
ABSTRACT
Adolescents living with HIV (ALHIV) struggle to remain engaged in HIV-related care and adhere to antiretroviral treatment (ART) due to a myriad of physical, psychological and cognitive-developmental challenges. We report on the profile of ALHIV aged 10–19 years on ART and the clinical factors associated with their retention in care. A retrospective cohort analysis was conducted with 16,108 ALHIV, aged 10–19 years, who were enrolled in 136 ART clinics in the Ehlanzeni district. Anonymised data were obtained from electronic medical records (Tier.net). Trends in retention in care among adolescents on ART was described using Kaplan-Meier survival estimates. Cox proportional analysis was performed to identify factors associated with retention in care over 2 years. More than half (53%) were females, and median duration on ART was 8 months. Retention in care among adolescents at months 6, 12, 18 and 24 was 90.5%, 85.4%, 80.8% and 76.2%, respectively. After controlling for confounders, risk of dying or lost to follow up increased for female adolescents (aHR = 1.28, 95% CI 1.10–1.49); being initiated on ART while pregnant (aHR = 2.72, 95% CI 1.99–3.69); history of TB infection (aHR = 1.71, 95% CI 1.10–2.65); and started ART at age 10–14 years (aHR = 2.45, 95% CI 1.96–3.05), and 15–19 years (aHR = 9.67, 95% CI 7.25–12.89). Retention in care among adolescents on ART over two-year period was considerably lower than the UNAIDS 2030 target of 95%. Of particular concern for intervention is the lower rates of retention in care among females and pregnant adolescents and starting ART between the ages of 10 and 19 years. Family or caregivers and peer support groups centred interventions designed to promote early initiation and retention in care through early case identification are needed.
Introduction
In 2018, an estimated 1.8 million adolescents (aged 10–19 years) were living with HIV (ALHIV) globally (Enane et al., Citation2018; MacPherson et al., Citation2015; Mark et al., Citation2017), of which 61.1% reside in Eastern and Southern Africa (Enane et al., Citation2018). Adolescents are the fastest growing age group of people living with HIV (PLHIV) (Naidoo, Munsami, & Archary, Citation2015), representing about 90% of those living with HIV in sub-Saharan Africa (Gittings et al., Citation2016). While the incidence of HIV amongst adults and children younger than 10 years has declined in the last decade, the HIV incidence amongst adolescents between the ages of 10 and 19 years has increased within the same period (Enane et al., Citation2018; Slogrove, Mahy, Armstrong, & Davies, Citation2017). The increase in HIV amongst adolescents is attributed to a generation of children infected with HIV prenatally who are surviving into adolescence, and increased incidence resulting from risky (sexual) behaviour (Enane et al., Citation2018).
To combat the increasing incidence of HIV and reduce AIDS-related mortality, UNAIDS in 2014 set an ambitious 95-95-95 target. The aim of the 95-95-95 target is end the AIDS epidemic by 2030 by achieving 95% of all PLHIV know their status; 95% of all diagnosed HIV positive on antiretroviral therapy (ART); and 95% of all those on treatment virally suppressed (UNAIDS, Citation2014). In August 2017, the South African National Department of Health (NDoH) rolled out the universal test and treat (UTT) campaign that aimed to make ART available to all PLHIV, regardless of their CD4 count, and with an emphasis on providing same-day initiation (SDI) subject to clinical and psychological readiness (Lilian, Rees, Mcintyre, Struthers, & Petersid, Citation2020). Despite tremendous gains made by the South African government in the implementation of UTT, adherence and retention in care among adolescents (10–19 years) remain poor (Kusemererwa et al., Citation2021). Therefore, AIDS-related deaths among ALHIV have increased compared to decreases among adults and children under 10 years (Ajayi, Otukpa, Mwoka, Kabiru, & Ushie, Citation2021; Enane et al., Citation2018; Gittings et al., Citation2016; Nachega, Mills, & Schechter, Citation2010). Adolescents experience a myriad of physical, psychological and cognitive developmental changes at this stage in life, which challenge adherence to ART and remaining engaged in care (Busza, Dauya, Bandason, Mujuru, & Ferrand, Citation2014; Hudelson & Cluver, Citation2015; Shroufi et al., Citation2013).
The World Health Organization (WHO) describes “retention in HIV care” as the continuous engagement from diagnosis in a package of prevention, treatment, support and care services (World Health Organization, Citation2011). Several studies reported on retention in care rates at 6 and 12 months among young adults (15–24 years) (World Health Organization, Citation2011), but there is a dearth of information on retention among adolescents (10–19 years) due to the challenges of accessing data and inherent ethical concerns among this age group (Murray et al., Citation2017). The current paper reports on the retention in care rate and the factors associated among adolescents (10–19 years) receiving ART in the Ehlanzeni district of South Africa based on routine clinical electronic data.
