
ABSTRACT
Evidence-based guidelines in HIV care aim to improve patients’ health outcomes, quality of care, and cost-effectiveness. Laboratory monitoring plays an important role in assessing clinical status of patients and forms an integral part of HIV treatment guidelines. The Dutch HIV monitoring foundation (Stichting HIV Monitoring) previously observed variation between HIV treatment centres in the Netherlands in terms of compliance with guidelines for performing laboratory tests. Drawing on qualitative research methods, this article aims to describe factors that influence guideline compliance for laboratory monitoring in outpatient HIV care in the Netherlands. Twelve semi-structured in-depth interviews were conducted with a convenience sample of physicians from four HIV treatment centres. In general, physicians perceived laboratory guidelines as useful. However, unclear online visual representation of the guidelines, a lack of set reminders for tests, and assessment of patients’ risk behaviour, which differs per patient, were identified as barriers to guideline compliance. The compartmentalisation of the Dutch healthcare system was viewed as hampering guideline compliance. A clinical-decision-support tool could possibly facilitate compliance with laboratory monitoring guidelines. Moreover, better alignment of HIV outpatient care, municipal health services and primary care, in terms of laboratory testing, could optimize efficiency, increase cost-effectiveness, and improve quality of HIV care.
Introduction
The Dutch association of HIV treating physicians (Nederlandse Vereniging van HIV Behandelaren, NVHB) provides national guidelines for the treatment and monitoring of people living with HIV (PLWH) in the Netherlands (“Richtlijnen - Nederlandse Vereniging van HIV Behandelaren,” Citationn.d.). These guidelines are adapted from those published by the American Department of Health and Human Services (DHHS, Panel on Antiretroviral Guidelines for Adults and Adolescents, Citation2016, http://bit.ly/2mizrVQ). To initiate and monitor appropriate treatment for HIV and to prevent, identify and treat opportunistic infections, comorbidities and co-infections, including sexually transmitted infections (STIs), the Dutch HIV treatment guidelines recommend a set of laboratory tests, to be performed prior to combination antiretroviral therapy (cART) and within 12 months of initiating HIV care. Moreover, tests are recommended after cART initiation to identify potential treatment toxicities and evidence of incident comorbidities. Finally, for men who have sex with men (MSM), repeat screening for hepatitis C virus (HCV) and syphilis co-infection is recommended.
The Dutch HIV treatment guidelines on laboratory testing are intended to support physicians in providing optimal health care, to standardize care across treatment centres and to avoid the inefficient use of resources. Not requesting laboratory tests as recommended can lead to an incorrect or delayed treatment plan, and the misallocation of healthcare providers’ time and resources. Furthermore, under-use of tests has been associated with lower quality of care (Grol, Citation2001; Thelwall & Maflahi, Citation2016), and increased direct and indirect healthcare costs (Qaseem et al., Citation2012; Weinberger, Citation2011; Woolf, Grol, Hutchinson, Eccles, & Grimshaw, Citation1999).
The Dutch HIV monitoring foundation (Stichting HIV Monitoring; SHM) has observed variation among Dutch HIV treatment centres in terms of how the guidelines for requesting laboratory tests are implemented in practice () (van Sighem et al., Citation2016). This study therefore examines factors that influence compliance with guidelines for laboratory testing. The findings offer insights into physicians’ perspectives on, and use of, guidelines and prompt recommendations to improve guideline compliance in HIV care in the Netherlands.
Table 1. Level of guideline compliance for laboratory assessment by centre, in 2012–2014 (van Sighem et al., Citation2016).
