
ABSTRACT
Current guidelines recommend starting antiretroviral therapy (ART) as soon as possible after HIV diagnosis to reduce morbidity, mortality and onward HIV transmission. We examined factors influencing ART initiation by women who seroconverted during the Evidence for Contraceptive Options and HIV Outcomes (ECHO) Trial. ECHO, conducted between 2015 and 2018, enrolled HIV-negative, sexually active women, aged 16–35 years, from four African countries. Follow-up was 12–18 months, with quarterly HIV testing. Women with incident HIV infection received extensive counselling by trial staff and referral to local facilities for HIV care. Of 304 women with ≥90 days follow-up time since HIV diagnosis, 186(61.2%) initiated ART within 90 days, 69(22.7%) initiated after 90 days, and 49(16.1%) had not initiated by the end of the study. There were no statistically significant differences in characteristics among women who initiated ART ≤90 days versus those who did not. Frequent reasons for delayed or non-initiation of ART included not feeling ready to start ART and being newly diagnosed. In a large clinical trial, ART initiation was modest within 90 days of HIV diagnosis and grew to 84% with longer observation. Despite extensive counselling on the importance of early ART initiation, personal barriers delayed some women from starting ART.
Introduction
In 2015, the World Health Organization (WHO) recommended that antiretroviral therapy (ART) be initiated by everyone living with HIV as soon as possible due to the impact of sustained ART on reduced mortality, morbidity, and sexual transmission to HIV-negative partners (Cohen et al., Citation2016; INSIGHT START Study Group et al., Citation2015; WHO, Citation2015). Despite these global recommendations and related national guidelines (Ministy of Health, National AIDS & STI Control Programme [NASCOP], Citation2016; Republic of Zambia, Ministry of Health, Citation2016; South African National Department of Health, Citation2019; The Government of the Kingdown of Eswatini, Citation2018), individuals sometimes delay or choose to not initiate ART (Ahmed et al., Citation2018; Larsen et al., Citation2019; Lee et al., Citation2019; Maughan-Brown et al., Citation2018; Pell et al., Citation2018; Plazy et al., Citation2015). Recent population-level surveys have found that 30% of South Africans and ∼12% of people living with HIV in Eswatini, Kenya, and Zambia who know their HIV diagnosis are not using ART (Human Sciences Research Council, Citation2018; Ministry of Health, Zambia, Citation2017; NASCOP, Citation2020; Swaziland Ministry of Health, Citation2017). In these and similar settings, factors influencing the decision to delay ART include feeling healthy, feeling unprepared to start lifelong ART, HIV stigma, a lack of social support, difficulties translating intentions into actions, costs incurred to access ART, concerns about confidentiality, low-quality health services, and incomplete understanding about the benefits of ART (Ahmed et al., Citation2018; Nhassengo et al., Citation2018; Sy et al., Citation2021). Provider-based factors, such as a lack of urgency to prescribe ART, particularly in people with higher CD4 counts, have also resulted in delayed or non-initiation of ART (Lee et al., Citation2019).
In this analysis among African women participating in a trial of contraceptives and HIV incidence (ECHO, the Evidence for Contraceptive Options and HIV Outcomes Trial) (ECHO Trial Consortium, Citation2019), we aimed to estimate the time to ART initiation and reasons that women did not initiate ART within 90 days. This study was conducted during the era of the WHO “Treat All” policy which was initiated in 2016, and implemented countrywide in the four countries of the study participants (WHO, Citation2017). Our study findings provide important data on reasons young African women participating in a clinical trial might delay ART initiation despite the provision of extensive counselling and support, and country policies that support rapid ART initiation.
Methods
Study population and procedures
The ECHO Trial was a randomised clinical trial, conducted between 2015 and 2018, that enrolled 7829 HIV-negative sexually active women aged 16–35 years from 12 sites in four African countries (Eswatini, Kenya, South Africa, and Zambia). Women were randomised to receive either intramuscularly injected depot medroxyprogesterone acetate (DMPA-IM), the copper intrauterine device (IUD) or levonorgestrel (LNG) implant. The primary study endpoint was HIV incidence. Women were followed quarterly for 12–18 months. The study population for this analysis comprised all women diagnosed with HIV during the ECHO Trial, who were ART naïve at the time of HIV diagnosis by the study.
