika, and Caruthers (Citation2008) article tested a model of ART adherence that was also used by Kekwaletswe, Jordaan, Nkosi, and Morojele (Citation2017). Both of the aforementioned studies found indirect associations of social support with ART adherence via medication taking self-efficacy and that self-efficacy mediated the relationship of depression on ART adherence.
The remaining studies that examined ART adherence as the only outcome examined resilience resources such as mood, engagement with medical provider, and social problem solving. Harzke et al. (Citation2004) did not find associations between resilience resources and ART adherence. In contrast, other study findings suggested that control beliefs and social support (Cook, Schmiege, Starr, Carrington, & Bradley-Springer, Citation2017) and social problem solving (Johnson, Elliott, Neilands, Morin, & Chesney, Citation2006) indirectly affected ART adherence via motivation (Cook, Schmiege, Starr, et al., Citation2017) and psychological health (e.g., social provisions and positive states) (Johnson et al., Citation2006). In the study conducted by Luszczynska, Sarkar, and Knoll (Citation2007), finding benefits in being an HIV patient partially mediated the relationship of self-efficacy with ART adherence while self-efficacy mediated associations of social support with ART adherence. Molassiotis et al. (Citation2002) found that some resilience resources were positively (e.g., internal locus of control) or negatively (e.g., family support for medication taking) associated with ART adherence.
Three articles examined resilience resources associated with healthcare engagement among PLWH. These studies suggested that PLWH who were engaged-in-care had higher proactive coping (Pecoraro et al., Citation2016), greater HIV treatment adherence self-efficacy (Chen et al., Citation2013), social support (Colasanti, Stahl, Farber, del Rio, & Armstrong, Citation2017; Pecoraro et al., Citation2016), and more spirituality/religious beliefs (Pecoraro et al., Citation2016). However, Chen et al. (Citation2013) also found that PLWH with better healthcare provider engagement had lower self-esteem.
Two studies, examined immune response (CD4 cell count) as the only outcome. While Trevino et al. (Citation2010) did not find that resilience resources (e.g., positive religious coping, social support) were predictive of CD4, Pandey and Shrivastava (Citation2017) found that social support partially mediated the association between hardiness and higher immune response.
The remaining six articles examined multiple HIV outcomes (e.g., CD4, viral load). In the Weaver et al., article (Citation2005), neither individual (i.e., approach-oriented coping) nor interpersonal (i.e., social support) level resilience were directly associated with medication adherence. Solano et al. (Citation1993) found that fighting spirit was higher in unchanged subjects (i.e., not symptomatic) and that low hardiness predicted a CD4 cell count decrease. Ironson, Stuetzle, and Fletcher (Citation2006) found that spirituality predicted greater preservation of CD4 and better viral load control. Kremer, Ironson, Kaplan, Stuetzle, and Fletcher (Citation2013) found that multiple dimensions of compassionate love (e.g., self) predicted undetectable viral load and CD4 cell count preservation. Turan, Fazeli, Raper, Mugavero, and Johnson (Citation2016) found that an experience sampling method measure of treatment self-efficacy predicted medication adherence, visit adherence, CD4 cell count, and viral load. Additionally, in the work by Thornton et al. (Citation2000) men living with HIV who scored in the lowest tertile of acceptance coping had five-fold greater risk of AIDS-related complex and AIDS diagnosis at follow-up.
Interpersonal- and Neighborhood/Community-Level: Four studies examined interpersonal and neighborhood/community-level resilience resources on ART adherence (n = 3) or CD4 and viral load (n = 1). Regarding ART adherence, neither Kioko and Pertet (Citation2017) nor Bogart et al. (Citation2015) found significant relationships between social support and ART adherence. However, there were associations of structural support interaction with stigma (Bogart et al., Citation2015) and not belonging to an HIV support group (Berg et al., Citation2004) with lower ART adherence. Wouters, Van Damme, Van Loon, van Rensburg, and Meulemans (Citation2009) found that multilevel social support was associated with higher CD4 cell count and viral suppression over time.
Individual-, Interpersonal-, and Neighborhood/Community-Level: Although two studies included resilience resources (e.g., self-efficacy, self-compassion, social support, social capital) at all three levels, only self-efficacy was associated with ART adherence in the studies by Nokes et al. (Citation2012) and Corless et al. (Citation2017).
Discussion
Based on our review of the literature, we conclude that there are significant gaps in the field of HIV resilience research and opportunities to advance scholarship in this area. Specifically, only two studies defined resilience. The common theme across these definitions was the focus on individual-level resilience resources. There is growing criticism that defining resilience exclusively as an individual-level phenomenon ignores the social context and social systems in which resilience may occur (Earnshaw et al., Citation2013; Herrick et al., Citation2014; Shaw, McLean, Taylor, Swartout, & Querna, Citation2016; Unger, Citation2008).
In the commentary of Shaw et al., the authors underscore that the majority of resilience research uses an individual-level definition even though resilience is complex and multilevel. Herrick et al. (Citation2014) propose a multilevel resilience framework for HIV prevention and argue that resilience resources may be important in conferring positive health outcomes to gay and bisexual men who face adversities. This work cites novel resilience resources (e.g., neighborhood affirmation) to support a multilevel definition of resilience. Also, the multilevel nature of resilience is supported by the grounded theoretical approach used by De Santis et al. (Citation2013) to identify intrinsic (e.g., spirituality) and extrinsic (e.g., social support, advocacy) resilience resources among PLWH.
