
ABSTRACT
Mother-to-child transmission of Human Immunodeficiency Virus (HIV) has been greatly reduced with the advance of intervention technology. However, adverse pregnancy outcomes (APOs) are still common, and little is known about the driving forces of APOs among pregnant women living with HIV in China. Between January 2004 and December 2020, a total of 638 pregnancies among pregnant women living with HIV were enrolled in this study, 84 (13.2%) pregnancies with 87 APOs were reported. Preterm birth (3.8%), ectopic pregnancy (3.4%), spontaneous abortion (2.0%), and embryo arrest (1.7%) were the most common APOs in pregnant women living with HIV. Exposure to antiretroviral drugs (ARVs) during the first trimester (RR = 4.077, 95% CI: 0.521, 1.484, P<0.001) and the first CD4+ T lymphocyte count (CD4 count)≤ 350/μl (RR = 2.227, 95% CI: 0.063, 0.991, P = 0.026) were risk factors of APOs. The age≤ 30 years (RR = −2.513, 95% CI: −1.067, −0.132, P = 0.012) was associated with the decreasing of APOs. Encouraging people to initiate combination antiretroviral therapy and reach a high CD4 count level before pregnancy would be helpful to prevent APOs. Pregnant women exposed to ARVs in the first trimester needed more attention for APOs.
Introduction
Mother-to-child transmission (MTCT) of the human immunodeficiency virus (HIV) has been well controlled through comprehensive intervention measures, including combination antiretroviral therapy (cART), infant prophylaxis, formula feeding, etc. In developed countries, the MTCT rate of HIV has decreased to 1.1% in 2016 from 6.8% in 2001 (Marcus, Citation2019). According to data released by the National Health Commission of the People's Republic of China, the MTCT rate of HIV dropped to 4.9% in 2017 (Transcript of the National Health Commission's regular press conference in, Citation2018, Citation2018). A study conducted by our team indicated that the total MTCT rate was 1.5% between 2017 and 2018 in Hubei province and the MTCT rate decreased to 0.3% on comprehensive intervention measures in 2020 (Dong et al., Citation2020). With the success of preventing mother-to-child transmission (PMTCT) for HIV, more and more pregnant women living with HIV preferred to deliver the child (Chen et al., Citation2018; Floridia et al., Citation2017; Marcus, Citation2019). Thus, monitoring the health of pregnant women living with HIV is becoming more and more essential.
Adverse pregnancy outcomes (APOs), such as preterm birth, ectopic pregnancy, spontaneous abortion, fetal death, et al., are more common among pregnant women living with HIV. Studies had shown HIV could significantly increase the risk of APOs in pregnant women (Choi et al., Citation2018; Rollins et al., Citation2007), and the influence of the antiretroviral drugs (ARVs) on APOs has gradually attracted attention (Kreitchmann et al., Citation2014). However, the impact of ARVs on APOs is still not clear and inconsistent. Some studies have shown an increased incidence of APOs by exposure to cART during pregnancy (Hu et al., Citation2019; Venkatesh et al., Citation2019), but others hold the opposite view (Lancaster et al., Citation2015). More importantly, previous studies only focused on one kind of APOs or a particular adverse birth outcome (Andany & Loutfy, Citation2013; Ekouevi et al., Citation2011; Hu et al., Citation2019). More studies are needed to evaluate the impact of HIV infection with a combination of ARVs on comprehensive APOs.
This study aimed to explore the incidence of APOs among pregnant women living with HIV in Hubei province, China from 2004 to 2020 and evaluated the associated risk factors.
