
ABSTRACT
There are limited data characterizing HIV retesting among high-risk adults in sub-Saharan Africa. From October-December 2018, we distributed recruitment cards offering health evaluations with HIV testing at venues frequented by individuals at-risk of HIV infection in Southwest Uganda. Those who attended were asked about their HIV testing history and risk factors: having >1 sexual partner, an HIV+ partner, STIs, and/or transactional sex. We defined “highest risk” as ≥3 risk factors and “frequent testing” as ≥3 tests within the past year. Of 1,777 cards distributed, 1,482 (83%) adults came to clinic: median age was 26(IQR: 22-31), 598 (40%) were men, and 334 (23%) were HIV+. Of 1,148 HIV-negative adults, 338 (29%) were highest risk and 205 (18%) were frequent testers. Frequent testing was similar in women (19%) and men (16%, p = 0.22). Among women, those at highest risk were more likely to report any testing (90% vs. 81%, p = 0.01) and frequent testing (25% vs. 18%, p = 0.06) than those at lower risk. Among men, any testing and frequent testing were similar between risk levels. Among adults recruited from high-risk venues in peri-urban Uganda, HIV risk behaviors were commonly reported, yet frequent retesting remained low. Interventions to promote retesting are needed, particularly among men.
Introduction
As efforts to increase HIV testing coverage throughout sub-Saharan Africa continue, regular retesting among at-risk adults who have previously tested negative remains of critical importance (UNAIDS, Citation2017). Frequent retesting of HIV-uninfected individuals at high risk allows for early identification of new infections and for linkage to expanding HIV prevention service options. For people who seroconvert, prompt knowledge of one’s HIV status and early access to antiretroviral therapy (ART) has the dual benefits of optimizing clinical outcomes (Girometti et al., Citation2017; Pilcher et al., Citation2017; Rutstein et al., Citation2017) and preventing further spread of HIV. (Kroon et al., Citation2017; Powers et al., Citation2011; Rutstein et al., Citation2017) Therefore, the World Health Organization recommends a minimum of annual retesting for high-risk individuals with more frequent testing (every 3–6 months) endorsed based on an individual’s specific risks or within the context of an HIV prevention intervention, (World Health Organization, Citation2015, Citation2019) and the Ugandan Ministry of Health (MoH) recommends retesting of key populations every three months (Uganda Ministry of Health, Citation2018).
Despite the importance of retesting following a negative HIV test, there are limited data characterizing retesting behavior among high-risk adults in sub-Saharan Africa (SSA), particularly following changes in country-specific guidelines recommending universal ART. Prior studies evaluating HIV retesting have found positive associations between more frequent retesting and increasing availability of HIV services, including start of the national ART program in Tanzania (Cawley et al., Citation2013), and qualitative findings in a treatment as prevention trial in South Africa that revealed high acceptability of repeat testing overall, as well as an increased understanding of risk behavior after receiving frequent testing (Orne-Gliemann et al., Citation2016). Some studies have also found associations between testing frequency and individual characteristics, such as being female, younger age, and knowing someone living with HIV (Hakim et al., Citation2019; Regan et al., Citation2013).
As countries and programs achieve increasingly high levels of population coverage of one-time HIV testing, understanding characteristics of high-risk individuals who are not engaging in routine HIV testing will be critical for developing interventions to promote retesting for those most at risk of infection. Our study sought to characterize retesting behavior and determine if HIV retesting was associated with risk factors among high-risk adults living in Southwestern Uganda.
Methods
From October–December 2018, we recruited adults at increased risk of HIV infection from a peri-urban community in Ibanda District, Uganda, to screen for enrollment into a randomized controlled trial (RCT) evaluating effectiveness of financial incentives to promote HIV retesting (NCT: 02890459). Ibanda District, in Southwestern Uganda, has an estimated adult HIV prevalence of 5.1% (UNAIDS, Citation2018b). In this nested, cross-sectional study, we sought to describe screening uptake and HIV positivity among adults following venue-based recruitment, and to characterize prior HIV testing behavior, including how testing frequency varied by self-reported risk, among HIV-uninfected adults that participated in screening for the parent trial.