Methods
Study design and participants
We conducted a retrospective cohort analysis of ALHIV (10–19 years) registered to receive ART from 136 clinics in the Ehlanzeni district between September 2002 and October 2017. A total of 16,108 adolescents met our inclusion criteria. Anonymised individual patient demographic (i.e., Gender and age), clinical and treatment outcome (viral load results after 3 months of ART initiation) data were extracted from electronic medical records (Tier.net). The current analysis provide a baseline to the larger study that aims to assess the effects of psychosocial support on adherence, treatment outcomes (viral suppression) and retention in care over 2 years for adolescents on ART.
Data source
The electronic ART database (Tier.net) developed by the University of Cape Town’s Centre for Infectious Disease Epidemiology and Research, is used by the South African health facilities to store patients’ routine clinical records electronically, and specifically for monitoring and management of ART patients.
Data collection
Anonymised patient data from 136 healthcare facilities were extracted from Tier.net in an excel format and subsequently imported into STATA statistical software. We searched for the relevant information from the Tier.net platform. Where information was missing, we accessed the patient’s folder to confirm the availability of the required information. The intensive data collection approach employed enabled the extraction of participants’ records from all included facilities where they may have received care, including undocumented silent transfers to a new facility.
The primary outcome was “retention in ART” at months 6, 12, 18 and 24 post HIV diagnosis and receiving a package of treatment, care and support services. The predictor variables were age, gender, method of entry into ART programme at the health facility, being on ART during pregnancy, age at ART initiation, duration on ART, initiated on Isoniazid Preventive Therapy (IPT), TB history, ART regimen, CD4 count at baseline and last ART visit, WHO stage at initiation, and same day ART initiation.
Analysis
Data were imported to STATA statistical software version 16.0 (STATA Corporation, College Station, Texas, U.S.A.) for analyses. Descriptive statistics were used to characterise the demographic and clinical profile of adolescents at baseline and/or specific time points after ART initiation. Comparisons between retention in care at months 6, 12, 18 and 24 and clinical parameters among ALHIV were measured using chi-square tests for proportions (replaced by Fisher’s exact test for sparse data), and Cox regression analysis adjusted for potential confounders and interactions. The Cox proportional hazard model employed a backward stepwise analysis, where we included all candidate variables in the initial model. At each step, the variable that is the least significant was removed; until no non-significant variables remained. The significance level was set at 95% at which variables can be removed from the model.
Survival analysis was assessed with “died” and “lost to follow-up” (LTFU) as the outcomes of interest, transferred out patients were treated as intention to treat (censored). We did a comparative survival analysis for the age and sex of the study participants using Kaplan-Meier survival descriptor. We reported the hazard ratios and p-values. An ALHIV was considered LTFU if no contact with healthcare provider was registered 90 days after their last facility ART visit. The patient record is then updated on Tier.net as LTFU and the date record was updated given as LTFU date. Therefore, by using the intention-to-treat population in this study, the retention in care definition was the proportion of HIV-infected adolescents alive and on ART at months 6, 12, 18, and 24 in the study sample. Using bivariate and multivariate analyses, we determined factors influencing retention in care at months 6, 12, 18, and 24.
Results
shows the demographic characteristics and clinical history of 16,108 ALHIV enrolled in the ART programme in 136 facilities in Ehlanzeni district South Africa between October 2002 and October 2017. The median duration on ART was eight months (median was reported because the variable is not normally distributed). Retention in care rates at 6, 12, 18, and 24 months were 90.5%, 85.4%, 80.8% and 76.2%, respectively. shows the Kaplan-Meier survival estimate for retention in care among adolescents living with HIV in Ehlanzeni district Mpumalanga.
Figure 1. Kaplan-Meier survival estimates for retention among adolescent over 2 years period.
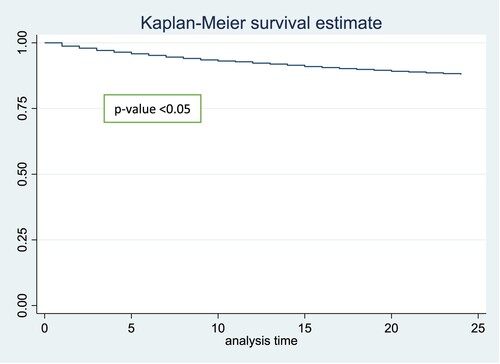
Table 1. Retention in care at 6, 12, 18 and 24 months by demographic characteristics and clinical outcomes of 16,108 adolescents on ART in Ehlanzeni district, South Africa, 2019.