Materials and methods
Conceptual framework
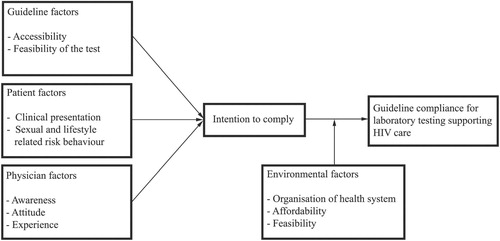
A conceptual framework was developed drawing on a clinical decision-making model (Hammarström et al., Citation2016), the quality of care model by Donabedian (Citation1966) and theories on guideline compliance (Adams & Balderson, Citation2016; Ajzen, Citation1991; Evenblij, Verbon, & van Leth, Citation2016). These models were adapted to fit issues around guideline compliance within HIV care in the Netherlands (). The framework consisted of four categories: guideline factors, patient factors, physician factors and environmental factors. The first three factors were expected to contribute to the intention to comply with guidelines. The environmental factors were expected to influence the intention to comply with guidelines. Conceivably, compliance with guidelines for laboratory testing that supports HIV care would depend on the intention to comply with guidelines and on environmental factors (such as the organization of the healthcare system and the affordability of tests). Moreover, the intention to comply with guidelines was expected to depend on multiple factors relating to physicians and patients.
Figure 1. Conceptual framework for guideline compliance in HIV care.
Site selection
In the Netherlands, HIV care may only be provided by specialized HIV physicians and is centralized in 26 certified HIV treatment centres (van Sighem et al., Citation2016). SHM collects, analyses and reports national data from all HIV treatment centres. Previous studies have found an association between centre size and the quality of care (Backus et al., Citation2010; Engelhard et al., Citation2016; Solomon, Flynn, & Lavetsky, Citation2005). Therefore, centres of different sizes (based on the number of PLWH in care in 2016) were selected to provide respondents with experience in diverse HIV care settings facilities. The selection of centres was also influenced by convenience: their proximity to Amsterdam because of the availability of the interviewer. Among the potential centres, the sampling was as random as possible, given the small population (i.e., small number of HIV treating physicians). TSB and DCMT contacted 18 HIV treating physicians by e-mail. Twelve physicians participated: eight physicians from three large centres (≥600 patients in care), three physicians from one mid-size centre (300–600 patients in care) and one physician from a small centre (<300 patients in care). The sample size was flexible and influenced by achieving theoretical data saturation, which was defined as the point at which no novel information emerged from subsequent interviews.
Data collection
For the semi-structured interviews, a topic guide was developed based on the conceptual framework, the quantitative results from the 2016 HIV Monitoring Report and the NVHB guidelines as of February 2017 (“Richtlijnen - Nederlandse Vereniging van HIV Behandelaren,” Citationn.d.; van Sighem et al., Citation2016). The topic guide was compiled in an iterative manner and consisted of questions pertaining to the physician’s knowledge, beliefs and attitudes towards, and experience with, the guidelines for laboratory testing (i.e., applicability, affordability and appropriateness), and perceived barriers and facilitators to complying with these guidelines. Additionally, three case-vignettes were presented: (1) upon initiating care after HIV diagnosis; (2) upon transferring into care from another HIV treatment centre (within or outside the Netherlands); and (3) during follow-up in HIV care. The case-vignettes contained questions about the physician’s actions during the consultations in all three situations. A pilot interview was conducted with one HIV treating physician to practice the interview and review whether the topic guide allowed physicians to give a full and coherent explanation of the topics. The interview guide was adapted in an iterative manner to decrease the risk of overlooking relevant topics (Fiksdal et al., Citation2014; Gray Citation2013; Maxwell, Citation2008; Strauss & Corbin, Citation1998).
The first author (DCMT) conducted all interviews face-to-face in Dutch by at the workplace of the HIV treating physician during April–May 2017. Participants did not receive compensation for participating in the interview. Interview duration ranged from 24 to 44 min with an average of 31 min. Because of the iterative process of interview guide design, if a new topic arose, it was added to the interview guide for subsequent interviews.
Interviews were recorded and transcribed verbatim. All data were anonymized. Transcripts were subjected to member checks (Barbour, Citation2001; Burnard, Citation1991; Riessman, Citation1993). The proposed study design was approved by the Ethics Committee of the Academic Medical Centre of the University of Amsterdam (Number W16_400).
Data analysis
Transcripts were coded using thematic analysis (Braun & Clarke, Citation2006). The coding scheme was developed using a semi-inductive approach, whereby core themes were derived from the conceptual framework, seen in and . Coding was conducted using a coding scheme that included themes that were initially hypothesized as relevant and that incorporated themes that emerged during data analysis.
