
ABSTRACT
We quantified treatment challenges faced by people living with HIV (PLHIV) in Russia. Cross-sectional data of 150 PLHIV in Russia were from the 2019 Positive Perspectives Survey. Mean age was 38.3 y. Two-thirds (68.0%[102/150]) had ever disguised their HIV pills, and 43.3%[65/150] said they would be stressed if someone saw their HIV pills. Overall, 14.7%[22/150] reported being ever diagnosed with substance use disorder (SUD). Self-rated optimal health was significantly lower among those with vs without a report of SUD on multiple health domains: sexual (40.9%[9/22] vs. 70.3%[90/128], p = 0.007), physical (22.7%[5/22] vs. 68.0%[87/128], p < 0.001), and overall health (27.3%[6/22] vs. 68.8%[88/128], p < 0.001). Those reporting SUD were more likely to miss HIV medication ≥ 1 time in the past month because they used recreational drugs (age and gender-adjusted prevalence ratio [APR] = 8.23, 95%CI = 6.99-9.68), could not afford their medication (APR = 3.28, 95%CI = 2.90-3.72), had to work (APR = 3.27, 95%CI = 2.97-3.60), or to avoid side effects (APR = 2.62, 95%CI = 2.37-2.89). Furthermore, self-reported SUD was strongly associated with numerous poor health conditions, including self-reported diagnosis of cancer (APR = 6.67, 95%CI = 5.24-8.48), mental illness (APR = 5.01, 95%CI = 4.53-5.55), and liver disease (APR = 4.29, 95%CI = 3.98-4.61). The distinct patterns of poorer health-related outcomes among PLHIV with SUD underscore the need to address behavioral and psychosocial challenges as part of holistic HIV care.
KEYWORDS:
Introduction
While HIV incidence has being declining steadily across most of Europe, the reverse has occurred in the Russian Federation, with a 35.6% increase in the incidence rate seen during 2009–2018 (ECDC/WHO, Citation2019). With about 1 million people living with HIV (PLHIV), Russia has the largest HIV epidemic in the region (ECDC/WHO, Citation2019).
Intimately tied with the HIV epidemic in Russia is an epidemic of injection drug use (Beyrer et al., Citation2017). Russia has the highest number of people who inject drugs in the region (1.8 million) (UNODC, Citation2016), and between 18% and 31% of injection drug users in Russia are thought to be living with HIV (UNODC, Citation2016). People who inject drugs accounted for the largest proportion of new HIV diagnoses in 2016 at 48.8% (Beyrer et al., Citation2017).
Characterizing PLHIV with substance use disorder (SUD) and examining their unique treatment needs is important as perceived treatment needs for HIV care may differ between PLHIV with vs without a history of drug use behavior, possibly because of varying behavioral risk factors and possible co-prevalence of other conditions such as HCV (Degenhardt et al., Citation2017; Mimiaga et al., Citation2010). To gain insights on these issues among PLHIV in Russia, this study assessed characteristics associated with self-reported SUD and explored whether perceived treatment needs differed systematically by SUD status.
Methodology
Data source
We analyzed data for 150 PLHIV from Russia who participated in the 2019 25-country Positive Perspectives Study – a self-reported survey of PLHIV aged ≥ 18 years on ART (de Los Rios et al., Citation2020; Okoli et al., Citation2021a; Okoli et al., Citation2021). Sample size was estimated based on desired precision of estimates using a margin of error of about 10%. Ethical review was provided by the Pearl Institutional Review Board (no. 18–080622).
Measures
We classified participants as having been ever diagnosed with SUD if they selected “Substance misuse – alcohol or drugs” in response to the following statement: “Please select which medical conditions below you have ever been diagnosed with by a doctor or other healthcare professional”. Self-reported viral suppression, self-rated health, ever diagnosis of other conditions, as well as HIV-related privacy behaviors (e.g., Hiding medications), were also assessed.
Suboptimal adherence was defined as a report of ≥ one reason for missing ART for ≥ 5 times within the past month (de Los Rios et al., Citation2020). Polypharmacy was defined as taking 5 + pills per day for any condition, or currently taking medicines for 5 + conditions, including HIV (Okoli et al., Citation2021b).
Analyses
Prevalence estimates were calculated and compared with Chi-square tests (p < 0.05). To explore factors explaining the differences in self-reported health outcomes between PLHIV with vs without self-reported SUD, we fitted several logistic regression models, each adjusting for separate explanatory variables. The control variables included education, employment, domicile, age, HIV duration, gender, polypharmacy, ART adherence, and comorbidities.
Exploratory Poisson regression analyses examined correlates of self-reported SUD among all participants, assessing for the following independent variables: age, gender/sexual orientation, year of HIV diagnosis, domicile, and employment. Age and gender-adjusted prevalence ratios were calculated to explore the relationship between SUD status and self-reported health outcomes that could potentially impair quality of life. Analyses were conducted using R Version 3.6.1.
