
ABSTRACT
This study focused on the creation and validation of an instrument to measure mental health professionals’ attitudes towards people living with HIV/AIDS. Rasch analyses (Rash, 1960, 1980) provided evidence to support a twodimensional (societal and personal dimensions) measurement of this attitude construct.
In the United States (U.S.), people living with HIV/AIDS (PLHIV) are a group equal in size (1.2 million; Centers for Disease Control and Prevention [CDC], Citation2020) to the number of active duty U.S. military personnel (U.S. Dept. of Defense, Citation2016). PLHIV share history, language, symbols, values, beliefs, and should be viewed as a unique, diverse culture group. As such, they should be viewed from a multicultural vantage point. A variety of mental health professionals (MHPs) such as counselors, psychologists, psychiatrists, psychiatric nurse practitioners (or other nurses trained in mental health service delivery), clinically trained social workers, or other professionals specifically trained in mental health service delivery may work with PLHIV. Yet the level to which MHPs are specifically competent to provide needed mental health services to PLHIV is unknown. The counseling profession values multicultural approaches to the therapeutic relationship, as evidenced by the American Counseling Association’s (ACA) ACA Code of Ethics (Citation2014) and the Multicultural and Social Justice Counseling Competencies (MSJCC) (Ratts et al., Citation2015). Counseling’s MSJCC include knowledge, attitudes, skills, and action as the cornerstones of competency (Arredondo et al., Citation1996; Ratts et al., Citation2015). This structure of competence has been the basis for several competency scale constructions to determine level of MHPs competency with diverse populations (Bidell, Citation2005; O’Hara et al., Citation2013; U. S. Dept. of Health and Human Services, Citation2008). Such a measure is needed to evaluate competency in working with PLHV. Rose et al. (Citation2015) created an instrument to measure counselors’ level of HIV/AIDS knowledge through the creation of the Professional Counselor HIV/AIDS Knowledge Questionnaire (PC-HA-KQ). They found that, on average, professional counselors’ and counseling students’ knowledge about HIV/AIDS was more accurate than that of the general public. However, Rose et al.’s (Citation2015) study did not address MHPs’ attitudes towards PLHIV.
According to social psychologists, attitudes are possibly the most significant part of human interaction (Gawronski, Citation2007). It would stand to reason that attitudes within the therapeutic relationship are of utmost importance to understanding the competence level of a MHP working with a client infected or affected by HIV/AIDS. What is more, attitudes are intertwined with knowledge and experience (Carney et al., Citation1994; Gawronski, Citation2007; Rose et al., Citation2015). As Petty et al. (Citation2007) contended, attitudes operate on a higher-order cognitive level and can change over time based on new information taken in through learning or experiences. Use of an appropriate attitude scale may provide helping professions with evidence needed to justify an increase in focus on students’ and practitioners’ attitudes toward PLHIV. As result, it could help to cultivate HIV/AIDS-related university programing, professional workshops, seminars, and conferences that aim to increase mental health professionals’ knowledge regarding PLHIV. Such an instrument could also be beneficial with MHPs who provide clinical mental health services. If a supervisor needs to determine which MHP to assign a PLHIV to for services, it would be of great benefit to that supervisor to know who among their staff has a favorable attitude towards such a client.
While no instrument exists to measure MPHs’ attitudes toward PLHIV, examples exist of ways to consider general AIDS attitudes. The first AIDS Attitude Scale (AAS1) was authored by Shrum et al. (Citation1989). The benefit of this initial scale addressing AIDS attitudes is the fact it even existed; that researchers recognized the need to better understand the attitudes surrounding the disease and those suffering from it. The drawbacks of this instrument, however, are many. For one, it was lengthy (54 items) which poses issues for participation completion and for narrowing down specific factors loaded within the scale. This was confirmed when the authors noted 12 factors which showed statistical weight for the instrument, but only three were able to be identified. This suggests the instrument is measuring a variety of elements which may or may not be relative to attitude towards AIDS. Another drawback is that only content validity evidence was provided and only internal consistency reliability was identified in the statistical analysis. The authors further indicated the instrument was only suitable for health education students (the sample used in the study). Based on this recommendation, the instrument’s limitations, and lack of research establishing validity with other demographics, the AAS1 is not an appropriate instrument for other populations.
