
ABSTRACT
Understanding the pathways that expose women to HIV transmission are vital in improving HIV prevention, especially among a “hidden” group of women without pre-established known risk for HIV. We investigated the pathways which place certain women at greater risk for HIV in a qualitative exploratory study with theoretical sampling using an emergent theory study design in an urban setting in Indonesia. We conducted semi-structured interviews with 47 HIV-infected women, one focus group discussion with five young women who occassionally engage in sex work, participant observation at six sex work venues and two midwife clinics, and 11 informal interviews with midwives, nurses, and obstetricians. Our research found that many women not characterized as belonging to a “high-risk group” or “key population” were nevertheless at increased risk for HIV. A history of sexual abuse, premarital sex, divorce, or involvement in sex work, often precipitated by poverty coupled with discriminatory public health policies further heightened women’s exposure to HIV. While reaching at-risk populations is a key strategy in HIV prevention, a novel and more tailored approach is needed to reach more hidden categories of women with less apparent risk behavior yet considerable risk for HIV infection.
Introduction
The HIV epidemic in Indonesia was initially concentrated in key at-risk populations, particularly among people who inject drugs (PWID) (Afriandi et al., Citation2009). However, the epidemic was predicted to spread beyond the at-risk PWID population (Des Jarlais et al., Citation2012), and certain structural policies born from normative discrimination against sexual nonconformity in Indonesia have enabled this epidemic transition to other at-risk populations as well as to “hidden” vulnerable groups (Indonesian Ministry of Health, Citation2014). With low HIV prevalence and incidence in the general population – 0.4 and 0.3 per 1000 population (UNAIDS, Citation2018) – identifying these vulnerable groups that are “hidden” among general population is relevant to HIV prevention strategy. In a cohort of clients at the biggest HIV clinic in Bandung, Indonesia collected in over seven years, only 7% women identified as female sex workers (FSW), 16% women had a history of injecting drug use (compared to 74% of men), and 26% had a positive partner (4% in men) at HIV diagnosis (Rahmalia et al., Citation2015). Notably, more than 50% of these women could not be ascribed to a pre-established HIV risk group.
Social and structural factors can increase women’s vulnerability to HIV acquisition, as seen in Nepal and Vietnam, where cultural sexual norms influence HIV vulnerability (Menger et al., Citation2015; Son et al., Citation2016). Identifying these new types of vulnerability is critical for further HIV prevention (Krishnaratne et al., Citation2016). Therefore, we set out to understand what social factors increase women’s vulnerability to HIV acquisition in Bandung in the midst of changing HIV epidemiology.
Given that socio-structural factors are multidimensional, accumulative, and difficult to assess (German & Latkin, Citation2012; Gupta et al., Citation2008), we opted for a qualitative methodological approach to facilitate identifying the vulnerability pathways leading to HIV infection among Bandung women.
Methods
Study site and population
The study took place in Bandung, an urban area with 8.5 million population and 97% identified as Muslims (Statistics Indonesia, Citation2010, Citation2017). Bandung is the capital of West Java, a province with the third highest HIV incidence in Indonesia (Adriansyah & Firdausi, Citation2017). Employment in ≥15 year olds is 51% in women and 81% in men (BPS Kota Bandung, Citation2020).
Study design and sampling
Qualitative exploratory research was conducted to investigate the vulnerabilities and retroactive pathways to HIV among women living with HIV in Bandung triangulating in-depth open and semi-structured interviews and participant observation. Theoretical sampling was applied with a total of 52 women recruited for the study via telephone or face-to-face contact. For maximum sample variation, we recruited 47 HIV-positive women, including those who dropped out or had not started treatment, for in-depth interviewing from 3 HIV clinics, 2 public health centers, 4 sex work venues, 1 midwife clinic, 1 Red Cross blood donation center, and 1 tuberculosis clinic. We recruited five women for a focus group discussion who were “indirect” sex workers (i.e., meeting online clients for sex while also having other jobs) and who tested HIV negative or have never tested to examine the dynamic of known risk with unknown HIV status. Finally, informal interviews were held with 4 obstetrician-gynecologists, 2 midwives, 1 general practitioner, and 5 nurses/HIV counselors to explore HIV testing and sexual and reproductive health (SRH) services.