Table 2. Coding scheme with definitions.
Results
Recruitment and participant characteristics
Of the 18 HIV treating physicians that were approached, six did not participate because of a lack of time (n = 2) or withdrew after member checking (n = 1). Three did not respond to requests for an interview. Twelve HIV treating physicians from four certified HIV treatment centres were included in this study (). The mean age of all participants was 52 years. The interviewed physicians had worked with HIV patients for an average of 19 years: six had worked as an HIV treating physician for over twenty years, and the remaining six physicians between six and twenty years. Physicians worked in large (n = 8), mid-size (n = 3) and small (n = 1) centres, caring for a total of 5,479 HIV-positive patients (29.0% of all 18,866 patients in HIV care in 2016) (Stichting HIV Monitoring, Citation2016). All participants were specialists in internal medicine. Nine also specialized in infectious diseases. Two also specialized in HIV care during pregnancy.
Table 3. Patient characteristics of the present study.
The following section elaborates the elements of the conceptual framework. Interview excerpts have been translated from Dutch to English to illustrate how respondents raised these issues.
Guideline factors
Accessibility and feasibility
Most physicians were familiar with the NVHB guidelines and perceived them as useful (n = 9) and supportive (n = 2) in decision-making for HIV care. One physician did not know the NVHB guidelines, but was familiar with the DHHS (i.e., American) guidelines and found these guidelines understandable and helpful. The variation in requests for cholesterol tests may be explained – as three respondents mentioned – by the fact that guidelines do not recommend cholesterol testing at a specific age. One physician stated that the presentation of the NVHB guidelines on the website was unclear, given the large amount of text on the webpage.
Patient factors
Clinical presentation
Three physicians indicated that patient preference and characteristics were paramount for their clinical decisions, and that guidelines played a secondary role in their decisions about requesting laboratory tests. All physicians indicated that they followed a routine in their consultations, during which the patient’s socio-demographic and clinical characteristics are taken into account to assess clinical presentation and risk behaviour (i.e., sexual risk behaviour and lifestyle-related risk behaviour) (n = 12). In addition, respondents indicated that nurses assessed information on patient’s complaints, physical symptoms and sexual behaviour during an intake interview. The nurses subsequently made this information available to the physicians through the patient files.
Two respondents mentioned that after patients have been under the care of the same physician for years or decades, the physician gains extensive knowledge of the patient and can therefore assess his/her risk more easily without further testing. On the other hand, despite being familiar with their own patients, four physicians from a large centre cited a lack of knowledge about their patients’ sexual partners as justification for requesting STI tests more frequently than recommended.
Physician factors
Awareness, attitude and experience
Overall, physicians were aware of guidelines for laboratory testing. Physicians did not experience any barriers to requesting tests and reported no instances of patients objecting to having blood taken (n = 12). However, one physician indicated that testing for HCV and syphilis could come across as patronizing for the patient, because it refers to sexual behaviour. Nonetheless, all HIV treating physicians said that they could always request all the tests they deemed necessary.
Environmental factors
Organization of the Dutch healthcare system
Almost half of the physicians described the compartmentalization of HIV care in the Netherlands (n = 5) as a barrier to compliance with the proposed testing scheme. Two mentioned the unclear task division between the Municipal Health Services (Gemeentelijke Gezondheidsdienst; GGD), general practitioners (GP) and HIV treatment centres. One physician suggested a need for more clearly defined roles for GPs, the GGDs and the HIV treatment centres, as well as having greater information regarding the costs of HIV care. Another mentioned that when STI testing was conducted at a GGD, the HIV treating physician was often unaware of which tests had been performed, making it necessary to repeat all tests. This physician mentioned that using electronic health records could improve accessibility of these results for all primary and secondary care providers, thereby preventing unnecessary repetition of tests.