The next AIDS Attitude Scale (AAS2) was created by Froman et al. (Citation1992) and focused on nurses’ attitudes. It’s first version consisted of 83 items, then was reduced to 27. After initial administration to nursing students, 6 questions were removed to make it a 21-item instrument which was then given to nursing and education students. Questions remained on the instrument, however, which referred to attitudes toward homosexuality instead of attitudes towards AIDS. An example is, “If I found out that a friend of mine was homosexual, I would not maintain the friendship” (p. 151). Such questions do not look at attitude towards AIDS; they look at attitude towards homosexuality. The authors claimed to identify two primary factors called Avoidance and Empathy. Closer investigation of the factors demonstrates problematic issues, such as victim blaming as a facet of the Avoidance factor. Further issues arise with many of the questions themselves. For example, three questions that deal with intravenous drug use (IVDU) and AIDS are in the factor of Avoidance, but it is not possible to know with the questions if the “avoidance” is relative to AIDS, of those who use illicit drugs, or those who use needles to use drugs. Four questions gauge attitudes regarding homosexuality and not AIDS. Here again, it is ambiguous if the attitude fueling the answer of these questions is about the construct of attitude towards AIDS or of the attitude towards homosexuality construct. What is more, two of the homosexuality questions do not even mention AIDS, they merely ask about homosexuality, which clearly indicates a respondent is indicating their attitude about that sexual orientation. Doing so decreases the instrument’s ability to measure one attitude construct (i.e., attitude towards AIDS) at a time when the items bring in attitudes about differing constructs (e.g., homosexuality). The second reason why the AAS2 is not an appropriate measure for MHPs is that it was created specifically for nurses and education students and therefore is not generalizable to other populations (Froman & Owen, Citation1998). The final concern is the authors contend their instrument is only appropriate for test/re-test situations and does not provide a view of AIDS attitudes if only administered once. The new instrument for MHPs sought to ensure an instrument can appropriately measure attitude towards PLHIV with a respondent only needing to complete it one time.
In continuing their work, Froman and Owen (Citation2001) took the AAS2 and reworded it for the general public, creating the AIDS Attitude Scale, General Public (AAS-G). Of note is that 47% of the samples used for the AAS-G testing were also registered nurses and/or nursing students, suggesting a fairly homogeneous sampling as the AAS2 even when it was intended to investigate non-medical personnel. With the questions reworded for use by the lay person, the AAS-G would sound on the surface to be applicable for use with MHPs, yet no MHPs were part of the original sample. In truth, such use of the AAS-G would negate the ability to investigate specific attitudes relating to issues MHPs would be exposed to that the general public would not (e.g., mandated reporting). Additional disadvantages of the AAS-G come from the same as its AAS2 predecessor. Specifically, questions ask about avoidance of homosexuals and IVDU and not just of AIDS, and it also requires test/re-test to determine a samples’ attitude.
These past measures are problematic because they (a) fail to provide psychometric support of accurate, unidimensional measurement of attitude; (b) look at the final stage of the disease process (AIDS) only; (c) fail to look at attitude towards PLHIV, instead of the virus (HIV) or disease (AIDS); (d) utilize questions which further stigmatize PLHIV; and (e) do not address specific situations nor competency elements of MHPs. Consequently, a new instrument is needed. This paper reports on the development of a Mental Health Professionals’ Attitude Towards People Living with HIV/AIDS Scale (MHP-PLHIV-AS).
The present authors developed and validated a qualitatively meaningful and statistically defensible measure of Mental Health Professionals’ Attitude Towards People Living with HIV/AIDS. The research questions were: Do items on the MHP-PLHIV-AS measure a unidimensional construct (attitudes towards PLHIV), or is there evidence of several dimensions within the data? Is the item ordering within each dimension theoretically meaningful (i.e., how well does it correspond to the construct theory)? How reliable is the item ordering within each dimension (i.e., do the items measure distinct levels of attitude within standard error estimates)? How well are the answer categories functioning and in what ways? And finally, how well do the items separate participants into statistically distinct and meaningful levels of attitude?