Ethical consideration
All in-depth interview participants provided written or verbal informed consent. The research received ethical approval from the Health Research Ethics Committee of the Faculty of Medicine Padjadjaran University in Bandung, Indonesia No. 143/UN6.C1.3.2/KEPK/PN/2016.
Data collection
In the in-depth interviews, data were collected with open-ended questions using a continuously adapted interview guide. A total of 47 interviews were carried out at public parks, cafes, or respondents’ residence. For respondents whose male partners were involved in their HIV treatment, the partner was informed of study participation, but respondents chose whether partner could be present during interview. Only one respondent was interviewed with her husband present.
The in-depth interviews explored circumstances that potentially exposed women to HIV; sexual and marital history; and perceived power over decisions related to sex and healthcare. The lead author, native to the area and fluent in the local languages, conducted all interviews, allaying cultural and linguistic misinterpretation. Most interviews lasted between 1 and 2.5 h. The interviews were not recorded, mitigating any participant discomfort. The interviewer took notes during the interview, typed a full summary directly afterwards and made interview and analytical memos for each interview. The full summaries were written in English.
In the focus group discussion with five at risk women with unknown HIV status, we explored knowledge of HIV and their risk perception; risk behavior; and experience with HIV prevention and testing. All participants consented to audio recording prior to the interview. A co-author with experience in youth SRH programs facilitated the focus group discussion while the lead author transcribed the audio recording and translated it to English.
Participant observation was conducted during mobile VCT in 3 brothels, 2 massage parlors, and 1 karaoke bar. Informal interviews with 7 female workers at the sex work venues investigated their work situation, background, perceptions of HIV risk, and condom use. More participant observation and informal interviews with 2 midwives, 4 obstetrics-gynecologists, 5 nurses/HIV counselors, and 1 general practitioner working in sexual and reproductive health at public and private hospitals explored HIV testing and the scope of SRH services.
All data collected were stored in a password-protected folder and backed up to an external hard drive monthly. In the summaries, the researcher assigned pseudonyms unrelated to respondents’ real name.
Data analysis
The data were analyzed through inductive or open coding concurrent to data collection. The analyses were reiterated until data saturation. Axial coding was performed to facilitate the analytic process. Data management and analysis was carried out on RQDA in the r platform. Analytical validity was ensured by team approach to data analysis and coding, and by presenting initial findings to groups of colleagues and peers.
Concept definitions
We define vulnerability beyond the common interpretation in epidemiology as risk, i.e., a probability of getting infected/becoming sick/having a condition with an increment of a risk factor. In this study vulnerability is related to perceptions, underlying social structures, and cultural logics rendering individuals susceptible to a disease by choice or by circumstance (Nichter, Citation2001).
HIV exposure refers to exposure via unprotected sexual transmission.
Sex work refers to all sexual activities where women received money or other material gains and perceived the activity as “work”. It includes transactional sex between a mistress and her “sugar daddy”, but not between a girlfriend and a boyfriend, nor a wife and her polygamous husband even though men in these relationships provide financial support.
Results
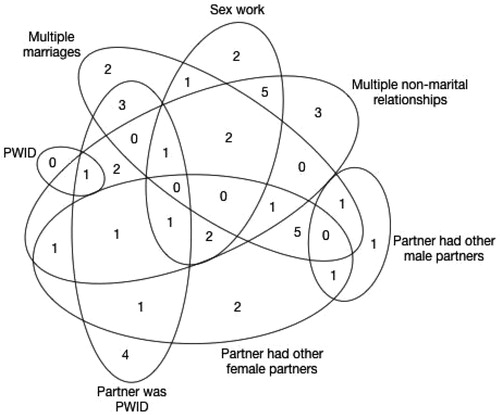
Based on our findings, we defined two categories of HIV transmission risk: women’s risk (sex work; multiple marriages; multiple non-marital sexual partners; PWID) and their sexual partner’s risk (PWID; had other female/male sexual partners). Theoretical saturation was reached upon completing semi-structured interviews with 47 women living with HIV, a focus group discussion with five young women engaging in occassional sex work and with unknown HIV status, participant observations and 11 informal interviews at sex work venues, public health centers, midwife clinics, and obstetrics and gynecology clinics at public and private hospitals.