Materials and methods
The participant recruitment and follow-up
This prospective cohort study was conducted between January 2004 to December 2020. During the study period, all pregnant women who were confirmed with HIV infection during the antenatal care period in Hubei Province were recruited. If a participant had more than one pregnancy during the study period, each pregnancy was treated as a separate event. The participant who had one of the following conditions were excluded: moved to other areas or lost to follow-up before the end of the pregnancy, selecting voluntary termination of pregnancy, or multifetation. All the participants received regular follow-up at 12, 16, 20, 28, 30, 36 weeks during gestation. Participants underwent common pregnancy tests, including ultrasound, blood routine examination, liver and kidney function, blood pressure, and blood sugar. For the pregnant women who had been diagnosed with HIV before pregnancy, the first CD4+ T lymphocyte count (CD4 count) test was performed before 12 weeks of gestation. For pregnant women diagnosed with HIV during pregnancy, the first CD4 count test was taken at the time of confirmation for HIV infection. APOs were ascertained and confirmed by those pregnancy tests and medical history.
Data collection and laboratory test
Demographic information of the participants was collected via the Acquired Immune Deficiency Syndrome (AIDS) Comprehensive Prevention and Control Data Information Management System of the Chinese Center for Disease Control and Prevention (CDC), including age, ethnicity, marital status, HIV status of sexual partner, transmission route of HIV, the time of exposure to ARVs, and the antiretroviral regimens. Laboratory test of pregnant women living with HIV: the first CD4 count during pregnancy was determined by CD4 count test kit (the Beckman Coulter, Inc) and flow cytometry. Enzyme-linked immunosorbent assay tests are used to detect hepatitis B surface antigen (HBsAg), hepatitis C antibody (HCV-Ab), and treponema pallidum antibody (TP-Ab) in women living with HIV. Syphilis infection was diagnosed for positive treponema pallidum antibody test. HBV infection was diagnosed for positive HBsAg. Positive HCV-Ab was diagnosed as HCV infection.
Antiretroviral regimens for pregnant women living with HIV
As recommendations from WHO and Chinese guidelines are constantly updated (WHO, Citation2005, Citation2010, Citation2013) (China, Citation2008; China, Citation2011, Citation2017), the regimens of ARVs for pregnant women living with HIV were categorized as: (1) no ARVs, no ARV drugs were used during pregnancy; (2) single AZT, only AZT during pregnancy; (3) LPV/r-based cART; (4) EFV-based cART; (5) NVP-based cART. The exposure period to ARVs was classified into the first, the second, and the third trimester, which were defined as 1-13, 14-27, and ≥ 28 weeks of gestation, respectively.
Adverse pregnancy outcomes and definitions
The following criteria were used to measure different APOs: (1) Preterm birth, childbirth before 37 weeks of pregnancy (259 days from the first day of the mother's last menstrual period, or 245 days after fertilization); (2) Stillbirth, the event that a fetus is born dead or stillborn; (3) Fetal death, death of the developing young in utero after 20 weeks of gestation; (4) Spontaneous abortion, expulsion of the product of fertilization before completing the term of gestation and without deliberate interference; (5) Ectopic pregnancy, a potentially life-threatening condition in which embryo implantation occurs outside the cavity of the uterus; (6) Pregnancy Induced Hypertension (PIH), a condition in pregnant women with elevated systolic (>140mmHg) and diastolic (>90mmHg) blood pressure on at least two occasions 6 h apart; (7) Gestational diabetes, defined as diabetes mellitus induced by pregnancy but resolved at the end of pregnancy; (8) Embryo arrest, defined as a stage at which an embryo dies and ceases to develop before 20 weeks of gestation; (9) Threatened abortions, uterine bleeding from a gestation of less than 20 weeks without any cervical dilatation. (“CitationQueensland Clinical Guideline: Gestational diabetes mellitus (GDM),”; “CitationQueensland Clinical Guideline: Hypertension and pregnancy,”; “CitationQueensland Clinical Guideline: Preterm labor and birth,”).
Statistical analysis
Continuous variables were expressed as means ± standard deviation (SD). Categorical variables were presented as count (%). Comparisons of continuous variables (abnormal distribution) were assessed using the Mann–Whitney U test, while categorical variables were evaluated using the χ2 or Fisher exact test. Furthermore, the multivariable modified Poisson regression method was used to estimate the simultaneous effects of risk factors of APOs in pregnant women living with HIV after adjusted for confounders including age, marital status, HIV status of sexual partner, transmission route of HIV, HBV infection, HCV infection, syphilis infection, CD4 count during pregnancy, ARVs regimen, the gestation of exposure to ARVs. The Risk Ratio (RR) and 95% confidence intervals (CI) were calculated in the model. Statistical significance was defined as a two-sided p-value of less than 0.05. Statistical analyses were conducted using the IBM SPSS Statistics (Version 20.0) software. Results were presented as RR with 95% CI generated using the forest plot package in Graphpad Prism (Version 8.2).