System for automatic test request
Even within the same centre, opinions on the feasibility of testing varied. For example, some physicians indicated that the electronic health record software in their centre was supportive (n = 3), whereas others did not find the system supportive at all (n = 2). Furthermore, two physicians mentioned that their system did not remind them to request tests for STIs (e.g., HCV and syphilis). Three physicians suggested using an automated system that reminds physicians to request STI tests after a standard period of time, especially if a patient belongs to the risk group of MSM. It was proposed that such a reminder could take the form of a pop-up in the health record system, which would integrate the NVHB recommendations. If a physician were then to register a patient as MSM, an automatic reminder would appear to request an HCV and/or syphilis test (n = 1).
Costs of laboratory testing
All physicians indicated that they had limited knowledge of the costs of laboratory tests. Five physicians mentioned that they did not let costs play a role in their intention to request a test, whereas three physicians said that they balanced the benefits of testing versus the costs of the test when deciding whether or not an expensive test was necessary.
However, costs did seem to play a role in complying with guideline recommendations for HCV testing. Nine of the 12 physicians described how they were guided by incident ALAT elevations (i.e., liver enzyme concentrations that could indicate HCV infection) when deciding on HCV testing. Furthermore, three of these nine physicians indicated that they tested for HCV once a year. Two physicians who mentioned that they were aware of the guideline for HCV laboratory testing indicated that, because of costs considerations, they monitored ALAT elevations instead ().
Table 4. Quotation table.
Discussion
This article examines factors that influence compliance with guidelines for laboratory testing in HIV care. The aim was to conduct interviews with physicians in an even distribution of centres of different sizes. Because this was not possible, the impact of centre-size was difficult to assess (). Also, there were no discernible differences in findings related to the physician’s duration of experience. In general, HIV treating physicians in the Netherlands, found the laboratory testing guidelines for HIV care useful. Perceived barriers to guideline compliance were: unclear visual representation of the NVHB guidelines on the website, lack of supportive clinical management software, compartmentalization of the Dutch healthcare system, and assessment of risk behaviour, which differs per patient.
Although the guidelines were considered useful in the process of requesting laboratory tests, physicians indicated that the deciding factors were a patient’s circumstances and clinical status. This points to patient-centred or person-centred care, emphasizing the importance of understanding the full context of a patient (Epstein & Street, Citation2011; De Raad voor Volksgezondheid en Samenleving Citation2017; Solà et al., Citation2014).
Furthermore, in line with previous research, costs also played a role in guideline compliance, especially for the HCV tests (Adams & Balderson, Citation2016), with some physicians monitoring liver enzymes rather than HCV antibody or HCV RNA, out of concern for cost-effectiveness. However, HCV infection is not necessarily accompanied by elevated ALAT levels. Therefore, this can result in cases of hepatitis being missed (Gholson et al., Citation1997; Giannini, Testa, & Savarino, Citation2005; Mofrad et al., Citation2003). The perceived cost-effectiveness of monitoring liver enzymes conflicts with the guideline recommendations, which state that it is cost-effective to monitor HCV because MSM are at risk of HCV, which has high treatment costs and a high risk of transmission (Götz et al., Citation2005; Kaplan-Lewis & Fierer, Citation2015; Linas, Wong, Schackman, Kim, & Freedberg, Citation2012; Popping, Citation2016; Woolf et al., Citation1999).
Strengths and limitations
This qualitative study provided additional insight into the quantitative findings of the SHM HIV Monitoring Report, which indicated variation in guideline compliance. The vignettes and coding sheet facilitated the systematic analysis of the intention to comply with guidelines (Ritchie, Lewis, Nicholls, & Ormston, Citation2013). During the 12 interviews, the point of theoretical saturation was reached because no new themes emerged during subsequent interviews. Future studies investigating guideline compliance could use the conceptual framework that was used in this study (Adams & Balderson, Citation2016; Ajzen, Citation1991; Evenblij et al., Citation2016; Foy, Walker, & Penney, Citation2001).
The findings are limited by the following: physicians’ responses may have been influenced by social desirability bias, in particular, a tendency to emphasize compliance with guidelines; and all the respondents were HIV treating physicians, thus the views of HIV nurses, counsellors, or other stakeholders in HIV care, such as GPs and health workers at the Municipal Health Services (Gemeentelijke Gezondheidsdienst; GGD) were not included.
