
ABSTRACT
The prevalence of non-communicable diseases (NCDs) is increasing in South Africa, in part due to poor nutrition, physical inactivity, and obesity. We characterized the habits and understanding of diet, exercise, and obesity among people with HIV (PWH) taking antiretroviral therapy (ART). We conducted a cross-sectional study of ART-experienced PWH attending an HIV community health center near Cape Town, South Africa. We included PWH currently prescribed ART, older than 21y, and not pregnant. We collected demographic and clinical information and interviewed participants regarding their behaviors and knowledge related to diet, physical activity, and obesity. From March 2015 – February 2016, we enrolled 458 participants. Self-reported diets were low in nutritional diversity: 202 reported eating only starch and protein without vegetable/fruit in the prior 24 h. Although most participants (96%) acknowledged that exercise had health benefits, only 215 participants engaged in daily 30-minute walking or exercise. One quarter of participants recognized nocontributors to obesity, and almost 20% identified no health problems associated with obesity. Participants had diets low in nutritional diversity, modest exercise habits, and limited understanding of the impact of obesity on health. Further understanding of barriers to improving diet and exercise and reducing obesity are essential, especially as PWH age.
KEYWORDS:
Introduction
Poor nutritional diversity, physical inactivity, and obesity contribute to the growing burden of non-communicable diseases (NCDs) in South Africa (Mayosi et al., Citation2009). The rise in obesity is connected to rapid urbanization and economic growth, resulting in a nutrition transition characterized by more high-energy dense foods and a sedentary lifestyle (Cois & Day, Citation2015; Kruger et al., Citation2002; Micklesfield et al., Citation2018; Pisa et al., Citation2015; Sedibe et al., Citation2014; Stringhini et al., Citation2016). Perceptions of body image are also influenced by cultural beliefs that view large body size as a symbol of attractiveness and affluence, especially for black women (Draper et al., Citation2016; Human Sciences Research Council, Citation2014; Muhihi et al., Citation2012; Okop et al., Citation2016). Stigma associated with HIV/AIDS or tuberculosis (TB) further perpetuates favorable opinions of large body size because weight loss occurs with these diseases (Draper et al., Citation2016).
Obesity predisposes individuals to cardiovascular disease (CVD), diabetes, musculoskeletal disorders, and some cancers (World Health Organization, Citation2018a). Compared to other upper-middle income countries, South Africa has the fourth highest probability of dying from one of four common NCDs: CVD, diabetes, cancer, and chronic respiratory diseases (World Health Organization, Citation2011). Without effective measures to reduce obesity, premature deaths due to NCDs in South Africa are likely to rise (World Health Organization, Citation2018b).
South Africa is now facing a double burden of disease, as the NCD threat expands in a region still heavily affected by the HIV epidemic (Mashinya et al., Citation2015; UNAIDS, Citation2017; van Heerden et al., Citation2017; Zungu et al., Citation2019). These competing epidemics are of substantial public health concern as people with HIV (PWH) on ART can live a near normal life expectancy and also face an increased risk of NCDs (Johnson et al., Citation2013). It is critical to understand who is at risk for NCDs and how to implement management strategies within the HIV care framework to curtail the impact of NCDs on morbidity and mortality.
Limited data are available regarding nutrition and exercise among PWH in sub-Saharan Africa (Bukusuba et al., Citation2010; Temu et al., Citation2015, Citation2017). We assessed self-reported patterns of diet and physical activity among ART-experienced PWH attending routine clinical care in South Africa, as well as their understanding of obesity and its relationship with other health problems.
Methods
Study design, setting, and participants
We conducted a cross-sectional study from March 2015 through February 2016 in a health clinic near Cape Town, South Africa that provides HIV, TB, and family planning services (Hyle et al., Citation2019). The local community is predominantly Xhosa with high HIV and TB burden, high unemployment, and low socio-economic status (Middelkoop et al., Citation2010). Participants were eligible if diagnosed with HIV, prescribed ART, older than 21y, and not pregnant (Hyle et al., Citation2019). The study protocol was approved by the Human Research Ethics Committee at University of Cape Town and the Institutional Review Board at Partners HealthCare.
