
ABSTRACT
The rules of conduct given to people living with HIV in Sweden in accordance with the Swedish Communicable Diseases Act stipulate disclosure obligation to sexual partners and mandatory condom use. Since 2013, treating physicians have the possibility to exempt patients from this disclosure obligation when no considerable risk of transmission is present. This study explored experiences of communication with clinical staff at HIV clinics regarding rules of conduct and infectiousness among men who have sex with men (MSM) living with HIV in Sweden. In-depth interviews were carried out with 10 MSM living with HIV in Sweden. Study participants all reported unmeasurable viral loads. Data were analyzed using qualitative content analysis. Five categories and one theme, “Navigating between rules and reality”, were identified. We found that MSM living with HIV had good relationships with clinical staff at HIV clinics. Inconsistencies emerged regarding how they experienced receiving information about the rules of conduct and infectiousness. The findings indicate that lack of sound routines regarding how information and rules of conduct are communicated negatively affects MSM living with HIV and poses potential risks for the individual. The participants’ expressed trust in staff at HIV clinics can provide a good basis for improved communication.
Introduction
Good communication between HIV care providers and patients living with HIV is essential to ensure access to correct information. It is especially important that people living with HIV are aware of their obligations in countries where HIV legislation stipulate specific rules of conduct.
The 4th section 2 § in the Swedish Communicable Diseases Act (SFS Citation2004:168), under which HIV infection is classified as a public health hazard among a number of other infections, stipulates that as soon as possible after HIV diagnosis the patient is to be given written individual rules of conduct by the treating physician. These rules are standardized and include an obligation to disclose HIV positive status to sexual partners and behave in a manner that minimizes risk of transmission, i.e., using condoms. HIV legislation have been criticized in Sweden (HIV-Sweden, Citation2012; IPPF, Citation2014), as well as in other countries (Haire & Kaldor, Citation2015; Kazatchkine, Bernard, & Eba, Citation2015), for being counterproductive, stigmatizing and for not being guided by scientific evidence.
Following the results from the HTPN 052 study (Cohen et al., Citation2011), the Swedish Reference Group for Antiretroviral Therapy and the Public Health Agency of Sweden published a report stating that the risk of HIV transmission is minimal when condom is used and very low when no condom is used, when a patient’s viral load is suppressed (Folkhälsomyndigheten, Citation2014). Following this statement, the National Board of Health and Welfare published a clarification (Socialstyrelsen, Citation2013) which made it possible for treating physicians to exempt patients from their disclosure obligation to sexual partners. Since the HTPN 052 study, a number of studies further confirmed how effective treatment lowers the risk of transmission (Bavinton et al., Citation2017; Cohen et al., Citation2011; Rodger et al., Citation2016).
Previous studies in Sweden have shown that the Swedish Communicable Diseases Control Act is perceived as both supportive, as it ensures access to free treatment, and as a burden, e.g., in regards to disclosure obligation (Christiansen, Lalos, & Johansson, Citation2008; Mehdiyar, Andersson, Hjelm, & Povlsen, Citation2016). To our knowledge, no previous studies have explored this topic since the possibility of being exempted from the obligation to disclose HIV status.
Aim
This study was designed to explore experiences and perceptions regarding communication about infectiousness and the rules of conduct with clinical staff at HIV clinics among MSM living with HIV in Sweden.
Methodology
Study design and data collection
We carried out a qualitative study with in-depth interviews following a semi-structured interview guide (Kvale & Brinkmann, Citation2009). 10 MSM living with HIV in Sweden were interviewed between November 2017 and February 2018. Six interviews were carried out in person and four were then conducted by videocall. Videocalls have been suggested to be a useful tool for qualitative research, as they allow a greater geographic distribution of participants (Janghorban, Latifnejad Roudsari, & Taghipour, Citation2014; Oates, Citation2015), while yielding data of quality equivalent to that from face-to-face interviews (Lo Iacono, Symonds, & Brown, Citation2016). Interviews were carried out in Swedish and English, recorded digitally and transcribed verbatim. Transcripts were verified by the second member of the research team. Recruitment continued until the research team concluded that sufficient saturation had been achieved.
Analysis
The collected data were analyzed according to qualitative content analysis as described by Graneheim and Lundman (Graneheim, Lindgren, & Lundman, Citation2017; Graneheim & Lundman, Citation2004) as illustrated in and . Interviews were transcribed and analyzed using MAX QDA (Version 12.3.2).