Results
The pregnant women living with HIV enrolled in the study
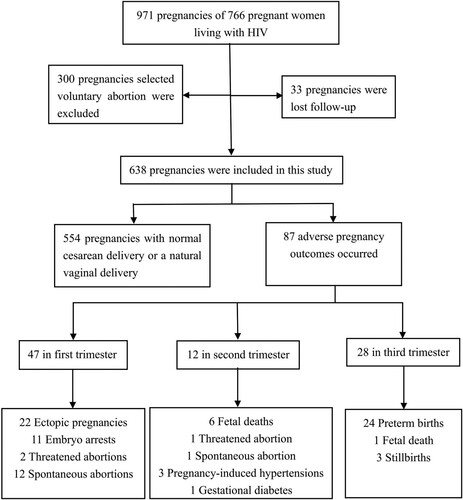
In total, 766 pregnant women living with HIV (971 pregnancies) were recruited in Hubei province from January 2004 to December 2020. Among them, 300 pregnancies (30.9%) who selected voluntary termination of pregnancy, and 33 pregnancies who were lost follow-up were excluded. Thus, a total of 638 pregnancies among participants were included in this reported study. ()
Figure 1. Flow chart for inclusion and exclusion of participants.
APOs
Overall, 22.3% (126/564) pregnant women living with HIV had twice or more times pregnancies. Among all enrolled 638 pregnancies, 84 (13.2%) pregnancies with 87 APOs were reported. There were 3.8% (24/638) preterm birth, 3.4% (22/638) ectopic pregnancies, 2.0% (13/638) spontaneous abortion, 1.7% (11/638) embryo arrest, 1.0% (7/638) fetal death, 0.5% (3/638) stillbirth, 0.5% (3/638) threatened abortions, 0.5% (3/638) PIH, 0.2% (1/638) gestational diabetes in all participants. ()
The risk factors of APOs among pregnant women living with HIV
Compared with pregnant women without APOs, the pregnant women with APOs were older (P = 0.001), have a high HCV prevalence (P = 0.004), unmarried (P = 0.022), and transmitted through sex transmission (P = 0.006). () There is no significant difference in the incidence of APOs between the pregnant women exposed to ARVs (55/379, 14.5%) and the pregnant women without ARVs (29/259, 11.2%) during pregnancy (P = 0.224). It's worth noting that the pregnant women living with HIV exposed to ARVs during the first trimester had a higher rate of APOs than those who were free for ARVs, exposed to ARVs during the second and third trimester (P = 0.001). No significant differences in the ethnicity, HIV status of sexual partner, HBV infection, syphilis infection, antiretroviral regimens, and CD4 count during pregnancy were observed between the two groups. ()
Table 1. Demographic information of pregnant women living with HIV (N = 638 pregnancies).
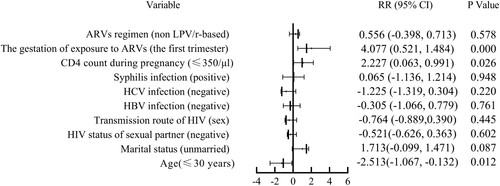
Multivariable modified Poisson regression method suggested that exposure to ARVs during the first trimester (RR = 4.077, 95% CI: 0.521, 1.484, P<0.001) and the first CD4 count≤ 350/μl (RR = 2.227, 95% CI: 0.063, 0.991, P = 0.026) were risk factors of APOs in pregnant women living with HIV. And the age≤ 30 years (RR = −2.513, 95% CI: −1.067, −0.132, P = 0.012) could reduce the occurrence of APOs in pregnant women living with HIV after adjusting for other factors. ()
Figure 2. Risk factors of APOs in pregnant women living with HIV.