HIV diagnosis
Two rapid HIV tests were conducted in parallel at every scheduled visit. If one or both rapid tests were positive, confirmatory testing was done using HIV ELISA and HIV RNA PCR tests. HIV infection was confirmed if the HIV ELISA was reactive and the HIV RNA PCR viral load was >400 copies/ml. If both criteria were not met, additional testing was done using Western blot, HIV DNA PCR, and/or additional HIV RNA PCR tests. All cases of possible seroconversion were adjudicated by an endpoints committee. Nucleic acid amplification testing for Chlamydia trachomatis and Neisseria gonorrhoeae and quantification of CD4 T cells were also conducted at visits with possible seroconversion. Women diagnosed with HIV remained in the study. CD4 T cell and HIV RNA testing were conducted quarterly by trial staff post seroconversion. Women with confirmed incident HIV infection received comprehensive counselling by study counsellors, nurses and clinicians, and referral to local HIV care providers for ongoing HIV care, including the initiation of ART. Linkage to care was ascertained via participant self-report.
Data collection
Through interviewer-administered questionnaires, demographic data were self-reported at baseline and sexual behaviour data were self-reported at baseline and quarterly. Reasons for not using ART were collected via participant self-report using closed-ended options with a category “other” that allowed for reasons which were not specified to be documented using open text. All data, including laboratory test results, were collected using paper-based case report forms and transmitted to the data centre via fax.
Statistical methods
Kaplan Meier curves were used to depict the time to ART initiation. Among women with ≥90 days follow-up after HIV diagnosis, associations of demographics at study enrolment (age, education, ever married, earning income, living with husband or partner), sexual behaviours and clinical characteristics at the HIV diagnosis visit, with initiation of ART ≤90 days of HIV diagnosis were estimated as relative risks using Poisson regression modified with robust error variance (Zou, Citation2004). Factors associated with ART initiation with a p-value <0.20 were included in a multivariable model.
Ethical statement
Research ethics committees for each of the study sites, the FHI360 Protection of Human Subjects Committee, and the WHO ethics committee approved the study. Participants completed written informed consent.
Results
Incident HIV infection
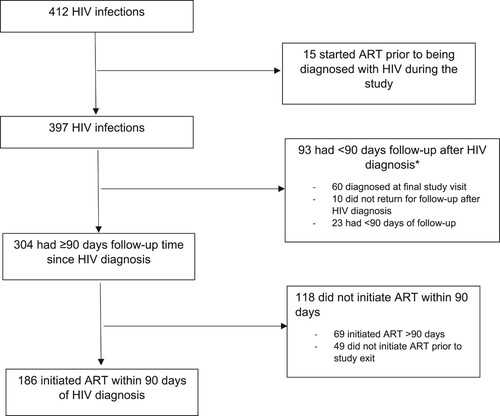
In total, 412 women (5.3% of the 7829 enrolled in the ECHO Trial) were diagnosed with HIV infection. Of these, 15 (3.6%) were determined retrospectively to have started ART prior to their study diagnosis and are excluded from analyses. Of the remaining 397 women, 304 (76.6%) contributed ≥90 days of follow-up time post-HIV diagnosis and are included in regression models ().
Figure 1. Participant flow: HIV diagnosis and commencement of antiretroviral therapy (ART).
Note: *23 women with <90 days follow-up reported initiating ART.
Participant characteristics
Of the 397 women who seroconverted and were not using ART at study diagnosis, approximately two-thirds (275, 69.3%) were aged 16–24 years, and most were unmarried (369, 92.9%) and not earning an income (323, 81.4%) (). The characteristics of women who had <90 days and ≥90 days of follow-up in the study subsequent to HIV diagnosis were similar.
Table 1. Participant characteristics by follow-up status.
ART initiation
Of the 93 women with <90 days follow-up time in the study subsequent to HIV diagnosis, 23 (24.7%) initiated ART prior to study exit. Among women with ≥90 days follow-up since HIV diagnosis (n=304), 186 (61.2%) initiated ART ≤90 days of HIV diagnosis, 69 (22.7%) initiated ART >90 days, and 49 women (16.1%) did not initiate ART by study exit (). Of note, the median time to ART initiation among women who initiated ART during the study was 39.5 days (IQR: 11-130), and >50% of women did not initiate ART within 30 days of HIV diagnosis (). Only four women (1.3%) had initiated ART on the day of HIV diagnosis. Demographics, sexual characteristics, and other factors were not significantly associated with initiating ART within 90 days (). The most frequent reasons women provided for not initiating ART at the first follow-up visit after HIV diagnosis were not being ready to start ART (15.3%) and being newly diagnosed (16.7%) (). Among all visits following HIV diagnosis, the most common reasons reported were not feeling ready to start ART (37.3%), having been newly diagnosed (21.3%), and feeling healthy (17.3%).