Recent scholarship across a variety of disciplines supports arguments to define resilience at multiple levels of a socioecological model of health. These research findings indicate that resilience resources exist at multiple levels and that each of these levels [(i.e., individual (Davidson et al., Citation2012; Earnshaw et al., Citation2013; Kent et al., Citation2011; Steinhardt, Mamerow, Brown, & Jolly, Citation2009); interpersonal (Earnshaw et al., Citation2013; Steinhardt et al., Citation2009); and neighborhood/community (Earnshaw et al., Citation2013; Herrick et al., Citation2014; Latkin et al., Citation2013)] is important. Given these findings, more studies should include definitions of resilience and should incorporate a socioecological perspective into the definition (Shaw et al., Citation2016).
Almost half of the articles reviewed focused on resilience resources at one level of a socioecological model of health. Of these articles, the majority examined interpersonal resilience resources with general social support being the resilience resource examined most often. While the evidence for associations between social support and viral load was mixed (Attonito et al., Citation2014; Friedman et al., Citation2017), the majority of the aforementioned studies found positive relationships of social support with ART adherence, clinic attendance, and disease progression. In the only study that examined social support specific to chronic disease management, Sodergard et al. (Citation2006) found that social support for medication taking was not associated with ART adherence. The second most frequently examined resilience resource level was the individual level. The majority of these studies examined self-efficacy and found consistent support for this resilience resource on multiple outcomes (i.e., ART adherence, CD4 cell count, and viral suppression). Two studies (Dale, Cohen, Weber, et al., Citation2014; Milam et al., Citation2004) examined other resilience resources, optimism and resilience (Connor-Davidson Resilience Scale), and found support for associations with CD4 cell count, ART adherence, and viral load. Lastly, only one study (Zachariah et al., Citation2007) examined neighborhood/community level resilience resources among PLWH in Africa; and found support for this resilience resource on ART adherence.
The remaining studies used a multilevel resilience resource perspective, with the overwhelming majority examining individual and interpersonal level resilience resources. These studies focused mostly on associations of resilience resources such as coping, self-efficacy, control beliefs, and social support with ART adherence. Although the findings regarding the aforementioned relationships were mixed [(e.g., (Harzke et al., Citation2004; Simoni et al., Citation2002)], the majority of the findings supported associations between social support and ART adherence [e.g., (Kekwaletswe et al., Citation2017; Peltzer et al., Citation2010)]. Some of the longitudinal findings indicated that control beliefs (Cook, Schmiege, Bradley-Springer, et al., Citation2017), social support (Cook, Schmiege, Bradley-Springer, et al., Citation2017) and self-efficacy for medication taking (Cha et al., Citation2008) predicted ART adherence. Some studies examining ART included other resilience resources such as medical provider communication, positive feelings, and managing mood; again there was mixed support for associations between these resilience resources and ART adherence [e.g., (Harzke et al., Citation2004; Molassiotis et al., Citation2002)]. The majority of the studies that looked at multiple HIV outcomes were longitudinal in nature. Findings from these studies indicated that resilience resources such as social support, hardiness, optimism, spirituality, compassionate love, and proactive coping, predicted CD4 cell count (Ironson et al., Citation2006; Kremer et al., Citation2013; Solano et al., Citation1993) and lower viral load (Ironson et al., Citation2006; Kremer et al., Citation2013). Another longitudinal study found that treatment self-efficacy also predicted medication adherence, visit adherence, CD4 cell count, and viral load (Turan et al., Citation2016). Three of the studies examined resilience resources that were associated with healthcare engagement and found that individual and interpersonal resources were critical to remaining engaged-in-care (Chen et al., Citation2013; Colasanti et al., Citation2017; Pecoraro et al., Citation2016).
Of the multilevel resilience resource studies, four included both interpersonal- and neighborhood/community-level resilience resources; the findings from these studies were mixed with regard to ART adherence or viral load and CD4 [e.g., (Kioko & Pertet, Citation2017; Wouters et al., Citation2009)]. Only two studies (Corless et al., Citation2017; Nokes et al., Citation2012) examined individual, interpersonal, and neighborhood/community-level resilience resources. In these two studies, only adherence self-efficacy was associated with ART adherence. However, in the work of Nokes et al. (Citation2012), it appears that social support and social capital were combined in analyses which may limit the interpretability of their findings.
Although this review included a large number of research studies, there remain opportunities for future HIV resilience research. These include examining resilience from a multilevel perspective, developing multilevel resilience measures tailored to PLWH, and examining adversities other than HIV. Although many studies examine multilevel resilience resources, 23 of the 27 studies focus on individual and interpersonal resilience resources. Few studies examine both interpersonal and neighborhood/community resilience resources or resilience resources at all three levels. Also, the majority of the studies included in the review overwhelmingly include general measures of interpersonal resilience resources that are not specific to living with HIV or focus on individual-level resilience resources while excluding potential neighborhood/community resilience resources. The studies that do include resilience resources specific to living with HIV mostly examine HIV-specific self-efficacy measures [(e.g., (Nokes et al., Citation2012; Wolf et al., Citation2007)]; very few studies include measures of social support specifically for PLWH or include neighborhood/community-level resilience resources specific to PLWH. While there are some published studies that have developed measures specific to PLWH, these studies mostly include measures developed at the individual level (e.g., HIV Self-Efficacy, health-related resilience, treatment optimism) (Brennan et al., Citation2009; Erlen, Cha, Kim, Caruthers, & Sereika, Citation2010; Renwick, Halpen, Rudman, & Friedland, Citation1999) while a few measure social support for PLWH (Cortes, Hunt, & McHale, Citation2014).
