
ABSTRACT
Low perceived social support (SS) negatively impacts health outcomes. We developed a measure of perceived SS for use in HIV care. We sought and categorized legacy items, selecting strongest items within categories. We elicited SS concepts from patients in English/Spanish, coded transcripts to match item pool content, and developed new items for salient unrepresented content. In focus groups, patients prioritized highly-matched items. We conducted cognitive interviews on high-priority items, and validity testing on final items against two legacy measures. From interviews (n = 32), we matched the following concepts: sense of belonging/inclusion; communication; emotional support; feeling accepted by others as a person; companionship; and practical support. We identified a new concept: support from friends/family in remaining healthy. Focus groups (n = 23) prioritized emotional support, communication, and support to remain healthy. Cognitive interviews (n = 30) found items were well-understood. The final 8-item measure performed well with patients (n = 708), with good construct validity. We used an Item Response Theory program to create a 3-item Short Form version of the measure, which captures 96% of patients indicating low social support. We developed the Multifactoral Assessment of Perceived Social Support (MAPSS) and Short Form (MAPSS-SF); brief, clinically relevant, sufficiently unidimensional measures of SS for use in HIV care.
Introduction
Lack of social support has a detrimental effect on health, increasing the risk of morbidity and mortality (Holt-Lunstad, Smith, & Layton, Citation2010) through a variety of mechanisms both physiological and psychosocial (DiMatteo, Citation2004; Hawkley, Burleson, Berntson, & Cacioppo, Citation2003; Uchino, Cacioppo, & Kiecolt-Glaser, Citation1996). Despite the large body of evidence suggesting the importance of social support to health (Broadhead et al., Citation1983; Cobb, Citation1976; Cohen, Citation1988), there remains a dearth of validated social support assessments that are brief enough for use in clinical care or that are applicable across populations (Cyranowski et al., Citation2013). We aimed to develop an improved measure to elicit patient levels of social support for use in busy HIV clinical care settings.
In the general population, insufficient social support has been linked to sub-optimal function of multiple physiological systems including the cardiac, immune, and endocrine systems (Cassel, Citation1976; Uchino et al., Citation1996). These effects are independent of changes in health behaviors, and point to direct influence of social engagement on vital systems, the mechanisms of which have been theorized widely (Cassel, Citation1976; Cohen, Citation1988; Cohen & Wills, Citation1985). Low levels of social support have also been associated with poor mental health outcomes, including high levels of depression (Krousel-Wood et al., Citation2010), and have been found to negatively impact health behaviors such as level of physical activity (Watt et al., Citation2014) and adherence to medical treatments (DiMatteo, Citation2004). Further, social support has been influential in the management of many chronic and complex medical conditions such as cancer (Costa et al., Citation2017; Pinquart & Duberstein, Citation2010), diabetes (Pamungkas, Chamroonsawasdi, & Vatanasomboon, Citation2017; Spencer-Bonilla et al., Citation2017), and HIV (Iribarren et al., Citation2017), by mitigating both the practical and emotional impact of ill health.
Among people living with HIV (PLWH), the physiological consequences of social support may be of particular importance, as metabolic, cardiovascular, and immunologic complications are common. Among PLWH, poor social support has been associated with lower adherence to antiretroviral medications (ARVs) (Scheurer, Choudhry, Swanton, Matlin, & Shrank, Citation2012) and use of unhealthy coping strategies (Iribarren et al., Citation2017; Power et al., Citation2003), while the presence of social support can predict earlier diagnosis, connection to care, and ARV adherence (Kelly, Hartman, Graham, Kallen, & Giordano, Citation2014). As a highly-stigmatized condition, HIV has a social dimension that presents a host of ongoing challenges with regards to creating and maintaining the level of social support required for optimal management of chronic illness. Social support has mediated some of the negative impacts of HIV related stigma, including decreased physical function and psychological functioning (Larios, Davis, Gallo, Heinrich, & Talavera, Citation2009).