Results
Of sampled participants, mean (SD) age was 38.3 (9.2) y and mean HIV duration was 6.4 (6.2) y; 66.0%[99/150] were male and 47.3%[71/150] identified as homosexual; 82.7%[124/150] reported viral suppression.
Health behaviors and outcomes associated with self-reported SUD among PLHIV
Overall, 14.7%[22/150] reported being ever diagnosed with SUD; of those diagnosed with HIV in the past one year, 15.2%[19/125] reported being ever diagnosed with SUD. Those with self-reported SUD were older than those not reporting SUD (mean ages = 42.0 vs. 37.7 y, respectively, p = 0.044) and reported being diagnosed with HIV for a greater number of years (11.3 vs. 5.6 y, respectively, p < 0.001). Within adjusted analysis, the likelihood of reporting SUD was about 6 times higher among those identifying as men who have sex with women, compared to men who have sex with men (adjusted prevalence ratio [APR] = 6.02, p = 0.015) ().
Table 1. Adjusted prevalence ratios and corresponding confidence intervals for factors associated with a report of drug use among people living with HIV in Russia, 2019 (N = 150).
Of specific reasons assessed for not sharing HIV status in the past, PLHIV with self-reported SUD reported higher percentage for non-disclosure because of fear of being denied financial benefits (31.8%[7/22] vs. 10.2%[13/128], p = 0.0059) but reported lower percentage for nondisclosure from fear of others telling people about their HIV status (36.4%[8/22] vs. 61.7%[79/128], p = 0.0265) (). PLHIV with self-reported SUD had significantly lower prevalence estimates for the following positive outcomes: optimal sexual health (40.9%[9/22] vs. 70.3%[90/128], p = 0.0074), optimal physical health (22.7%[5/22] vs. 68.0%[87/128], p = 0.0001), and optimal overall health (27.3%[6/22] vs. 68.8%[88/128], p = 0.0002). Furthermore, those with self-reported SUD reported greater anxiety over having to take more and more medications with age (72.7%[16/22] vs. 48.4%[62/128], p = 0.0350). After adjusting for age and gender, strong associations were seen between self-reported SUD and a report of ever being diagnosed with cancer (APR = 6.67, 95%CI, 5.24-8.48), mental illness (APR = 5.01, 95%CI = 4.53-5.55), and liver disease (APR = 4.29, 95%CI = 3.98-4.61), among other outcomes ().
Figure 1. Adjusted prevalence ratios for the relationship between self-reported substance use disorder and self-reported diagnosis of various medical conditions among people living with HIV in the Russian Federation, 2019 (N = 150).
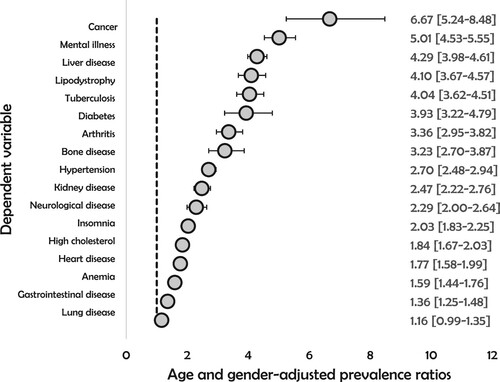
Table 2. Percentage of people living with HIV in Russia who reported various treatment related challenges, overall and by drug use behavior, Russia, 2019 (N = 150).
The observed gap between those with vs. without self-reported SUD in relation to both self-rated overall and physical health remained statistically significant following adjustment for indicators of socio-economic position, socio-demographic factors, and medication characteristics such as polypharmacy and suboptimal adherence. However, statistical significance disappeared following adjustment for underlying non-HIV comorbidities, for both self-rated optimal health (p = 0.117) and physical health (p = 0.070).
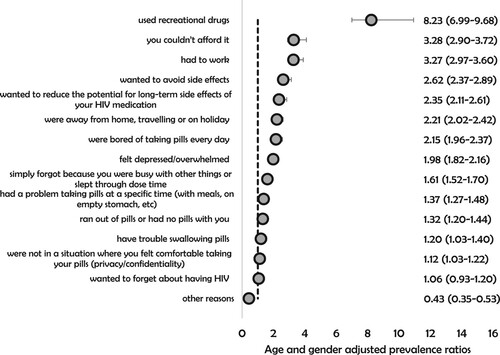
Recreational drug use accounted for only a small percentage of past-month missed HIV medications for ≥ 1 time in the overall population (4.0%, 6/150), although this was significantly higher among those with than without self-reported SUD (13.6%[3/22] vs 2.3%[3/128], respectively, p = 0.013). Other reasons for missing HIV medications in the overall population are depicted in . Compared to those not reporting SUD, those with self-reported SUD had higher likelihoodof missing HIV medication for ≥ 1 time in the past month for the following reasons: used recreational drugs (APR = 8.23, 95%CI = 6.99-9.68), couldn’t afford their medication (APR = 3.28, 95%CI = 2.90-3.72), had to work (APR = 3.27, 95%CI = 2.97-3.60), to avoid side effects (APR = 2.62, 95%CI = 2.37-2.89), and to reduce the potential for long-term side effects of HIV medication (APR = 2.35, 95%CI = 2.11-2.61) ().
