
ABSTRACT
Disclosure of human immunodeficiency virus (HIV) infection status improves treatment adherence and HIV prevention. Social networks influence such disclosure by people living with HIV/AIDS (PLWH). This study aimed to investigate the disclosure status of Korean PLWH and determine the social network characteristics associated with disclosure. A cross-sectional study design was used, and 148 Korean PLWH answered self-report questionnaires that included items on the characteristics of social networks and disclosure. Logistic regression and decision tree analysis were performed. In total, 81 participants (54.7%) reported disclosing HIV status to the most important supporter. Five factors were found to influence disclosure: age, self-help group participation, living arrangement, social network relationship, and tie strength; three groups had higher percentages of nondisclosure. The findings suggest that healthcare practitioners should provide adequate counseling by considering the characteristics of social networks and disclosure status of PLWH. Researchers should identify high-risk populations using decision tree analysis.
Introduction
Disclosure of human immunodeficiency virus (HIV) infection status refers to people living with HIV/AIDS (PLWH) informing others about their HIV-positive status voluntarily or involuntarily (Eustace & Ilagan, Citation2010). Disclosure is a complex process that involves making a decision, an act of disclosure, a mediating process in which social support is provided, and a long-term outcome (Chaudoir et al., Citation2011). Disclosure allows PLWH to receive social support from important others, which also affects treatment adherence and HIV prevention (Chaudoir et al., Citation2011). However, HIV disclosure can also lead to negative experiences, such as discrimination and social isolation, due to stigma (Hult et al., Citation2012). Thus, HIV disclosure needs to be approached carefully considering various factors.
Disclosure is reported to be mainly affected by demographic, psychological, and social network factors. The demographic factors include age, sex, race or ethnicity, residence, and socioeconomic status (Obermeyer et al., Citation2011). Psychological factors such as fear of stigmatization, discrimination, and rejection and feelings of shame or guilt, act as barriers to disclosure (Hult et al., Citation2012; Mayfield Arnold et al., Citation2008). Social network characteristics of PLWH also affect disclosure (Bairan et al., Citation2007), such as social relationship types and the strength of the person’s social ties with a supporter (Lugalla et al., Citation2012; Maman et al., Citation2014).
In Korea, as of 2019, there were 13,857 PLWH; additionally, 1,005 new HIV infections occur each year (Korea Centers for Disease Control & Prevention [KCDC], Citation2019). However, research on disclosure of HIV status is insufficient. Korea is expected to show different results than other countries because of its Asian cultural characteristics emphasizing avoidance of family conflict (Yoshioka & Schustack, Citation2001) and a reluctance toward discussing sexual minorities or sexually transmitted infections beyond marital relationships. Further, since there are generally few opportunities in Korea to meet PLWH, it is easy to receive negative information about HIV through indirect channels (e.g., television, the Internet) and form negative attitudes (Shim & Kim, Citation2020). As HIV disclosure is influenced by contextual environments, such as family, community, and sociocultural norms (Eustace & Ilagan, Citation2010), it is necessary to study the disclosure status and related social network characteristics of Korean PLWH to provide effective counseling and interventions.
Decision tree (DT) and logistic regression (LR) analyzes are methods for identifying the associated factors of the population for categorical dependent variables. Traditionally, LR is used to identify population risk factors, indicating the average of one independent variable for the entire population (Fernández et al., Citation2016). Contrastingly, DT can identify the interaction of several independent variables and identify risky subgroups, which is useful when classification or prediction is required in the healthcare field (Fernández et al., Citation2016; Lemon et al., Citation2003). Previous qualitative studies on social network characteristics that affect disclosure have reported that PLWH prefer disclosing their infection status to close and trusted family members or partners with whom they share strong ties (Lugalla et al., Citation2012; Maman et al., Citation2014). However, few studies analyzed those at risk for nondisclosure with DT among PLWH. To identify factors affecting disclosure by PLWH and characteristics of subgroups that prefer nondisclosure, both analytical methods are necessary to compare results.
This study aimed to (1) investigate disclosure status, (2) derive the subgroups at risk for nondisclosure through DT analysis, and (3) identify factors influencing nondisclosure of PLWH in Korea. The study’s findings could provide basic data that healthcare practitioners (HCPs) can use to support disclosure at facilities providing treatment and counseling for PLWH.