PLWH have indicated the importance of social dimensions of health and a willingness to have it addressed in the context of clinical care (Fredericksen et al., Citation2015, Citation2016). Growing evidence suggests that there may be value in addressing social support in clinical care, given the observed relationship between poor social support and negative health outcomes and its inverse (Cassel, Citation1976; Iribarren et al., Citation2017; Kelly et al., Citation2014; Krousel-Wood et al., Citation2010; Larios et al., Citation2009; Power et al., Citation2003; Scheurer et al., Citation2012; Uchino et al., Citation1996), and that social support interventions can improve health outcomes (Hogan, Linden, & Najarian, Citation2002).
We developed the Multifactoral Assessment of Perceived Social Support (MAPSS), a brief touch-screen-administered measure for use in primary care for patients living with HIV.
Methods
Methodological overview
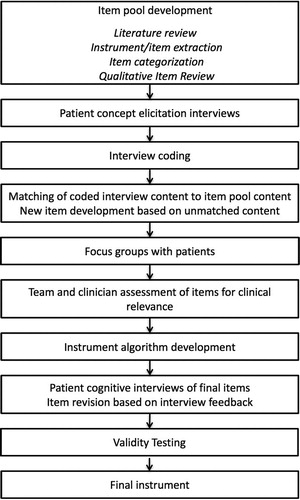
provides a methodological overview of our approach. We developed a literature review-based item pool of legacy social support items, using NIH-Patient Reported Outcomes Measurement Information System (PROMIS) protocols for instrument development (Cella et al., Citation2007). We categorized items and winnowed them within each category to best alternatives. We conducted in-depth patient interviews covering item pool content areas, coded interview transcripts to match pool content, and identified unmatched content requiring new item development. We selected items from commonly matched concepts and conducted patient focus groups to prioritize items. We conducted cognitive interviews with patients on a final set of items, and then performed validation testing on the finalized items.
Figure 1. Methodological overview.
Item pool development, categorization, and winnowing
We conducted a literature review with the assistance of health reference librarians using Medline and the Health and Psychosocial Instruments (HAPI) database to identify social support measures developed or used in care between 1965 and 2015. We used the terms social support, emotional support, and social isolation. This search yielded 38 measures (see Supplement 1). We excluded measures from population-based surveys not intended for clinical care, as well as measures not in North American English, requiring interviewer administration, targeting minors only, not known to be used in clinical care, lacking reliability or validity testing, not measuring patient perception of quality of social support, and/or measures inaccessible after two attempts to contact authors. Exclusions yielded 14 measures and 175 items (Supplement 1).
Two trained qualitative researchers separately used an open-coding process to classify candidate items, with the goal of identifying several areas of social support and later meeting to discuss possible codes for item categorization. Coders shared and reconciled into seven categories of social support: belonging/inclusion, communication, emotional support, feelings of acceptance by others, fun with others, practical support, and overall quality ratings. Within each category, coders further categorized content by theme (i.e., within the dimension of practical support, subcategories included “getting advice”, “getting help in a crisis”, and “being cared for when sick”). Coders independently performed the PROMIS Qualitative Item Review (QIR) (DeWalt, Rothrock, Yount, Stone, & Group, Citation2007) to select the best item among similar alternatives within each content area. Coders reconciled discordance in QIR coding and achieved consensus regarding best alternatives for each sub-category, resulting in a pool of 72 distinct legacy candidate items.
Study population and recruitment
For each study activity, we recruited English-speaking and Spanish-speaking patients in HIV care aged 18+ that were able to consent, from 4 U.S. clinics within the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS): Fenway Community Health (FCH)- Boston, MA; 1917 Clinic at the University of Alabama at Birmingham (UAB); Owen Clinic at the University of California at San Diego (UCSD); and Madison Clinic at Harborview Medical Center/University of Washington-Seattle (UW). For concept elicitation and cognitive interviews, we recruited patients upon arrival on-site, prior to their scheduled HIV care visit. We recruited focus group participants by telephone.
Quantitative validity testing occurred by showing the final measure within a web-based patient-reported outcomes assessment routinely administered on an iPad as part of HIV care at UCSD and UW, and as an ongoing research initiative integrated into HIV clinical care at Fenway and UAB; depending on the clinic, either research or clinic staff queried patients’ willingness to complete the assessment while waiting to see their provider. Human subjects approval for all research activity was approved by each institution’s Institutional Review Board.