Data collection
A Research Assistant obtained informed consent and interviewed participants using a standardized form to collect demographic and clinical information. As previously described, we defined elevated blood pressure as SBP [DBP] ≥140 [90] mmHg and elevated blood sugar as fasting [random] glucose ≥7.0 [11.0] mmol or self-reported medication use (Hyle et al., Citation2019; Whitworth, Citation2003; World Health Organization, Citation2006). The Research Assistant asked six questions about participants’ diet, physical activity, and the health impact of obesity, based on a questionnaire developed by the Food and Agriculture Organization (FAO) (Macias & Glasauer, Citation2014) (Supplementary Table 1). Participants could select multiple responses, provide a unique free-text answer, or state, “I don’t know”. A Research Nurse extracted data from clinical records regarding height, weight, and HIV and TB treatment (Hyle et al., Citation2019).
Statistical analysis
We reported data for categorical variables as counts and percentages and continuous variables as medians and inter-quartile ranges (IQR). We defined participant knowledge of contributors or health problems associated with obesity based on the number of correct multiple-choice answers (i.e., Selection of 2 > 1>0 answers); we did not categorize any free text answers as correct answers. We then performed Armitage trend tests to examine for associations between patient knowledge regarding obesity with (1) age (≥40y); (2) sex (male); (3) monthly household income (≥R3,500 [top quartile]); (4) obesity (BMI ≥30 kg/m²); (5) duration of ART (≥7.3y [top quartile]); (6) elevated blood pressure or elevated glucose (yes); and (7) history of hypertension or diabetes (yes). We considered p-values ≤0.05 to be statistically significant and used SAS software (version 9.4) (SAS Institute).
Results
Of the 458 participants, 356 (78%) were female, median age was 38y (IQR 33-44y), and median household income was R2,400 (IQR, R1,440-3,500) (). The 125 (27%) participants with elevated blood pressure or glucose were significantly more likely to be male (30% vs 19%, p = 0.01) and older (43y vs 36y, p < 0.001) than those without; BMI was not significantly different.
Table 1. Demographics, diet, and physical activity among ART-experienced adults in South Africa.
Diet and physical activity in the prior 24 h were self-reported (). Most participants (n = 441/448, 98%) acknowledged health benefits of physical activity. Although 91% of participants perceived no barriers to exercise, 36/453 (8%) stated it was difficult to exercise, primarily citing physical pain or tiredness as a cause. No significant differences existed in responses regarding diet or physical activity among participants with or without elevated blood pressure or elevated glucose.
Four hundred fifty-four participants provided responses to the questions regarding contributors to and outcomes of obesity. Although two correct answers were offered as multiple choice, 118 participants (26%) recognized neither contributor and selected the answer, “I don’t know”. Of the remaining 336 participants, 250 (74%) identified only an energy-dense diet, and 54/336 (16%) selected only reduced physical activity; 33/336 participants (10%) correctly identified both contributors to obesity (A). Participants provided 80 distinct answers as contributors to obesity, which we grouped into six themes: being happy (n = 46), medications including ART (n = 12), stress (n = 6), genetics (n = 5), being healthy (n = 6), and unhealthy lifestyles (n = 5).
Figure 1. (A) Participant responses to the question, “Can you tell me the reasons why people are overweight or obese?” Four hundred fifty-four participants responded, including 118 (26%) who stated that they did not know the answer despite being provided with multiple choice answers (box). Among those providing responses, most participants (n=204/336, 61%) endorsed that an energy-dense diet alone was the cause of obesity (black circle), while 20 participants (6%) believed that less physical activity was the only cause (white circle). Only 33 participants (10%) attributed obesity to both diet and physical activity. Eighty participants provided a unique response not offered as a multiple-choice answer in the survey (gray circle). Some participants selected multiple responses (overlapping circles). (B) Participant responses to the question, “What are the health problems that occur when a person is overweight or obese?” Four hundred fifty-four participants responded, including 78 (17%) participants who stated that they did not know (box). Among those providing responses, most (n=283/376, 75%) believed that being overweight or obese only caused chronic illness (black circle) and an additional 14% (n=53/376) of participants believed reduced quality of life was the only health outcome of being overweight or obese (white circle). Only 15 participants (4%) of those providing responses chose both chronic illness and reduced quality of life. Twenty-six participants provided an original response (gray circle). Some participants selected multiple responses (overlapping circles).