Methods
Participants
Participants were 148 PLWH (Mage: 36.25 ± 11.421 years) who received antiretroviral treatment through outpatient HIV care in Korea. Inclusion criteria were (1) aged at least 18 years and (2) no problems with communication or filling out the questionnaire. Using convenience sampling, a recruitment notice was posted in the counseling rooms of five hospitals’ infectious medicine outpatient departments.
Procedure
This study used data collected in a prior study (IRB No: 2015-0040). Additional IRB approval was obtained for conducting the secondary analysis (IRB No: Y-2017-0088). Data were collected between September 2016 to March 2017 from 179 respondents. Thirty-one participants whose responses to main variables (social network characteristics and disclosure status to the most important supporter) were missing were excluded; 148 were included in the final analysis. In the counseling room, prior to the survey, the research assistant (HIV counseling nurse) explained the study to participants and obtained their written consent. The time taken to complete the self-report paper-and-pencil questionnaire was 20–25 minutes; after the questionnaire was completed, participants were provided a $20 gift card as compensation for their time.
Variables
Demographic characteristics
Demographic characteristics included age, sex, education level, economic status, employment, self-help group participation, marital status, and living arrangements. To evaluate economic status, participants were asked to select one of three responses (low, middle, and high) to the question “What is your economic level?”
Social network characteristics and disclosure status
The scale for social network characteristics was constructed by the researchers with reference to previous studies investigating Korean adults and PLWH (Bogart et al., Citation2015; Jeong et al., Citation2012; Kim et al., Citation2008; Appendix 1 (see supplemental material)). Participants listed up to 24 people by their nickname or initials in response to “the person whom you think as the most important in your life (social supporter)” in order of importance. For each supporter, participants noted their HIV disclosure status, relationship, and contact frequency on 7-point Likert-type scales ranging from “rarely contacted” to “five or more times per week”, as well as the strength of their social tie on a 10-point Likert scale ranging from “very weak” to “very strong”. In this study, the social network characteristics and disclosure status of the most important supporter in participants’ social networks were used for the analysis.
Analysis
Data were analyzed using SPSS/WIN 23.0. To analyze differences in disclosure status according to demographic and social network characteristics, a Chi-squared test and a t-test were conducted. DT analysis evaluates risky subgroups based on classification and regression trees (CART). CART can be used for both categorical and continuous dependent variables (Song & Ying, Citation2015). Gini index and twoing criteria were used to select input variable, and child nodes were split binarily from parent nodes (Song & Ying, Citation2015). The minimum number of cases to be split was analyzed by specifying 10 as the parent node and 5 as the child node. The differences in characteristics of the subgroups at risk of nondisclosure to the most important supporter derived by DT were analyzed by one-way ANOVA and Fisher’s exact test. Finally, LR analysis was performed to analyze the factors that influenced disclosure.
Receiver operating characteristic (ROC) curves for the DT and LR analyzes were plotted to compare the efficacy of the two methods for assessing factors influencing HIV disclosure. ROC curve is a plot that displays the sensitivity and 1-specificity of a diagnostic test (Mandrekar, Citation2010). Area under the ROC curve (AUC) is considered an effective measure to summarize the diagnostic accuracy of the test; it ranges from 0 to 1. An AUC value of 0.5 indicates no discriminative value, 0.7–0.8 is considered acceptable, 0.8–0.9 is considered excellent, and a value of 1 reflects a perfect test (Fernández et al., Citation2016; Hosmer & Lemeshow, Citation2000; Mandrekar, Citation2010).
Results
Participants’ average social network size was 6.18 (±5.452; range: 1–24). Eighty-one participants (54.7%) reported disclosing their HIV infection status to their most important supporter. The disclosure rates to their second and third most important social supporters were 41.1% (58/141) and 46.3% (57/123), respectively. In the Chi-squared test and t-test, HIV infection status disclosure showed statistically significant differences depending on age, self-help group participation, marital status, living arrangements, relationship with the most important supporter, contact frequency, and tie strength ().