Figure 1. Example of the analytical process.

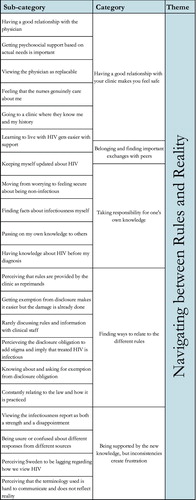
Figure 2: The main findings of the study: Sub-categories, categories & theme
Ethical considerations
All participants were given written and oral information about the study prior to giving consent to participate in the study, which included the possibility to end their participation at any time. To ensure anonymity of the study participants all were assigned an identity number (Ip1-Ip10) and no names or personal information were collected. The Regional Ethical Review Board of Stockholm approved the study.
Results
Study participants
All of the included study participants were MSM living with HIV in Sweden, on antiretroviral treatment, and reported unmeasurable viral load. An overview of study participants is presented in .
Table 1. Study participants (N = 10)
Navigating between rules and reality
The analysis resulted in an overarching theme, Navigating between rules and reality, based on the five categories and 21 sub-categories, as presented in . The overarching theme reflects the need for MSM living with HIV in Sweden to find strategies to cope with reality based on information and rules that have been communicated to them, sometimes drawing conclusions from contradictory information. The categories are presented below.
Having a good relationship with your clinic makes you feel safe
Participants experienced HIV clinics as a place where they felt safe and welcome. Their good and personal relationship with physicians and nurses contributed to this. They perceived their relationships with nurses to be especially close, describing them as friendly, caring, trustworthy, welcoming and empathetic.
In that sense I think it’s great to have such a close relationship with both the physicians and nurses. Because when we meet, we have fun. And they know me, they know the way I am. (Ip6)
He asks me questions and stuff, yeah, just like I don’t spend a lot of time, just one, two, three, four questions and everything. “Ok, you need to go and do your blood samples”, and that’s all. Nothing really important. (Ip10)
Taking responsibility for one’s own knowledge
According to the participants, information about HIV and rules of conduct was not routinely given by the staff at HIV clinics. However, participants described themselves as knowledgeable as they sought to keep themselves updated on new facts and information. They could also get information from clinical staff by asking directly for it.
So, I asked my doctor like this: I want to know, how infectious am I really? “Well, you are hardly infectious at all, because you’re under 50.” (Ip9)
After multiple ifs and buts [the nurse] finally explained the thing with low infectiousness. I recently thought about this and it was very moralizing. “Well, don’t forget that there is still a risk of transmission”. All I really wanted was a clear answer. (…) But she hardly wanted to give me that information. (Ip2)
In the beginning I was more worried, like that, I believe. Yes, then I was quite stressed about it. But now, since quite a few years, I believe, well, I expect that I am not infectious. (Ip5)
There was a security within myself that the virus cannot be transmitted, and reasonably I should be able to have sex on equal terms, as if I didn’t have the virus. (Ip2)
Finding ways to relate to the different rules
How the rules of conduct were received differed among the participants. The mandatory disclosure to sexual partners and the mandatory condom use were topics all had discussed with their physicians. Receiving the rules of conduct in writing was experienced negatively by some. One participant recalls feeling like he was seen as a criminal when the physician brought out, what he interpreted as, an excerpt from the Swedish statute book. Others only recalled vague mentions of the rules of conduct, and some described how they had to figure out the rules on their own. Participants also described the time of diagnosis as a crisis.
I believe that if I hadn’t been the person I am, so that I figured those things out and found out all the things anyway afterwards, then [the physician] actually did something wrong, I think. But I never got my disclosure obligations on paper, I didn’t get anything more than vague words in the beginning. (Ip1)
I believe it was more, like, how can you survive? Will I work? I mean questions about life that are bigger than the rules of conduct, more existential questions, I would say, were important at that time. (Ip3)
Participants perceived the rules as stigmatizing and that they wrongly convey well managed HIV as infectious. Some also experienced that physicians conveyed the rules in a negative manner.
[rules of conduct] have been mentioned from time to time, and then I’ve felt that, well, this feels like some kind of reprimand, it feels like, not okay at all. (Ip3)
I think it is really bad that they don’t tell you this. Really bad. (Ip8)
When I think about my sexual life and how diligent I am with my medication, and that I go to all my appointments as I am supposed to, then I think they could have told me. (Ip7)
The specific rules of conduct that some participants described being mentioned repeatedly by physicians were the HIV disclosure obligation to sexual partners and the mandatory condom use. Misconceptions and being unaware of specific rules existed among the participants. One such example was a participant who first became aware about the disclosure obligation to medical staff during the interview.