Concept elicitation interviews
We used content areas to develop an interview guide that elicited concepts of social support. We invited patients for hour-long interviews in either English or Spanish, offering $30 compensation. Questions included “How would you define social support?”, “How would you describe social support in your life?” and “What does ‘good’ social support look like?”
Matching interview content and development of new content
Using Dedoose qualitative software (“Dedoose version 5.0.11”, Citation2014), two coders attempted matching interview excerpts to item pool content. Interview content matched 67 of the 72 items. Matched items were to be deemed eligible for possible inclusion in focus groups. However, 67 being too many items to realistically administer to patients, we narrowed the number down by selecting only the concepts referenced by 4+ patients. This resulted in 11 candidate legacy items. We developed three additional items from high-prevalence concepts unmatched to the item pool, totaling 14 items.
Patient focus groups
We presented 14 items to patients in both English and Spanish-language focus groups. We asked patients to organize a pile of 14 cards, upon each of which was a social support item. Patients placed cards in rank order priority of importance based on their perception of clinical relevance to PLWH. After ∼10 min, we asked patients to share and explain rationales for rank orderings. After discussion, we invited patients to change their rank order prioritizations if they desired, in case group discussion changed their mind about priorities. Patients received $50 for participation for the 90-minute group. Based on their prioritization, we narrowed the number of items down from 14 items to nine items for cognitive interviews.
Cognitive interview testing
We tested nine candidate items for comprehensibility among English- and Spanish-speaking patients in their respective languages. Interviews were up to 45 min in length; participants received $25. We reviewed less-than-unanimously understood items for opportunities to clarify.
Validity testing
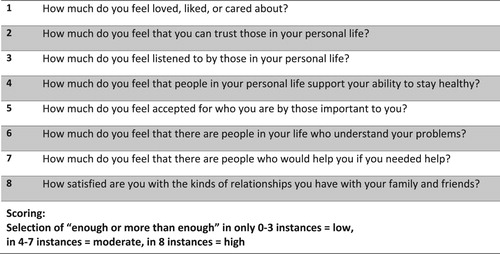
We administered the finalized measure (see ) via touch screen tablet to patients completing a routine assessment of patient reported outcomes alongside two validated measures, the Berlin Social Support Scale (BSSS) (DiMillo, Hall, Ezer, Schwarzer, & Korner, Citation2017) and the PROMIS Emotional Support Short Form (PROMIS, Citation2016). We selected these measures due to their brevity for feasible co-administration with the MAPSS in the context of clinical care.
Figure 2. Multifactoral assessment of perceived social support (MAPSS).
We assessed dimensionality using confirmatory factor analysis, with the weighted least squares with mean and variance estimator in Mplus (Muthén & Muthén, Citation2006). Criteria for model fit were Confirmatory Fit Index (CFI) CFI > 0.95, Tucker Lewis Index (TLI) >0.95, and root mean squared error of approximation (RMSEA) < 0.05 (Reeve et al., Citation2007). Item response theory (IRT) social support scores were computed in Parscale (Muraki & Bock, Citation2003). We examined differential item functioning (DIF) due to sex, sexual orientation, race, survey language, age, and HIV risk factor, using the Stata program -difwithpar- (Crane, Gibbons, Jolley, & van Belle, Citation2006). Relationships between the IRT-based MAPSS score and other measures were measured using Pearson correlation coefficients. We used a t-test to compare the item “How much do you feel that there are people who would help you if you needed help?” with the BSSS instrumental scale.
Development of the MAPSS Short Form (MAPSS-SF)
We were interested in shortening the scale for use in routine clinical care. We used Firestar, an Item Response Theory simulation program (Choi, Citation2009) to determine which three items were most useful in discriminating levels of support.
Results
A total of n = 793 patients participated in study activity; 85 patients for qualitative activity and 708 for quantitative validation testing. By site, 46% of participants were from UCSD, 23% UW, 18% UAB, and 13% from FCH.