Table 1. Differences in disclosure of HIV infection status by People Living with HIV/AIDS (PLWH) to the most important supporter according to characteristics of participants (N = 148).
displays the DT analysis results. Nine groups were identified, of which three groups had higher percentages of not disclosing their HIV infection status than the root node. Based on the DT CART algorithm, six factors were used in group composition: living arrangements, age, employment, social network relationship, tie strength, and contact frequency. The characteristics of the three groups with high-risk of nondisclosure are shown in . The first group was Group III (in their 40s, unmarried and other marital status (divorced, separated, and widowed) (72.7%), living with family (90.9%), and relationship with the most important supporter was mother (63.6%) or others (children, relative, and mentor) (36.4%)); here, all individuals (100%; n = 11) did not disclose their HIV infection status to their most important supporter. The second group was Group VII (in their 20s, unmarried and other marital status (divorced, separated, and widowed) (92.3%), living with family (100%), and relationship with the most important supporter was mother (76.9%) or father (23.1%)); here, 69.2% of individuals reported nondisclosure (n = 13). The last group was Group I (in their 30s, unmarried or other marital status (divorced, separated, and widowed) (100%), and lived alone (100%)), and 67.9% of individuals did not disclose their HIV infection status (n = 53).
Figure 1. Decision tree to clarify the social relationship and network factors associated with disclosure of HIV infection status.
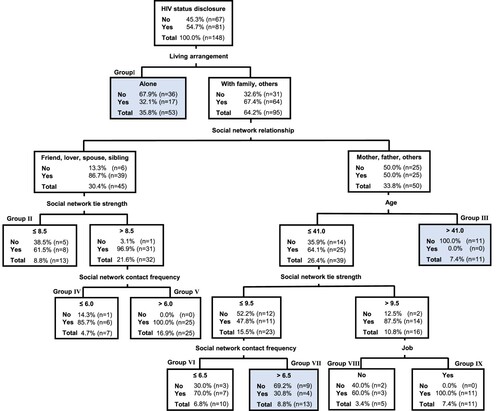
Table 2. Characteristics of participants in the high-risk nondisclosure groups (N = 77).
In the LR analysis, the probability of disclosure of HIV infection status to the most important supporter increased if the PLWH participated in a self-help group, were living with family or others, and selected their spouse or others, rather than mother, as the most important supporter (). The probability of nondisclosure increased with age. However, if the tie strength with the most important supporter increased, the probability of nondisclosure decreased. Therefore, living arrangements, age, social network relationship, and tie strength were factors related to disclosure derived from the two analysis methods.
Table 3. Factors associated with PLWH’s nondisclosure of HIV infection status to the most important supporter (N = 145).
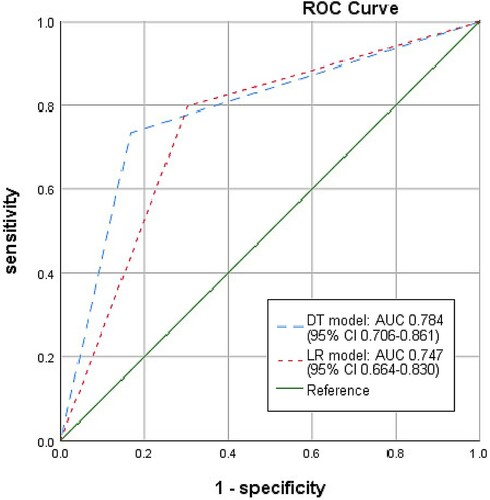
compares the AUC of the DT and LR analyzes based on ROC curves. For the DT and LR models, the AUC (95%CI) was 0.784 (0.706, 0.861) and 0.747 (0.664, 0.830), respectively.
Figure 2. Receiver operating characteristic curves for decision tree and logistic regression model.
Discussion
We found that 54.7% of the participants had disclosed their HIV infection status to their most important supporter. In a previous study, the percentages of “disclosure to anybody” by adult PLWH in the United States and Europe were 82% and 85–97%, respectively, and “disclosure to family” were 70–87% and 53–77%, respectively (Obermeyer et al., Citation2011). The general population of Korea has a stigmatizing attitude toward HIV infection (Lee et al., Citation2015); the low percentage of disclosure in this study may be due to stigma acting as a barrier. As disclosure is a complex process with various attributes (Eustace & Ilagan, Citation2010; Lugalla et al., Citation2012), it is necessary to consider sociocultural factors such as stigma and cultural values, along with demographic and social network characteristics when providing nursing interventions.