Discussion
More than one million women living with HIV of reproductive age become pregnant globally each year (Myer et al., Citation2018), understanding the incidence and risk factors of APOs is essential in further improving the health of pregnant women living with HIV. Our study extended the existing literature by follow-up the pregnant women living with HIV in Hubei province, China, during 2004-2020. The incidence and the composition of APOs in pregnant women living with HIV were investigated. In addition, the risk factors of APOs were explored to provide a reference for PMTCT of HIV.
The incidences of APOs among pregnant women living with HIV vary significantly among different countries and regions (Hu et al., Citation2019; Onono et al., Citation2021; Tarar et al., Citation2021). The rate of preterm birth (3.8%), spontaneous abortion (2.0%), fetal death (1.0%), and stillbirth (0.5%) in Hubei province is lower than that in Pakistan and Kenya (Onono et al., Citation2021; Tarar et al., Citation2021). The total incidence of APOs among pregnant women living with HIV in our study (13.2%) is higher than former study among HIV-negative pregnant women in China (9.7%) (Jiayu et al., Citation2011). One study also showed that pregnant women living with HIV had a higher incidence of preterm birth and ectopic pregnancy than HIV-negative pregnant women (3.76% vs. 1.16%, 3.45% vs. 0.08%) (Pan et al., Citation2016). In addition, other studies suggested that the incidence of APOs in pregnant women living with HIV was higher than that in HIV-negative pregnant women in other countries (Gray & McIntyre, Citation2007; Haeri et al., Citation2009; Ørbaek et al., Citation2020). Due to regional differences in economic levels, maternal care service and the rate of selected voluntary abortion can deviate from the results of different studies. In general, more comprehensive health counseling and examination should be provided to pregnant women with HIV to reduce the incidence of APOs.
Our study found that exposure to ARVs during pregnancy did not increase the incidence of APOs. As is known to all, cART can significantly decrease the MTCT of HIV. By mid-2019, almost all low-middle income countries were fully implementing lifelong cART (WHO, Citation2019). Previous studies have shown that pregnant women living with HIV who did not receive cART tend to have a high incidence of spontaneous abortion, ectopic pregnancy, and stillbirth than pregnant women with cART (Ganguly et al., Citation2021; Hu et al., Citation2019), as they tend to have a high incidence of vaginal inflammation (Rittenhouse et al., Citation2021). Meanwhile, our study also found that CD4 count≤ 350/μl could significantly increase the incidence of APOs in pregnant women living with HIV. Although the CD4 count of pregnant women living with HIV fluctuates over time, few women were tested for CD4 count multiple times during pregnancy. Our finding is consistent with the previous studies, which reported that low CD4 count was associated with preterm birth, stillbirth, and spontaneous abortion in pregnant women living with HIV (Ezechi et al., Citation2012; Ezechi et al., Citation2013; Favarato et al., Citation2019). Thus, initiating cART early and maintaining a high CD4 count before pregnancy would be essential in reducing APOs.
Our study also suggested that the pregnant women living with HIV exposure to ARVs during the first trimester had a high rate of APOs. This finding is consistent with the results of a European collaborative study, which showed that the use of highly active antiretroviral therapy increased the rate of preterm birth to 24.9% over four years, especially starting early at the first trimester can lead to severe preterm birth (Thorne et al., Citation2004). Another study showed that first-trimester initiation of protease inhibitors or integrase strand transfer inhibitors were associated with preterm birth (O'Brien et al., Citation2020). And there has also been shown that pregnant women who received cART before pregnancy have a higher incidence of spontaneous abortion, preterm birth, and stillbirth than pregnant women who begin antiretroviral therapy after pregnancy (Theron et al., Citation2021; Uthman et al., Citation2017). Because prolonged cART before pregnancy can lead to maternal vascular malperfusion and affect placental growth (Dos Reis et al., Citation2020; Ikumi et al., Citation2021). Studies have shown that the association between ARVs and APOs may be placental mediated, particularly during placental implantation and development (Ikumi et al., Citation2021). And animal models also show that ARVs may disrupt nerve development and maturation (Sarkar et al., Citation2020). Starting cART as early as possible has been a consensus. But the pregnant women living with HIV exposure to ARVs in the first trimester needed more attention, such as pregnancy-related examination and guidance from professional doctors.