Method
Phase I: construction
In an effort to enhance clarity of the MHP-PLHIV-AS’s content validity, an established and accepted statistical manner of item inclusion was used for this study; namely, the approach first introduced by Lawshe (Citation1975). Lawshe proposed that individuals who are experienced at performing the task being investigated are qualified to determine the domain (and its categories) of investigation. To that end, Lawshe conveyed both a method and quantitative measurement to help improve content validity of an instrument through the meticulous development of its items. Lawshe indicated that a panel of experts, a “Content Evaluation Panel” (CEP; p. 566), be constructed to define the domain, facets, and relevant items accordingly. For the MHP-PLHIV-AS, a CEP of six HIV/AIDS experts collectively constructed a set of statements. With a panel of this size, all members were required to define an item as essential in order for it to be included (Lawshe, Citation1975; Wilson et al., Citation2012). The CEP included a State of Ohio Public Health Official with 26 years of HIV/AIDS experience; an Ohio dually Licensed Professional Counselor and Licensed Social Worker with 25 years of HIV/AIDS experience; an Ohio Licensed Professional Clinical Counselor with 24 years of HIV/AIDS experience; an Ohio county Health Department Disease Intervention Specialist with 18 years of HIV/AIDS experience, and a second Ohio county Health Department Disease Intervention Specialist with 2 years of HIV/AIDS experience.
The methodology for the instrument development followed the framework developed by Wolfe and Smith (Citation2007): (a) define the purpose, (b) identify the specifications of the instrument, (c) develop the items (Enos, Citation2008), (d) expert reviews, and (e) pilot test. The CEP used this structured approach, along with the researchers’ construct theory, to guide scale development.
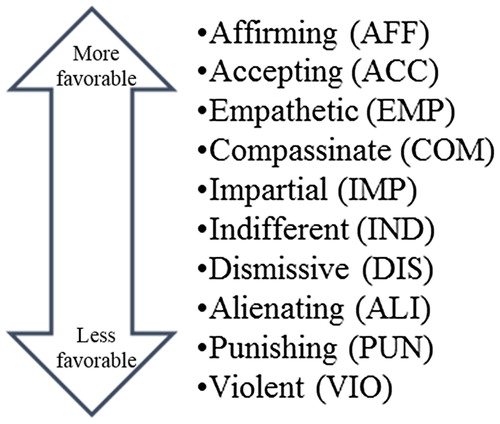
The original construct theory provided a hypothesized unidimensional construct ranging from a less favorable to more favorable attitude. Qualitative labels were created by the CEP as a guide in their writing items to represent a progression of attitude along a continuum. Item development along a linear continuum served to test that the construct was unidimensional. The CEP then wrote statements within each attitude level and determined a 4-point agreement rating scale (“1 = Strongly Disagree, 2 = Disagree, 3 = Agree, 4 = Strongly Agree”) for each item. Wolfe and Smith (Citation2007) strongly encouraged a four-category option. They argued against the inclusion of a fifth, mid-range “neutral” option because participants are likely to choose neutrality for reasons other than the construct under investigation, thus decreasing reliability and validity. The CEP supported this view, with the understanding that after the pilot study it could be changed if necessary. represents the initial levels of the construct.
Figure 1. Levels of the “attitude towards PLHIV” construct.
Data analysis
Data were analyzed with the Rasch Measurement Model (RMM) (Rasch, Citation1960, Citation1980) using the Winsteps computer software, Version 3.70.1.1 (Linacre, Citation2011). The Rasch model transforms Likert-type ordinal data into continuous, equal interval units (logits) and tests the extent to which the data fit a unidimensional additive model suitable for summation, parametric statitsics, and valid inferences made at the level of the construct rather than the individual item. The RMM models the relationship between a person’s ability and the difficulty of the item in a probabilistic fashion, based on the foundational principles of measurement, such as equal-interval, additivity, and invariance (Rasch, Citation1960, Citation1980). One of the significant benefits of utilizing RMM is that the analysis provides evidence to support the extent to which one can infer reliability and validity about the quantifiable structure of the attitude variable. When unidimensionality is determined, for example, it demonstrates the instrument’s content validity (i.e., if the items are unified, their content is based on the construct of investigation). As such, RMM gives a strong foundation to the instrument and its use and interpretation.