The high proportion of PLWH who disclosed their status to their partners may be attributable to sexual relationships being a path to HIV infection, making disclosure to a partner necessary to prevent transmission. Thus, couples counseling should be provided to PLWH with sexual partners, and the counseling needs of PLWH with partners can be assumed to be high. Female spouses of Korean PLWH were found to experience betrayal, anger, and fear when they initially learned of their husband’s HIV status; however, if they overcame these difficulties, they restored their relationship with their husbands and became a major social support (Seo & Jeong, Citation2017). Meanwhile, PLWH who disclosed their HIV status to their mother perceived help from their mother to be more important than did PLWH who did not disclose their status (Uphold et al., Citation2012). Korean national guidelines state that PLWH should notify their partners of their infection status for HIV testing (KCDC, Citation2019); however, specific service protocols for relationship or family counseling are insufficient. Therefore, it is necessary to develop intervention programs that consider the importance of social networks, such as spouses, partners, and mothers, that can be used as part of counseling services with PLWH.
LR and DT analysis indicated that living arrangements affected the group most likely not to disclose. PLWH who lived alone were more likely to not disclose than those who lived with family or others. In a previous study, PLWH disclosed HIV status for the first time to their closest or most trusted family members (Maman et al., Citation2014). Furthermore, in a context without the opportunity to interact with others, PLWH has been found to not disclose their status (Hult et al., Citation2012). Greene et al. (Citation2013) reported an intervention that provided disclosure strategies and enhanced skills to improve potential responses to disclosure, thereby increasing disclosure efficacy and reducing disclosure anxiety. Therefore, HCPs need to identify the difficulties of PLWH living alone, provide necessary interventions to support disclosure or improve social support, and introduce them to appropriate self-help groups.
In the LR results, as age increased, the probability of nondisclosure increased. Additionally, the DT analysis showed that in Group III, 100% of PLWH over 41 years old did not disclose. This was consistent with the findings of previous studies. Brown et al. (Citation2015) showed that men aged 50 and older who have sex with men were more likely to not disclose their infection status in sexual relationships than those aged 18–34 years, because of fear of isolation, internalized stigma, and discrimination. Further, Emlet (Citation2006) showed that a higher proportion of adults over 50 years old did not disclose to social networks including, family and friends, compared with young adults (20–39 years old). Thus, further research is needed to explore disclosure status, social networks, and related outcomes among older PLWH.
Tie strength with the most important supporter was also a factor associated with disclosure. Similar results were found in previous studies where disclosure was influenced by close and trusted social relationships (Lugalla et al., Citation2012; Maman et al., Citation2014). Specifically, Bairan et al. (Citation2007) reported that PLWH disclosed their infection status in long-term, non-casual, committed sexual relationships, or in nonsexual relationships with close family or friends. Through disclosure, PLWH expect to receive support or relief, and inform the social supporter of the possibility of transmission (Hult et al., Citation2012; Mayfield Arnold et al., Citation2008). Contrastingly, PLWH with weak social ties can find it difficult to expect a positive outcome through disclosure. In “The Brief Disclosure Intervention”, tie strength was considered by allowing participants to target two or three social network members from whom positive reactions were expected through disclosure (Greene et al., Citation2013). Therefore, interventions to support disclosure require careful consideration of the strength of ties with social networks.
The LR analysis showed that self-help group participation increased the likelihood of disclosure. Through self-help groups, PLWH disclosed their infection status to other PLWH, allowing them to establish their identity as PLWH and share their experiences with HIV (Nobre et al., Citation2016). In this study, 15% of the participants had participated in a self-help group, which was lower than results from Rwanda (52.5%) and Nigeria (24.6%; Elul et al., Citation2013; Ndu et al., Citation2011). Recently, studies have sought to improve the social support of PLWH through self-help groups using social media platforms or mobile applications (Flickinger et al., Citation2017; Ndu et al., Citation2011). Through these platforms, it is possible to exchange information, discuss HIV, establish a community (Taggart et al., Citation2015), and express support (Flickinger et al., Citation2017). Therefore, HCPs should supply information on HIV self-help groups to PLWH who lack social networks so that they can gain the necessary social support and benefits from these groups.