Study staff first engaged in community mobilization meetings with health officials, community representatives, and local business owners to identify venues frequented by adults considered at increased risk of HIV infection due to drinking, transactional sex, or high mobility, and to facilitate local support for community-based recruitment. Study staff then visited these venues to distribute recruitment cards that invited adults, in both English and the local language (Runyankole), to come to a local government-run clinic the following day for a free health evaluation, which included HIV testing and a one-time cash transport reimbursement of 10,000 Ugandan Shillings (∼U.S.$2.70 in 2018). Recruitment cards were distributed until enrollment into the parent RCT was complete. The majority of recruitment was done in the afternoon, with recruitment at bars and markets extended through 9:00pm. Individuals who were unable to come to the clinic the following day were informed that they could come at a later date but might experience a longer wait time if all appointment slots were full.
Adults who presented to the clinic with recruitment cards underwent rapid HIV antibody testing according to Uganda MoH guidelines (Uganda Ministry of Health, Citation2018), as well as screening for hypertension, diabetes, and malaria (if febrile). Adults who self-reported as HIV-positive were not offered rapid HIV testing but received the other health services, including linkage to care and ART for those not on ART, and were classified as known positives. Those who tested HIV-positive during screening were provided same-day linkage to care and ART at their preferred clinic and were classified as newly diagnosed infections. Those who screened positive for hypertension, diabetes or malaria were also provided same-day linkage.
Following the health evaluation, all individuals completed a short screening questionnaire that asked about mobility, HIV testing history, and risk factors during the past 12 months, including having: >1 sexual partner, a sexual partner living with HIV, diagnosis or treatment of a sexually-transmitted infection (STI), and participation in transactional sex. Transactional sex was defined as either paying or receiving financial compensation or non-financial gifts in exchange for sex, although we did not distinguish between commercial sex work and other forms of transactional sex (Stoebenau et al., Citation2016; UNAIDS, Citation2018). We defined “highest risk” as having at least three of the four risk factors and “lower risk” as having fewer than three risk factors within the past year. We defined “frequent testing” as having at least three prior HIV tests within the past year.
All individuals who presented for the health evaluation were included in this nested cross-sectional analysis, while only those who tested HIV-negative were enrolled into the parent RCT study. We used chi-squared tests with a significance cut-off of p<0.05 to compare differences in testing history and risk factors between men and women, and logistic regression, stratified by sex and adjusting for age, to explore the association between testing history and the binary indicator of “highest risk” among individuals who tested HIV-negative at screening. Descriptive statistics of medians and interquartile ranges (IQR) were used for baseline characteristics.
The Makerere University School of Medicine Research and Ethics Committee (Uganda), the Uganda National Council for Science and Technology, and the University of California San Francisco (UCSF) Committee on Human Research (USA) approved the study protocol. The UCSF Committee on Human Research served as the institutional review board of record for investigators from the University of Pennsylvania (USA).
Results
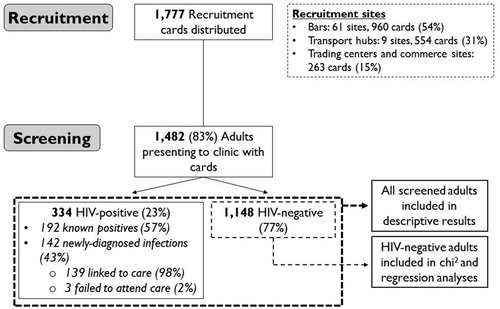
From October-December 2018, study staff distributed 1777 recruitment cards at community venues in Ibanda District, Uganda (). Of the 1777 cards, 960 (54%) were distributed among 61 bars; 554 (31%) were distributed among nine transport hubs (i.e., Truck stops and motorcycle taxi stages); and 263 (15%) were distributed at trading centers and other locations such as hotels, restaurants, food vendors and hair salons. From all cards distributed, 1,482 (83%) adults presented at the local government-run clinic for the free health evaluation. All adults presenting to clinic arrived within a week of their recruitment date, with most arriving the day after their recruitment. The majority of women presenting with cards had been recruited from bars (677/884; 77%), while most men were recruited from transport hubs (491/598; 82%). Median age was 26 years (IQR: 22–31), 598 (40%) were men, 125 (8%) were planning to move within the next six months, and 334 (23%) were HIV-positive: a prevalence four times higher than the general population (UNAIDS, Citation2018b). HIV positivity was higher among women than men (33% vs. 7%, p<0.001). Of 334 adults living with HIV, 192 (57%) were known positives by self-report and 142 (43%) were considered newly-diagnosed infections. Of the 142 individuals with newly-diagnosed infections, 139 (98%) were successfully linked to care and 3 (2%) failed to attend clinic despite repeated phone calls. Of adults with newly-diagnosed infections who completed the survey, 69/139 (50%) reported ≥1 HIV test in the previous year. The proportion of adults living with HIV who reported ≥1 risk factor in the past year was similar for both known and newly-diagnosed infections (86% vs 84%).