Specific RMM diagnostic benchmarks were established in order to ascertain if the construct is unidimensional or multidimensional. Evidence of unidimensionality required that all items have positive point-biserial correlations, Rasch factor analysis yield variance accounted for by the measure as ≥50% (Linacre, Citation2005), ≤10% first contrasting variance, and <2.0 eigenvalue (Linacre, Citation2005, Citation2016). To investigate if the response categories were functioning appropriately, rating scale category probability was set at .5 (50%) (Linacre, Citation2002, Citation2006) for each category (“1 = Strongly Disagree, 2 = Disagree, 3 = Agree, 4 = Strongly Agree”) as supporting evidence of distinct, respondent usage of each category.
Phase II: pilot
The study was subjected to an appropriate university Internal Review Board (IRB) for use of the instrument, adult informed consent, and study procedures. Because participant recruitment and data collection were facilitated by professional counselors, the research practices conformed to the American Counseling Association’s ACA Code of Ethics (Citation2014). Phase II participants were recruited from master- and doctoral-level students of psychology, counseling, and social work. Recruitment was done with the assistance of graduate-level program class instructors who were asked to provide the participation activity to their students. Snowball sampling also occurred, such that qualifying graduate students were encouraged to share the opportunity to participate with other mental health graduate students. Such students were already providing mental health related services to clients through practicum and internship placements. They qualified for participation after being provided informed consent, the opportunity to discuss any questions or concerns, and gave their consent to participate and to withdraw at any time.
The pilot assessed the functioning of the 4-point rating-scale in capturing the distinctions made by the respondents, the wording of the items, length of the instrument, and the extent to which the items measured the construct under investigation (i.e., attitudes towards PLHIV). Forty-three graduate students in counseling, social work, and psychology served as the Phase II pilot sample (n = 43). This is an appropriate pilot sample size for RMM when a validation phase is to be conducted next (Linacre, Citation2016). The pilot phase participants’ ages ranged from 22 to 56 (M = 30.02 years, SD = 10.85 years); 5 were male, 36 were female, and 2 did not provide their sex.
The data from the initial pilot sample were analyzed for the extent to which the items measured attitudes towards PLHIV. A Rasch factor analysis was conducted to assess if the MHP-PLHIV-AS had an appropriate level of unidimensionality. The diagnostics suggested that the instrument might consist of two dimensions because seven items (1, 2, 4, 10, 12, 20, & 24) out of the 25-total had negative point-biserial correlations, yet the overall dimensionality was over 75%. Typically, negative point-biserial correlated items of a pilot phase are not removed in cases such as this pilot when the data support the original construct theory (Bond & Fox, Citation2015; Linacre, Citation2016). Thus, more data exploration was called for to further explore and investigate the structure of the MHP-PLHIV-AS.
Phase III: validation
The same IRB process, adult informed consent, study procedures, and ethical research participation standards were utilized for Phase III. Degreed and licensed MHPs from across the United States were recruited for the validation phase and students qualified as well, but were different participants than those in the pilot study. The Phase III sampling occurred in three fashions. First, master- and doctoral-level mental health students were recruited through their instructors. Instructors sent a recruitment email to their classes to invite students to participate. The recruitment email was clear that participation was voluntary. Second, professional mental health organizations were asked for publicly-available, non-private contact information (e.g., name and email addresses) for helping professionals who qualified for participation. Finally, snowball sampling was encouraged by requesting those who were contacted for participation share with their similarly-licensed or certified colleagues, as well as mental health graduate-level students who qualified for participation. As with the pilot phase, participants were provided informed consent, the opportunity to ask questions, agreed to participate, and knew they could withdraw at any time. Four-hundred and sixty-six MHPs responded to the participation request. However, 12 were removed from the sample because they were not mental health professionals. provides the sample’s (n = 454) descriptive statistics. provides the sample’s primary credential identification.
Table 1. Validation study – summary of demographic characteristics (n = 454).
Table 2. Validation study – summary credentials (n = 454).