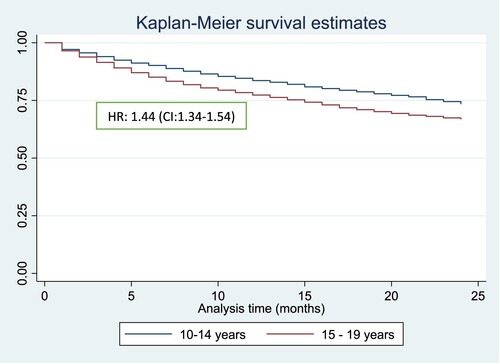
Compared to older adolescents (15–19 years), younger adolescents (10–14 years) were more likely to be retained in care at 6 months (91.6% vs 89.5%), 12 months (86.9% vs 83.9%), 18 months (82.6% vs 79.1%), and 24 months (78.1% vs 74.5%). shows the Kaplan-Meier survival estimates for retention among younger adolescent (10–14 years) compared to older adolescents (15–19 years) over 2 years’ period.
Figure 2. Kaplan-Meier survival estimates for retention among younger adolescent (10-14 years) compared to older adolescents (15-19 years) over 2 years period.
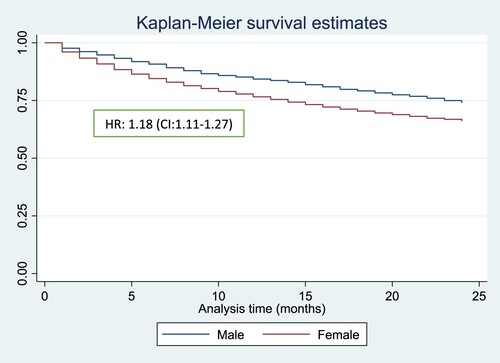
In terms of gender comparison males were more likely to be retained in care compared to females at 6 months (92.1% vs 89.0%), 12 months (87.2% vs 83.7%), 18 months (83.0% vs 78.9%), and 24 months (78.8% vs 73.9%). shows the Kaplan-Meier survival estimate for retention in care among adolescent males compared to females over 2-years’ period.
Figure 3. Kaplan-Meier survival estimates for retention among adolescent males compared to females over 2 years period.
Most (70.2%) of the adolescents attended the ART programme in the clinic they were initiated as new patients as opposed to transferred in from another clinic. Adolescents with previous ART experience were more likely to remain in care compared to ART naïve adolescents at 6 months (99.1% vs 86.4%), 12 months (98.1% vs 80.0%), 18 months (96.4% vs 74.2%), and 24 months (94.4% vs 68.5%; p = 0.000).
Amongst the female adolescents, 6.5% were reported pregnant at the time of enrolling into ART. Compared to pregnant adolescent girls, non-pregnant adolescents are more likely to remain in care at 6 months (90.8% vs 64.9%), 12 months (86.3% vs 50.9%), 18 months (81.7% vs 44.0%), and 24 months (77.2% vs 35.5%; p = 0.000).
Most (67.1%) of the adolescents were initiated on ART between 0 and 9 years. Compared to adolescents who initiated on ART at 10–14 years and 15–19 years, adolescents who initiated on ART at age 0–9 years are more likely to be retained in care at 6 months (92.8% vs 90.3% vs 72.7%), 12 months (88.5% vs 85.4% vs 60.9%), 18 months (84.5% vs 80.6% vs 53.3%), and 24 months (80.7% vs 75.4% vs 44.3%; p = 0.000).
Adolescents with a history of TB were less likely to be retained in care at 6 months (66.9% vs 93.6%), 12 months (60.3% vs 90.3%), 18 months (54.8% vs 87.4%), and 24 months (49.4% vs 84.0%; p = 0.000).
Compared to adolescents with CD4 count >200 at baseline, adolescents with CD4 count <200 at baseline were less likely to remain in care at 6 months (88.3% vs 91.6%); 12 months (82.8% vs 85.9%); 18 months (77.1% vs 81.3%); and 24 months (71.3% vs 77.1%; p = 0.000). Similarly, adolescents with CD4 count >200 at last visit were more likely to remain in care at 6 months (94.9% vs 84.1%); 12 months (90.9% vs 77.9%); 18 months (86.8% vs 72.3%); and 24 months (77.1% vs 71.3%; p = 0.000).