Concept elicitation and matching to legacy scale themes
Demographic and clinical characteristics of concept elicitation interview participants (n = 32) are shown in .
Table 1. Demographic and clinical characteristics.
We matched 637 interview excerpts to legacy items with high inter-rater reliability. We identified the following concepts: sense of belonging/inclusion (e.g., feeling part of a community or group) (23 patients, or 72%); feeling fully accepted by others as a person (19 patients, or 59%); practical support (18 patients, 56%), communication (e.g., sharing thoughts or feelings with others) (15 patients, or 47%); emotional support (feeling loved/liked/cared about) (14 patients, or 44%); and companionship (11 patients, 34%). A new concept not found in the item pool was feeling supported by friends/family in efforts to remain healthy (i.e., maintaining sobriety among former substance users)(6 patients, 18%).
Patient focus groups
In focus groups (n = 23, 18 in English, 5 in Spanish, ), of the 14 items presented, groups in both languages highly prioritized feeling “loved, liked, or cared about”, feeling “listened to”, having others that one can trust, and having others that “support your well being”. Spanish-speaking patients attributed higher priority to the item, “How satisfied are you with the kinds of relationships you have with your family and friends?” than did English-speaking patients (ranked #4 vs. #11, respectively), as well as the item, “How much have you felt that there are people who would help you if you needed help?” (#2 vs. #8, respectively). Spanish-speaking patients attributed lower priority to the item, “How much can you share your feelings with those in your personal life?” (#9 vs. #2, respectively). See Supplement 2 for a full list of rank order selections.
Cognitive interview testing
Cognitive interviews (n = 30, ) included 18 English-language and 12 Spanish-language interviews. All but two items were well understood by all patients in their respective languages. In English, exceptions were “How much do you feel that people in your personal life support your well-being?” in which the concept of “well-being” was defined differently by over one-third of patients. The item and concept, “How much do you feel that you belong to a group or community?”, was poorly understood in both languages, with inconsistent interpretations among over half of patients.
Final development of MAPSS
We narrowed down the list of items from 9 to 8. We removed the “group/community” item due to low prioritization and inconsistency in interpretation of the concept. We revised the item, “How much do you feel that people in your personal life support your well-being”, changing the words “well being” to “ability to stay healthy”, which was more easily understood by patients yet still representative of the central concept. For response options, we created the binary response options “not enough” and “enough or more than enough”, deeming multi-point scales less clear in identifying whether or not a patient is satisfied with their level of social support. We phrased items in present tense, eliminating the need for a recall window.
Validity testing
We performed validity testing with 708 patients (). The final measure took an average of 43 s to complete (range: 17–77 s, median 41). Our MAPSS score was sufficiently unidimensional, with CFI = 0.999, TLI = 0.998, and RMSEA = 0.035. The median standard error of measurement (SEM) was 0.71, because 65% of the sample endorsed all the items, the highest level of social support, where the SEM was 0.71. For those endorsing none of the items, the SEM was 0.44, while for those endorsing 1–7 of the items the SEM ranged from 0.20 to 0.33. Cronbach’s alpha was 0.92. There was no salient DIF due to sex, sexual orientation, race, survey language, age, and HIV risk factor (Supplement 3).
External validity was strong, with correlations of 0.72 with the BSSS and 0.69 for the sum of the PROMIS Emotional Support Short Form items. Within the BSSS, the correlation was 0.70 for the emotional scale and 0.72 for the instrumental scale. BSSS instrumental scores were significantly higher for those that said “enough” for the item “ … there are people who would help you if you needed help?” (mean 3.6 (SD 0.6) for “enough” versus 2.3 (0.8) for “not enough”; p < 0.0001).
Development of the MAPSS Short Form (MAPSS-SF)
Simulation results clearly pointed to these 3 items for the MAPSS-Short Form: feeling “listened to by those in your personal life”, feeling “that there are people in your life who understand your problems”, and being “satisfied with the kinds of relationships you have with your family and friends”. The MAPSS-SF and the MAPSS have a correlation on 0.95. We divided participants into three groups based on their full MAPSS scores: Low (0–3 points), Medium (4–7 points) and High (8 points). On the MAPSS-SF, a sum score of 0 or 1 identified 96% of those with Low social support on the full MAPSS, the group clinicians would most want to ascertain. None of those with Low support endorsed all 3 of the MAPSS-SF items. The Medium group is less defined with the MAPSS-SF, with 31% scoring 0–1, 51% scoring 2, and 18% endorsing all 3 items. If we ask solely about feeling “listened to by those in your personal life” and stop for those who endorse that item, we will misclassify 8% of the PLWH who have Low social support as High.