Results
Validation phase – step one
The MHP-PLHIV-AS’ descriptive statistics are provided in . Data were analyzed in three steps to test various configurations of the attitude towards PLHIV construct. A summary of these steps, the corresponding data analyses, and resulting interpretations are provided in . As was found with the pilot phase data, items 1, 2, 4, 10, 12, 20, and 24 (5 items represented affirming and two items represented indifference) did not behave statistically the same as the rest of the items. That is, these seven items had negative point-biserial correlations and the eigenvalue was high (5.66), suggesting more than one dimension. Yet, dimensionality was at 73%, a level supportive of the conclusion that all items on the instrument were measuring the same variable.
Table 3. Validation study – MHP-PLHIV-AS descriptive statistics (n = 454).
Table 4. Validation phase – data analyses process.
Validation phase – step two
In step two, the instrument was hypothesized and analyzed as two dimensions. Based on their negative point-biserial correlations, items 1, 2, 4, 10, 12, 20, and 24 were analyzed as “dimension 1”. The remaining 18 items were analyzed together as “dimension 2”. Dimension 1 had a lower than desired dimensionality (42.5%), and an unexplained contrast of 12.90%, but an eigenvalue of 1.5 in the first contrast. Dimension 2 had acceptable dimensionality at 51.80%, a first unexplained contrast of 5.20%, and an eigenvalue of 1.9. When dimension 1 (seven items) and dimension 2 (18 items) were analyzed separately, all but one item’s (Item 14; IMP1) point-biserial correlations were positive. The IMP1 item (#14), when grouped with dimension 2, had a negative point-biserial correlation (-.02), denoting it was not appropriate as part of dimension 2. Item 14 was then re-grouped to examine if it fit with dimension 1.
Validation phase – step three
The third step included two adjustments to the two dimensions. First, the impartial item (14), “It does not matter one way or another if someone is a PLHIV”, was moved from dimension 2 to test whether this item fit better with dimension 1. Additionally, the items on the second dimension were reverse coded so that a higher score would represent a more favorable attitude. These 17 items’ preferred answer of a more favorable attitude would mean an answer of “Strongly Disagree”. The result of that response, however, would be a score of “1” for those items. These items needed to be recoded such that their more favorable response would equate to a score of “4”, not a score of “1”. These adjustments resulted in eight items (1, 2, 4, 10, 12, 14, 20, & 24) for dimension 1, representing more favorable attitudes towards PLHIV. Dimension 2 (the remaining 17 items) representing less favorable attitudes with reverse coding. The grouping by dimensions, expected responses, and point-biserial correlations are presented in . When considered as these two dimensions, all items on the MHP-PLHIV-AS produced positive point-biserial correlations. Further, each dimension had acceptable levels of dimensionality, with 48.9% for dimension 1 and 54.1% for dimension 2. These results strengthened the conclusion that attitudes toward PLHIV consists of two distinct dimensions.
Table 5. Validation phase – two dimensions with “impartial” item moved to dimension 1 and dimension 1 items re-coded.
When interpreting the meaning of each dimension, a different pattern than the original linear approach the CEP had intended became clear. Dimension 1’s items reflected societal, collective, and advocacy and social justice elements surrounding PLHIV. The items in dimension 2 all focused on closer proximity and interpersonal attitude towards PLHIV. Consequently, dimension 1 was renamed as the “societal dimension” and dimension 2 renamed to the “personal dimension”, and analyses were considered from this perspective. represents the Rasch analysis results for the items grouped by societal and personal dimensions.
Table 6. Validation phase – point-biserial correlations, societal and personal dimensions.
The items within the societal dimension all had positive point-biserial correlations and accounted for 48.90% of the variance, slightly below the desired 50% cut-off. It had a first unexplained contrast of 10.70%, which is .70% above the desired cut-off, but the eigenvalue was at 1.67. This evidence supported the unidimensionality of the societal dimension, even if not completely meeting the study’s desired cut-offs. The personal dimension’s items also all had positive point-biserial correlations. The dimensionality accounted for 54.1% of the variance, and the first unexplained contrast accounted for 4.60%, with an eigenvalue of 1.7. This evidence supported an acceptable level of unidimensionality for the personal dimension.