Participants also described how they kept updated about court cases related to HIV. Discrepancies arose when reports about court cases were contradictory to information received from clinical staff. Based on how the prosecutors dealt with the cases, some participants drew conclusions regarding their own rules of conduct.
As I have understood it, a prosecutor would not move on with the investigation if the person is well treated. If it, in an unlikely event, would happen, then I feel that it’s not something that I would lose. (Ip2)
Belonging and finding important exchanges with peers
Through peer interaction, the participants found belonging, support and coping strategies for living with HIV.
Because they are also HIV positive, they know everything, they know what you are going through, they know what you think and how you function. (Ip6)
Being able to share those experiences and getting support about it, and also, well, also the information that comes from their physicians and so. (Ip5)
Being supported by the new knowledge, but inconsistencies create frustration
Understanding the effects of treatment on infectiousness was described as a relief. However, through exchanged experiences with their peers it became evident to the participants that medical staff communicated different information and rules to different patients. They also described how different staff at the same clinic gave different information. This resulted in frustration, unease, and misunderstandings.
There are quite different responses. Even from the same unit, institution, the response depends on who you talk to. As a person living with HIV I find this quite unpleasant. (Ip4)
When information about infectiousness was communicated, the terminology used raised challenges. They had difficulties relating to the terms “minimal risk” and “very small risk” and translating them into information relevant to their reality and communicating it to others. The terminology was perceived as conveying HIV as infectious, even when well treated.
It’s very hard to describe the position of the research with your own words. It’s very difficult to put in words the content of a theoretical risk that is so small it doesn’t even have to be considered. (Ip4)
The newer ones that come (…) Well, they are more like “But, my goodness, you are not infectious anymore!”, or something like that, yes. (Ip5)
They are bolder in other countries. My experience is that in many other countries they are more direct, like, if you are undetectable then you cannot transmit HIV. (Ip2)
Discussion
The aim was to explore how MSM living with HIV in Sweden experienced and perceived communication with clinical staff at their HIV clinic about infectiousness and the rules of conduct. Through the analysis of the interviews, the over-arching theme Navigating between rules and reality emerged. Due to inconsistencies in the information they had received from the clinical staff, MSM living with HIV in Sweden were left to navigate their everyday life partly based on this information, as well as on the information they could find out on their own or together with their peers. Thus, MSM living with HIV in Sweden had to ensure that they were aware of current rules and regulations, even when the rules were not always clearly communicated. They then drew their own conclusions regarding what rules applied to them. In a country where people living with HIV can be prosecuted for not complying with the rules of conduct (Allard, Citation2009; Elliott, Citation2003; Symington, Citation2008), this is a heavy burden to put on the individual.
We found that that uncertainties and misconceptions regarding the rules of conduct exist among MSM living with HIV in Sweden. A previous study found that misconceptions also occurred among migrants from Africa living with HIV in Sweden (Åsander, Belfrage, Pehrson, Lindstein, & Björkman, Citation2004). Studies from countries with legal frameworks of HIV similar to that of Sweden also support this finding (Dodds, Bourne, & Weait, Citation2009; Kapiriri, Tharao, Muchenje, Masinde, & Ongoiba, Citation2016). A challenge found is that even if the treating physician is consistent in the communication to one patient, discrepancies concerning what is communicated by clinical staff to patients become evident when MSM living with HIV exchange experiences with peers. Some of the inconsistencies and frustration expressed by the study participants arose from the unspecific terminology of the Swedish official statement from 2013, using the terms minimal and very low in regards to infectiousness. This can be contrasted by a statement from US CDC clearly stating that there is effectively no risk of sexual transmission of HIV from a person who achieves and maintains undetectable viral load (McCray & Mermin, Citation2017).
It is noteworthy that some MSM living with HIV in Sweden do not recall receiving their rules of conduct in accordance with the Communicable Diseases Control Act. In the law it is stated that the rules of conduct should be individual and communicated in writing, by the treating physician, as soon as possible following the diagnosis. However, as it is known that the HIV diagnosis can result in stress and trauma, including PTSD (Moskowitz, Hult, Bussolari, & Acree, Citation2009; Murphy & Hevey, Citation2013; Nightingale, Sher, & Hansen, Citation2010; Theuninck, Lake, & Gibson, Citation2010), the mental health of the individual at the time of diagnosis might affect how the information is received and recalled. Thus, the findings show the importance of giving the information repeatedly over time, adapted to individual needs, while considering the mental health of the patient.