Nearly half (45.7%) of the adolescents were initiated on ART at WHO stage 1. Compared to adolescents with WHO stage 2, 3, and 4, adolescents with WHO stage 1 were less likely to retain in care at 6, 12, 18 and 24 months (p = 0.000). Similarly, adolescents with WHO stage 4 were more likely to remain in care at 18 and 24 months (p = 0.000).
Only 12.3% of the adolescents were on second line regimen. Adolescents on second-line regimen were more likely to be retained in ART care at 6 months (99.1% vs 89.3%); 12 months (98.4% vs 83.5%); 18 months (97.8% vs 78.4%); and 24 months (92.1% vs 58.4%).
More than two-third (69.2%) of the adolescents achieved a viral suppression of <1000 RNA copies/mL. Adolescents with viral load <1000 RNA copies/mL were more likely to remain in care at 6 months (99.4% vs 95.3%); 12 months (96.5% vs 91.8%); 18 months (92.9% vs 87.8%); and 24 months (88.6% vs 83.4%).
Factors associated with retention in care among adolescent living with HIV
shows the Cox proportional hazard analysis to understand risk factors for retention in care. After controlling for the effect of cofounders, the risk of dropping out of ART care increased for female adolescents (aHR = 1.28, 95% CI 1.10-1.49); new naive ART adolescents (aHR = 1.83, 95% CI 1.48-2.27); initiated on ART during pregnancy (aHR = 2.72, 95% CI 1.99-3.69); had a history of TB (aHR = 1.71, 95% CI 1.10-2.65); age at ART start 10–14 years (aHR = 2.45, 95% CI 1.96-3.05), and 15–19 years (aHR = 9.67, 95% CI 7.25-12.89).
Table 2. Cox proportional hazard analysis of factors associated with retention in care over 24 months among adolescents on ART in Ehlanzeni district, South Africa (N = 16,108).
Conversely, the risk of ALHIV dropping out of ART care decreased for adolescents with CD4 count >200 at baseline (aHR = 0.94, 95% CI 0.79-1.12) and CD4 count >200 at last visit (aHR = 0.66, 95% CI 0.54-0.80); on second-line regimen (aHR = 0.38, 95% CI 0.29-0.50); and being virally suppressed (viral load <1000 RNA copies/mL) (aHR = 0.30, 95% CI 0.26-0.35) respectively. There was no significant statistical relationship between retention in care and age; initiating on IPT; and same-day ART initiation.
Discussion
In this paper we report on the retention in care rate over a two-year period and its associated factors among ALHIV (10–19 years) receiving ART in the Ehlanzeni district of South Africa. Although the retention in care of ALHIV reported in this study over a two-year period falls short of the USAID 95-95-95 for 2030 target, there is hope that this retention in care rates can improve if urgent interventions and resources are directed to this vulnerable age group. In our study, the median duration on ART was 8 months. ALHIV in Ehlanzeni achieved the UNAIDS’ 90-90-90 target for 2020. However, the retention in care at 6 months declined sharply when observed at 12 months from 90% to 85%. Another study conducted in the Cape Metropole, South Africa found even lower retention in care at 4, 12 and 24 months as 68.6%, 50.5% and 36.4%, respectively (Van Wyk et al., Citation2020). A study on mental health of ALHIV (13-19 years) accessing treatment and care in Johannesburg health facilities found that being HIV is a predisposing factor to developing mental health challenges, which in turn negatively impacts on retention in care (Woollett, Cluver, Bandeira, & Brahmbhatt, Citation2017). Therefore, interventions that improve the mental health of ALHIV should be integrated in the HIV care and treatment programmes (Okonji et al., Citation2020). Furthermore, a recent qualitative study found that ALHIV drop out of care when they do not understand the reason for daily medication intake as a result of not being disclosed to (Lanyon et al., Citation2020).
Our findings show that male ALHIV were more likely to be retained in ART care compared to females. Associations between gender and retention in care among adolescents are conflicting. While some studies report that attrition rates among males are higher compared to females (Kusemererwa et al., Citation2021; Mutasa-Apollo et al., Citation2014), the opposite association were observed in a study in the Cape Metropole in South Africa (Van Wyk et al., Citation2020), which is consistent with our study findings. There is growing qualitative evidence suggesting that men's disinclination to engage in HIV care is linked to masculinity – set of local beliefs and practices that capture what it means in a particular context to be a man (Chikovore et al., Citation2016; Mukumbang, Citation2021; Nyamhanga, Muhondwa, & Shayo, Citation2013; Skovdal et al., Citation2011). In the Cape Metropole study nearly half of the female adolescents initiated on ART were pregnant, which may account for higher dropout among females compared to males. It is well documented in the literature that adolescent pregnant women are more likely to be lost-to-follow-up from ART care after giving birth (Matyanga et al., Citation2016; Nuwagaba-Biribonwoha et al., Citation2018). The syndemic of early motherhood and HIV increases the vulnerability of these adolescent mothers to disengaging from HIV care (Toska, Laurenzi, Roberts, Cluver, & Sherr, Citation2020).