Sample characteristics and HIV transmission risk
All women living with HIV were between 18 and 42 years old, some with a rural upbringing, some having worked elsewhere in Indonesia. Ten women had dropped out of school at various levels. Six women had never been married nor had any children. Of the 15 women with a history of sex work, 10 were diagnosed during a screening at sex work venues (). Twelve women were diagnosed while pregnant: seven at antenatal care, three through a positive partner, and two based on symptoms. Six women had experienced sexual harassment or rape and 11 had experienced partner violence.
Table 1. Characteristics of HIV-positive women (n = 47).
Given that HIV transmission risks can overlap, a Venn diagram was constructed (). Partner’s risk behaviors were discovered after HIV diagnosis through women’s personal inquiries, or with the help of a counselor. Eight respondents chose not to inquire. The HIV transmission route could not be identified for four respondents.
Figure 1. Venn diagram showing characteristics related to HIV transmission risk of the study participants. Possible HIV transmission risks were not identified in four participants.
Pathways leading to HIV transmission
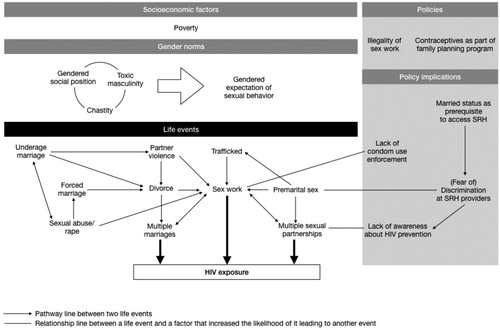
We found several plausible pathways leading to respondents’ HIV exposure (). Frequently precipitated by sexual abuse, premarital sex, or divorce, set to the backdrop of external systemic vulnerability, such as unequal gender norms, socioeconomic vulnerability, and discriminatory public health policies, respondents tended to be less discriminating in their subsequent sexual/romantic relationships, went on to have multiple marriages, multiple sexual partnerships, or engaged in sex work – leading to HIV exposure. These pathways all shared a common thread, namely (self)marginalization due to (in)voluntary nonconformity to social norms.
Figure 2. The pathways of life events leading up to HIV exposure (under the blue box). Women have different events as starting point. The external factors (under the gray boxes) surrounding the life events are socioeconomic factors, gender norms, and government policies related to sex work and sexual and reproductive health.
Sexual abuse
Six respondents cited suffering from sex abuse. One victim of childhood sexual abuse grew up believing in the taboo placed on her – a ruined woman.
“ … I woke up to find my stepbrother on top of me, and I felt something wet … I was eight years old. I was too afraid to ask anyone, not even my mother. It happened several times … After that, I felt different. I felt sinful … When I got older, I felt like a broken person. I felt worthless. No good man will ever want me … .” (Rukmini, 37)
Premarital sex
Women whose first sexual experience was consensual premarital sex also accepted their HIV diagnosis as deserved. Seventeen respondents cited losing virginity to a boyfriend.
“ … I had sex with a boyfriend back then … when I married my husband I felt lucky that he wanted me even though he knew I was not a virgin. So when he later told me he was HIV positive, I knew I had to accept him for he had accepted me [not being a virgin at marriage].” (Rininta, 38)
Divorce
Divorce was also stigmatizing and compelled many women to remarry whoever would take them, while simultaneously also breeding the perception that they were only worthy of a certain caliber of man. Eight respondents divorced and remarried before HIV diagnosis. Among divorced women, decisions to quickly remarry often meant only later discovering their new husband’s extramarital sexual relationships and HIV risk. Believing she needed to remarry, but that she was only good enough for certain kinds of men, one woman chose to marry a divorced man over a bachelor only to find out that he had another wife after he had died of AIDS.