Figure 2. Percentage of people living with HIV in Russia who reported different reasons for missing HIV medication for varying number of times in the past month, 2019 (N = 150).
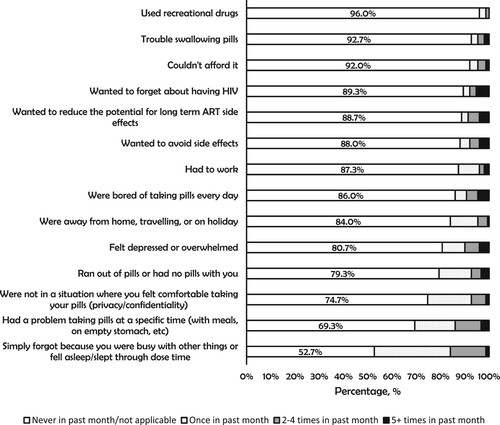
Figure 3. Adjusted prevalence ratios for the relationship between self-reported substance use disorder and reasons for missing HIV medication for at least one time within the past month among people living with HIV in the Russian Federation, 2019 (N = 150).
Treatment challenges in the overall population
PLHIV experienced many physical, emotional, and psychological challenges with their HIV treatment (). Overall, 68.0%[102/150] had ever disguised their HIV medication in the past 6 months to prevent unwanted disclosure, and 43.3%[65/150] reported they would be stressed if someone were to see their medication. Overall, 40.7%[61/150] felt HIV had a negative impact on their life.
The percentage who reported ever switching their ART for any reason was 63.3%[95/150]. Specific reasons for switching among those who switched were: to reduce side effects (57.9%[55/95]), reduce the number of pills (29.5%[28/95]), to reduce the number of medicines taken (24.2%[23/95]), because of ART resistance (12.6%[12/95]), drug–drug interactions (7.4%[7/95]), and cost (3.2%[3/95]).
Overall, 86.0%[129/150] were optimistic that future advances in HIV medicines will improve their overall health and wellbeing and of these 89.2%[115/129] were open to a regimen with fewer medicines while 72.1%[93/129] indicated openness towards a non-daily regimen.
Discussion
This study’s major findings were: (1) 14.6% of all surveyed PLHIV had self-reported SUD and this was associated with poorer health outcomes, multimorbidity, and distinct patterns of nonadherence. (2) Treatment challenges in the overall population were prevalent and diverse, including various emotional, psychological, and physical challenges. The diversity of treatment challenges calls for a diversity of treatment options to meet unique treatment needs. A holistic consideration of patient-related factors beyond virologic control, may improve health-related quality of life as espoused in the fourth “90” target that aims to improve the quality of life among PLHIV (Lazarus et al., Citation2016).
SUD is a diagnosable illness arising from the prolonged and repeated use of one or a combination of substances in high doses, resulting in significant impairment in health and function which may require special treatment (US Department of Health and Human Services, Citation2016). By focusing on SUD, our study may however underestimate recreational drug use behavior among study participants. Only individuals with a report of “ever being diagnosed with [substance misuse] by a doctor or other healthcare professional” were included in the applied definition, effectively capturing only the most serious cases and/or those with access to care. Consequently, whereas only 15.2% of those diagnosed in the past year in our study had a self-reported diagnosis of a substance use disorder, Beyrer and colleagues report that in 2016, people who inject drugs comprised 48.8% of all new diagnosis (Beyrer et al., Citation2017). There is need for barrier-free access to mental health services and addiction among PLHIV with substance use disorder (Pedersen et al., Citation2017).
Limitations
This study has some limitations. First, these data are cross-sectional in nature, and only associations can be drawn. Second, participants were selected non-probabilistically, which may limit the study’s generalizability. Finally, self-reports for variables such as viral control, may be misclassified.
Conclusion
Overall, 14.7% of PLHIV had self-reported SUD; these individuals had poorer health-related outcomes. Within the overall population of PLHIV, a variety of emotional, psychological, and physical challenges to treatment were identified. Increasing flexibility of ART delivery and expandingtreatment choices may improve PLHIV’s health-related quality of life.