Figure 1. Venue-based recruitment of HIV-negative adults screened for a randomized-controlled trial of incentives strategies to promote HIV retesting in Uganda.
Of 1148 HIV-negative adults, median age was 25 years (IQR: 21–30), 554 (48%) were men, and median age was higher for men than women (27 vs. 23; p<0.001) (). Among HIV-negative adults, 892 (78%) reported having ≥1 HIV test in the past year, 205 (18%) were frequent testers, and 1,124 (98%) reported a willingness to return for retesting within the next six months. Women were more likely than men to have tested in the past year (82% vs. 73%, p<0.001), yet frequent testing was similar by sex (19% women vs. 16% men, p = 0.22).
Table 1. HIV risk factors and retesting frequency, stratified by sex, among HIV-negative adults recruited from high-risk community venues and screened for a randomized-controlled trial of incentive strategies to promote HIV retesting in Uganda.
Among HIV-negative adults, 721 (63%) reported ≥1 risk factor in the last year, and 338 (29%) were considered “highest risk”. Risk factors differed by sex, with more women reporting having sexual partners living with HIV and participating in transactional sex, and more men reporting having multiple sexual partners (). Though more men than women reported having any risk factor (66% vs. 60%, p = 0.05), a greater proportion of women were at highest risk (19% vs. 12%, p = 0.001).
Among HIV-negative women, a greater proportion of those at highest risk had an HIV test in the last year (90% vs. 81%, p = 0.01) and were frequent testers (25% vs. 18%, p = 0.06) than those at lower risk (). Women’s age-adjusted odds of any HIV testing in the last year doubled if they were at highest risk compared to lower risk (aOR: 2.04, CI: 1.16-4.36, p = 0.04). Women’s adjusted odds of frequent testing in the last year did not significantly differ between risk categories. Among HIV-negative men the proportion reporting any HIV testing in the last year was similar between those at highest and lower risk (74% vs. 72%, p = 0.75), as was frequent testing in the past year (11% vs. 17%, respectively, p = 0.17). Neither men’s adjusted odds of any HIV test nor adjusted odds of frequent testing significantly differed between risk categories.
Table 2. Association between self-reported level of HIV risk and frequency of testing for HIV-negative men and women screened for a randomized-controlled trial of incentives strategies to promote HIV retesting in Uganda.
Discussion
In this study of adults at increased risk of HIV acquisition in peri-urban Uganda, though the majority of adults reported having had an HIV test in the past year, frequent HIV retesting was uncommon. Despite the high HIV prevalence (23%) and high frequency of HIV risk behaviors reported, fewer than 20% of HIV-negative adults reported engaging in HIV retesting on a quarterly basis as recommended by the Ugandan MoH. Women reported increased testing frequency as their level of risk increased, but this pattern was not observed for men.
Failure to meet the recommended retesting frequency in high-risk populations may result in delayed diagnosis and treatment as well as missed opportunities to link to prevention services. Indeed, nearly half (42%) of adults living with HIV in our study reported being unaware of their HIV status. Individuals with undiagnosed recent infections, in particular, are more likely to transmit HIV (Powers et al., Citation2011; Rutstein et al., Citation2017). Therefore, frequent retesting with linkage to prevention, including voluntary male circumcision and PrEP, if HIV-uninfected and ART if HIV-infected, is a key part of efforts to interrupt transmission (Buchbinder & Liu, Citation2016). Although PrEP was not widely available through Ugandan government clinics at the time of this study, PrEP is now included in Uganda national guidelines (Uganda Ministry of Health, Citation2018) and availability has increased in recent years (PEPFAR Monitoring, Evaluation, and Reporting Database, Citationn.d.). However, PrEP implementation is still being scaled up and, despite progress, is not uniformly available at this time at clinical sites across Uganda (PrEP Watch: Uganda, Citationn.d.). Emphasis on frequent retesting may serve a critical role in expanding PrEP uptake in key populations. Given that nearly all (98%) of the HIV-negative adults in our study reported a willingness to retest in six months yet only 18% were frequent testers, our findings suggest interventions to promote retesting, including access to self-testing, are needed in such communities.