Recommendations
In view of the low request rates reported for some recommended laboratory tests, a clinical decision support tool integrated into electronic health records could facilitate compliance with laboratory test requests, for example, through individualized reminders. Such support tools could also prompt assessment of sexual and lifestyle risk behaviour, counter difficulties in guideline communication, and improve healthcare processes (Bright et al., Citation2012; Lobach & Hammond, Citation1997; Peleg, Citation2013).
Based on the observation that costs influenced the intention to comply with guidelines, especially for HCV testing, more insight is needed into the costs and cost-effectiveness of testing algorithms (Balshem et al., Citation2011; Guyatt et al., Citation2008). The DHHS guidelines have a strength of recommendation and quality of evidence grading (Panel on Antiretroviral Guidelines for Adults and Adolescents, Citation2016). We recommend that the Dutch NVHB guidelines highlight this.
Lastly, as a long-term recommendation, standards of care in HIV treatment centres must align with the guidelines from the GGD, in terms of STI testing and primary care. The NVHB should engage with GP organizations to discuss task distribution, as well as defining these roles in the guidelines.
Conclusion
Compliance with HIV treatment guidelines by HIV treating physician in the Netherland can be improved. The over- and under-request of recommended laboratory test compromises the overall efficiency, cost-effectiveness and quality of HIV care. A tailored clinical decision support tool in HIV treatment centres in the Netherlands could improve compliance. Policy makers should seek the alignment of HIV care provided by HIV treating physicians, GPs and municipal health authorities in the Netherlands. These suggestions could also promote the identification, prevention and appropriate treatment of other co-infections, opportunistic infections and comorbidities.
Acknowledgements
We would like to thank all HIV treating physicians who participated in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
T. Sonia Boender http://orcid.org/0000-0002-4418-3713
Additional information
Funding
References
- Adams, L. M., & Balderson, B. H. (2016). HIV providers’ likelihood to prescribe pre-exposure prophylaxis (PrEP) for HIV prevention differs by patient type: A short report. AIDS Care, 28(9), 1154–1158. doi: 10.1080/09540121.2016.1153595
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. doi: 10.1016/0749-5978(91)90020-T
- Backus, L. I., Boothroyd, D. B., Phillips, B. R., Belperio, P. S., Halloran, J. P., Valdiserri, R. O., & Mole, L. A. (2010). National quality forum performance measures for HIV/AIDS care: The Department of Veterans Affairs’ experience. Archives of Internal Medicine, 170(14), 1239–1246. doi: 10.1001/archinternmed.2010.234
- Balshem, H., Helfand, M., Schünemann, H. J., Oxman, A. D., Kunz, R., Brozek, J., … Norris, S. (2011). GRADE guidelines: 3. Rating the quality of evidence. Journal of Clinical Epidemiology, 64(4), 401–406. doi: 10.1016/j.jclinepi.2010.07.015
- Barbour, R. S. (2001). Checklists for improving rigour in qualitative research: A case of the tail wagging the dog? BMJ, 322(7294), 1115–1117. doi: 10.1136/bmj.322.7294.1115
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. doi: 10.1191/1478088706qp063oa
- Bright, T. J., Wong, A., Dhurjati, R., Bristow, E., Bastian, L., Coeytaux, R. R., … Musty, M. D. (2012). Effect of clinical decision-support systems: A systematic review. Annals of Internal Medicine, 157(1), 29–43. doi: 10.7326/0003-4819-157-1-201207030-00450
- Burnard, P. (1991). A method of analysing interview transcripts in qualitative research. Nurse Education Today, 11(6), 461–466. doi: 10.1016/0260-6917(91)90009-Y
- De Raad voor Volksgezondheid en Samenleving, R. (2017). Zonder context geen bewijs. Over de illusie van evidence-based practice in de zorg.