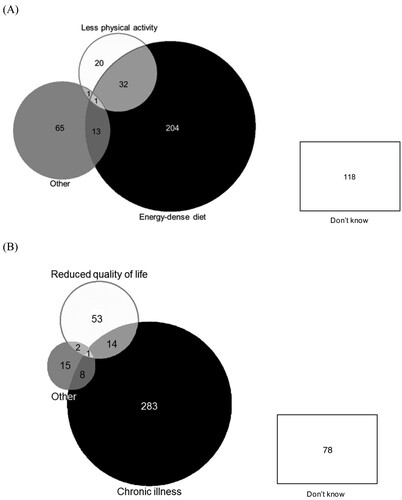
Despite multiple-choice options, 78 participants (17%) stated that they did not know if health problems were linked to obesity. Of the remaining 376 participants, 306 (81%) recognized an association between obesity and chronic illness, and 70 participants (19%) agreed that obesity could result in reduced quality of life; 15 participants (4%) noted both associations (B). No participants correctly responded that obesity could lead to premature death. Participants offered 26 additional answers: shortness of breath (n = 9), excessive sweating (n = 4), chest pain (n = 4), other physical conditions including epilepsy (n = 3) and stroke (n = 3), musculoskeletal pain (n = 2), and not being attractive to one’s husband (n = 1).
Providing more correct answers to the obesity questions was not associated with age ≥40y, male sex, BMI ≥30 kg/m², ART ≥7.3y, or prior diagnosis of hypertension or diabetes. Participants with monthly household income ≥ R3,500 (top quartile) answered more questions correctly about contributors to obesity (p < 0.001); participants with elevated blood pressure or glucose were less likely to select correct answers regarding contributors to obesity (p = 0.01).
Discussion
ART-experienced PWH in South Africa reported poor nutritional diversity in their diets, moderate levels of physical activity, and limited understanding of the health implications of obesity. One-quarter of participants could not specify any contributors to obesity, and almost 20% could not identify any health problems associated with obesity.
Participants’ diets lacked nutritional diversity. Over half of participants reported no fruit or vegetable intake over the prior 24 h, similar to prior reports among women with HIV in Uganda (Bukusuba et al., Citation2010). Poor nutritional diversity can contribute to obesity (Govender et al., Citation2017; Human Sciences Research Council, Citation2014; Micklesfield et al., Citation2013), especially with highly caloric but more affordable foods (Deeks, Citation2011). Potential barriers to nutritionally diverse diets include cost, access to diverse foods, and knowledge of healthy nutrition.
Most participants endorsed that physical activity has benefits, but fewer than half reported daily exercise. These findings are similar to those reported from PWH on ART in Rwanda, in which 70% of participants were inactive according to the World Health Organization’s definition: “not participating in 30 min of moderate physical activity per day for five or more days a week” (Frantz & Murenzi, Citation2013). Inconsistencies between participants’ opinions of exercise and reported behavior suggest potential barriers: available time, safety within the community, cultural beliefs, or fear of negative physical effects with exercise (Roos et al., Citation2015). Qualitative work is needed to understand barriers and to develop strategies to encourage and support increased physical activity.
Although more than half of individuals with available BMI were overweight or obese, 3% of participants recognized all health consequences of obesity, and almost 20% recognized none. An understanding among PWH of obesity-related health risks is essential; elevated BMI is associated with increased inflammation among PWH, leading to early onset of CVD, cancers, and other diseases (Huis In ‘t Veld et al., Citation2018; Mashinya et al., Citation2016; Mave et al., Citation2016). It is especially concerning that individuals with elevated blood pressure or glucose, who are at increased risk of obesity and NCDs, were less likely to provide correct answers regarding the health impact of obesity. Interventions to overcome structural and knowledge barriers are necessary to develop sustainable solutions, especially given weight gain associated with dolutegravir-based ART, which is now first-line ART in South Africa (Hill et al., Citation2019; World Health Organization, Citationn.d.; Republic of South Africa National Department of Health, Citation2020).
This study has limitations. BMI data were not available for many participants because height and weight were not always included in the clinical chart and were not obtained at the study visit. Our findings regarding the associations with BMI are limited to younger participants with fewer years on ART because participants without available BMI were older (39y versus 37y) and had spent longer on ART (7.2y versus 3.0y). We assessed diets within a 24-hour period, which may not be representative of diets over a longer period. Data are from a single site and may not be generalizable to other settings.
Poor nutritional diversity, moderate physical activity, and knowledge gaps regarding obesity and health among ART-experienced PWH were common and could contribute to obesity and NCDs, especially as this population ages. Expanding national and community health education to promote healthy behaviors and reduce obesity will benefit PWH, especially given longer life expectancies on ART.