Discussion
We created the MAPSS, a brief, clinically relevant, unidimensional measure of social support for patients in HIV care, inclusive of concepts of social support prioritized highly by PLWH, with simple response options, that are well-understood by both English and Spanish speakers. In addition, we developed a 3-item short form (MAPSS-SF) based on this measure for use in time-constrained clinic settings.
We grounded development of the MAPSS in prior research to select aspects of social support most relevant to health outcomes among PLWH. Social support is commonly conceptualized in two key ways. First, social support is framed as either “perceived” or “received”; in this framework, perceived support refers to subjective perceptions of the quality of support, while received support refers to, for example, enumeration of specific supportive actions offered to the recipient (Barrera, Citation1986; Taylor, Citation2011). We emphasized perceived social support, as this framing has proven more consistent in predicting health outcomes (Holt-Lunstad et al., Citation2010; Uchino, Citation2009; Uchino, Bowen, Carlisle, & Birmingham, Citation2012). The second key theoretical conceptualization distinguishes between “structural” social support, meaning the extent to which one is integrated into a social network (Krause, Citation1986); and “functional” social support, typically operationalized as emotional, instrumental (i.e., practical), informational (i.e., provision of advice), and companionship support (Uchino, Citation2004). We emphasized functional support as it is more closely related to medication adherence (DiMatteo, Citation2004; Magrin et al., Citation2015), which is critically important for PLWH. In addition, we thought it critical that the measure capture several aspects of social support. Multifactoral measures of social support have been found to be more closely associated with mortality risk than more narrowly targeted measures; Holt-Lunstad, et al., Argue that this may be due to the “multiple pathways” between social support and health outcomes represented in such measures (Holt-Lunstad et al., Citation2010).
We developed three new items that emerged from highly prevalent concepts among our patients: “How much do you feel accepted for who you are by those important to you?”, “How much do you feel that you can trust those in your personal life?” and “How much do you feel that people in your personal life support your ability to stay healthy?”. The “acceptance” item is grounded in our patients’ experience of HIV-related stigma and other types of discrimination, and its impact on their individual and social well-being (Fredericksen et al., Citation2015). The “trust” item is, in part, rooted in patient expressions of ongoing concern over unwanted disclosure of their HIV status. The “support your ability to stay healthy” item is based on discussions of the need to feel supported in their personal substance use recovery, a concept commonly relevant to many PLWH given high rates of substance abuse (Crane et al., Citation2017). All three concepts ranked in the mid-to-high range in focus group exercises.
There is a clear need for a measure of social support that is realistic for use in routine care. No existing legacy measure in our review was simultaneously comprehensive and brief enough to be feasible for routine administration in busy clinical settings. Further, to our knowledge, no validated measure has been designed specifically for use with adult PLWH in HIV care. We suspect that social support as a topic is under-addressed in most patient-provider discussions, in part due to competing clinical concerns that characterize HIV care, and provider focus on prioritizing and resolving more easily-treatable problems (Fredericksen et al., Citation2015). Yet, PLWH have emphasized the importance of addressing broader social issues (i.e., HIV-related stigma) in order to meaningfully address adverse health behaviors (Fredericksen et al., Citation2015). We have found that PLWH prioritize both HIV-related stigma and social support as among their top concerns. PLWH state they would like their HIV care providers to at least acknowledge, if not somehow address, the health impacts of HIV stigma-related social stressors (Fredericksen et al., Citation2015, Citation2016).