- Donabedian, A. (1966). Evaluating the quality of medical care. The Milbank Memorial Fund Quarterly, 44(3), 166–206. doi: 10.2307/3348969
- Engelhard, E. A. N., Smit, C., Van Sighem, A., Reiss, P., Nieuwkerk, P. T., Kroon, F. P., … Geerlings, S. E. (2016). Impact of HIV care facility characteristics on the cascade of care in HIV-infected patients in the Netherlands. AIDS (London, England), 30(2), 301–310. doi: 10.1097/QAD.0000000000000938
- Epstein, R. M., & Street, R. L. (2011). The values and value of patient-centered care. Annals Family Med.
- Evenblij, K., Verbon, A., & van Leth, F. (2016). Intention of physicians to implement guidelines for screening and treatment of latent tuberculosis infection in HIV-infected patients in The Netherlands: A mixed-method design. BMC Public Health, 16(1), 915. doi: 10.1186/s12889-016-3539-2
- Fiksdal, A. S., Kumbamu, A., Jadhav, A. S., Cocos, C., Nelsen, L. A., Pathak, J., & McCormick, J. B. (2014). Evaluating the process of online health information searching: A qualitative approach to exploring consumer perspectives. Journal of Medical Internet Research, 16(10), e224. doi: 10.2196/jmir.3341
- Foy, R., Walker, A., & Penney, G. (2001). Barriers to clinical guidelines: The need for concerted action. British Journal of Clinical Governance, 6(3), 166–174. doi: 10.1108/EUM0000000005680
- Gholson, C. F., Morgan, K., Catinis, G., Favrot, D., Taylor, B., Gonzalez, E., & Balart, L. (1997). Chronic hepatitis C with normal aminotransferase levels: A clinical histologic study. American Journal of Gastroenterology, 92(10), 1788–1792.
- Giannini, E. G., Testa, R., & Savarino, V. (2005). Liver enzyme alteration: A guide for clinicians. Canadian Medical Association Journal, 172(3), 367–379. doi: 10.1503/cmaj.1040752
- Götz, H. M., van Doornum, G., Niesters, H. G. M., den Hollander, J. G., Thio, H. B., & de Zwart, O. (2005). A cluster of acute hepatitis C virus infection among men who have sex with men – results from contact tracing and public health implications. AIDS (London, England), 19(9), 969–974. doi: 10.1097/01.aids.0000171412.61360.f8
- Gray, D. E. (2013). Doing research in the real world, Sage: London.
- Grol, R. (2001). Improving the quality of medical care: Building bridges among professional pride, payer profit, and patient satisfaction. Jama, 286(20), 2578–2585. doi: 10.1001/jama.286.20.2578
- Guyatt, G. H., Oxman, A. D., Vist, G. E., Kunz, R., Falck-Ytter, Y., Alonso-Coello, P., & Schünemann, H. J. (2008). GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ, 336(7650), 924–926. Retrieved from http://www.bmj.com/content/336/7650/924.abstract doi: 10.1136/bmj.39489.470347.AD
- Hammarström, A., Wiklund, M., Stålnacke, B.-M., Lehti, A., Haukenes, I., & Fjellman-Wiklund, A. (2016). Developing a tool for increasing the awareness about gendered and intersectional processes in the clinical assessment of patients – A study of pain rehabilitation. PloS One, 11(4), e0152735. doi: 10.1371/journal.pone.0152735
- Kaplan-Lewis, E., & Fierer, D. S. (2015). Acute HCV in HIV-infected MSM: Modes of acquisition, liver fibrosis, and treatment. Current HIV/AIDS Reports, 12(3), 317–325. doi: 10.1007/s11904-015-0279-3
- Linas, B. P., Wong, A. Y., Schackman, B. R., Kim, A. Y., & Freedberg, K. A. (2012). Cost-effective screening for acute hepatitis C virus infection in HIV-infected men who have sex with men. Clinical Infectious Diseases, 55(2), 279–290. doi: 10.1093/cid/cis382
- Lobach, D. F., & Hammond, W. E. (1997). Computerized decision support based on a clinical practice guideline improves compliance with care standards. The American Journal of Medicine, 102(1), 89–98. doi: 10.1016/S0002-9343(96)00382-8
- Maxwell, J. A. (2008). Designing a qualitative study. In The Sage handbook of applied social research methods (Vol. 2, pp. 214–253). London: Sage.