Figure 2. Days to antiretroviral therapy (ART) initiation using Kaplan-Meier methods.
Note: *Restricted to women with ≥90 days of follow-up in the trial subsequent to HIV diagnosis.
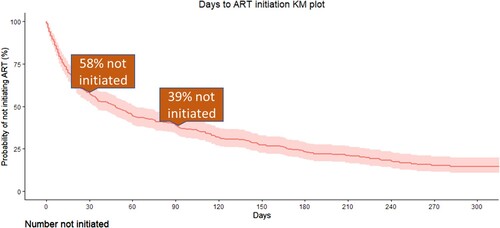
Table 2. Participant characteristics and association with antiretroviral therapy (ART) initiation within 90 days.
Table 3. Reasons women provided for not initiating antiretroviral therapy (ART) at follow-up visits after HIV diagnosis.
Discussion
Women who acquired HIV during the ECHO Trial received comprehensive counselling by trial staff, and referral to local health facilities for ongoing HIV care. With this level of support, 61% had initiated ART within 90 days of HIV diagnosis, and 84% by the end of study participation. Initiation was higher than a recent community-based cluster randomised trial where 47% of participants initiated ART within six months of referral (Sabapathy et al., Citation2017), and similar to a recent vaccine efficacy trial where 82% initiated ART by 24 weeks (Grey, Citation2020). Overall, despite the provision of extensive counselling and support in clinical trials, there remains a gap in early ART initiation among trial participants, and a need for increased efforts to promote earlier initiation of ART.
Frequent reasons for not initiating ART in our cohort were not feeling ready to start ART, being newly diagnosed, and feeling healthy, which may signal personal barriers related to acceptance of HIV status and need for lifelong medication. In a systematic review of qualitative studies from low-and-middle income countries, “feeling healthy” was a key factor in the decision to defer ART (Ahmed et al., Citation2018), however other trials have documented structural barriers such as busy or crowded clinics, and inconvenient clinic hours to be major barriers to initiating ART (Pry et al., Citation2020; Sabapathy et al., Citation2017).
Our study has some limitations. We did not collect detailed data on the referral process, such as the proximity of referral sites to research sites and provider-related factors, which could impact timing to ART initiation. Also, the timing and extent to which the “Treat All” policy was implemented between and within the participating countries might not have been uniform. Additional in-depth information on reasons for delayed or non-initiation of ART would have been useful to better understand barriers to early ART initiation.
While ART use among all individuals diagnosed with HIV offers several benefits, the rapidity of initiation needs to be balanced against the readiness of individuals to start ART, and take into account reasons individuals might not want to initiate ART, to avoid later gaps in ART use and dropout from HIV care. It is notable that even in a clinical trial setting where women receive comprehensive individualised supportive care from trained trial staff, ART was often not initiated immediately or even within a few months. To combat this, clinicians and other healthcare providers providing ART, can normalise the practice of immediate ART initiation and provide detailed information to allow individuals to make informed decisions about when to start ART, while balancing the importance of respecting the individuals rights and choices, and patient autonomy.
Acknowledgments
We thank the women that participated in the ECHO Trial for their dedication and commitment to the trial. We are also grateful to the trial staff including the counsellors, nurses and clinicians for the clinical care provided to women in the trial.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Access to data from the ECHO Trial may be requested through submission of a research concept to [email protected]. The concept must include the research question, data requested, analytic methods, and steps taken to ensure ethical use of the data. Access will be granted if the concept is evaluated to have scientific merit and if sufficient data protections are in place. As of the time of publication, data access applications are in process with the governing institutional review boards of the ECHO Trial to make de-identified data publicly available.