“ … my boss set me up with his nephew. We went out several times, and he gave me a gold bracelet as a promise. I returned it when I met this man … I thought that was the right thing [to do]. The boss’ nephew is a good man, but he’s a bachelor … He deserves a young unmarried woman … The other man was ten years older than me and he said he’d been married. So I thought we were more compatible. If I’d known then that he still had a wife I wouldn’t have married him.” (Maemunah, 38)
Multiple marriages
Five respondents had an arranged marriage for financial reasons. This set them on a cycle of divorces and remarriages that eventually exposed them to HIV.
I got married three times. I was fifteen when I got married the first time. I am the oldest child and I have five younger siblings. My parents were poor … I was arranged to marry a distant relative soon after I graduated junior high school. I only met him once before marriage. I didn’t want to get married then, but my parents had to marry me off because it helped with their finances. (Neni, 40)
I did not finish school because I got married … He was around twenty at the time and I was fourteen. He asked my parents to marry me. We were poor so my parents said yes … But he hardly ever gave me any money … We moved a lot to find cheap rent … Once I caught him cheating, and he got enraged. He hit me and dragged me by my hair across the room. But he didn’t want to divorce … so I left him and looked for work … One day this man offered to give me a ride … He was very nice. We became really close … He could give me up to 50k IDR [USD 3.50] per day. My husband has never done that. Even to get 10k IDR [USD 0.7] to buy food was very difficult. Sometimes I felt like a beggar asking him for money. (Tati, 39)
Sex work
Marginalization and poverty also led to sex work. Some women were advised by close friends to pursue sex work after already having lost their virginity. Limited job opportunities – besides factory work – also fueled engaging in sex work. Ten respondents cited financial constraints as accelerants to sex work.
“ … I started working [as a sex worker] to pay for my younger siblings’ education. My mother doesn’t work, and my father isn’t there … Me and my siblings have different fathers and none of them give my mother money … I would work until all my siblings finish high school. This kind of job should end with me.” (Esti, 21)
“ … Maybe I was drugged, because I hardly remember what happened … When I told my parents about [the rape], they were furious. My father went to look for him and urged him to marry me immediately. We got married a month later … Two days after the wedding, a woman with a baby came looking for my husband … Apparently she was the first wife of my husband … I had no idea he has a wife … After that, sometimes he’d stay for a few days and then left, maybe to his first wife’s home, or maybe somewhere else … I didn’t want to ask for a divorce. I was already a ruined person, and being divorced wouldn’t be a good thing.” (Nina, 29)
Systemic elements
Institutional discrimination and structural inequality further heightened women’s vulnerability to HIV exposure; pregnant teenage girls were forced to leave school as cited by three respondents; and unmarried women were denied free contraceptives at SRH clinics as experienced by two respondents.
Sex work criminalization
Policies making sex work illegal bred underground brothels and illicit sex work activities at karaoke bars or massage parlors, complicating sexually transmitted infection (STI) prevention and screening programs. Five FSW respondents cited the challenges of asking clients to use condom in underground brothels.
Full quotes illustrating these findings are found in the Supplementary material table.
Discussion
This study shows that a complex interplay of factors affect women’s vulnerability to HIV in Bandung, Indonesia. In particular, (in)voluntary deviations from social norms, such as suffering from sexual abuse, pre- and extramarital sex, divorce, or sex work, pave pathways to HIV infection among a hidden group of at-risk women. Social and structural inequalities, such as poverty, discriminatory policies for sex work, and unequal access to sexual and reproductive health programs further accelerate these pathways to HIV infection.