Qualitative studies of resilience among PLWH highlight the limitations of existing quantitative studies and extant measures (Bartone, Ursano, Wright, & Ingraham, Citation1989; Connor & Davidson, Citation2003; Wagnild & Young, Citation1993). Qualitative findings indicate that among PLWH, mastery for management of HIV is important but absent from most resilience measures (Emlet, Tozay, & Raveis, Citation2011; Hussen et al., Citation2014; Kaplan et al., Citation2014; Teti, French, Bonney, & Lightfoot, Citation2015). Other studies suggest that interpersonal resilience components (e.g., HIV support groups and relationships with healthcare professionals) are important but are excluded from most measures (Emlet et al., Citation2011; Hussen et al., Citation2014; Kaplan et al., Citation2014; Teti et al., Citation2015), or need further development as evidenced by the limited inclusion of social support specific for PLWH in the reviewed studies (Molassiotis et al., Citation2002; Sodergard et al., Citation2006). Neighborhood social capital (e.g., availability of clinics that distribute equipment and financial vouchers, and availability of supportive organizations for PLWH) may also be critical to fostering positive adaptation to adversities (Emlet et al., Citation2011; Hussen et al., Citation2014; Kaplan et al., Citation2014; Tariq et al., Citation2016; Teti et al., Citation2015), yet these components have been excluded from the most used resilience measures. The qualitative findings indicate the need for resilience measures that are better tailored to HIV-related resilience resources. Additionally, most studies included in this review focused only on living with HIV as the adversity. PLWH encounter multiple adversities and future studies should consider the relationships and interactions between these different types of adversities and resilience resources with HIV-related health behaviors and outcomes. Taken together, these research gaps suggest that definitions of resilience as multilevel resources, multilevel resilience measures specific to PLWH, and examination of additional adversities are warranted.
Limitations
Our review sheds light on gaps within the literature regarding how resilience has been defined and studied among PLWH in relation to HIV health behaviors and outcomes; nonetheless, there are a few limitations. First, our review excluded studies of children and adolescents and given that their lives and experiences are often examined within the context of their families and neighborhood/community systems (e.g., schools), perhaps a broader review would have yielded additional insights about resilience at the interpersonal and neighborhood/community levels [e.g., see (Betancourt, Meyers-Ohki, Charrow, & Hansen, Citation2013)]. Second, we did not include “medical care” in our search term and may have missed some multilevel resilience studies; however, many of the studies identified using the search criteria referred to engagement in care (i.e., medical care). Also, we did not include other outcomes such as mental health or quality of life; these studies may have included multilevel approaches to resilience. Despite these limitations, our review provides implications for next steps in advancing the study, definition, and measurement of resilience among PLWH.
Conclusions
PLWH face multiple adversities and resilience resources at the individual, interpersonal, and neighborhood/community levels may be important in helping them to thrive with good health behaviors and outcomes despite these adversities. However, the overwhelming focus on individual-level resilience resources in studies among PLWH misses the opportunities to understand fully the range of resilience resources at the interpersonal and neighborhood/community levels that may be pivotal in empowering PLWH to adapt positively and strive in the face of adversity. Using a SMH to guide the study of resilience is likely to advance the understanding of resilience resources among PLWH and inform interventions to enhance their resilience.
Supplemental Material
Download MS Word (151 KB)Acknowledgements
The authors thank Rashid Ahmed, Caile Criscione, Alexandra Fortune, Chelsea Phou, Rachelle Reid, Sherene Saundes, and Jeremy Wang for their assistance with conducting the literature searches.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Michael P. Carey http://orcid.org/0000-0003-4652-964X
Additional information
Funding
References
- Afolabi, B. A., Afolabi, M. O., Afolabi, A. A., Odewale, M. A., & Olowookere, S. A. (2013). Roles of family dynamics on adherence to highly active antiretroviral therapy among people living with HIV/AIDS at a tertiary hospital in Osogbo, South-West Nigeria. African Health Sciences, 13(4), 920–926. doi: 10.4314/ahs.v13i4.9
- Aidala, A. A., Wilson, M. G., Shubert, V., Gogolishvili, D., Globerman, J., Rueda, S., … Rourke, S. B. (2016). Housing status, medical care, and health outcomes among people living with HIV/AIDS: A systematic review. American Journal of Public Health, 106(1), e1–e23. doi: 10.2105/AJPH.2015.302905
- Attonito, J., Devieux, J. G., Lerner, B. D., Hospital, M. M., & Rosenberg, R. (2014). Antiretroviral treatment adherence as a mediating factor between psychosocial variables and HIV viral load. Journal of the Association of Nurses in AIDS Care, 25(6), 626–637. doi: 10.1016/j.jana.2014.08.001
- Baral, S., Logie, C. H., Grosso, A., Wirtz, A. L., & Beyrer, C. (2013). Modified social ecological model: A tool to guide the assessment of the risks and risk contexts of HIV epidemics. BMC Public Health, 13, S293. doi: 10.1186/1471-2458-13-482
- Bartone, P. T., Ursano, R. J., Wright, K. M., & Ingraham, L. H. (1989). The impact of a military air disaster on the health of assistance workers. A prospective study. The Journal of Nervous and Mental Disease, 177(6), 317–328.