Authorship
EPH, RAP, and KM designed the study. EPH and EBM wrote the first draft of the manuscript. EPH, EBM, LGB, AX, RAP, RPW, and KM provided critical revisions of the manuscript. All authors have read and approved the final version of the paper.
Ethical standards disclosure
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Human Research Ethics Committee at University of Cape Town (575/2014) and by the Partners Human Research Committee (Institutional Review Board) at Massachusetts General Hospital (2014P001661/PHS). Written informed consent was obtained from all subjects/patients.
Disclaimer
The findings, conclusions, and views expressed in this report are those of the author(s) and do not necessarily represent the official position of their affiliated institutions.
Supplemental Material
Download MS Word (44.5 KB)Acknowledgements
The authors would like to acknowledge Ms. Heidi Freislich, Ms. Alicia Letago, and Ms. Nokukanya Tiyane for their assistance with data collection in this study and Ms. Bridget Bunda, Ms. Mary Feser, and Ms. Maya Hajny Fernandez for their assistance on manuscript preparation.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bukusuba, J., Kikafunda, J. K., & Whitehead, R. G. (2010). Nutritional knowledge, attitudes, and practices of women living with HIV in eastern Uganda. Journal of Health, Population and Nutrition, 28(2), 182–188. https://doi.org/10.3329/jhpn.v28i2.4890
- Cois, A., & Day, C. (2015). Obesity trends and risk factors in the South African adult population. BMC Obesity, 2(1), 42. https://doi.org/10.1186/s40608-015-0072-2
- Deeks, S. G. (2011). HIV infection, inflammation, immunosenescence, and aging. Annual Review of Medicine, 62(1), 141–155. https://doi.org/10.1146/annurev-med-042909-093756
- Draper, C. E., Davidowitz, K. J., & Goedecke, J. H. (2016). Perceptions relating to body size, weight loss and weight-loss interventions in black South African women: A qualitative study. Public Health Nutrition, 19(3), 548–556. https://doi.org/10.1017/S1368980015001688
- Frantz, J. M., & Murenzi, A. (2013). The physical activity levels among people living with human immunodeficiency virus/acquired immunodeficiency syndrome receiving high active antiretroviral therapy in Rwanda. SAHARA J: Journal of Social Aspects of HIV/AIDS Research Alliance, 10(3–4), 113–118. https://doi.org/10.1080/17290376.2014.886081
- Govender, L., Pillay, K., Siwela, M., Modi, A., & Mabhaudhi, T. (2017). Food and nutrition insecurity in selected rural communities of KwaZulu-Natal, South Africa-linking human nutrition and agriculture. International Journal of Environmental Research and Public Health, 14(1), 17. https://doi.org/10.3390/ijerph14010017.
- Hill, A., Venter, F., Delaporte, E., Sokhela, S., Kouanfack, C., Moorhouse, M., McCann, K., Simmons, B., & Calmy, A. (2019, July 22). Progressive rises in weight and clinical obesity for TAF/FTC/DTG and TDF/FTC/DTG versus TDF/FTC/EFV: ADVANCE and NAMSAL trials. International AIDS Society, Mexico City, Mexico.