Finally, probability graphs were reviewed to determine the utility of the 4-point rating scale in measuring attitudes. The rating scale probability graphs demonstrated that respondents used all four rating category options as distinct and meaningful from one another, evidenced by a minimum of 50% probability for each category (for each dimension) and appropriate threshold distances between each category (Linacre, Citation2002, Citation2006). Such evidence suggests that participants utilized the full, four-option rating scale categories.
The question of whether items measure attitude via a single or multiple dimension was answered. Rasch diagnostics supported the conclusion that the MHP-PLHIV-AS measures both a societal dimension and a personal dimension of attitudes towards PLHIV. It was also answered that the items demonstrated a range of attitude. They did not correspond to the original construct theory of attitudes ranging from affirming to violent; rather, they ranged from relative to proximal distance to the individual. Further, the respondents answering the MHP-PLHIV-AS reliably distinguished among the four rating scale options for each item. In its current state the MHP-PLHIV-AS has sufficient psychometric evidence to measure of MHPs’ attitudes towards PLHIV. In order to understand an individual’s attitude towards PLHIV, two separate scores (societal and a personal scores), should be calculated. When considered separately, the two scores provide a profile of the individual’s attitude at both the personal and societal dimensions.
Discussion
Over a million persons are infected with HIV in the United States alone (CDC, Citation2020). People living with HIV/AIDS have unique mental health needs. Heretofore, MHPs lacked an instrument with which to measure attitudes toward PLHIV, a key element in competency. This study represents the first known effort to measure MHPs’ attitudes towards people living with HIV/AIDS. The study’s results indicate that the MHP-PLHIV-AS is a unitary measure of attitude towards PLHIV through two dimensions: societal and personal. This is evidence that not only can societal and personal attitudes be measured with the one instrument but, in fact, both must be measured in order to gain a meaningful assessment of MHPs’ attitude towards PLHIV. Conclusions drawn from the data (i.e., validity) should come from looking at the unidimensionality, and the dual-dimensional nature of the overall construct. The analysis suggests that attitude towards PLHIV can be different depending on the proximity to the individual. That is, attitude is relational and valid conclusions can be drawn when considering the dual-dimensional nature of the construct. To evaluate an individual’s score, therefore, would require evaluating the societal level score and the personal level score to determine a “level of attitude”.
The societal dimension includes elements such as social justice, government funding for research, and broader-stroke views of PLHIV, that are further in physical distance from the individual. Examples include “PLHIV are discriminated against” (Item 4), and “It is appropriate to spend money on HIV/AIDS (i.e., research, care, treatment)” (Item 24). The personal items are proximally closer to the individual and things specific to MHPs interactions with PLHV. “I should be allowed to choose if I provide mental health services to clients who are HIV-positive” (Item 15) is an example.
MHP educators and supervisors can use this instrument to identify gaps in students’ and supervisees’ training. Rose et al. (Citation2015) found that few professional counselors receive HIV/AIDS education in their university training, and even less engage continuing education opportunities once they are credentialed and work in the field. This leaves MHPs lacking in discussions relating to HIV/AIDS. When attitude is influenced by knowledge (Carney et al., Citation1994; Rose et al., Citation2015), education is key to improving attitudes towards HIV/AIDS.
As an example of one way to utilize the scoring of the MHP-PLHIV-AS, consider Counselor Smith who works in a community mental health agency. Counselor Smith’s MHP-PLHIV-AS responses produced a Level 2 score on the personal domain and a Level 5 score on the societal domain. This suggests that Counselor Smith has favorable attitudes (i.e., high societal domain) on PLHIV issues such as needing unique services, advocacy and social justice, and perhaps even financial aid for medications. Counselor Smith is not, however, particularly comfortable being in close proximity of PLHIV (i.e., low personal domain) which can negatively impact their direct work with PLHIV. This could help Counselor Smith’s supervisor know that some additional training on HIV transmission may be warranted to help Counselor Smith recognize they are not at risk of infection from a client within the confines of the therapeutic relationship. A reverse example, where Counselor Smith scored high on the personal domain but low on the societal domain, would indicate that they are very comfortable being around PLHIV, but hold less favorable attitudes regarding advocacy and social justice for PLHIV. In this situation, Counselor Smith would benefit from better awareness and knowledge surrounding the unique intersectionality issues experienced by PLHIV as a direct result of the disease. In either case, Counselor Smith may be viewed as “Empathic” in attitude. The original levels the CEP intended are still possible; it just requires the use of two scores to draw the conclusion of an overall attitude level, consequent label, and what that means for the individual both collectively and within the respective dimensions. This could, and in fact should, be done with the MHP-PLHIV-AS so it can be utilized effectively in real-world application in determining MHPs’ attitude towards PLHIV.