- Berg, K. M., Demas, P. A., Howard, A. A., Schoenbaum, E. E., Gourevitch, M. N., & Arnsten, J. H. (2004). Gender differences in factors associated with adherence to antiretroviral therapy. Journal of General Internal Medicine, 19(11), 1111–1117. doi: 10.1111/j.1525-1497.2004.30445.x
- Betancourt, T. S., Meyers-Ohki, S. E., Charrow, A., & Hansen, N. (2013). Annual research review: Mental health and resilience in HIV/AIDS-affected children – a review of the literature and recommendations for future research. Journal of Child Psychology and Psychiatry, 54(4), 423–444. doi: 10.1111/j.1469-7610.2012.02613.x
- Bogart, L. M., Wagner, G. J., Green, H. D., Jr., Mutchler, M. G., Klein, D. J., & McDavitt, B. (2015). Social network characteristics moderate the association between stigmatizing attributions about HIV and non-adherence among black Americans living with HIV: A longitudinal assessment. Annals of Behavioral Medicine, 49(6), 865–872. doi: 10.1007/s12160-015-9724-1
- Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? American Psychologist, 59(1), 20–28. doi: 10.1037/0003-066X.59.1.20
- Brennan, D. J., Welles, S. L., Miner, M. H., Ross, M. W., Mayer, K. H., Rosser, B. R., & The Positive Connections Team. (2009). Development of a treatment optimism scale for HIV-positive gay and bisexual men. AIDS Care, 21(9), 1090–1097. doi: 10.1080/09540120802705859
- Catz, S. L., Kelly, J. A., Bogart, L. M., Benotsch, E. G., & McAuliffe, T. L. (2000). Patterns, correlates, and barriers to medication adherence among persons prescribed new treatments for HIV disease. Health Psychology, 19(2), 124–133. doi: 10.1037/0278-6133.19.2.124
- Cha, E., Erlen, J. A., Kim, K. H., Sereika, S. M., & Caruthers, D. (2008). Mediating roles of medication-taking self-efficacy and depressive symptoms on self-reported medication adherence in persons with HIV: A questionnaire survey. International Journal of Nursing Studies, 45(8), 1175–1184. doi: 10.1016/j.ijnurstu.2007.08.003
- Chen, W. T., Wantland, D., Reid, P., Corless, I. B., Eller, L. S., Iipinge, S., … Webel, A. R. (2013). Engagement with health care providers affects self- efficacy, self-esteem, medication adherence and quality of life in people living with HIV. Journal of AIDS and Clinical Research, 4(11), 256. doi: 10.4172/2155-6113.1000256
- Colasanti, J., Stahl, N., Farber, E. W., del Rio, C., & Armstrong, W. S. (2017). An exploratory study to assess individual and structural level barriers associated with poor retention and re-engagement in care among persons living with HIV/AIDS. JAIDS Journal of Acquired Immune Deficiency Syndromes, 74, S113–S120. doi: 10.1097/Qai.0000000000001242
- Colbert, A. M., Sereika, S. M., & Erlen, J. A. (2013). Functional health literacy, medication-taking self-efficacy and adherence to antiretroviral therapy. Journal of Advanced Nursing, 69(2), 295–304. doi: 10.1111/j.1365-2648.2012.06007.x
- Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18(2), 76–82. doi: 10.1002/da.10113
- Cook, P. F., Schmiege, S. J., Bradley-Springer, L., Starr, W., & Carrington, J. M. (2017). Motivation as a mechanism for daily experiences’ effects on HIV medication adherence. Journal of the Association of Nurses in AIDS Care, doi: 10.1016/j.jana.2017.09.003
- Cook, P. F., Schmiege, S. J., Starr, W., Carrington, J. M., & Bradley-Springer, L. (2017). Prospective state and trait predictors of daily medication adherence behavior in HIV. Nursing Research, 66(4), 275–285. doi: 10.1097/Nnr.0000000000000216
- Corless, I. B., Hoyt, A. J., Tyer-Viola, L., Sefcik, E., Kemppainen, J., Holzemer, W. L., … Nicholas, P. K. (2017). 90-90-90-plus: maintaining adherence to antiretroviral therapies. AIDS Patient Care and STDs, 31(5), 227–236. doi: 10.1089/apc.2017.0009
- Cortes, A., Hunt, N., & McHale, S. (2014). Development of the scale of perceived social support in HIV (PSS-HIV). AIDS and Behavior, 18(12), 2274–2284. doi: 10.1007/s10461-014-0902-0
- Dale, S. K., Cohen, M. H., Kelso, G. A., Cruise, R. C., Weber, K. M., Watson, C., … Brody, L. R. (2014). Resilience among women with HIV: Impact of silencing the self and socioeconomic factors. Sex Roles, 70(5-6), 221–231. doi: 10.1007/s11199-014-0348-x
- Dale, S., Cohen, M., Weber, K., Cruise, R., Kelso, G., & Brody, L. (2014). Abuse and resilience in relation to HAART medication adherence and HIV viral load among women with HIV in the United States. AIDS Patient Care and STDs, 28(3), 136–143. doi: 10.1089/apc.2013.0329
- Dale, S. K., Grimes, T., Miller, L., Ursillo, A., & Drainoni, M. L. (2016). “In our stories”: The perspectives of women living with HIV on an evidence-based group intervention. J Health Psychology, doi: 10.1177/1359105315622558
- Dale, S. K., Weber, K. M., Cohen, M. H., Kelso, G. A., Cruise, R. C., & Brody, L. R. (2015). Resilience moderates the association between childhood sexual abuse and depressive symptoms among women with and at-risk for HIV. AIDS and Behavior, 19(8), 1379–1387. doi: 10.1007/s10461-014-0855-3
- Davidson, J., Stein, D. J., Rothbaum, B. O., Pedersen, R., Szumski, A., & Baldwin, D. S. (2012). Resilience as a predictor of treatment response in patients with posttraumatic stress disorder treated with venlafaxine extended release or placebo. Journal of Psychopharmacology, 26(6), 778–783. doi: 10.1177/0269881111413821
- De Santis, J. P., Florom-Smith, A., Vermeesch, A., Barroso, S., & DeLeon, D. A. (2013). Motivation, management, and mastery: A theory of resilience in the context of HIV infection. Journal of the American Psychiatric Nurses Association, 19(1), 36–46. doi: 10.1177/1078390312474096
- Earnshaw, V. A., Bogart, L. M., Dovidio, J. F., & Williams, D. R. (2013). Stigma and racial/ethnic HIV disparities: Moving toward resilience. American Psychologist, 68(4), 225–236. doi: 210.1037/a0032705
- Emlet, C. A., Shiu, C., Kim, H. J., & Fredriksen-Goldsen, K. (2017). Bouncing back: Resilience and mastery among HIV-positive older gay and bisexual men. The Gerontologist, 57(Suppl. 1), S40–S49. doi: 10.1093/geront/gnw171
- Emlet, C. A., Tozay, S., & Raveis, V. H. (2011). “I’m not going to die from the AIDS”: Resilience in aging with HIV disease. The Gerontologist, 51(1), 101–111. doi: 10.1093/geront/gnq060
- Erlen, J. A., Cha, E. S., Kim, K. H., Caruthers, D., & Sereika, S. M. (2010). The HIV medication taking self-efficacy scale: Psychometric evaluation. Journal of Advanced Nursing, 66(11), 2560–2572. doi: 10.1111/j.1365-2648.2010.05400.x
- Fletcher, D., & Sarkar, M. (2013). Psychological resilience: A review and critique of definitions, concepts and theory. European Psychologist, 18, 12–23.