- Huis In ‘t Veld, D., Pengpid, S., Colebunders, R., & Peltzer, K. (2018). Body mass index and waist circumference in patients with HIV in South Africa and associated socio-demographic, health related and psychosocial factors. AIDS and Behavior, 22(6), 1972–1986. https://doi.org/10.1007/s10461-017-1737-2
- Human Sciences Research Council. (2014). The South African national health and nutrition examination survey, 2012. http://www.hsrc.ac.za/en/research-data/view/6493
- Hyle, E. P., Bekker, L.-G., Martey, E. B., Huang, M., Xu, A., Parker, R. A., Walensky, R. P., & Middelkoop, K. (2019). Cardiovascular risk factors among ART-experienced people with HIV in South Africa. Journal of the International AIDS Society, 22(4), e25274. https://doi.org/10.1002/jia2.25274
- Johnson, L. F., Mossong, J., Dorrington, R. E., Schomaker, M., Hoffmann, C. J., Keiser, O., Fox, M. P., Wood, R., Prozesky, H., Giddy, J., Garone, D. B., Cornell, M., Egger, M., Boulle, A., & International epidemiologic databases to evaluate AIDS Southern Africa collaboration. (2013). Life expectancies of South African adults starting antiretroviral treatment: Collaborative analysis of cohort studies. PLoS Medicine, 10(4), e1001418. https://doi.org/10.1371/journal.pmed.1001418
- Kruger, H. S., Venter, C. S., Vorster, H. H., & Margetts, B. M. (2002). Physical inactivity is the major determinant of obesity in black women in the north west province, South Africa: The THUSA study. Transition and Health during urbanisation of South Africa. Nutrition (Burbank, Los Angeles County, Calif.), 18(5), 422–427. https://doi.org/10.1016/S0899-9007(01)00751-1
- Macias, Y. F., & Glasauer, P. (2014). Guidelines for assessing nutrition-related knowledge, attitudes and practices. Food and Agriculture Organization of the United Nations. http://www.fao.org/docrep/019/i3545e/i3545e00.htm
- Mashinya, F., Alberts, M., Colebunders, R., & Van Geertruyden, J.-P. (2016). Weight status and associated factors among HIV infected people on antiretroviral therapy in rural dikgale, Limpopo, South Africa. African Journal of Primary Health Care & Family Medicine, 8(1), e1–e8. https://doi.org/10.4102/phcfm.v8i1.1230
- Mashinya, F., Alberts, M., Van Geertruyden, J.-P., & Colebunders, R. (2015). Assessment of cardiovascular risk factors in people with HIV infection treated with ART in rural South Africa: A cross sectional study. AIDS Research and Therapy, 12(1), 42. https://doi.org/10.1186/s12981-015-0083-6
- Mave, V., Erlandson, K. M., Gupte, N., Balagopal, A., Asmuth, D. M., Campbell, T. B., Smeaton, L., Kumarasamy, N., Hakim, J., Santos, B., Riviere, C., Hosseinipour, M. C., Sugandhavesa, P., Infante, R., Pillay, S., Cardoso, S. W., Tripathy, S., Mwelase, N., Berendes, S., … ACTG PEARLS and NWCS 319 study team. (2016). Inflammation and change in body weight with antiretroviral therapy initiation in a multinational cohort of HIV-infected adults. The Journal of Infectious Diseases, 214(1), 65–72. https://doi.org/10.1093/infdis/jiw096
- Mayosi, B. M., Flisher, A. J., Lalloo, U. G., Sitas, F., Tollman, S. M., & Bradshaw, D. (2009). The burden of non-communicable diseases in South Africa. Lancet (London, England), 374(9693), 934–947. https://doi.org/10.1016/S0140-6736(09)61087-4
- Micklesfield, L. K., Kagura, J., Munthali, R., Crowther, N. J., Jaff, N., Gradidge, P., Ramsay, M., & Norris, S. A. as members of AWI-Gen the H3Africa Consortium. (2018). Demographic, socio-economic and behavioural correlates of BMI in middle-aged black men and women from urban johannesburg, South Africa. Global Health Action, 11(sup2), 1448250. https://doi.org/10.1080/16549716.2018.1448250.
- Micklesfield, L. K., Lambert, E. V., Hume, D. J., Chantler, S., Pienaar, P. R., Dickie, K., Puoane, T., & Goedecke, J. H. (2013). Socio-cultural, environmental and behavioural determinants of obesity in black South African women: Review articles. Cardiovascular Journal of Africa, 24(9–10), 369–375. https://doi.org/10.5830/CVJA-2013-069
- Middelkoop, K., Bekker, L.-G., Myer, L., Whitelaw, A., Grant, A., Kaplan, G., McIntyre, J., & Wood, R. (2010). Antiretroviral program associated with reduction in untreated prevalent tuberculosis in a South African township. American Journal of Respiratory and Critical Care Medicine, 182(8), 1080–1085. https://doi.org/10.1164/rccm.201004-0598OC
- Muhihi, A. J., Njelekela, M. A., Mpembeni, R., Mwiru, R. S., Mligiliche, N., & Mtabaji, J. (2012). Obesity, overweight, and perceptions about body weight among middle-aged adults in Dar es Salaam, Tanzania. ISRN Obesity, 2012, 1–6. https://doi.org/10.5402/2012/368520
- Okop, K. J., Mukumbang, F. C., Mathole, T., Levitt, N., & Puoane, T. (2016). Perceptions of body size, obesity threat and the willingness to lose weight among black South African adults: A qualitative study. BMC Public Health, 16(1), 365. https://doi.org/10.1186/s12889-016-3028-7
- Pisa, P. T., Pedro, T. M., Kahn, K., Tollman, S. M., Pettifor, J. M., & Norris, S. A. (2015). Nutrient patterns and their association with socio-demographic, lifestyle factors and obesity risk in rural South African adolescents. NutrientS, 7(5), 3464–3482. https://doi.org/10.3390/nu7053464
- Republic of South Africa National Department of Health. (2020). 2019 ART clinical guidelines for the management of HIV in adults, pregnancy, adolescents, children, infants and neonates. https://www.knowledgehub.org.za/system/files/elibdownloads/2020-05/2019%20ART%20Guideline%2028042020%20pdf.pdf
- Roos, R., Myezwa, H., & van Aswegen, H. (2015). “If you have a problem with your heart, you have a problem with your life”: self-perception and behaviour in relation to the risk of ischaemic heart disease in people living with HIV. African Journal of Primary Health Care & Family Medicine, 7(1), 772.vhttps://doi.org/10.4102/phcfm.v7i1.772.