Additional information
Funding
References
- Ahmed, S., Autrey, J., Katz, I. T., Fox, M. P., Rosen, S., Onoya, D., Bärnighausen, T., Mayer, K. H., & Bor, J. (2018). Why do people living with HIV not initiate treatment? A systematic review of qualitative evidence from low- and middle-income countries. Social Science & Medicine (1982), 213, 72–84. https://doi.org/10.1016/j.socscimed.2018.05.048
- Cohen, M. S., Chen, Y. Q., McCauley, M., Gamble, T., Hosseinipour, M. C., Kumarasamy, N., Hakim, J. G., Kumwenda, J., Grinsztejn, B., Pilotto, J. H., Godbole, S. V., Chariyalertsak, S., Santos, B. R., Mayer, K. H., Hoffman, I. F., Eshleman, S. H., Piwowar-Manning, E., Cottle, L., Zhang, X. C. … HPTN 052 Study Team. (2016). Antiretroviral therapy for the prevention of HIV-1 transmission. The New England Journal of Medicine, 375(9), 830–839. https://doi.org/10.1056/NEJMoa1600693
- Evidence for Contraceptive Options and HIV Outcomes (ECHO) Trial Consortium. (2019). HIV incidence among women using intramuscular depot medroxyprogesterone acetate, a copper intrauterine device, or a levonorgestrel implant for contraception: A randomised, multicentre, open-label trial. Lancet (London, England), 394(10195), 303–313. https://doi.org/10.1016/S0140-6736(19)31288-7
- The Government of the Kingdom of Eswatini. (2018). The National Multisectoral HIV and AIDS Strategic Framework (NSF) 2018–2023. https://hivpreventioncoalition.unaids.org/wp-content/uploads/2019/06/Eswatini_NSF-2018-2023_final.pdf
- Grey, G. E., & Presentation of HVTN702 Study Data. (2020). Proceedings of the Conference on retroviruses and opportunitistic infections (CROI), Virtual, 8-11 March 2020. http://www.croiwebcasts.org/console/player/44778?mediaType=audio&
- Human Sciences Research Council, South Africa. (2018). HIV Impact Assessment Summary: The Fifth South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017. http://www.hsrc.ac.za/uploads/pageContent/9237/SABSSMV_Impact_Assessment_Summary_ZA_ADS_cleared3.pdf
- Larsen, A., Cheyip, M., Tesfay, A., Vranken, P., Fomundam, H., Wutoh, A., & Aynalem, G. (2019). Timing and predictors of initiation on antiretroviral therapy among newly-diagnosed HIV-Infected persons in South Africa. AIDS and Behavior, 23(2), 375–385. https://doi.org/10.1007/s10461-018-2222-2
- Lee, M. J., Venturelli, S., McKenna, W., Teh, J., Negedu, O., Florman, K. E., Musbahi, E., Bailey, A. C., Mackie, N. E., Fox, J., & Fidler, S. (2019). Reasons for delayed antiretroviral therapy (ART) initiation in the era of early ART initiation guidelines: A retrospective service evaluation. International Journal of STD & AIDS, 30(4), 415–418. https://doi.org/10.1177/0956462418814985
- INSIGHT START Study Group, Lundgren, J. D., Babiker, A. G., Gordin, F., Emery, S., Grund, B., Sharma, S., Avihingsanon, A., Cooper, D. A., Fätkenheuer, G., Llibre, J. M., Molina, J. M., Munderi, P., Schechter, M., Wood, R., Klingman, K. L., Collins, S., Lane, H. C., Phillips, A. N., & Neaton, J. D. (2015). Initiation of antiretroviral therapy in early asymptomatic HIV infection. The New England Journal of Medicine, 373(9), 795–807. https://doi.org/10.1056/NEJMoa1506816
- Maughan-Brown, B., Smith, P., Kuo, C., Harrison, A., Lurie, M. N., Bekker, L. G., & Galárraga, O. (2018). Readiness for antiretroviral therapy: Implications for linking HIV-Infected individuals to care and treatment. AIDS and Behavior, 22(3), 691–700. https://doi.org/10.1007/s10461-017-1834-2
- Ministry of Health, National AIDS & STI Control Programme. (2016). Guidelines on use of antiretroviral drugs for treating and preventing HIV infection in Kenya, 2016 edition. NASCOP.