- Friedman, M. R., Coulter, R. W., Silvestre, A. J., Stall, R., Teplin, L., Shoptaw, S., … Plankey, M. W. (2017). Someone to count on: Social support as an effect modifier of viral load suppression in a prospective cohort study. AIDS Care, 29(4), 469–480. doi: 10.1080/09540121.2016.1211614
- Fullilove, R. E. (2006). African Americans, health disparities and HIV/AIDS: Recommendations for confronting the epidemic in black America. Retrieved from http://nmac.org/wp-content/uploads/2012/08/African-American-health-disparities-and-HIV-AIDS.pdf
- Haddaway, N. R., Collins, A. M., Coughlin, D., & Kirk, S. (2015). The role of Google scholar in evidence reviews and its applicability to grey literature searching. Plos One, 10(9), e0138237. doi: 10.1371/journal.pone.0138237
- Harzke, A. J., Williams, M. L., Nilsson-Schonnesson, L., Ross, M. W., Timpson, S., & Keel, K. B. (2004). Psychosocial factors associated with adherence to antiretroviral medications in a sample of HIV-positive African American drug users. AIDS Care, 16(4), 458–470. doi: 10.1080/09540120410001683394
- Herrick, A. L., Stall, R., Goldhammer, H., Egan, J. E., & Mayer, K. H. (2014). Resilience as a research framework and as a cornerstone of prevention research for gay and bisexual men: Theory and evidence. AIDS and Behavior, 18(1), 1–9. doi: 10.1007/s10461-012-0384-x
- Holtzman, C. W., Brady, K. A., & Yehia, B. R. (2015). Retention in care and medication adherence: Current challenges to antiretroviral therapy success. Drugs, 75(5), 445–454. doi: 410.1007/s40265-40015-40373-40262
- Howe, C. J., Cole, S. R., Napravnik, S., Kaufman, J. S., Adimora, A. A., Elston, B., … Mugavero, M. J. (2014). The role of at-risk alcohol/drug use and treatment in appointment attendance and virologic suppression among HIV+ African Americans. AIDS Research and Human Retroviruses, 30(3), 233–240.
- Hu, T. Q., Zhang, D. J., & Wang, J. L. (2015). A meta-analysis of the trait resilience and mental health. Personality and Individual Differences, 76, 18–27. doi: 10.1016/j.paid.2014.11.039
- Hussen, S. A., Tsegaye, M., Argaw, M. G., Andes, K., Gilliard, D., & del Rio, C. (2014). Spirituality, social capital and service: Factors promoting resilience among expert patients living with HIV in Ethiopia. Global Public Health, 9(3), 286–298. doi:210.1080/17441692.17442014.17880501. Epub 17442014 Feb 17441613.
- Huynh, A. K., Kinsler, J. J., Cunningham, W. E., & Sayles, J. N. (2013). The role of mental health in mediating the relationship between social support and optimal ART adherence. AIDS Care, 25(9), 1179–1184. doi: 10.1080/09540121.2012.752787
- Ironson, G., Balbin, E., Stuetzle, R., Fletcher, M. A., O’Cleirigh, C., Laurenceau, J. P., … Solomon, G. (2005). Dispositional optimism and the mechanisms by which it predicts slower disease progression in HIV: Proactive behavior, avoidant coping, and depression. International Journal of Behavioral Medicine, 12(2), 86–97. doi: 10.1207/s15327558ijbm1202_6
- Ironson, G., Stuetzle, R., & Fletcher, M. A. (2006). An increase in religiousness/spirituality occurs after HIV diagnosis and predicts slower disease progression over 4 years in people with HIV. Journal of General Internal Medicine, 21, S62–S68. doi: 10.1111/j.1525-1497.2006.00642.x
- Johnson, M. O., Elliott, T. R., Neilands, T. B., Morin, S. F., & Chesney, M. A. (2006). A social problem-solving model of adherence to HIV medications. Health Psychology, 25(3), 355–363. doi: 10.1037/0278-6133.25.3.355
- Kamau, T. M., Olson, V. G., Zipp, G. P., & Clark, M. (2011). Coping self-efficacy as a predictor of adherence to antiretroviral therapy in men and women living with HIV in Kenya. AIDS Patient Care and STDs, 25(9), 557–561. doi: 10.1089/apc.2011.0125
- Kaplan, R. L., Wagner, G. J., Nehme, S., Aunon, F., Khouri, D., & Mokhbat, J. (2014). Forms of safety and their impact on health: An exploration of HIV/AIDS-related risk and resilience among trans women in Lebanon. Health Care for Women International, 3, 3.