- Sedibe, H. M., Kahn, K., Edin, K., Gitau, T., Ivarsson, A., & Norris, S. A. (2014). Qualitative study exploring healthy eating practices and physical activity among adolescent girls in rural South Africa. BMC Pediatrics, 14(1), 211. https://doi.org/10.1186/1471-2431-14-211
- Stringhini, S., Forrester, T. E., Plange-Rhule, J., Lambert, E. V., Viswanathan, B., Riesen, W., Korte, W., Levitt, N., Tong, L., Dugas, L. R., Shoham, D., Durazo-Arvizu, R. A., Luke, A., & Bovet, P. (2016). The social patterning of risk factors for noncommunicable diseases in five countries: Evidence from the modeling the epidemiologic transition study (METS). BMC Public Health, 16(1), 956. https://doi.org/10.1186/s12889-016-3589-5
- Temu, T. M., Bahiru, E., Bukachi, F., Bloomfield, G. S., Muiruri, P., & Farquhar, C. (2017). Lay beliefs about hypertension among HIV-infected adults in Kenya. Open Heart, 4(1), e000570. https://doi.org/10.1136/openhrt-2016-000570
- Temu, T. M., Kirui, N., Wanjalla, C., Ndungu, A. M., Kamano, J. H., Inui, T. S., & Bloomfield, G. S. (2015). Cardiovascular health knowledge and preventive practices in people living with HIV in Kenya. BMC Infectious Diseases, 15(1), 421. https://doi.org/10.1186/s12879-015-1157-8
- UNAIDS. (2017). Number of people living with HIV. http://aidsinfo.unaids.org/
- van Heerden, A., Barnabas, R. V., Norris, S. A., Micklesfield, L. K., van Rooyen, H., & Celum, C. (2017). High prevalence of HIV and non-communicable disease (NCD) risk factors in rural KwaZulu-Natal, South Africa. Journal of the International AIDS Society, 20(2), e25012. https://doi.org/10.1002/jia2.25012.
- Whitworth, J. A., World Health Organization, International Society of Hypertension Writing Group. (2003). 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. Journal of Hypertension, 21(11), 1983–1992. https://doi.org/10.1097/01.hjh.0000084751.37215.d2.
- World Health Organization. (2006). Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia. https://www.who.int/diabetes/publications/diagnosis_diabetes2006/en/
- World Health Organization. (2011). Global status report on noncommunicable diseases 2014. https://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1
- World Health Organization. (2018a). Obesity and overweight. https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight
- World Health Organization. (2018b). South Africa. https://apps.who.int/iris/bitstream/handle/10665/274512/9789241514620-eng.pdf?ua=1
- World Health Organization. (n.d.). New high-quality antiretroviral therapy to be launched in South Africa, Kenya and over 90 low- and middle-income countries at reduced price. World Health Organization. https://www.who.int/hiv/mediacentre/news/high-quality-arv-reduced-price/en/
- Zungu, N. P., Mabaso, M. L., Kumalo, F., Sigida, S., Mlangeni, L., Wabiri, N., & Chasela, C. (2019). Prevalence of non-communicable diseases (NCDs) and associated factors among HIV positive educators: Findings from the 2015/6 survey of Health of educators in Public schools in South Africa. PloS One, 14(2), e0209756. https://doi.org/10.1371/journal.pone.0209756