Limitations
There is opportunity for improving the dimensionality of the two dimensions. Item 7, “All humans, including PLHIV, deserve love, respect, and happiness”, is an outlier for the societal dimension (outfit mean-square is .55, below the .75 cut off). This suggests that MHPs consider other factors when looking at this item than just PLHIV. It could mean, for example, that MHPs have too many elements (e.g., love, respect, and happiness) to consider within a single item.
The societal dimension had figures close to the cut-off marks for the study, meaning that the dimension is measuring the construct properly, yet it could be strengthened. Options to increase power to the unidimensional nature of the dimension include modifying the aforementioned AFF2 item (#7). Adding items within this dimension is another to increase utility in the overall dimension. Improvement recommendations for the personal dimension include considering five items (5, 6, 8, 9, and 13) whose mean-squares were outside the preferred level be reworded to achieve enhanced fit. Item 9 (DIS2), for example, in its reverse-coded meaning state says, “Everyone is at risk of HIV infection”. Perhaps the item confuses respondents, such as some knowing that only individuals exposed to infected bodily fluids are at risk. In short, while there is opportunity to improve the MHP-PLHIV-AS further, it already provides an accurate measure of MHPs attitude towards PLHIV. Research looking at enhancements to the instrument are already being undertaken.
Acknowledgements
The authors would like to thank the members of the Content Evaluation Panel. The instrument’s creation would not have been possible without their devotion to PLHIV, expertise, and support throughout the study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
- Arredondo, P., Toporek, M. S., Brown, S., Jones, J., Locke, D. C., Sanchez, J., & Stadler, H. (1996). Operationalization of the multicultural counseling competencies. Association for Multicultural Counseling and Development. https://doi.org/fzn9v3
- Bidell, M. P. (2005). The sexual orientation counselor competency scale: Assessing attitudes, skills, and knowledge of counselors working with lesbian, gay, and bisexual clients. Counselor Education and Supervision, 44(4), 267–279. doi: 10.1002/j.1556-6978.2005.tb01755.x
- Bond, T. G., & Fox, C. M. (2015). Applying the Rasch model: Fundamental measurement in the human sciences (3rd ed.). Routledge. https://doi.org/d6rq
- Carney, J., Werth, J. L., & Emanuelson, G. (1994). The relationship between attitudes toward persons who are gay and persons with AIDS, and HIV and AIDS knowledge. Journal of Counseling & Development, 72(6), 646–650. doi: 10.1002/j.1556-6676.1994.tb01696.x
- Centers for Disease Control and Prevention (CDC). (2020, June). HIV in the United States and dependent areas: At a glance. https://www.cdc.gov/hiv/statistics/overview/ataglance.html
- Enos, M. (2008). Steps leading to a straight line: Constructing a variable. Rasch Measurement Transactions, 22(1), https://www.rasch.org/rmt/rmt221f.htm
- Froman, R. D., & Owen, S. V. (1998). Further validation of the AIDS attitude scale. Research in Nursing and Health, 20(2), 161–167. doi:10.1002/(SICI)1098-240X(199704)20:2<161::AID-NUR8>3.0.CO;2-I
- Froman, R. D., & Owen, S. V. (2001). Measuring attitudes toward persons with AIDS: The AAS-G as an alternate form of the AAS. Scholarly Inquiry for Nursing Practice, 15(2), 161–177. https://pubmed.ncbi.nlm.nih.gov/11695492/
- Froman, R. D., Owen, S. V., & Daisy, C. (1992). Development of a measure of attitudes toward persons with AIDS. Journal of Nursing Scholarship, 24(2), 149–152. doi: 10.1111/j.1547-5069.1992.tb00240.x