In this study, the AUC in the DT analysis (0.784) was slightly higher than that in the LR analysis (0.747). The 95%CI in the DT analysis also exceeded 0.7, indicating that it was acceptable in terms of diagnostic accuracy. These results highlight the necessity of DT analysis to assess factors influencing HIV infection status disclosure. DT analysis allows for the identification of high-risk groups for behavioral interventions and development of treatment strategies (Lemon et al., Citation2003). In particular, this study presented profiles of subgroups at risk of nondisclosure to the most important supporter and analyzed the differences in subgroup characteristics. These results are useful for HCPs who provide counseling and care for PLWH to identify those who need social support and link them to appropriate interventions and services. Contrastingly, LR analysis is used to identify the average effect of the total sample; it is difficult to identify the characteristics of each subgroup that requires intervention (Fernández et al., Citation2016). DT analysis has disadvantages in that the accuracy is low compared to other data mining methods, such as clustering and neural networks (Kaushal & Shukla, Citation2014), and it is difficult to interpret compared to LT analysis. Therefore, it is suggested that both DT and LR analyzes should be used in exploratory studies or clinical settings to identify the factors associated with disclosure of HIV infection status and distinguish risk groups that require prioritized counseling.
This study’s findings should be interpreted considering several limitations. First, because convenience sampling was used, selection bias may have influenced the results. Therefore, attention should be paid to generalization and interpretation of the study’s results. Second, the distribution of main variables is likely to be overestimated, as participants with low levels of social network characteristics or nondisclosure status may have been relatively more represented in the missing data. Third, secondary data were used, which limited the utilizable variables. In addition to the demographic and social network characteristics included in this study, further research is needed involving disease-related or psychosocial factors (sexual orientation, years since HIV diagnosis, and HIV disease status – CD4 counts and viral suppression) that may affect HIV infection status disclosure.
Conclusions
This study analyzed factors related to disclosure of HIV infection status and social network characteristics in Korean PLWH. The findings showed that 54.7% of the participants disclosed their status to their most important supporter. Five factors affected disclosure: age, self-help group participation, living arrangements, social network relationship, and tie strength. The findings suggest that HCPs need to provide adequate counseling by considering the characteristics of social networks and disclosure status of PLWH. Additionally, researchers should identify high-risk populations using DT analysis. This study is meaningful in that it identifies both high-risk subgroups and factors that affect HIV status disclosure.
Acknowledgements
We thank all the PLWH who participated in our study and the nurses and physicians who cooperated with the research. This study was performed in line with the principles of the Declaration of Helsinki. The authors express our gratitude to Dr. Chang Gi Park, who gave professional advice on research methodology. The previous study from which data were used had obtained approval from the institutional review board of the institution to which the researcher belonged (IRB No: 2015-0040), and additional approval was obtained for the secondary analysis (IRB No: Y-2017-0088). Informed consent was obtained from all participants included in the study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Additional information
Funding
References