This study also had some limitations. First, HIV viral load (VL) was also used as an essential evaluation index, but VL did not widely carry out in the early stage of this study, and pregnant women in some resource-limited areas were not tested for their VL during pregnancy. Second, there is an unavoidable statistical bias because it is impossible to assess the likelihood of APOs in selective voluntary abortions. Finally, we have a limited number of participants and need more investigation to explore the association between ARVs and APOs.
In conclusion, our study revealed pregnant women living with HIV had a high rate of APOs. For reducing the incidence of APOs, cART should be provided as early as possible, and a high-level CD4 count should be maintained. Pregnant women living with HIV exposed to ARVs in the first trimester had a higher risk for APOs, which needed more attention.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Andany, N., & Loutfy, M. R. (2013). HIV protease inhibitors in pregnancy. Drugs, 73(3), 229–247. https://doi.org/10.1007/s40265-013-0017-3
- Chen, F. F., Guo, W., Qin, Q. Q., Cai, C., & Cui, Y. (2018). Spatial-temporal distribution of newly detected HIV/AIDS cases among aged 15 years or older women in China, 2010-2016. Zhonghua liu Xing Bing xue za zhi = Zhonghua Liuxingbingxue Zazhi, 39(6), 739–744. https://doi.org/10.3760/cma.j.issn.0254-6450.2018.06.009
- China. (2008). Implementationplanforpreventionofmother-to-childtransmissionofHIV(revised). http://www.gov.cn/gzdt/2008-05/30/content_999767.htm
- China. (2011). Implementation plan for prevention of mother-to-child transmission of HIV, syphilis, and hepatitis B. https://view.officeapps.live.com/op/view.aspx?src=http%3A%2F%2Fwww.gov.cn%2Fgzdt%2Fatt%2Fatt%2Fsite1%2F20110224%2F001e3741a2cc0ecfebbf01.doc&wdOrigin=BROWSELINK
- China. (2017). Implementation plan for prevention of mother-to-child transmission of HIV, syphilis, and hepatitis B. https://www.chinacdc.cn/jkzt/fybj/xgzcfg/201801/P020180104574896456689.pdf
- Choi, H., Kim, M. H., Lee, S. J., Kim, E. J., Lee, W., Jeong, W., Jung, I. Y., Ahn, J. Y., Jeong, S. J., Ku, N. S., Baek, J. H., Choi, Y. H., Kim, H. Y., Kim, J. M., & Choi, J. Y. (2018). Pregnancy rates and outcomes of HIV-infected women in korea. Journal of Korean Medical Science, 33(47), e296. https://doi.org/10.3346/jkms.2018.33.e296
- Dong, Y., Guo, W., Gui, X., Liu, Y., Yan, Y., Feng, L., & Liang, K. (2020). Preventing mother to child transmission of HIV: Lessons learned from China. BMC Infectious Diseases, 20(1), 792. https://doi.org/10.1186/s12879-020-05516-3
- Dos Reis, H. L. B., Boldrini, N. A. T., Rangel, A. F. R., Barros, V. F., Merçon de Vargas, P. R., & Miranda, A. E. (2020). Placental growth disorders and perinatal adverse outcomes in Brazilian HIV-infected pregnant women. PloS One, 15(4), e0231938. https://doi.org/10.1371/journal.pone.0231938
- Ekouevi, D. K., Coffie, P. A., Ouattara, E., Moh, R., Amani-Bosse, C., Messou, E., Sissoko, M., Anglaret, X., Eholié, S. P., Danel, C., & Dabis, F. (2011). Pregnancy outcomes in women exposed to efavirenz and nevirapine: An appraisal of the IeDEA West Africa and ANRS databases, abidjan, côte d'Ivoire. Journal of Acquired Immune Deficiency Syndromes, 56(2), 183–187. https://doi.org/10.1097/QAI.0b013e3181ff04e6