To address pre-ART lost to follow-up, the NDoH implemented same-day initiation (SDI) – ART initiation on the same day of HIV diagnosis. While there is evidence suggesting that same-day ART initiation improves clinical outcomes including viral load suppression and retention in care at 12 months after ART initiation (Ford et al., Citation2018), a recent systematic review showed that same-day ART initiation is a risk factor for retention in care (Knettel et al., Citation2018). In this study, we found no significant relationship in retention in care among adolescents initiated on ART on the same day of HIV diagnosis compared to those who did not initiate on the same-day of receiving their HIV diagnosis. Same day initiation is influenced by the acceptability by adolescents (Lilian et al., Citation2020); and the absence of clinical symptoms of TB and meningitis (Ford et al., Citation2018; Lilian et al., Citation2020). Structural factors (e.g., Overcrowded clinics), social factors (e.g., Perceived stigma) and psychological factors (e.g., Poor ART readiness) have been found to increase the risk of poor retention in care among people initiating ART on the same day (Pry et al., Citation2020). Adolescent and youth staff training and implementation of adolescent and youth-friendly services have been shown to facilitate engagement in care among adolescent and youth populations (Okonji et al., Citation2020; Ruria et al., Citation2017).
Our study found higher retention in care among adolescents with a CD4 count >200 at baseline and at last visit. Our finding is consistent with another study that found higher risk to lost to follow-up among adolescents with low CD4 count (Matyanga et al., Citation2016). Our findings revealed that adolescents with suppressed viral load were less likely to drop out of care compared to those who did not achieve viral load suppression. This finding is consistent with a study that found direct correlation between perceived improved health outcomes with retention in care (Van Wyk et al., Citation2020). These adolescents are likely to remain in care because they are motivated by their health status and by the association between treatment and health outcomes (Bernays, Paparini, Seeley, & Rhodes, Citation2017; Van Wyk et al., Citation2020).
Complex medications i.e., Increased dosing (twice daily) and medications with adverse side effects are risk factors for adherence and subsequently retention in care (Holtzman, Brady & Yehia, Citation2015). Our study found higher retention in care among adolescents on second-line regimen compared to those on first line regimen. Greater emphasis on monitoring and follow up of patients who have been switched to second-line treatment requires greater attention and follow-up to remain in care.
Our study also found that the risk of dying or being lost-to-follow-up increased among adolescents who started ART between the ages of 10 and 19 years compared to 0 and 9 years. This is because older adolescents initiate on ART at a stage of advanced immunodeficiency (Enane et al., Citation2018; Shroufi et al., Citation2013). This finding is consistent with that of another study that found that older adolescents (15–19 years) were more likely to initiate late (Maskew et al., Citation2019). In addition, evidence suggest that significant amount of older adolescents drop out of care as they transition from adolescent ART care to adult ART care (Meloni et al., Citation2020).
Similarly, the risk of ALHIV dying or becoming lost to follow-up increased for adolescents newly initiated on ART compared to those previously initiated on ART. Another study showed that patients newly initiated on ART were more likely to require additional retention in care support compared to patients previously initiated on ART (Brown et al., Citation2016). The retention of adolescents newly diagnosed with HIV on ART care requires that the adolescent is mentally and clinically prepared and are ready to initiate on ART (Ford et al., Citation2018; Lilian et al., Citation2020).
Although TB manifestations among HIV positive children are more severe and progression to death is more rapid than in HIV-negative children (Jacobs et al., Citation2020; Palme, Gudetta, Bruchfeld, Muhe, & Giesecke, Citation2002), early detection of TB infection and disease significantly reduces mortality in children and ALHIV (Vonasek et al., Citation2021). We found that ALHIV who were diagnosed with TB were more likely to die or become lost-to-follow-up compared to ALHIV without TB disease. This result is consistent with a systematic review that observed a higher case fatality rate among children with HIV receiving treatment for TB compared to those without HIV (Jenkins et al., Citation2017).