- Ministry of Health, Zambia. (2017). Zambia population-based HIV impact assessment (ZAMPHIA) 2016: First Report. Zambia, Ministry of Health. https://phia.icap.columbia.edu/wp-content/uploads/2017/11/FINAL-ZAMPHIA-First-Report_11.30.17_CK.pdf
- National AIDS and STI Control Programme (NASCOP). (2020). Preliminary KENPHIA 2018 Report. Nairobi: NASCOP; 2020. Nairobi: NASCOP. https://phia.icap.columbia.edu/wp-content/uploads/2020/04/KENPHIA-2018_Preliminary-Report_final-web.pdf
- Nhassengo, P., Cataldo, F., Magaço, A., Hoffman, R. M., Nerua, L., Saide, M., Cuco, R., Hoek, R., Mbofana, F., Couto, A., Gudo, E., Chicumbe, S., & Dovel, K. (2018). Barriers and facilitators to the uptake of test and treat in Mozambique: A qualitative study on patient and provider perceptions. PloS one, 13(12), e0205919. https://doi.org/10.1371/journal.pone.0205919
- Pell, C., Vernooij, E., Masilela, N., Simelane, N., Shabalala, F., & Reis, R. (2018). False starts in ‘test and start': A qualitative study of reasons for delayed antiretroviral therapy in Swaziland. International Health, 10(2), 78–83. https://doi.org/10.1093/inthealth/ihx065
- Plazy, M., Newell, M. L., Orne-Gliemann, J., Naidu, K., Dabis, F., & Dray-Spira, R. (2015). Barriers to antiretroviral treatment initiation in rural KwaZulu-Natal, South Africa. HIV Medicine, 16(9), 521–532. https://doi.org/10.1111/hiv.12253
- Pry, J., Chipungu, J., Smith, H. J., Bolton Moore, C., Mutale, J., Duran-Frigola, M., Savory, T., & Herce, M. E. (2020). Patient-reported reasons for declining same-day antiretroviral therapy initiation in routine HIV care settings in Lusaka, Zambia: Results from a mixed-effects regression analysis. Journal of the International AIDS Society, 23(7), e25560. https://doi.org/10.1002/jia2.25560
- Republic of Zambia, Ministry of Health. (2016). Zambia consolidated guidelines for treatment & prevention of HIV infection. http://www.differentiatedcare.org/Portals/0/adam/Content/fLl-2LVqM0izU06VDY6DqQ/File/Zambia_Consolidated_2016_Guidelines.pdf
- Sabapathy, K., Mubekapi-Musadaidzwa, C., Mulubwa, C., Schaap, A., Hoddinott, G., Stangl, A., Floyd, S., Ayles, H., Fidler, S., Hayes, R., & HPTN 071 (PopART) study team. (2017). Predictors of timely linkage-to-ART within universal test and treat in the HPTN 071 (PopART) trial in Zambia and South Africa: Findings from a nested case-control study. Journal of the International AIDS Society, 20(4), e25037. https://doi.org/10.1002/jia2.25037
- South African National Department of Health. (2019). 2019 ART clinical guidelines for the management of HIV in adults, pregnancy, adolescents, children, infants and neonates. https://www.knowledgehub.org.za/system/files/elibdownloads/2020-05/2019%20ART%20Guideline%2028042020%20pdf.pdf
- Swaziland Ministry of Health. (2017). Swaziland HIV incidence measurement survey 2: A population-based HIV impact assessment: SHIMS2 2016–2017. http://phia.icap.columbia.edu/wp-content/uploads/2017/11/Swaziland_new.v8.pdf
- Sy, K., Tariq, S., Ramjee, G., Blanchard, K., Leu, C. S., Kelvin, E. A., Exner, T. M., Gandhi, A. D., Lince-Deroche, N., Mantell, J. E., O'Sullivan, L. F., & Hoffman, S. (2021). Predictors of antiretroviral therapy initiation in eThekwini (Durban), South Africa: Findings from a prospective cohort study. PloS one, 16(2), e0246744. https://doi.org/10.1371/journal.pone.0246744
- World Health Organization (WHO). (2015). Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. https://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/
- World Health Organization (WHO). (2017). Fact sheet: TREAT ALL: Policy adoption and implementation status in Countries. Retrieved November 9, 2020, from https://apps.who.int/iris/bitstream/handle/10665/258538/WHO-HIV-2017.35-eng.pdf?ua=1
- Zou, G. (2004). A modified poisson regression approach to prospective studies with binary data. American Journal of Epidemiology, 159(7), 702–706. https://doi.org/10.1093/aje/kwh090