- Ezechi, O. C., David, A. N., Gab-Okafor, C. V., Ohwodo, H., Oladele, D. A., Kalejaiye, O. O., Ezeobi, P. M., Gbajabiamila, T. A., Adu, R. A., Oke, B., Musa, Z. A., Ekama, S. O., Ilesanmi, O., Odubela, O., Somefun, E. O., Herbertson, E. C., Onwujekwe, D. I., & Ujah, I. A. (2012). Incidence of and socio-biologic risk factors for spontaneous preterm birth in HIV positive Nigerian women. BMC Pregnancy and Childbirth, 12(1), 93. https://doi.org/10.1186/1471-2393-12-93
- Ezechi, O. C., Gab-Okafor, C. V., Oladele, D. A., Kalejaiye, O. O., Oke, B. O., Ohwodo, H. O., Adu, R. A., Ekama, S. O., Musa, Z., Onwujekwe, D. I., David, A. N., & Ujah, I. A. (2013). Pregnancy, obstetric and neonatal outcomes in HIV positive Nigerian women. African Journal of Reproductive Health, 17(3), 160–168. PMID: 24069778.
- Favarato, G., Townsend, C. L., Peters, H., Sconza, R., Bailey, H., Cortina-Borja, M., Tookey, P., & Thorne, C. (2019). Stillbirth in Women Living With HIV Delivering in the United Kingdom and Ireland: 2007-2015. Journal of Acquired Immune Deficiency Syndromes, 82(1), 9–16. https://doi.org/10.1097/QAI.0000000000002087
- Floridia, M., Tamburrini, E., Masuelli, G., Martinelli, P., Spinillo, A., Liuzzi, G., Vimercati, A., Alberico, S., Maccabruni, A., Pinnetti, C., Frisina, V., Dalzero, S., & Ravizza, M. (2017). Rate, correlates and outcomes of repeat pregnancy in HIV-infected women. HIV Medicine, 18(6), 440–443. https://doi.org/10.1111/hiv.12473
- Ganguly, S., Chakraborty, D., Goswami, D. N., Biswas, S., Debnath, F., & Saha, M. K. (2021). High Stillbirth among HIV-infected pregnancy in West Bengal, India; A retrospective cohort study. Japanese Journal of Infectious Diseases, 74(5), 424–428. https://doi.org/10.7883/yoken.JJID.2020.811
- Gray, G. E., & McIntyre, J. A. (2007). Hiv and pregnancy. BMJ, 334(7600), 950–953. https://doi.org/10.1136/bmj.39176.674977.AD
- Haeri, S., Shauer, M., Dale, M., Leslie, J., Baker, A. M., Saddlemire, S., & Boggess, K. (2009). Obstetric and newborn infant outcomes in human immunodeficiency virus-infected women who receive highly active antiretroviral therapy. American Journal of Obstetrics and Gynecology, 201(3), 315.e311–315. https://doi.org/10.1016/j.ajog.2009.06.017
- Hu, F., Liang, J. J., Lu, J. J., Hu, Y. F., Hu, Y., Yu, J., Zou, X. W., Ma, Y. H., & Lin, S. F. (2019). Effects of antiretroviral therapy and HIV exposure in utero on adverse pregnancy and infant outcomes: A prospective cohort study in guangzhou, China. Biomedical and Environmental Sciences, 32(10), 719–729. https://doi.org/10.3967/bes2019.092
- Ikumi, N. M., Malaba, T. R., Pillay, K., Cohen, M. C., Madlala, H. P., Matjila, M., Anumba, D., Myer, L., Newell, M.-L., & Gray, C. M. (2021). Differential impact of antiretroviral therapy initiated before or during pregnancy on placenta pathology in HIV-positive women. AIDS (London, England), 35(5), 717–726. https://doi.org/10.1097/QAD.0000000000002824
- Jiayu, N., Ling, J., & Zhen, Y. (2011). Analysis on the influencing factors of adverse pregnancy outcomes in natural pregnancy women. Clinical Medicine &Engineering, 28(11), 1589–1590. https://doi.org/10.3969/j.issn.1674-4659.2021.11.1589