Sex work criminalization, condom confiscation by law enforcement, and sex work venue licensing (UNDP, Citation2012) has hampered STI prevention and increased transmission risk due to the lack of condom enforcement at sex work establishments (Basuki et al., Citation2002), workers operating outside of the system (UNDP, Citation2012), lack of risk perception among clients (Fauk et al., Citation2018), and the power imbalance in condom negotiation between clients and workers (Muchomba et al., Citation2015). However, outside of sex work, the systemic denial of access to contraceptives at SRH services for unmarried women (IPPF, Citation2016) is but one example of structural discrimination against a “hidden” vulnerable group of women that exponentially increases their vulnerability to HIV exposure.
Stigma surrounding premarital sex has also facilitated HIV expansion. Though unmarried women are not expected to have sex, extramarital sex among youth is quite common (Irmawaty, Citation2013). Yet the lack of knowledge on safe sexual behavior due to poor sexual education may have diminished risk perception for HIV transmission (Wong, Citation2012) as most schools avoid sexual education altogether or only discuss biological aspects (Creagh, Citation2004; Pakasi & Kartikawati, Citation2013). A school-based sexual education program reaching over 81,000 teenagers in West Java (Pohan et al., Citation2011) was only permitted to promote abstinence (Sumintardja et al., Citation2011) due to prevailing norms that youth sex is unhealthy or dangerous (Holzner & Oetomo, Citation2004). Moreover, structural gender inequalities in sexual behavior stigmatizing women having engaged in premarital sex (Keleher & Franklin, Citation2008) may account for young unmarried women with sexual experience being more likely to resort to sex work (Miller et al., Citation2011).
Perception of nonconformity led to (self)marginalization that increased HIV exposure. An orthodox interpretation of religious tenets restricting the ways in which gender, sex, and reproductive matters are viewed in Indonesia (Bennett, Citation2005). While general HIV prevalence is lower in Muslim majority countries (Drain et al., Citation2006), expectations of conformity to religious and social norms invokes guilt in women with (in)voluntary deviations. Involving religious leaders in HIV education (Kemper et al., Citation2016) should be implemented with caution; the use of language that judge certain behaviors could reinforce marginalization.
This study has several limitations. We strove for maximum variation in the process of purposive sampling, but some women and their vulnerabilities may have remained elusive. The retrospective nature of data collection signifies that the perceptions of certain life events reflects what respondents feel now versus when they happened. But as most were major life events, we believe that their significance remains accurate. To our knowledge, this is the first study investigating the intersect between characteristics of HIV-infected women in Indonesia and their vulnerabilities in the pathways to HIV exposure.
Though these “hidden” at-risk women suffered from external social and structural marginalization, their acquiesence of and conformity to this marginalization further accelerated their pathways to HIV exposure. While reaching at-risk populations is a key strategy in HIV prevention, a novel and more tailored approach is needed to reach those with less apparent risk behavior. Improving access to SRH education and services regardless of marital status and incorporating HIV testing in these services would contribute to HIV prevention among women in Indonesia.
Acknowledgements
We would like to express our deepenst thanks to the counselors at the HIV clinics in Hasan Sadikin General Hospital, Ujungberung General Hospital, PKBI, and Rumah Cemara who provided us with access to their clients. We would also like to thank our research assistant Eli Rohaeli. We are most grateful to all women and health personnel for their time and efforts while participating in the study and their confidence in our research. We extend our gratitude to Elizabeth Toomer for her tremendous help in language editing of this manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adriansyah, A. A., & Firdausi, N. J. (2017). Trend of new HIV cases in Indonesia 2012–2016. Medical and Health Science Journal, 1(2), 1–12.