We found that even though MSM living with HIV experienced challenges and felt frustration regarding lacking and inconsistent communication and the terminology used regarding infectiousness, they had a good relationship with the clinical staff at the HIV clinics, whom they found knowledgeable, trustworthy and welcoming. The participants’ relationships with nurses were described as especially important. Nurses do not have a formal obligation regarding the rules of conduct, in contrast to physicians, and this might influence participants’ perceptions of the various staff members.
The findings indicate that lack of sound routines and/or guidelines regarding how information is communicated to patients at HIV clinics in Sweden negatively affects MSM living with HIV. Although we found that participants experienced good relationships with the staff, contradictory and lack of information might negatively affect these relationships in the long run. Poor communication also results in a number of direct risks for the individual, one of the more serious consequences being the risk of prosecution. The law places the responsibility on the individual to know his or her obligations, but finding, understanding and interpreting the law demands a certain level of agency.
In regards to the methodology, the limited scope of the study aim and a clearly defined study population made it possible to reach saturation within ten interviews. However, it cannot be excluded that additional participants might have provided other perspectives.
Conclusion
The current study suggests that through their clinics, MSM living with HIV in Sweden should have access to correct and up-to-date information, not only concerning legal and policy aspects but also regarding scientific progress such as information about infectiousness. The establishment of sound routines and explicit guidelines for the communication of such information is crucial for improved quality of care. Finally, the participants’ expressed trust in the clinical staff seems to provide an important prerequisite for improved communication, indicating that such efforts are feasible.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Allard, P. (2009). Criminal law and cases of HIV transmission or exposure. HIV/AIDS Policy & Law Review, 14(2), 56–58.
- Åsander, A.-S., Belfrage, E., Pehrson, P. O., Lindstein, T., & Björkman, A. (2004). HIV-infected African families living in Stockholm/Sweden: Their social network, level of disclosure and knowledge about HIV. [Article]. International Journal of Social Welfare, 13(1), 77–88. doi:10.1111/j.1369-6866.2004.00299.x
- Bavinton, B., Grinsztejn, B., Phanuphak, N., Jin, F., Zablotska, I., Prestage, G., … Grulich, A. (2017). HIV treatment prevents HIV transmission in male serodiscordant couples in Australia, Thailand and Brazil. 9th IAS Conference on HIV Science (IAS 2017), Paris, France.
- Christiansen, M., Lalos, A., & Johansson, E. E. (2008). The Law of Communicable Diseases Act and disclosure to sexual partners among HIV-positive youth. Vulnerable Children and Youth Studies, 3(3), 234–242. doi:10.1080/17450120802069109
- Cohen, M. S., Chen, Y. Q., McCauley, M., Gamble, T., Hosseinipour, M. C., Kumarasamy, N. … Fleming, T. R. (2011). Prevention of HIV-1 infection with Early antiretroviral Therapy. New England Journal of Medicine, 365(6), 493–505. doi:10.1056/NEJMoa1105243
- Dodds, C., Bourne, A., & Weait, M. (2009). Responses to criminal prosecutions for HIV transmission among gay men with HIV in England and Wales. Reproductive Health Matters, 17(34), 135–145. doi:10.1016/s0968-8080(09)34475-4
- Elliott, R. (2003). Criminal Law and HIV transmission/exposure: Another Swedish Case. [Article]. Canadian HIV/AIDS Policy & Law Review, 8(1), 77–77.