- Kreitchmann, R., Li, S. X., Melo, V. H., Fernandes Coelho, D., Watts, D. H., Joao, E., Coutinho, C. M., Alarcon, J. O., & Siberry, G. K. (2014). Predictors of adverse pregnancy outcomes in women infected with HIV in Latin America and the Caribbean: a cohort study. BJOG : an international journal of obstetrics and gynaecology, 121(12), 1501–1508. https://doi.org/10.1111/1471-0528.12680
- Lancaster, K. E., Kwok, C., Rinaldi, A., Byamugisha, J., Magwali, T., Nyamapfeni, P., Salata, R. A., & Morrison, C. S. (2015). Incident pregnancy and pregnancy outcomes among HIV-infected women in Uganda and Zimbabwe. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics, 131(3), 255–259. https://doi.org/10.1016/j.ijgo.2015.06.035
- Marcus, U. (2019). HIV infections and HIV testing during pregnancy, Germany, 1993 to 2016. Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin, 24(48), 1900078. https://doi.org/10.2807/1560-7917.ES.2019.24.48.1900078
- Myer, L., Phillips, T. K., Zerbe, A., Brittain, K., Lesosky, M., Hsiao, N.-Y., Remien, R. H., Mellins, C. A., McIntyre, J. A., & Abrams, E. J. (2018). Integration of postpartum healthcare services for HIV-infected women and their infants in South Africa: A randomised controlled trial. PLoS Medicine, 15(3), e1002547. https://doi.org/10.1371/journal.pmed.1002547
- O'Brien, B. E., Williams, P. L., Huo, Y., Kacanek, D., Chadwick, E. G., Powis, K. M., Correia, K., Haddad, L. B., Yee, L. M., Chakhtoura, N., Dola, C., & Van Dyke, R. B. (2020). Repeat pregnancies Among US women living With HIV in the SMARTT study: Temporal changes in HIV Disease status and Predictors of preterm birth. Journal of Acquired Immune Deficiency Syndromes, 85(3), 346–354. https://doi.org/10.1097/QAI.0000000000002445
- Onono, M., Odwar, T., Wahome, S., Helova, A., Bukusi, E. A., Hampanda, K., Turan, J., & Abuogi, L. (2021). Behavioral interventions can mitigate adverse pregnancy outcomes Among women conceiving on ART and those initiated on ART during pregnancy: Findings from the MOTIVATE trial in southwestern Kenya. Journal of Acquired Immune Deficiency Syndromes, 86(1), 46–55. https://doi.org/10.1097/QAI.0000000000002521
- Ørbaek, M., Thorsteinsson, K., Moseholm Larsen, E., Katzenstein, T. L., Storgaard, M., Johansen, I. S., Pedersen, G., Bach, D., Helleberg, M., Weis, N., & Lebech, A. M. (2020). Risk factors during pregnancy and birth-related complications in HIV-positive versus HIV-negative women in Denmark, 2002-2014. HIV Medicine, 21(2), 84–95. https://doi.org/10.1111/hiv.12798
- Pan, Y., Zhang, S., Wang, Q., Shen, H., Zhang, Y., Li, Y., Yan, D., & Sun, L. (2016). Investigating the association between prepregnancy body mass index and adverse pregnancy outcomes: A large cohort study of 536 098 Chinese pregnant women in rural China. BMJ Open, 6(6), e011227. https://doi.org/10.1136/bmjopen-2016-011227
- Queensland Clinical Guideline: Gestational diabetes mellitus (GDM). https://www.health.qld.gov.au/.
- Queensland Clinical Guideline: Hypertension and pregnancy. https://www.health.qld.gov.au/.
- Queensland Clinical Guideline: Preterm labor and birth. https://www.health.qld.gov.au/.