- Bairan, A., Taylor, G. A. J., Blake, B. J., Akers, T., Sowell, R., & MendiolaJr.R. (2007). A model of HIV disclosure: Disclosure and types of social relationships. Journal of the American Academy of Nurse Practitioners, 19(5), 242–250. https://doi.org/https://doi.org/10.1111/j.1745-7599.2007.00221.x
- Bogart, L. M., Wagner, G. J., Green, H. D., Mutchler, M. G., Klein, D. J., & McDavitt, B. (2015). Social network characteristics moderate the association between stigmatizing attributions about HIV and non-adherence among Black Americans living with HIV: A longitudinal assessment. Annals of Behavioral Medicine, 49(6), 865–872. https://doi.org/https://doi.org/10.1007/s12160-015-9724-1
- Brown, M. J., Serovich, J. M., Kimberly, J. A., & Umasabor-Bubu, O. (2015). Disclosure and self-efficacy among HIV-positive men who have sex with men: A comparison between older and younger adults. AIDS Patient Care and STDs, 29(11), 625–633. https://doi.org/https://doi.org/10.1089/apc.2015.0133
- Chaudoir, S. R., Fisher, J. D., & Simoni, J. M. (2011). Understanding HIV disclosure: A review and application of the disclosure processes model. Social Science & Medicine, 72(10), 1618–1629. https://doi.org/https://doi.org/10.1016/j.socscimed.2011.03.028
- Elul, B., Basinga, P., Nuwagaba-Biribonwoha, H., Saito, S., Horowitz, D., Nash, D., Mugabo, J., Mugisha, V., Rugigana, E., Nkunda, R., & Asiimwe, A. (2013). High levels of adherence and viral suppression in a nationally representative sample of HIV-infected adults on antiretroviral therapy for 6, 12, and 18 months in Rwanda. PLoS One, 8(1), e53586. https://doi.org/https://doi.org/10.1371/journal.pone.0053586
- Emlet, C. A. (2006). A comparison of HIV stigma and disclosure patterns between older and younger adults living with HIV/AIDS. AIDS Patient Care and STDs, 20(5), 350–358. https://doi.org/https://doi.org/10.1089/apc.2006.20.350
- Eustace, R. W., & Ilagan, P. R. (2010). HIV disclosure among HIV positive individuals: A concept analysis. Journal of Advanced Nursing, 66(9), 2094–2103. https://doi.org/https://doi.org/10.1111/j.1365-2648.2010.05354.x
- Fernández, L., Mediano, P., García, R., Rodríguez, J. M., & Marín, M. (2016). Risk factors predicting infectious lactational mastitis: Decision tree approach versus logistic regression analysis. Maternal and Child Health Journal, 20(9), 1895–1903. https://doi.org/https://doi.org/10.1007/s10995-016-2000-6
- Flickinger, T. E., DeBolt, C., Waldman, A. L., Reynolds, G., Cohn, W. F., Beach, M. C., Ingersol, K., & Dillingham, R. (2017). Social support in a virtual community: Analysis of a clinic-affiliated online support group for persons living with HIV/AIDS. AIDS and Behavior, 21(11), 3087–3099. https://doi.org/https://doi.org/10.1007/s10461-016-1587-3
- Greene, K., Carpenter, A., Catona, D., & Magsamen-Conrad, K. (2013). The brief disclosure intervention (BDI): Facilitating African Americans’ disclosure of HIV. Journal of Communication, 63(1), 138–158. https://doi.org/https://doi.org/10.1111/jcom.12010
- Hosmer, D. W., & Lemeshow, S. (2000). Applied logistic regression. Wiley.
- Hult, J. R., Wrubel, J., Bränström, R., Acree, M., & Moskowitz, J. T. (2012). Disclosure and nondisclosure among people newly diagnosed with HIV: An analysis from a stress and coping perspective. AIDS Patient Care and STDs, 26(3), 181–190. https://doi.org/https://doi.org/10.1089/apc.2011.0282
- Jeong, C. J., Lee, S. O., Kang, J. H., Kim, J. A., Kim, H. R., Oh, K. O., Lee, S. J., Jun, H. Y., & Hong, S. K. (2012). A study on social support networks for each life-cycle stage of adults. The Journal of Korean Academic Society of Nursing Education, 18(3), 436–445. https://doi.org/https://doi.org/10.5977/jkasne.2012.18.3.436
- Kaushal, A., & Shukla, M. (2014). Comparative analysis to highlight pros and cons of data mining techniques-clustering, neural network and decision tree. International Journal of Computer Science and Information Technologies, 5(1), 651–656.