- Folkhälsomyndigheten. (2014). Smittsamhet vid behandlad hivinfektion. Kunskapsunderlag från Folkhälsomyndigheten och referensgruppen för Antiviral terapi (RAV). Folkhälsomyndigheten. Retrieved from https://www.folkhalsomyndigheten.se/contentassets/09eb6d39f18b49ca83934cea3d325d11/smittsamhet-vid-behandlad-hivinfektion.pdf
- Graneheim, U. H., Lindgren, B. M., & Lundman, B. (2017). Methodological challenges in qualitative content analysis: A discussion paper. Nurse Education Today, 56, 29–34. doi:10.1016/j.nedt.2017.06.002
- Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105–112. doi:10.1016/j.nedt.2003.10.001
- Haire, B., & Kaldor, J. (2015). HIV transmission law in the age of treatment-as-prevention. Journal of Medical Ethics, 41(12), 982–986. doi:10.1136/medethics-2014-102122
- HIV-Sweden. (2012). Brittisk juridikprofessor till hårt angrepp mot Sveriges hiv-lagstiftning. Retrieved from http://www.hiv-sverige.se/brittisk-juridikprofessor-till-hart-angrepp-mot-sveriges-hiv-lagstiftning/
- IPPF. (2014). Challenging Sweden's HIV Policy. Retrieved from https://www.ippf.org/blogs/challenging-swedens-hiv-policy
- Janghorban, R., Latifnejad Roudsari, R., & Taghipour, A. (2014). Skype interviewing: The new generation of online synchronous interview in qualitative research. International Journal of Qualitative Studies on Health and Well-Being, 9, 24152. doi:10.3402/qhw.v9.24152
- Kapiriri, L., Tharao, W., Muchenje, M., Masinde, K. I., & Ongoiba, F. (2016). ‘ … they should understand why … ’ The knowledge, attitudes and impact of the HIV criminalisation law on a sample of HIV+ women living in Ontario. Global Public Health, 11(10), 1231–1245. doi:10.1080/17441692.2016.1146318
- Kazatchkine, C., Bernard, E., & Eba, P. (2015). Ending overly broad HIV criminalization: Canadian scientists and clinicians stand for justice. Journal of the International AIDS Society, 18(1), 20126. doi:10.7448/IAS.18.1.20126
- Kvale, S., & Brinkmann, S. (2009). Interviews: Learning the craft of qualitative research (2nd ed.). Thousand Oaks: SAGE Publications, Inc.
- Lo Iacono, V., Symonds, P., & Brown, D. H. K. (2016). Skype as a tool for qualitative research interviews. Sociological Research Online, 21(2), 1–15. doi: 10.5153/sro.3952
- McCray, E., & Mermin, J. H. (2017). Dear Colleague: September 27, 2017. Retrieved from https://www.cdc.gov/hiv/library/dcl/dcl/092717.html
- Mehdiyar, M., Andersson, R., Hjelm, K., & Povlsen, L. (2016). HIV-positive migrants’ encounters with the Swedish health care system. Global Health Action, 9(1), 31753. doi: 10.3402/gha.v9.31753
- Moskowitz, J. T., Hult, J. R., Bussolari, C., & Acree, M. (2009). What works in coping with HIV? A meta-analysis with implications for coping with serious illness. Psychological Bulletin, 135(1), 121–141. doi: 10.1037/a0014210
- Murphy, P. J., & Hevey, D. (2013). The relationship between internalised HIV-related stigma and posttraumatic growth. AIDS and Behavior, 17(5), 1809–1818. doi: 10.1007/s10461-013-0482-4
- Nightingale, V. R., Sher, T. G., & Hansen, N. B. (2010). The Impact of receiving an HIV diagnosis and Cognitive Processing on Psychological Distress and Posttraumatic Growth. Journal of Traumatic Stress, 23(4), 452–460. doi:10.1002/jts.20554
- Oates, J. (2015). Use of Skype in interviews: The impact of the medium in a study of mental health nurses. Nurse Researcher, 22(4), 13–17. doi: 10.7748/nr.22.4.13.e1318
- Rodger, A. J., Cambiano, V., Bruun, T., Vernazza, P., Collins, S., van Lunzen, J. … Lundgren, J. (2016). Sexual activity without condoms and risk of hiv transmission in serodifferent couples when the hiv-positive partner is using suppressive antiretroviral therapy. JAMA, 316(2), 171–181. doi: 10.1001/jama.2016.5148
- SFS 2004:168. (2004). Smittskyddslag. Stockholm: Socialdepartementet.
- Socialstyrelsen. (2013). Den behandlande läkarens och enskilde individens ansvar vid pågående behandling mot hivinfektion Dnr 3.1-40828/2013). Socialstyrelsen. https://www.socialstyrelsen.se/SiteCollectionDocuments/fortydligande-smittskyddslagen-behandling-hiv-131021.pdf
- Symington, A. (2008). Sweden: Man found guilty of infecting two women with HIV. HIV/AIDS Policy & Law Review, 13(1), 62, 64.
- Theuninck, A. C., Lake, N., & Gibson, S. (2010). HIV-Related Posttraumatic stress Disorder: Investigating the Traumatic Events. AIDS Patient Care and STDs, 24(8), 485–491. doi: 10.1089/apc.2009.0231