Disclosure statement
Authors SK, BY, AP, OM, PdlR, and CO are employees of ViiV Healthcare. EZ and AB are employees of GlaxoSmithKline. No other conflicts of interest were reported.
Additional information
Funding
References
- Beyrer, C., Wirtz, A. L., O’Hara, G., Léon, N., & Kazatchkine, M. (2017). The expanding epidemic of HIV-1 in the Russian Federation. PLoS Medicine, 14(11), e1002462. https://doi.org/10.1371/journal.pmed.1002462
- Degenhardt, L., Peacock, A., Colledge, S., Leung, J., Grebely, J., Vickerman, P., Stone, J., Cunningham, E. B., Trickey, A., Dumchev, K., Lynskey, M., Griffiths, P., Mattick, R. P., Hickman, M., & Larney, S. (2017). Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: A multistage systematic review. The Lancet Global Health, 5(12), e1192–e1207. https://doi.org/10.1016/S2214-109X(17)30375-3
- de Los Rios, P., Okoli, C., Castellanos, E., Allan, B., Young, B., Brough, G., Muchenje, M., Eremin, A., Corbelli, G. M., McBritton, M., Hardy, W. D., & Van de Velde, N. (2021). Physical, emotional, and psychosocial challenges associated with daily dosing of HIV medications and their impact on indicators of quality of life: Findings from the Positive Perspectives study. AIDS and Behavior, 25(3), 961–972. https://doi.org/10.1007/s10461-020-03055-1
- de Los Rios, P., Okoli, C., Punekar, Y., Allan, B., Muchenje, M., Castellanos, E., Richman, B., Corbelli, G. M., Hardy, W. D., Young, B., & Van de Velde, N. (2020). Prevalence, determinants, and impact of suboptimal adherence to HIV medication in 25 countries. Preventive Medicine, 139. https://doi.org/10.1016/j.ypmed.2020.106182
- ECDC/WHO. (2019). European centre for disease prevention and control/WHO Regional Office for Europe. HIV/AIDS Surveillance in Europe 2019–2018 Data. Stockholm: ECDC; 2019. https://www.ecdc.europa.eu/en/publications-data/hivaids-surveillance-europe-2019-2018-data
- Lazarus, J. V., Safreed-Harmon, K., Barton, S. E., Costagliola, D., Dedes, N., Del Amo Valero, J., Gatell, J. M., Baptista-Leite, R., Mendão, L., Porter, K., Vella, S., & Rockstroh, J. K. (2016). Beyond viral suppression of HIV - the new quality of life frontier. BMC Medicine, 14(1), 94. https://doi.org/10.1186/s12916-016-0640-4
- Mimiaga, M. J., Safren, S. A., Dvoryak, S., Reisner, S. L., Needle, R., & Woody, G. (2010). “We fear the police, and the police fear us”: Structural and individual barriers and facilitators to HIV medication adherence among injection drug users in Kiev, Ukraine. AIDS Care, 22(11), 1305–1313. https://doi.org/10.1080/09540121003758515
- Okoli, C., Brough, G., Allan, B., Castellanos, E., Young, B., Eremin, A., Corbelli, G. M., Mc Britton, M., Muchenje, M., Van de Velde, N., & de Los Rios, P. (2021a). Shared decision making between patients and healthcare providers and its association with favorable health outcomes among people living with HIV. AIDS and Behavior 25(5), 1384–1395. https://doi.org/10.1007/s10461-020-02973-4.
- Okoli, C., de Los Rios, P., Eremin, A., Brough, G., Young, B., & Short, D. (2021b). Relationship between polypharmacy and quality of life among people in 24 countries living With HIV. Preventing Chronic Disease, 17, E22. https://doi.org/10.5888/pcd17.190359
- Okoli, C., Van de Velde, N., Richman, B., Allan, B., Castellanos, E., Young, B., Brough, G., Eremin, A., Corbelli, G. M., Mc Britton, M., Hardy, W. D., & de Los Rios, P. (2021). Undetectable equals untransmittable (U = U): awareness and associations with health outcomes among people living with HIV in 25 countries. Sexually Transmitted Infections, 97(1), 18–26. https://doi.org/10.1136/sextrans-2020-054551
- Pedersen, E. R., Marshall, G. N., & Kurz, J. (2017). Behavioral health treatment receipt among a community sample of young adult veterans. The Journal of Behavioral Health Services & Research, 44(4), 536–550. https://doi.org/10.1007/s11414-016-9534-7
- UNODC. (2016). United Nations Office on Drugs and Crime (UNODC) (2016) ‘World Drug Report 2016.’ https://www.unodc.org
- U.S. Department of Health and Human Services (HHS), Office of the Surgeon General. (2016). Facing addiction in America: The surgeon general’s report on alcohol, drugs, and health. Washington, DC: HHS, November.