A key question is: how might HIV care providers meaningfully address lack of social support? Simply identifying patients with low social support may in itself be valuable, even without a specific intervention; identifying previously undefined lack of social support may alone catalyze active pursuit of solutions. Provider awareness of low social support may help contextualize patient reports of adverse health behaviors, such as anonymous condom-less sex, binge drinking, or other substance use. Prior research on health priorities of PLWH has found that such health behaviors may serve as a means of coping with broader social problems related to living with HIV such as anticipated and enacted HIV-related stigma (Fredericksen et al., Citation2015). With delivery of MAPSS results to providers, positive endorsement of any of its items may initiate discussion with the possibility of identifying a way forward.
Limitations
Design of the MAPSS is grounded in the concepts of social support elicited from PLWH in HIV care in CNICS clinics, most sites of which are located in public hospital settings. These concepts of social support do not necessarily represent those of PLWH in HIV care elsewhere. We also note that the social support needs of other sub-populations of PLWH, such as women and youth/young adults, may differ.
Strengths
Our work draws from the perspectives and feedback of a highly geographically and demographically diverse group of patients.
Conclusions
Inadequate social support is a common issue among PLWH, predictive of poor health outcomes. We developed the MAPSS, a brief, clinically relevant, 8-item measure of social support for use with English and/or Spanish-speaking PLWH, and the 3-item MAPSS-SF, that may provide social context for adverse health behaviors and catalyze patient-provider discussion toward improving patient quality of life.
Supplemental Material
Download Zip (839.3 KB)Acknowledgements
We thank our patients, as well as the Madison Clinic Patient Panel for guidance in domain selection and development of the measure. This work was funded by the Patient Centered Outcomes Research Institute (PCORI) SC14-1403-14081 with additional support from the National Institute of Allergy and Infectious Diseases (NIAID) [CNICS R24 AI067039, UW CFAR NIAID Grant P30 AI027757; and UAB CFAR grant P30 AI027767].
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Kenneth H. Mayer http://orcid.org/0000-0001-7460-733X
Additional information
Funding
References
- Barrera, M. (1986). Distinctions between social support concepts, measures, and models. American Journal of Community Psychology, 14(4), 443–445.
- Broadhead, W. E., Kaplan, B. H., James, S. A., Wagner, E. H., Schoenbach, V. J., Grimson, R., … Gehlbach, S. H. (1983). The epidemiologic evidence for a relationship between social support and health. American Journal of Epidemiology, 117(5), 521–537.
- Cassel, J. (1976). The contribution of the social environment to host resistance: The fourth wade hampton frost lecture. American Journal of Epidemiology, 104(2), 107–123.
- Cella, D., Yount, S., Rothrock, N., Gershon, R., Cook, K., Reeve, B., … Rose, M. (2007). The patient-reported outcomes measurement information system (PROMIS): Progress of an NIH roadmap cooperative group during its first two years. Medical Care, 45(5 Suppl 1), S3–S11. doi:10.1097/01.mlr.0000258615.42478.55 00005650-200705001-00002 [pii]
- Choi, S. (2009). Firestar: Computerized adaptive testing simulation program for polytomous item response theory models. Applied Psychological Measurement, 33(8), 644–645.
- Cobb, S. (1976). Presidential address-1976. Social support as a moderator of life stress. Psychosomatic Medicine, 38(5), 300–314.
- Cohen, S. (1988). Psychosocial models of the role of social support in the etiology of physical disease. Health Psychology, 7(3), 269–297.
- Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357.
- Costa, A. L. S., Heitkemper, M. M., Alencar, G. P., Damiani, L. P., Silva, R. M. D., & Jarrett, M. E. (2017). Social support is a predictor of lower stress and higher quality of life and resilience in Brazilian patients with colorectal cancer. Cancer Nursing, 40(5), 352–360. doi: 10.1097/NCC.0000000000000388
- Crane, P. K., Gibbons, L. E., Jolley, L., & van Belle, G. (2006). Differential item functioning analysis with ordinal logistic regression techniques: DIFdetect and difwithpar. Medical Care, 44(11 Suppl 3), S115–S123.