- Rittenhouse, K. J., Mwape, H., Nelson, J. A. E., Mwale, J., Chipili, G., Price, J. T., Hudgens, M., Stringer, E. M., De Paris, K., Vwalika, B., & Stringer, J. S. A. (2021). Maternal HIV, antiretroviral timing, and spontaneous preterm birth in an urban Zambian cohort: The role of local and systemic inflammation. Aids (london, England), 35(4), 555–565. https://doi.org/10.1097/QAD.0000000000002808
- Rollins, N. C., Coovadia, H. M., Bland, R. M., Coutsoudis, A., Bennish, M. L., Patel, D., & Newell, M.-L. (2007). Pregnancy outcomes in HIV-infected and uninfected women in rural and urban South Africa. Journal of acquired immune deficiency syndromes (1999), 44(3), 321–328. https://pubmed.ncbi.nlm.nih.gov/17195768 https://doi.org/10.1097/QAI.0b013e31802ea4b0
- Sarkar, A., Balogun, K., Guzman Lenis, M. S., Acosta, S., Mount, H. T., & Serghides, L. (2020). In utero exposure to protease inhibitor-based antiretroviral regimens delays growth and developmental milestones in mice. PloS One, 15(11), e0242513. https://doi.org/10.1371/journal.pone.0242513
- Tarar, S. H., Afzal, M., Atta, H., & Shah, S. M. A. (2021). Obstetric outcomes of Human Immunodeficiency Virus positive mothers in tertiary care hospital. Journal of the Pakistan Medical Association, 71, 69–72. https://doi.org/10.47391/jpma.552
- Theron, G., Brummel, S., Fairlie, L., Pinilla, M., McCarthy, K., Owor, M., Chinula, L., Makanani, B., Violari, A., Moodley, D., Chakhtoura, N., Browning, R., Hoffman, R., & Fowler, M. G. (2021). Pregnancy outcomes of women conceiving on antiretroviral therapy (ART) compared to those commenced on ART during pregnancy. Journal of Biochemistry and Molecular Biology, 73(2), e312–e320. https://doi.org/10.1093/cid/ciaa805
- Thorne, C., Patel, D., & Newell, M.-L. (2004). Increased risk of adverse pregnancy outcomes in HIV-infected women treated with highly active antiretroviral therapy in Europe. AIDS (London, England), 18(17), 2337–2339. https://pubmed.ncbi.nlm.nih.gov/15577551 https://doi.org/10.1097/00002030-200411190-00019
- Transcript of the National Health Commission's regular press conference in 2018. (2018). http://www.scio.gov.cn/xwfbh/gbwxwfbh/xwfbh/wsb/Document/1642083/1642083.htm.
- Uthman, O. A., Nachega, J. B., Anderson, J., Kanters, S., Mills, E. J., Renaud, F., Essajee, S., Doherty, M. C., & Mofenson, L. M. (2017). Timing of initiation of antiretroviral therapy and adverse pregnancy outcomes: a systematic review and meta-analysis. The lancet. HIV, 4(1), e21–e30. https://doi.org/10.1016/S2352-3018(16)30195-3
- Venkatesh, K. K., Farhad, M., Fenton, T., Moodley, D., Naik, S., Nakabiito, C., Fairlie, L., Fowler, M. G., Stringer, J. S. A., & Chi, B. H. (2019). Association between HIV antiretroviral therapy and preterm birth based on antenatal ultrasound gestational age determination: a comparative analysis. AIDS (London, England), 33(15), 2403–2413. https://doi.org/10.1097/QAD.0000000000002367
- WHO. (2005). Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Guidelines on care, treatment, and support for women living with HIV/AIDS and their children in resource-constrained settings. https://www.who.int/hiv/pub/mtct/en/arvdrugsguidelines_web.pdf
- WHO. (2010). Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Recommendations for a public health approach. http://apps.who.int/iris/bitstream/handle/10665/75236/9789241599818_eng.pdf;sequence=1
- WHO. (2013). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Recommendations for a public health approach. https://www.who.int/publications/i/item/9789241505727
- WHO. (2019). HIV/AIDs data and statistics. https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/prevention-of-mother-to-child-transmission