- Kekwaletswe, C. T., Jordaan, E., Nkosi, S., & Morojele, N. K. (2017). Social support and the mediating roles of alcohol use and adherence self-efficacy on antiretroviral therapy (ART) adherence among ART recipients in Gauteng, South Africa. AIDS and Behavior, 21(7), 1846–1856. doi: 10.1007/s10461-016-1595-3
- Kent, M., Davis, M. C., Stark, S. L., & Stewart, L. A. (2011). A resilience-oriented treatment for posttraumatic stress disorder: Results of a preliminary randomized clinical trial. Journal of Traumatic Stress, 24(5), 591–595. doi:510.1002/jts.20685. Epub 22011 Sep 20682.
- Kioko, M. T., & Pertet, A. M. (2017). Factors contributing to antiretroviral drug adherence among adults living with HIV or AIDS in a Kenyan rural community. African Journal of Primary Health Care & Family Medicine, 9(1), e1–e7. doi: 10.4102/phcfm.v9i1.1343
- Kremer, H., Ironson, G., Kaplan, L., Stuetzle, R., & Fletcher, M. A. (2013). Compassionate love as a predictor of reduced HIV disease progression and transmission risk. Evidence-Based Complementary and Alternative Medicine, 2013, 1–13. doi: 10.1155/2013/819021
- Langebeek, N., Gisolf, E. H., Reiss, P., Vervoort, S. C., Hafsteinsdottir, T. B., Richter, C., … Nieuwkerk, P. T. (2014). Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: A meta-analysis. BMC Medicine, 12, e438. doi: 10.1186/preaccept-1453408941291432
- Latkin, C. A., German, D., Vlahov, D., & Galea, S. (2013). Neighborhoods and HIV: A social ecological approach to prevention and care. American Psychologist, 68(4), 210–224. doi: 210.1037/a0032704
- Leipold, B., & Greve, W. (2009). Resilience a conceptual bridge between coping and development. European Psychologist, 14(1), 40–50. doi: 10.1027/1016-9040.14.1.40
- Leserman, J., Petitto, J. M., Gu, H., Gaynes, B. N., Barroso, J., Golden, R. N., … Evans, D. L. (2002). Progression to AIDS, a clinical AIDS condition and mortality: Psychosocial and physiological predictors. Psychological Medicine, 32(6), 1059–1073.
- Luszczynska, A., Sarkar, Y., & Knoll, N. (2007). Received social support, self-efficacy, and finding benefits in disease as predictors of physical functioning and adherence to antiretroviral therapy. Patient Education and Counseling, 66(1), 37–42. doi: 10.1016/j.pec.2006.10.002
- Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543–562.
- Marshall, R., Beach, M. C., Saha, S., Mori, T., Loveless, M. O., Hibbard, J. H., … Korthuis, P. T. (2013). Patient activation and improved outcomes in HIV-infected patients. Journal of General Internal Medicine, 28(5), 668–674. doi: 10.1007/s11606-012-2307-y
- Martin, A. S., Distelberg, B., Palmer, B. W., & Jeste, D. V. (2015). Development of a new multidimensional individual and interpersonal resilience measure for older adults. Aging and Mental Health, 19(1), 32–45. doi: 10.1080/13607863.2014.909383
- Masten, A. S. (2001). Ordinary magic: Resilience processes in development. American Psychologist, 56(3), 227–238.
- McCoy, S. I., Strauss, R. P., MacDonald, P. D., Leone, P. A., Eron, J. J., & Miller, W. C. (2009). Social support and delays seeking care after HIV diagnosis, North Carolina, 2000–2006. AIDS Care, 21(9), 1148–1156. doi: 10.1080/09540120902730021
- Milam, J. E., Richardson, J. L., Marks, G., Kemper, C. A., & McCutchan, A. J. (2004). The roles of dispositional optimism and pessimism in HIV disease progression. Psychology & Health, 19(2), 167–181. doi: 10.1080/08870440310001652696
- Mo, P. K., & Mak, W. W. (2009). Intentionality of medication non-adherence among individuals living with HIV/AIDS in Hong Kong. AIDS Care, 21(6), 785–795. doi: 10.1080/09540120802511968
- Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Prisma Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Journal of Clinical Epidemiology, 62(10), 1006–1012. doi: 10.1016/j.jclinepi.2009.06.005
- Molassiotis, A., Nahas-Lopez, V., Chung, W. Y., Lam, S. W., Li, C. K., & Lau, T. F. (2002). Factors associated with adherence to antiretroviral medication in HIV-infected patients. International Journal of STD & AIDS, 13(5), 301–310. doi: 10.1258/0956462021925117
- Mugavero, M. J., Amico, K. R., Horn, T., & Thompson, M. A. (2013). The state of engagement in HIV care in the United States: From cascade to continuum to control. Clinical Infectious Diseases, 57(8), 1164–1171. doi:1110.1093/cid/cit1420. Epub 2013 Jun 1123.