- Crane, H. M., McCaul, M. E., Chander, G., Hutton, H., Nance, R. M., Delaney, J. A. C., … Kitahata, M. M. (2017). Prevalence and factors associated with Hazardous alcohol use among persons living with HIV across the US in the current Era of antiretroviral treatment. AIDS and Behavior, 21(7), 1914–1925. doi: 10.1007/s10461-017-1740-7
- Cyranowski, J. M., Zill, N., Bode, R., Butt, Z., Kelly, M. A., Pilkonis, P. A., … Cella, D. (2013). Assessing social support, companionship, and distress: National Institute of health (NIH) Toolbox adult social relationship scales. Health Psychology, 32(3), 293–301. doi: 10.1037/a0028586
- Dedoose version 5.0.11. (2014). Sociocultural Research Consultants LLC. Retrieved from http://www.dedoose.com
- DeWalt, D. A., Rothrock, N., Yount, S., Stone, A. A., & Group, P. C. (2007). Evaluation of item candidates: The PROMIS qualitative item review. Medical Care, 45(5 Suppl 1), S12–S21. doi: 10.1097/01.mlr.0000254567.79743.e2
- DiMatteo, M. R. (2004). Social support and patient adherence to medical treatment: A meta-analysis. Health Psychology, 23(2), 207–218. doi: 10.1037/0278-6133.23.2.207
- DiMillo, J., Hall, N. C., Ezer, H., Schwarzer, R., & Korner, A. (2017). The Berlin social support scales: Validation of the received support scale in a Canadian sample of patients affected by melanoma. Journal of Health Psychology, 1359105317700968. doi:10.1177/1359105317700968.
- Fredericksen, R. J., Edwards, T. C., Merlin, J. S., Gibbons, L. E., Rao, D., Batey, D. S., … Patrick, D. L. (2015). Patient and provider priorities for self-reported domains of HIV clinical care. AIDS Care, 27(10), 1255–1264. doi: 10.1080/09540121.2015.1050983
- Fredericksen, R. J., F. E., Gibbons, L. E., Loo, S., Avendano-Soto, S., Anderson, W. A., … Crane, H. C. (2016). Prioritization of domain content areas to address in HIV clinical care among patients living with HIV and HIV care providers in the United States. Paper presented at the International Society of Quality of Life Copenhagen, Denmark.
- Hawkley, L. C., Burleson, M. H., Berntson, G. G., & Cacioppo, J. T. (2003). Loneliness in everyday life: Cardiovascular activity, psychosocial context, and health behaviors. Journal of Personality and Social Psychology, 85(1), 105–120.
- Hogan, B. E., Linden, W., & Najarian, B. (2002). Social support interventions: Do they work? Clinical Psychology Review, 22(3), 381–440.
- Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7(7), e1000316. doi: 10.1371/journal.pmed.1000316
- Iribarren, S., Siegel, K., Hirshfield, S., Olender, S., Voss, J., Krongold, J., … Schnall, R. (2017). Self-management strategies for coping with adverse symptoms in persons living with HIV with HIV associated non-AIDS conditions. AIDS and Behavior. doi: 10.1007/s10461-017-1786-6
- Kelly, J. D., Hartman, C., Graham, J., Kallen, M. A., & Giordano, T. P. (2014). Social support as a predictor of early diagnosis, linkage, retention, and adherence to HIV care: Results from the steps study. Journal of the Association of Nurses in AIDS Care, 25(5), 405–413. doi: 10.1016/j.jana.2013.12.002
- Krause, N. (1986). Social support, stress, and well-being among older adults. Journal of Gerontology, 41(4), 512–519.
- Krousel-Wood, M., Islam, T., Muntner, P., Holt, E., Joyce, C., Morisky, D. E., … Frohlich, E. D. (2010). Association of depression with antihypertensive medication adherence in older adults: Cross-sectional and longitudinal findings from CoSMO. Annals of Behavioral Medicine, 40(3), 248–257. doi: 10.1007/s12160-010-9217-1
- Larios, S. E., Davis, J. N., Gallo, L. C., Heinrich, J., & Talavera, G. (2009). Concerns about stigma, social support and quality of life in low-income HIV-positive Hispanics. Ethnicity & Disease, 19(1), 65–70.