- Afriandi, I., Aditama, T. Y., Mustikawati, D., Oktavia, M., Alisjahbana, B., & Riono, P. (2009). HIV and injecting drug use in Indonesia: Epidemiology and national response. Acta Medica Indonesiana, 41(Suppl 1), 75–78. http://www.ncbi.nlm.nih.gov/pubmed/19920303
- Basuki, E., Wolffers, I., Devillé, W., Erlaini, N., Luhpuri, D., Hargono, R., Maskuri, N., Suesen, N., & van Beelen, N. (2002). Reasons for not using condoms among female sex workers in Indonesia. AIDS Education and Prevention, 14(2), 102–116. https://doi.org/10.1521/aeap.14.2.102.23901
- Bennett, L. R. (2005). Women, Islam and modernity: Single women, sexuality and reproductive health in contemporary Indonesia. Taylor & Francis. https://books.google.fr/books?id=hHt_AgAAQBAJ
- BPS Kota Bandung. (2020). Kota Bandung Dalam Angka 2020, 350.
- Creagh, S. (2004). [High school level sex education in Yogyakarta]. Australian Consortium For In Country Indonesian Studies and Faculty of Social and Political Sciences Universitas Muhammadiyah Malang.
- Des Jarlais, D. C., Feelemyer, J. P., Modi, S. N., Arasteh, K., Mathers, B. M., Degenhardt, L., & Hagan, H. (2012). Transitions from injection-drug-use-concentrated to self-sustaining heterosexual HIV epidemics: Patterns in the international data. PloS One, 7(3), e31227. https://doi.org/10.1371/journal.pone.0031227
- Drain, P. K., Halperin, D. T., Hughes, J. P., Klausner, J. D., & Bailey, R. C. (2006). Male circumcision, religion, and infectious diseases: An ecologic analysis of 118 developing countries. BMC Infectious Diseases, 6(1), 172. https://doi.org/10.1186/1471-2334-6-172
- Fauk, N. K., Kustanti, C. Y., Liana, D. S., Indriyawati, N., Crutzen, R., & Mwanri, L. (2018). Perceptions of determinants of condom use behaviors among male clients of female sex workers in Indonesia: A qualitative inquiry. American Journal of Men’s Health, 12(4), 666–675. https://doi.org/10.1177/1557988318756132
- German, D., & Latkin, C. A. (2012). Social stability and HIV risk behavior: Evaluating the role of accumulated vulnerability. AIDS and Behavior, 16(1), 168–178. https://doi.org/10.1007/s10461-011-9882-5
- Gupta, G. R., Parkhurst, J. O., Ogden, J. A., Aggleton, P., & Mahal, A. (2008). Structural approaches to HIV prevention. The Lancet, 372(9640), 764–775. https://doi.org/10.1016/S0140-6736(08)60887-9
- Holzner, B. M., & Oetomo, D. (2004). Youth, sexuality and sex education messages in Indonesia: Issues of desire and control. Reproductive Health Matters, 12(23), 40–49. https://doi.org/10.1016/S0968-8080(04)23122-6
- IMPACT, H. P. A. S. W. G. (2011). Teacher’s handbook: Reproductive health education. E. N. Sumintardja, T. Hidayat, B. Alisjahbana, L. Pinxten & H. J. Hospers (Eds.). Bandung: Faculty of Medicine Universitas Padjadjaran.
- Indonesian Ministry of Health. (2014). Estimates and projection of HIV / AIDS in Indonesia 2011-2016. Jakarta. http://www.ino.searo.who.int/LinkFiles/HIV-AIDS_and_sexually_transmitted_infections_Estimates_and_Projection_HIV_AIDS_ENGLISH.pdf
- IPPF. (2016). Overprotected and underserved: The influence of law on young people’s access to sexual and reproductive health in Indonesia.