- Murphy, D. A., Marelich, W. D., Hoffman, D., & Steers, W. N. (2004). Predictors of antiretroviral adherence. AIDS Care, 16(4), 471–484. doi: 10.1080/09540120410001683402
- Nokes, K., Johnson, M. O., Webel, A., Rose, C. D., Phillips, J. C., Sullivan, K., … Holzemer, W. L. (2012). Focus on increasing treatment self-efficacy to improve human immunodeficiency virus treatment adherence. Journal of Nursing Scholarship, 44(4), 403–410. doi: 10.1111/j.1547-5069.2012.01476.x
- Nunn, A., Yolken, A., Cutler, B., Trooskin, S., Wilson, P., Little, S., & Mayer, K. (2014). Geography should not be destiny: Focusing HIV/AIDS implementation research and programs on microepidemics in US neighborhoods. American Journal of Public Health, 104(5), 775–780. doi: 10.2105/AJPH.2013.301864
- O’Cleirigh, C., Ironson, G., Weiss, A., & Costa, P. T. (2007). Conscientiousness predicts disease progression (CD4 number and viral load) in people living with HIV. Health Psychology, 26(4), 473–480. doi: 10.1037/0278-6133.26.4.473
- O’Leary, A., Jemmott, J. B., III., Stevens, R., Rutledge, S. E., & Icard, L. D. (2014). Optimism and education buffer the effects of syndemic conditions on HIV status among African American men who have sex with men. AIDS and Behavior, 18(11), 2080–2088. doi: 2010.1007/s10461-10014-10708-10460
- Pandey, D., & Shrivastava, P. (2017). Mediation effect of social support on the association between hardiness and immune response. Asian Journal of Psychiatry, 26, 52–55. doi: 10.1016/j.ajp.2017.01.022
- Pecoraro, A., Pacciolla, A., O’Cleirigh, C., Mimiaga, M., Kwiatek, P., Blokhina, E., … Woody, G. E. (2016). Proactive coping and spirituality among patients who left or remained in antiretroviral treatment in St Petersburg, Russian Federation. AIDS Care, 28(3), 334–338. doi: 10.1080/09540121.2015.1096895
- Pellowski, J. A., Kalichman, S. C., Matthews, K. A., & Adler, N. (2013). A pandemic of the poor: Social disadvantage and the U.S. HIV epidemic. American Psychologist, 68(4), 197–209. doi: 110.1037/a0032694
- Peltzer, K., Friend-du Preez, N., Ramlagan, S., & Anderson, J. (2010). Antiretroviral treatment adherence among HIV patients in KwaZulu-Natal, South Africa. BMC Public Health, 10, CD007268. doi: 10.1186/1471-2458-10-111
- Poudel, K. C., Buchanan, D. R., Amiya, R. M., & Poudel-Tandukar, K. (2015). Perceived family support and antiretroviral adherence in HIV-positive individuals: Results from a community-based positive living with HIV study. International Quarterly of Community Health Education, 36(1), 71–91. doi: 10.1177/0272684X15614220
- Power, R., Koopman, C., Volk, J., Israelski, D. M., Stone, L., Chesney, M. A., & Spiegel, D. (2003). Social support, substance use, and denial in relationship to antiretroviral treatment adherence among HIV-infected persons. AIDS Patient Care and STDs, 17(5), 245–252. doi: 10.1089/108729103321655890
- Reif, S., Proeschold-Bell, R. J., Yao, J., Legrand, S., Uehara, A., Asiimwe, E., & Quinlivan, E. B. (2013). Three types of self-efficacy associated with medication adherence in patients with co-occurring HIV and substance use disorders, but only when mood disorders are present. Journal of Multidisciplinary Healthcare, 6, 229–237. doi: 10.2147/JMDH.S44204
- Renwick, R., Halpen, T., Rudman, D., & Friedland, J. (1999). Description and validation of a measure of received support specific to HIV. Psychological Reports, 84(2), 663–673. doi: 10.2466/pr0.1999.84.2.663
- Safren, S. A., Biello, K. B., Smeaton, L., Mimiaga, M. J., Walawander, A., Lama, J. R., … Pearls Study Team. (2014). Psychosocial predictors of non-adherence and treatment failure in a large scale multi-national trial of antiretroviral therapy for HIV: Data from the ACTG A5175/PEARLS trial. Plos One, 9(8), e104178. doi: 10.1371/journal.pone.0104178
- Sagarduy, J. L. Y., Lopez, J. A. P., Remirez, M. T. G., & Davila, L. E. F. (2017). Psychological model of ART adherence behaviors in persons living with HIV/AIDS in Mexico: A structural equation analysis. Revista De Saude Publica, 51. doi:Artn 8110.11606/S1518-8787.2017051006926
- Sauceda, J. A., Wiebe, J. S., & Simoni, J. M. (2014). Childhood sexual abuse and depression in Latino men who have sex with men: Does resilience protect against nonadherence to antiretroviral therapy? Journal of Health Psychology, 25, 1359105314546341.