- Magrin, M. E., D’Addario, M., Greco, A., Miglioretti, M., Sarini, M., Scrignaro, M., … Crocetti, E. (2015). Social support and adherence to treatment in hypertensive patients: A meta-analysis. Annals of Behavioral Medicine, 49(3), 307–318. doi: 10.1007/s12160-014-9663-2
- Muraki, E., & Bock, D. (2003). PARSCALE for Windows (version 4.1). Chicago: Scientific Software International.
- Muthén, L., & Muthén, B. (2006). Mplus users guide Version 4.1 ed. Los Angeles, CA.
- Pamungkas, R. A., Chamroonsawasdi, K., & Vatanasomboon, P. (2017). A systematic review: Family support integrated with diabetes self-management among uncontrolled type II diabetes mellitus patients. Behavioral Sciences, 7(3), doi: 10.3390/bs7030062
- Pinquart, M., & Duberstein, P. R. (2010). Associations of social networks with cancer mortality: A meta-analysis. Critical Reviews in Oncology/Hematology, 75(2), 122–137. doi: 10.1016/j.critrevonc.2009.06.003
- Power, R., Koopman, C., Volk, J., Israelski, D. M., Stone, L., Chesney, M. A., & Spiegel, D. (2003). Social support, substance use, and Denial in relationship to antiretroviral treatment adherence among HIV-Infected Persons. AIDS Patient Care and Stds, 17(5), 245–252. doi: 10.1089/108729103321655890
- PROMIS. (2016). PROMIS Item Bank v2.0, Emotional Support Short Form 4a. Retrieved from http://www.healthmeasures.net/administrator/components/com_instruments/uploads/PROMIS SF v2.0 - Emotional Support 4a 6-23-2016.pdf
- Reeve, B. B., Hays, R. D., Bjorner, J. B., Cook, K. F., Crane, P. K., Teresi, J. A., … Cella, D. (2007). Psychometric evaluation and calibration of health-related quality of life item banks: Plans for the patient-reported outcomes measurement information system (PROMIS). Medical Care, 45(5 Suppl 1), S22–S31. doi:10.1097/01.mlr.0000250483.85507.04 00005650-200705001-00004 [pii]
- Scheurer, D., Choudhry, N., Swanton, K. A., Matlin, O., & Shrank, W. (2012). Association between different types of social support and medication adherence. The American Journal of Managed Care, 18(12), e461–e467.
- Spencer-Bonilla, G., Ponce, O. J., Rodriguez-Gutierrez, R., Alvarez-Villalobos, N., Erwin, P. J., Larrea-Mantilla, L., … Montori, V. M. (2017). A systematic review and meta-analysis of trials of social network interventions in type 2 diabetes. BMJ Open, 7(8), e016506. doi: 10.1136/bmjopen-2017-016506
- Taylor, S. E. (2011). Social support: A review. In M. S. Friedman (Ed.), The handbook of health psychology (pp. 189–214). New York, NY: Oxford University Press.
- Uchino, B. N. (2004). Social support and physical health: Understanding the health consequences of relationships. New Haven: Yale University Press.
- Uchino, B. N. (2009). Understanding the links between social support and physical health: A life-span perspective with emphasis on the separability of perceived and received support. Perspectives on Psychological Science, 4(3), 236–255. doi: 10.1111/j.1745-6924.2009.01122.x
- Uchino, B. N., Bowen, K., Carlisle, M., & Birmingham, W. (2012). Psychological pathways linking social support to health outcomes: A visit with the “ghosts” of research past, present, and future. Social Science & Medicine, 74(7), 949–957. doi: 10.1016/j.socscimed.2011.11.023
- Uchino, B. N., Cacioppo, J. T., & Kiecolt-Glaser, J. K. (1996). The relationship between social support and physiological processes: A review with emphasis on underlying mechanisms and implications for health. Psychological Bulletin, 119(3), 488–531.
- Watt, R. G., Heilmann, A., Sabbah, W., Newton, T., Chandola, T., Aida, J., … Tsakos, G. (2014). Social relationships and health related behaviors among older US adults. BMC Public Health, 14(533), doi: 10.1186/1471-2458-14-533