HIV retesting behaviors differed by sex, with women more likely to retest as their risk behavior increased whereas men’s retesting rates did not differ by risk level. These findings are consistent with previous studies (Hakim et al., Citation2019; Knight et al., Citation2014; Regan et al., Citation2013) and suggest that women may be more aware of how certain behaviors can increase HIV risk or may be more motivated to manage such increased risk by seeking retesting. Women in SSA tend to have more opportunities for HIV retesting through engagement in antenatal programs, which may also contribute to gender differences in HIV retesting (Camlin et al., Citation2016; Mak et al., Citation2016). Other studies in SSA have shown that many men believe that HIV sero-concordance between couples is likely (Ndyabakira et al., Citation2019) and often rely on their partner’s HIV results as a proxy test for their own status (Camlin et al., Citation2016; Mak et al., Citation2016; Musoke et al., Citation2018), and that norms of masculinity may create barriers to testing (Sileo et al., Citation2019) further supporting the finding that men’s HIV testing patterns may not be driven by their risk behaviors. High-risk men are thus in need of additional interventions to promote retesting, such as targeted incentives for testing and education on the association between behavior and HIV risk and the benefits of early diagnosis.
Another key finding of our study is that distributing recruitment cards in bars – known locations for transactional sex in this study community – and other venues visited by at-risk adults, and offering free, multi-disease health evaluations with a transportation reimbursement resulted in a high proportion of recruited adults who came to the local clinic for screening. Although mobile, community-based HIV testing approaches can also reach at-risk populations, (Herce et al., Citation2018; Sharma et al., Citation2015) our distribution of recruitment cards at venues selected with community input provides evidence for a simple, high-yield alternative means of reaching at-risk adults to promote HIV testing with same-day linkage to care and treatment. Such an approach could also be leveraged to screen for other diseases with shared risk factors, including STIs and TB, may be translatable to other settings, and merits further investigation.
This study has several limitations. First, our analyses were limited to adults who voluntarily attended the health evaluation; those who opted out may be of even higher risk, potentially resulting in a non-representative sample. However, of the 1776 recruitment cards distributed, 83% were returned. Second, while our definition of “frequent testing” was based on Uganda MoH retesting recommendations for key populations, there are no similar guidelines for categorizing risk. We chose to define “highest risk” as having more than half (≥3) of the four risk factors evaluated; secondary analyses using a cut-off of ≥2 risk factors showed similar results. Third, our study relied on self-reported HIV testing history and risk factors. Self-report may overestimate actual HIV testing, and differential reporting biases for men and women could account for some of the differences by sex. Finally, while our analyses were adjusted for age, we were unable to examine other potential confounding factors such as education and economic status due to limited demographic data in this screening dataset.
As one-time HIV testing coverage increases in sub-Saharan Africa, frequent retesting of individuals at high risk for HIV will become increasingly important to identify new infections early and start ART promptly, thereby reducing individual morbidity and onward transmission of HIV. Our data suggest a need for interventions to promote frequent retesting among high-risk adults.
Author contributors
GC, HT and DK designed the study with involvement from MK and DH. HT, AN, KM, DK, GC supervised the data collection. KM analyzed the data. KM and GC led interpretation of the results, with involvement from DK, AN, HT, CC, MK and DH. KM wrote the first draft. All authors reviewed the manuscript and approved the final draft.
Acknowledgements
We gratefully acknowledge our research staff, community advisory board members, and especially the communities and participants involved in this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Buchbinder, S. P., & Liu, A. Y. (2016). CROI 2016: Hot spots in HIV infection and advances in HIV prevention. Topics in Antiviral Medicine, 24(1), 10–28.