Study limitations
This study has a number of limitations. Firstly, as is the case for all retrospective cohort studies, it is subject to other risk or confounding factors that may be present but were not measured such as household income status, head of household, type of social support and psychosocial wellbeing. Secondly, adolescents described as lost-to-follow up in Tier.net may be under-reported due to unrecorded mortality and silent transfers. Silent transfers were treated as still in care as they do not have outcome date and ART outcome as died or lost to follow-up.
Conclusion
Retention in care among adolescents on ART over two-year period was considerably lower than the UNAIDS 2030 target of 95%. Of particular concern for intervention is the lower rates of retention in care among females and pregnant adolescents and starting ART between the ages of 10 and 19 years. Family or caregivers and peer support groups centred interventions designed to promote early initiation and retention in care through early case identification, quality clinical and psychosocial support, as they transition from adolescent to adult ART care are needed.
Declarations
Ethics approval and consent to participate
Ethics clearance was obtained from the University of the Western Cape Biomedical Research Ethics committee (BM19/1/8) and the National Health Research Ethics committee to use the electronic medical dataset (Tier.net) (MP_202102_006). We adhered to the 1964 declaration of Helsinki guidelines. According to the declaration, research that involves human subjects amongst others must keep with the following (1) strive to protect life, health, privacy, and the dignity of the research participants, (2) employ greater care to protect the participants from harm and (3) conduct the research because the importance of the research purpose, outweighs the risk that might be attributed to the study either at present or in the future (18th WMA General Assembly, Helsinki, 2001).
Data extraction excluded adolescent’s unique identifiers such as name, surname, patient folder number and identity number to ensure anonymity.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due it belonging to the South African National Department of Health, but are available from the corresponding author on reasonable request.
Authors’ contributions
EFO and BVW designed the study. EFO analyzed the data and developed the manuscript with editorial and content input from BVW and FCM. All authors read and approved the final manuscript.
Authors’ information
This paper is a component of his PhD programme that aims to make a case for a psychosocial support intervention specifically designed to improve adherence and retention amongst adolescents living with HIV and AIDS.
Acknowledgements
We acknowledge the Mpumalanga Department of Health and Right to care for granting us permission to use the routine programme data for this analysis.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ajayi, A. I., Otukpa, E. O., Mwoka, M., Kabiru, C. W., & Ushie, B. A. (2021). Adolescent sexual and reproductive health research in sub-Saharan Africa: A scoping review of substantive focus, research volume, geographic distribution and Africa-led inquiry. BMJ Global Health, 6(2), e004129. https://doi.org/10.1136/bmjgh-2020-004129
- Bernays, S., Paparini, S., Seeley, J., & Rhodes, T. (2017). Not taking it will just be like a Sin: Young people living with HIV and the stigmatization of less-than-perfect adherence to antiretroviral therapy. Medical Anthropology: Cross Cultural Studies in Health and Illness, 36(5), 485–499. https://doi.org/10.1080/01459740.2017.1306856
- Brown, L. B., Havlir, D. V., Ayieko, J., Mwangwa, F., Owaraganise, A., Kwarisiima, D., Jain, V., Ruel, T., Clark, T., Chamie, G., Bukusi, E. A., Cohen, C. R., Kamya, M. R., Petersen, M. L., & Charlebois, E. D. (2016). High levels of retention in care with streamlined care and universal test and treat in East Africa. Aids (london, England), 30(18), 2855–2864. https://doi.org/10.1097/QAD.0000000000001250
- Busza, J., Dauya, E., Bandason, T., Mujuru, H., & Ferrand, R. A. (2014). I don’t want financial support but verbal support. How do caregivers manage children ‘ s access to and retention in HIV care in urban Zimbabwe ? Journal of the International AIDS Society, 17(1), 1–9. https://doi.org/10.7448/IAS.17.1.18839
- Chikovore, J., Gillespie, N., McGrath, N., Orne-Gliemann, J., Zuma, T., & Group, O. B. of the A. 12249 T. S. (2016). Men, masculinity, and engagement with treatment as prevention in KwaZulu-Natal, South Africa. AIDS Care, 28(sup3), 74–82. https://doi.org/10.1080/09540121.2016.1178953
- Enane, L. A., Davies, M. A., Leroy, V., Edmonds, A., Apondi, E., Adedimeji, A., & Vreeman, R. C. (2018). Traversing the cascade: Urgent research priorities for implementing the ‘treat all’ strategy for children and adolescents living with HIV in sub-Saharan Africa. Journal of Virus Eradication, 4(Supplement 2), 40–46. https://doi.org/10.1016/S2055-6640(20)30344-7
- Ford, N., Migone, C., Calmy, A., Kerschberger, B., Kanters, S., Nsanzimana, S., Mills, E. J., Meintjes, G., Vitoria, M., Doherty, M., & Shubber, Z. (2018). Benefits and risks of rapid initiation of antiretroviral therapy. AIDS (London, England), 32(1), 17–23. https://doi.org/10.1097/QAD.0000000000001671
- Gittings, L., Toska, C., Hodes, R., Cluver, L., Zungu, N., Govender, K., Chademana, K. E., & Gutiérrez, V. (2016). Resourcing resilience: The case for social protection for HIV-positive children on antiretroviral treatment in Eastern and Southern Africa. RIATT-ESA Report.