- Gawronski, B. (2007). Editorial: Attitudes can be measured! But what is an attitude? Social Cognition, 25(5), 573–581. doi: 10.1521/soco.2007.25.5.573
- Lawshe, C. H. (1975). A quantitative approach to content validity. Personnel Psychology, 28(4), 563–575. doi: 10.1111/j.1744-6570.1975.tb01393.x
- Linacre, J. M. (2002). Optimizing rating scale category effectiveness. Journal of Applied Measurement, 3(1), 85–106. https://pubmed.ncbi.nlm.nih.gov/11997586/
- Linacre, J. M. (2005). Dimensionality investigation – an example. WINSTEPS Rasch Analysis and Rasch Measurement Software. https://www.winsteps.com/winman/multidimensionality.htm
- Linacre, J. M. (2006). Table 2.2 mean observed categories (average or expected categories: Rash-half-point threshholds). WINSTEPS Rasch Analysis and Rasch Measurement Software. https://www.winsteps.com/winman/table2_2.htm
- Linacre, J. M. (2011). Old Rasch forum: Rasch on the run – 2011. Rasch Forum. https://www.rasch.org/forum2011.htm
- Linacre, J. M. (2016). A user’s guide to WINSTEPS MINISTEP Rash-model computer programs (program manual 3.92.0). WINSTEPS Rasch Analysis and Rasch Measurement. https://www.winsteps.com
- O’Hara, C., Dispenza, F., Brack, G., & Blood, R. A. C. (2013). The preparedness of counselors-in-training to work with transgender clients: A mixed methods investigation. Journal of LGBT Issues in Counseling, 7(3), 236–256. doi: 10.1080/15538605.2013.812929
- Petty, R. E., Briñol, P., & DeMarree, K. G. (2007). The meta-cognitive model (MCM) of attitudes: Implications for attitude measurement, change, and strength. Social Cognition, 25(5), 573–581. doi: 10.1521/soco.2007.25.5.657
- Rasch, G. (1960). On general laws and the meaning of measurement in psychology. In J. Neyman (Ed.), Proceedings of the fourth Berkeley symposium on mathematical statistics and probability (Vol. 4) (pp. 321–333). Contributions to Biology and Problems of Medicine. https://projecteuclid.org/euclid.bsmsp/1200512872#info
- Rasch, G. (1980). Probabilistic models for some intelligence and attainment tests. University of Chicago Press.
- Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies (MSJCC). https://www.counseling.org/docs/default-source/competencies/multicultural-and-social-justice-counseling-competencies.pdf?sfvrsn=20
- Rose, J. S., Osborne, L., Hairston, T., Laux, J. M., & Pawelczak, M. (2015). HIV/AIDS knowledge among professional counselors and counseling students in Ohio. Journal of LGBT Issues in Counseling, 9(1), 2–16. doi: 10.1080/15538605.2014.997333
- Shrum, J. C., Turner, N. H., & Bruce, K. E. (1989). Development of an instrument to measure attitudes toward acquired immune deficiency syndrome. AIDS Education and Prevention, 1(3), 222–230. https://pubmed.ncbi.nlm.nih.gov/2641242/
- U. S. Department of Defense (DoD). (2016). Department of defense (DoD) releases fiscal year 2017 president’s budget proposal. https://www.defense.gov/News/News-Releases/News-Release-View/Article/652687/department-of-defense-dod-releases-fiscal-year-2017-presidents-budget-proposal/
- U. S. Department of Health and Human Services (HHS). (2008). Addiction counseling competencies: The knowledge, skills, and attitudes of professional practice (technical assistance publication [TAP] series 21). https://store.samhsa.gov/sites/default/files/d7/priv/sma12-4171.pdf
- Wilson, R. F., Pan, W., & Schumsky, D. A. (2012). Recalculation of the critical values for Lawshe’s content validity ratio. Measurement and Evaluation in Counseling and Development, 45(3), 197–210. doi: 10.1177/0748175612440286
- Wolfe, E. W., & Smith, E. V. (2007). Instrument development tools and activities for measure validation using Rasch models: Part I – instrument development tools. Journal of Applied Measurement, 8(1), 97–123 . https://pubmed.ncbi.nlm.nih.gov/17215568/