- Irmawaty, L. (2013). Premarital sex behavior of university students. Jurnal Kesehatan Masyarakat, 9(1), 44–52. https://doi.org/1858-1196
- Keleher, H., & Franklin, L. (2008). Changing gendered norms about women and girls at the level of household and community: A review of the evidence. Global Public Health, 3(SUPPL. 1), 42–57. https://doi.org/10.1080/17441690801892307
- Kemper, S., Sihaloho, E. D., Siregar, A. Y. M., Tromp, N., & Baltussen, R. (2016). Cost analysis of religious based HIV/AIDS information, education and communication in Bandung, Indonesia, 1–14. https://niche1.nl/resources/content/publication_file_177_sophie_kemper_article._cost_analysis_of_religious_based_education.pdf
- Krishnaratne, S., Hensen, B., Cordes, J., Enstone, J., & Hargreaves, J. R. (2016). Interventions to strengthen the HIV prevention cascade: A systematic review of reviews. The Lancet HIV, 3(7), e307–e317. https://doi.org/10.1016/S2352-3018(16)30038-8
- Menger, L. M., Kaufman, M. R., Harman, J. J., Tsang, S. W., & Shrestha, D. K. (2015). Unveiling the silence: Women’s sexual health and experiences in Nepal. Culture, Health and Sexuality, 17(3), 359–373. https://doi.org/10.1080/13691058.2014.937462
- Miller, C. L., Fielden, S. J., Tyndall, M. W., Zhang, R., Gibson, K., & Shannon, K. (2011). Individual and structural vulnerability among female youth who exchange sex for survival. Journal of Adolescent Health, 49(1), 36–41. https://doi.org/10.1016/j.jadohealth.2010.10.003
- Muchomba, F. M., Chan, C., & El-Bassel, N. (2015). Importance of women’s relative socioeconomic status within sexual relationships in communication about safer sex and HIV/STI prevention. Journal of Urban Health, 92(3), 559–571. https://doi.org/10.1007/s11524-014-9935-y
- Nichter, M. (2001). Risk, vulnerability, and harm reduction: Preventing STIs in Southeast Asia by antibiotic prophylaxis, a misguided practice. In C. M. Obermeyer (Ed.), Cultural perspectives on reproductive health (pp. 333). Oxford University Press.
- Pakasi, D. T., & Kartikawati, R. (2013). Between needs and taboos: Sexuality and reproductive health education for high school students. Jurnal Makara Seri Kesehatan, 17(2), 79–87. https://doi.org/10.7454/msk.v17i2.xxxx
- Pohan, M. N., Hinduan, Z. R., Riyanti, E., Mukaromah, E., Mutiara, T., Tasya, I. A., Sumintardja E.N., Pinxten W.J.L., Hospers, H. J. (2011). HIV-AIDS prevention through a life-skills school based program in Bandung, West Java, Indonesia: Evidence of empowerment and partnership in education. Procedia - Social and Behavioral Sciences, 15, 526–530. https://doi.org/10.1016/j.sbspro.2011.03.135
- Rahmalia, A., Wisaksana, R., Meijerink, H., Indrati, A. R., Alisjahbana, B., Roeleveld, N., van der Ven, A. J. A. M., Laga, M., & van Crevel, R. (2015). Women with HIV in Indonesia - are they bridging a concentrated epidemic to a wider community? BMC Research Notes, 8(1), 757. https://doi.org/10.1186/s13104-015-1748-x
- Son, D. T., Oh, J., Heo, J., Huy, N. V., Minh, H. V., Choi, S., & Hoat, L. N. (2016). Early sexual initiation and multiple sexual partners among Vietnamese women : Analysis from the multiple indicator cluster survey, 2011 early sexual initiation and multiple sexual partners among Vietnamese women : Analysis from the multiple Indicator Clu. Global Health Action, 9(1), 29575. https://doi.org/10.3402/gha.v9.29575
- Statistics Indonesia. (2010). Hasil Sensus Penduduk 2010 Provinsi Jawa Barat. West Java Census 2010.
- Statistics Indonesia. (2017). Jawa Barat province in figures 2017.
- UNAIDS. (2018). Country factsheets Indonesia 2018. https://www.unaids.org/en/regionscountries/countries/indonesia
- UNDP. (2012). Sex work and the law in Asia and the Pacific.
- Wong, L. P. (2012). Qualitative inquiry into premarital sexual behaviours and contraceptive use among multiethnic young women: Implications for education and future research. PloS One, 7(12), e51745. https://doi.org/10.1371/journal.pone.0051745