- Camlin, C. S., Ssemmondo, E., Chamie, G., El Ayadi, A. M., Kwarisiima, D., Sang, N., Kabami, J., Charlebois, E., Petersen, M., Clark, T. D., Bukusi, E. A., Cohen, C. R., Kamya, M. R., & Havlir, D., & SEARCH Collaboration. (2016). Men “missing” from population-based HIV testing: Insights from qualitative research. AIDS Care, 28 (Suppl 3), 67–73. https://doi.org/10.1080/09540121.2016.1164806
- Cawley, C., Wringe, A., Isingo, R., Mtenga, B., Clark, B., Marston, M., Todd, J., Urassa, M., & Zaba, B. (2013). Low rates of repeat HIV testing despite increased availability of antiretroviral therapy in rural Tanzania: Findings from 2003-2010. PloS One, 8(4), e62212. https://doi.org/10.1371/journal.pone.0062212
- Girometti, N., Nwokolo, N., McOwan, A., & Whitlock, G. (2017). Outcomes of acutely HIV-1-infected individuals following rapid antiretroviral therapy initiation. Antiviral Therapy, 22(1), 77–80. https://doi.org/10.3851/IMP3080
- Hakim, A. J., Mukasa, B., Hundley, L., Odiit, M., Ogwal, M., Sendagala, S., Karamagi, Y., Sande, E., & Hladik, W. (2019). Correlates of undiagnosed HIV infection and retesting among voluntary HIV testing Clients at Mildmay clinic, Uganda. AIDS and Behavior, 23(4), 820–834. https://doi.org/10.1007/s10461-018-2274-3
- Herce, M. E., Miller, W. M., Bula, A., Edwards, J. K., Sapalalo, P., Lancaster, K. E., Mofolo, I., Furtado, M. L. M., & Weir, S. S. (2018). Achieving the first 90 for key populations in sub-Saharan Africa through venue-based outreach: Challenges and opportunities for HIV prevention based on PLACE study findings from Malawi and Angola. Journal of the International AIDS Society, 21 (Suppl 5), e25132. https://doi.org/10.1002/jia2.25132
- Knight, L., McGrath, N., van Rooyen, H., Humphries, H., van Heerden, A., & Richter, L. (2014). Characteristics of sexually experienced HIV testers aged 18 to 32 in rural South Africa: Baseline results from a community-based trial, NIMH Project Accept (HPTN 043). BMC Public Health, 14(1), 1164. https://doi.org/10.1186/1471-2458-14-1164
- Kroon, E. D. M. B., Phanuphak, N., Shattock, A. J., Fletcher, J. L. K., Pinyakorn, S., Chomchey, N., Akapirat, S., de Souza, M. S., Robb, M. L., Kim, J. H., van Griensven, F., Ananworanich, J., & Wilson, D. P. (2017). Acute HIV infection detection and immediate treatment estimated to reduce transmission by 89% among men who have sex with men in Bangkok. Journal of the International AIDS Society, 20(1), 21708. https://doi.org/10.7448/IAS.20.1.21708
- Mak, J., Mayhew, S. H., von Maercker, A., Colombini, M., & Integra Research Team, I. R. T. (2016). Men’s use of sexual health and HIV services in Swaziland: A mixed methods study. Sexual Health, 13(3), 265–274. https://doi.org/10.1071/SH15244
- Musoke, P., Hatcher, A., Rogers, A. J., Achiro, L., Bukusi, E., Darbes, L., Kwena, Z., Oyaro, P., Weke, E., & Turan, J. M. (2018). Men’s hopes, fears and challenges in engagement in perinatal health and the prevention of mother-to-child transmission of HIV in rural Kenya. Culture, Health & Sexuality, 20(11), 1259–1272. https://doi.org/10.1080/13691058.2018.1426785
- Ndyabakira, A., Chamie, G., Emperador, D., Marson, K., Kamya, M. R., Havlir, D. V., Kwarisiima, D., & Thirumurthy, H. (2019). Men’s beliefs about the likelihood of Serodiscordance in couples with an HIV-positive partner: Survey evidence from Rural Uganda. AIDS and Behavior, https://doi.org/10.1007/s10461-019-02531-7
- Orne-Gliemann, J., Zuma, T., Chikovore, J., Gillespie, N., Grant, M., Iwuji, C., Larmarange, J., McGrath, N., Lert, F., & Imrie, J. & TasP Study Group (2016). Community perceptions of repeat HIV-testing: Experiences of the ANRS 12249 treatment as prevention trial in rural South Africa. AIDS Care, 28 (Suppl 3), 14–23. https://doi.org/10.1080/09540121.2016.1164805