- Kim, G. S., Cho, Y. H., Ra, J. S., & Park, J. Y. (2008). Correlations among self-efficacy, social support networks, and health behavior in undergraduate students. Journal of Korean Academy of Community Health Nursing, 22(2), 211–223. https://doi.org/https://doi.org/10.12799/jkachn.2018.29.3.279
- Korea Centers for Disease Control & Prevention (KCDC). (2019). 2020 HIV/AIDS management guideline. http://www.cdc.go.kr/board.es?mid=a20507020000&bid=0019&act=view&list_no=365658
- Lee, B., Oh, H., Kim, Y., & Jeon, E. (2015). National survey on HIV/AIDS knowledge, attitudes, beliefs, and behavior in the general population. Cheongju: Centers for Disease Control and Prevention (Korea). http://www.cdc.go.kr/board.es?mid=a20301070302&bid=0051&act=view&list_no=127184
- Lemon, S. C., Roy, J., Clark, M. A., Friedmann, P. D., & Rakowski, W. (2003). Classification and regression tree analysis in public health: Methodological review and comparison with logistic regression. Annals of Behavioral Medicine, 26(3), 172–181. https://doi.org/https://doi.org/10.1207/S15324796ABM2603_02
- Lugalla, J., Yoder, S., Sigalla, H., & Madihi, C. (2012). Social context of disclosing HIV test results in Tanzania. Culture, Health & Sexuality, 14(Suppl. 1), S53–S66. https://doi.org/https://doi.org/10.1080/13691058.2011.615413
- Maman, S., van Rooyen, H., & Groves, A. K. (2014). HIV status disclosure to families for social support in South Africa (NIMH Project Accept/HPTN 043). AIDS Care, 26(2), 226–232. https://doi.org/https://doi.org/10.1080/09540121.2013.819400
- Mandrekar, J. N. (2010). Receiver operating characteristic curve in diagnostic test assessment. Journal of Thoracic Oncology, 5(9), 1315–1316. https://doi.org/https://doi.org/10.1097/JTO.0b013e3181ec173d
- Mayfield Arnold, E., Rice, E., Flannery, D., & & Rotheram-Borus, M. J. (2008). HIV disclosure among adults living with HIV. AIDS Care, 20(1), 80–92. https://doi.org/https://doi.org/10.1080/09540120701449138
- Ndu, A. C., Arinze-Onyia, S. U., Aguwa, E. N., & Obi, I. E. (2011). Prevalence of depression and role of support groups in its management: A study of adult HIV/AIDS patients attending HIV/AIDS clinic in a tertiary health facility in South-eastern Nigeria. Journal of Public Health and Epidemiology, 3(4), 182–186. https://doi.org/https://doi.org/10.5897/JPHE.9000093
- Nobre, N. R., Kylmä, J., Kirsi, T., & Pereira, M. (2016). Social networks of older adults living with HIV in Finland. AIDS Care, 28(2), 186–190. https://doi.org/https://doi.org/10.1080/09540121.2015.1071774
- Obermeyer, C. M., Baijal, P., & Pegurri, E. (2011). Facilitating HIV disclosure across diverse settings: A review. American Journal of Public Health, 101(6), 1011–1023. https://doi.org/https://doi.org/10.2105/AJPH.2010.300102
- Seo, M. H., & Jeong, S. H. (2017). Life experiences of uninfected women living with HIV-infected husbands: A phenomenological study. Journal of Korean Academy of Nursing, 47(6), 781–793. https://doi.org/https://doi.org/10.4040/jkan.2017.47.6.781
- Shim, M. S., & Kim, G. S. (2020). Factors influencing young Korean men’s knowledge and stigmatizing attitudes about HIV infection. International Journal of Environmental Research and Public Health, 17(21), 8076. https://doi.org/https://doi.org/10.3390/ijerph17218076
- Song, Y. Y., & Ying, L. U. (2015). Decision tree methods: Applications for classification and prediction. Shanghai Archives of Psychiatry, 27(2), 130–135. https://doi.org/https://doi.org/10.11919/j.issn.1002-0829.215044
- Taggart, T., Grewe, M. E., Conserve, D. F., Gliwa, C., & Isler, M. R. (2015). Social media and HIV: A systematic review of uses of social media in HIV communication. Journal of Medical Internet Research, 17(11), e248. https://doi.org/https://doi.org/10.2196/jmir.4387
- Uphold, C. R., Shehan, C. L., Bender, J. M., & Bender, B. S. (2012). Emotional bonds and social support exchange between men living with HIV infection and their mothers. American Journal of Men’s Health, 6(2), 97–107. https://doi.org/https://doi.org/10.1177/1557988311413118
- Yoshioka, M. R., & Schustack, A. (2001). Disclosure of HIV status: Cultural issues of Asian patients. AIDS Patient Care and STDs, 15(2), 77–82. https://doi.org/https://doi.org/10.1089/108729101300003672