- Holtzman, C. W., Brady, K. A., & Yehia, B. R. (2015). Retention in care and medication adherence: Current challenges to antiretroviral therapy success. Drugs, 75(5), 445–454. https://doi.org/10.1016/j.molmed.2014.11.008.Mitochondria
- Hudelson, C., & Cluver, L. D. (2015). Factors associated with adherence to antiretroviral therapy among adolescents living with HIV/AIDS in low- and middle-income countries: A systematic review. AIDS Care, 27(7), 805–816. https://doi.org/10.1080/09540121.2015.1011073
- Jacobs, T. G., Svensson, E. M., Musiime, V., Rojo, P., Dooley, K. E., McIlleron, H., Aarnoutse, R. E., Burger, D. M., Turkova, A., Colbers, A., Abrams, E., Archary, M., Belew, Y., Best, B., Burger, D., Burry, J., Capparelli, E., Carpenter, D., Casas, E., … Wolf, H. (2020). Pharmacokinetics of antiretroviral and tuberculosis drugs in children with HIV/TB co-infection: A systematic review. Journal of Antimicrobial Chemotherapy, 75(12), 3433–3457. https://doi.org/10.1093/jac/dkaa328
- Jenkins, H. E., Yuen, C. M., Rodriguez, C. A., Nathavitharana, R. R., McLaughlin, M. M., Donald, P., Marais, B. J., & Becerra, M. C. (2017). Mortality in children diagnosed with tuberculosis: A systematic review and meta-analysis. The Lancet Infectious Diseases, 17(3), 285–295. https://doi.org/10.1016/S1473-3099(16)30474-1
- Knettel, B. A., Cichowitz, C., Ngocho, J. S., Knippler, E. T., Chumba, L. N., Mmbaga, B. T., & Watt, M. H. (2018). Retention in HIV care during pregnancy and the postpartum period in the option B+ Era: Systematic review and meta-analysis of studies in Africa. JAIDS Journal of Acquired Immune Deficiency Syndromes, 77(5), 427–438. https://doi.org/10.1097/QAI.0000000000001616
- Kusemererwa, S., Akena, D., Nakanjako, D., Kigozi, J., Nanyunja, R., Nanfuka, M., Kizito, B., Okello, J. M., Marotta, C., & Sewankambo, N. K. (2021). Strategies for retention of heterosexual men in HIV care in sub-Saharan Africa: A systematic review. PLoS ONE, 16(2 February), 1–13. https://doi.org/10.1371/journal.pone.0246471
- Lanyon, C., Seeley, J., Namukwaya, S., Musiime, V., Paparini, S., Nakyambadde, H., Matama, C., Turkova, A., & Bernays, S. (2020). Because we all have to grow up”: supporting adolescents in Uganda to develop core competencies to transition towards managing their HIV more independently. Journal of the International AIDS Society, 23(S5), 40–46. https://doi.org/10.1002/jia2.25552
- Lilian, R. R., Rees, K., Mcintyre, J. A., Struthers, H. E., & Petersid, R. P. H. (2020). Same-day antiretroviral therapy initiation for HIV-infected adults in South Africa: Analysis of routine data. 15(1), e0227572. https://doi.org/10.1371/journal.pone.0227572
- MacPherson, P., Munthali, C., Ferguson, J., Armstrong, A., Kranzer, K., Ferrand, R. A., & Ross, D. A. (2015). Service delivery interventions to improve adolescents’ linkage, retention and adherence to antiretroviral therapy and HIV care. Tropical Medicine & International Health, 20(8), 1015–1032. https://doi.org/10.1111/tmi.12517
- Mark, D., Armstrong, A., Andrade, C., Penazzato, M., Hatane, L., Taing, L., Runciman, T., & Ferguson, J. (2017). HIV treatment and care services for adolescents: A situational analysis of 218 facilities in 23 sub-Saharan African countries. Journal of the International AIDS Society, 20, 24–33. https://doi.org/10.7448/IAS.20.4.21591.