- PEPFAR Monitoring, Evaluation, and Reporting Database. (n.d.). Retrieved September 25, 2020, from https://mer.amfar.org/location/Uganda/PrEP_NEW
- Pilcher, C. D., Ospina-Norvell, C., Dasgupta, A., Jones, D., Hartogensis, W., Torres, S., Calderon, F., Demicco, E., Geng, E., Gandhi, M., Havlir, D. V., & Hatano, H. (2017). The effect of same-day observed initiation of antiretroviral therapy on HIV viral load and treatment outcomes in a US Public Health Setting. JAIDS Journal of Acquired Immune Deficiency Syndromes, 74(1), 44–51. https://doi.org/10.1097/QAI.0000000000001134
- Powers, K. A., Ghani, A. C., Miller, W. C., Hoffman, I. F., Pettifor, A. E., Kamanga, G., Martinson, F. E., & Cohen, M. S. (2011). The role of acute and early HIV infection in the spread of HIV and implications for transmission prevention strategies in Lilongwe, Malawi: A modelling study. The Lancet, 378(9787), 256–268. https://doi.org/10.1016/S0140-6736(11)60842-8
- PrEP Watch: Uganda. (n.d.). PrEPWatch. Retrieved September 25, 2020, from https://www.prepwatch.org/country/uganda/
- Regan, S., Losina, E., Chetty, S., Giddy, J., Walensky, R. P., Ross, D., Holst, H., Katz, J. N., Freedberg, K. A., & Bassett, I. V. (2013). Factors associated with self-reported repeat HIV testing after a negative result in Durban, South Africa. PloS One, 8(4), e62362. https://doi.org/10.1371/journal.pone.0062362
- Rutstein, S. E., Ananworanich, J., Fidler, S., Johnson, C., Sanders, E. J., Sued, O., Saez-Cirion, A., Pilcher, C. D., Fraser, C., Cohen, M. S., Vitoria, M., Doherty, M., & Tucker, J. D. (2017). Clinical and public health implications of acute and early HIV detection and treatment: A scoping review. Journal of the International AIDS Society, 20(1), 21579. https://doi.org/10.7448/IAS.20.1.21579
- Sharma, M., Ying, R., Tarr, G., & Barnabas, R. (2015). Systematic review and meta-analysis of community and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature, 528(7580), S77–S85. https://doi.org/10.1038/nature16044
- Sileo, K. M., Fielding-Miller, R., Dworkin, S. L., & Fleming, P. J. (2019). A scoping review on the role of masculine norms in men’s engagement in the HIV care continuum in sub-Saharan Africa. AIDS Care, 31(11), 1435–1446. https://doi.org/10.1080/09540121.2019.1595509
- Stoebenau, K., Heise, L., Wamoyi, J., & Bobrova, N. (2016). Revisiting the understanding of “transactional sex” in sub-Saharan Africa: A review and synthesis of the literature. Social Science & Medicine, 168, 186–197. https://doi.org/10.1016/j.socscimed.2016.09.023
- Uganda Ministry of Health. (2018, September). Consolidated guidelines for the prevention and treatment of HIV and AIDS in Uganda. https://elearning.idi.co.ug/pluginfile.php/5675/mod_page/content/19/Uganda%20HIV%20%20Guidelines%20-%20September%202018.pdf
- UNAIDS. (2017, July 20). Ending AIDS: Progress towards the 90-90-90 targets. https://www.unaids.org/sites/default/files/media_asset/Global_AIDS_update_2017_en.pdf
- UNAIDS. (2018a). Transactional sex and HIV risk: From analysis to action. Geneva: Joint United Nations Programme on HIV/AIDS and STRIVE. https://www.unaids.org/en/resources/documents/2018/transactional-sex-and-hiv-risk
- UNAIDS. (2018b, September). Uganda HIV/AIDS country progress report July 2016-June2017. https://www.unaids.org/sites/default/files/country/documents/UGA_2018_countryreport.pdf
- World Health Organization. (2015). Consolidated guidelines on HIV testing services: 5Cs: consent, confidentiality, counselling, correct results, and connection. http://www.ncbi.nlm.nih.gov/books/NBK316021/
- World Health Organization. (2019, November 27). Consolidated guidelines on HIV testing services for a changing epidemic. https://www.who.int/publications-detail/consolidated-guidelines-on-hiv-testing-services-for-a-changing-epidemic