- Mofrad, P., Contos, M. J., Haque, M., Sargeant, C., Fisher, R. A., Luketic, V. A., … Sanyal, A. J. (2003). Clinical and histologic spectrum of nonalcoholic fatty liver disease associated with normal ALT values. Hepatology, 37(6), 1286–1292. doi: 10.1053/jhep.2003.50229
- Panel on Antiretroviral Guidelines for Adults and Adolescents. (2016). Guidelines for the use ofantiretroviral agents in HIV-1-infected adults and adolescents. Department of Human Services. Retrieved from http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
- Peleg, M. (2013). Computer-interpretable clinical guidelines: A methodological review. Journal of Biomedical Informatics, 46(4), 744–763. doi: 10.1016/j.jbi.2013.06.009
- Popping, S., van Kampen, J., Verbon, A., Boucher, C., & van de Vijver, D. (2016). Intensive hepatitis C monitoring in previously HCV infected HIV-positive MSM is a cost saving method to reduce the HCV epidemic. Presented at: Netherlands conference on HIV pathogenesis, epidemiology, prevention and treatment; 22 November 2016. Abstract O10. [Accessed 10 July 2017]. Available at: http://nchivorg/abstracts/.
- Qaseem, A., Alguire, P., Dallas, P., Feinberg, L. E., Fitzgerald, F. T., Horwitch, C., … Wiese, J. G. (2012). Appropriate use of screening and diagnostic tests to foster high-value, cost-conscious care. Annals of Internal Medicine, 156(2), 147–149. doi: 10.7326/0003-4819-156-2-201201170-00011
- Richtlijnen - Nederlandse Vereniging van HIV Behandelaren. (n.d.). Retrieved from http://richtlijnhiv.nvhb.nl/index.php/Hoofdpagina
- Riessman, C. K. (1993). Narrative analysis (Vol. 30). Newbury Park: Sage.
- Ritchie, J., Lewis, J., Nicholls, C. M., & Ormston, R. (2013). Qualitative research practice: A guide for social science students and researchers. London: Sage.
- Solà, I., Carrasco, J. M., del Campo, P. D., Gracia, J., Orrego, C., Martínez, F., … de Gaminde, I. (2014). Attitudes and perceptions about clinical guidelines: A qualitative study with Spanish physicians. PloS One, 9(2), e86065. doi: 10.1371/journal.pone.0086065
- Solomon, L., Flynn, C., & Lavetsky, G. (2005). Managed care for AIDS patients: Is bigger better? JAIDS Journal of Acquired Immune Deficiency Syndromes, 38(3), 342–347.
- Stichting HIV Monitoring. (2016). Jaarverslag 2016. Retrieved from https://www.hiv-monitoring.nl/nederlands/over-shm/jaarverslagen/
- Strauss, A., & Corbin, J. (1998). Basics of qualitative research techniques. London: Sage.
- Thelwall, M., & Maflahi, N. (2016). Guideline references and academic citations as evidence of the clinical value of health research. Journal of the Association for Information Science and Technology, 67(4), 960–966. doi: 10.1002/asi.23432
- van Sighem, A. I., Smit, C., Wit, F. W. N. M., Boender, T. S., Matser, A., & Reiss, P. (2016). Monitoring Report 2016. Human Immunodeficiency Virus (HIV) Infection in the Netherlands. Amsterdam.
- Weinberger, S. E. (2011). Providing high-value, cost-conscious care: A critical seventh general competency for physicians. Annals of Internal Medicine, 155(6), 386–388. doi: 10.7326/0003-4819-155-6-201109200-00007
- Woolf, S. H., Grol, R., Hutchinson, A., Eccles, M., & Grimshaw, J. (1999). Clinical guidelines: Potential benefits, limitations, and harms of clinical guidelines. BMJ, 318(7182), 527. doi: 10.1136/bmj.318.7182.527