- Shaw, J., McLean, K. C., Taylor, B., Swartout, K., & Querna, K. (2016). Beyond resilience: Why we need to look at systems too. Psychology of Violence, 6(1), 34–41. doi: 10.1037/vio0000020
- Simoni, J. M., Frick, P. A., Lockhart, D., & Liebovitz, D. (2002). Mediators of social support and antiretroviral adherence among an indigent population in New York City. AIDS Patient Care and STDs, 16(9), 431–439. doi: 10.1089/108729102760330272
- Sodergard, B., Halvarsson, M., Tully, M. P., Mindouri, S., Nordstrom, M. L., Lindback, S., … Lindblad, A. K. (2006). Adherence to treatment in Swedish HIV-infected patients. Journal of Clinical Pharmacy and Therapeutics, 31(6), 605–616. doi: 10.1111/j.1365-2710.2006.00782.x
- Solano, L., Costa, M., Salvati, S., Coda, R., Aiuti, F., Mezzaroma, I., & Bertini, M. (1993). Psychosocial factors and clinical evolution in HIV-1 infection: A longitudinal study. Journal of Psychosomatic Research, 37(1), 39–51. doi: 10.1016/0022-3999(93)90122-V
- Spies, G., & Seedat, S. (2014). Depression and resilience in women with HIV and early life stress: Does trauma play a mediating role? A cross-sectional study. BMJ Open, 4(2), e004200. doi: 004210.001136/bmjopen-002013-004200
- Steinhardt, M., & Dolbier, C. (2008). Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. Journal of American College Health, 56(4), 445–453. doi: 410.3200/JACH.3256.3244.3445-3454
- Steinhardt, M. A., Mamerow, M. M., Brown, S. A., & Jolly, C. A. (2009). A resilience intervention in African American adults with type 2 diabetes: A pilot study of efficacy. The Diabetes Educator, 35(2), 274–284. doi: 10.1177/0145721708329698
- Tariq, S., Elford, J., Tookey, P., Anderson, J., de Ruiter, A., O’Connell, R., & Pillen, A. (2016). “It pains me because as a woman you have to breastfeed your baby”: decision-making about infant feeding among African women living with HIV in the UK. Sexually Transmitted Infections. doi: 10.1136/sextrans-2015-052224
- Teti, M., French, B., Bonney, L., & Lightfoot, M. (2015). “I created something new with something that had died”: Photo-narratives of positive transformation among women with HIV. AIDS and Behavior, 20, 20.
- Thornton, S., Troop, M., Burgess, A. P., Button, J., Goodall, R., Flynn, R., … Easterbrook, P. J. (2000). The relationship of psychological variables and disease progression among long-term HIV-infected men. International Journal of STD & AIDs, 11(11), 734–742. doi: 10.1258/0956462001915165
- Tomakowsky, J., Lumley, M. A., Markowitz, N., & Frank, C. (2001). Optimistic explanatory style and dispositional optimism in HIV-infected men. Journal of Psychosomatic Research, 51(4), 577–587.
- Trevino, K. M., Pargament, K. I., Cotton, S., Leonard, A. C., Hahn, J., Caprini-Faigin, C. A., & Tsevat, J. (2010). Religious coping and physiological, psychological, social, and spiritual outcomes in patients with HIV/AIDS: Cross-sectional and longitudinal findings. AIDS and Behavior, 14(2), 379–389. doi: 10.1007/s10461-007-9332-6
- Tugade, M. M., Fredrickson, B. L., & Barrett, L. F. (2004). Psychological resilience and positive emotional granularity: Examining the benefits of positive emotions on coping and health. Journal of Personality, 72(6), 1161–1190. doi: 10.1111/j.1467-6494.2004.00294.x
- Turan, B., Fazeli, P. L., Raper, J. L., Mugavero, M. J., & Johnson, M. O. (2016). Social support and moment-to-moment changes in treatment self-efficacy in men living with HIV: Psychosocial moderators and clinical outcomes. Health Psychology, 35(10), 1126–1134. doi: 10.1037/hea0000356
- Unger, M. (2008). Resilience across cultures. British Journal of Social Work, 38(2), 218–235.
- Wagnild, G. M., & Young, H. M. (1993). Development and psychometric evaluation of the Resilience Scale. Journal of Nursing Measurement, 1(2), 165–178.
- Waldrop-Valverde, D., Guo, Y., Ownby, R. L., Rodriguez, A., & Jones, D. L. (2014). Risk and protective factors for retention in HIV care. AIDS and Behavior, 18(8), 1483–1491. doi: 10.1007/s10461-013-0633-7
- Weaver, K. E., Llabre, M. M., Duran, R. E., Antoni, M. H., Ironson, G., Penedo, F. J., & Schneiderman, N. (2005). A stress and coping model of medication adherence and viral load in HIV-positive men and women on highly active antiretroviral therapy (HAART). Health Psychology, 24(4), 385–392. doi: 10.1037/0278-6133.24.4.385
- Williams, A. B., Shahryarinejad, A., Andrews, S., & Alcabes, P. (1997). Social support for HIV-infected mothers: Relation to HIV care seeking. Journal of the Association of Nurses in AIDS Care, 8(1), 91–98. doi: 10.1016/S1055-3290(97)80040-4
- Wolf, M. S., Davis, T. C., Osborn, C. Y., Skripkauskas, S., Bennett, C. L., & Makoul, G. (2007). Literacy, self-efficacy, and HIV medication adherence. Patient Education and Counseling, 65(2), 253–260. doi: 10.1016/j.pec.2006.08.006
- Wouters, E., Van Damme, W., Van Loon, F., van Rensburg, D., & Meulemans, H. (2009). Public-sector ART in the Free State Province, South Africa: Community support as an important determinant of outcome. Social Science and Medicine, 69(8), 1177–1185. doi: 10.1016/j.socscimed.2009.07.034
- Zachariah, R., Teck, R., Buhendwa, L., Fitzerland, M., Labana, S., Chinji, C., … Harries, A. D. (2007). Community support is associated with better antiretroviral treatment outcomes in a resource-limited rural district in Malawi. Transactions of the Royal Society of Tropical Medicine and Hygiene, 101(1), 79–84. doi: 10.1016/j.trstmh.2006.05.010