- Maskew, M., Bor, J., MacLeod, W., Carmona, S., Sherman, G. G., & Fox, M. P. (2019). Adolescent HIV treatment in South Africa’s national HIV programme: A retrospective cohort study. The Lancet HIV, 6(11), e760–e768. https://doi.org/10.1016/S2352-3018(19)30234-6
- Matyanga, C. M. J., Takarinda, K. C., Owiti, P., Mutasa-Apollo, T., Mugurungi, O., Buruwe, L., & Reid, A. J. (2016). Outcomes of antiretroviral therapy among younger versus older adolescents and adults in an urban clinic, Zimbabwe. Public Health in Action, 6(2), 97–104. https://doi.org/10.5588/pha.15.0077
- Meloni, S. T., Agaba, P., Chang, C. A., Yiltok, E., Oguche, S., Ejeliogu, E., Agbaji, O., Okonkwo, P., Larson, B. A., & Kanki, P. J. (2020). Longitudinal evaluation of adherence, retention, and transition patterns of adolescents living with HIV in Nigeria. PLOS ONE, 15(7), e0236801. https://doi.org/10.1371/journal.pone.0236801
- Mukumbang, F. C. (2021). Leaving no man behind: How differentiated service delivery models increase men’s engagement in HIV care. International Journal of Health Policy and Management, 10(3), 129. https://doi.org/10.34172/IJHPM.2020.32
- Murray, K. R., Dulli, L. S., Ridgeway, K., Dal Santo, L., De Mora, D. D., Olsen, P., Darrow de Mora, D., Silverstein, H., Sued, O., & McCarraher, D. R. (2017). Improving retention in HIV care among adolescents and adults in low- and middle-income countries: A systematic review of the literature. PLoS ONE, 12(9). https://doi.org/10.1371/journal.pone.0184879
- Mutasa-Apollo, T., Shiraishi, R. W., Takarinda, K. C., Dzangare, J., Mugurungi, O., Murungu, J., Abdul-Quader, A., Fox, M. P., & Woodfill, C. J. I. (2014). Patient retention, clinical outcomes and attrition-associated factors of HIV-infected patients enrolled in Zimbabwe’s national antiretroviral therapy programme, 2007-2010. PLoS ONE, 9(1), 1–11. https://doi.org/10.1371/journal.pone.0086305.
- Nachega, J. B., Mills, E. J., & Schechter, M. (2010). Antiretroviral therapy adherence and retention in care in middle-income and low-income countries: Current status of knowledge and research priorities. Current Opinion in HIV and AIDS, 70–77. https://doi.org/10.1097/COH.0b013e328333ad61.
- Naidoo, K., Munsami, A., & Archary, M. (2015). Adolescent antiretroviral management: Understanding the complexity of non-adherence. South African Medical Journal, 105(11), 953. https://doi.org/10.7196/SAMJ.2015.v105i11.10150
- Nuwagaba-Biribonwoha, H., Kiragga, A. N., Yiannoutsos, C. T., Musick, B. S., Wools-Kaloustian, K. K., Ayaya, S., Wolf, H., Lugina, E., Ssali, J., Abrams, E. J., & Elul, B. (2018). Adolescent pregnancy at antiretroviral therapy (ART) initiation: A critical barrier to retention on ART. Journal of the International AIDS Society, 21(9), e25178. https://doi.org/10.1002/jia2.25178
- Nyamhanga, T. M., Muhondwa, E. P. Y., & Shayo, R. (2013). Masculine attitudes of superiority deter men from accessing antiretroviral therapy in Dar es Salaam, Tanzania. Global Health Action, 6(1), 21812. https://doi.org/10.3402/gha.v6i0.21812
- Okonji, E. F., Mukumbang, F. C., Orth, Z., Vickerman-Delport, S. A., & Wyk, B. V. (2020). Psychosocial support interventions for improved adherence and retention in ART care for young people living with HIV (10–24 years): a scoping review. BMC Public Health 2020 20:1, 20(1), 1–11. https://doi.org/10.1186/S12889-020-09717-Y
- Palme, I. B., Gudetta, B., Bruchfeld, J., Muhe, L., & Giesecke, J. (2002). Impact of human immunodeficiency virus 1 infection on clinical presentation, treatment outcome and survival in a cohort of Ethiopian children with tuberculosis. The Pediatric Infectious Disease Journal, 21(11), 1053–1061. https://doi.org/10.1097/00006454-200211000-00016
- Pry, J., Chipungu, J., Smith, H. J., Bolton Moore, C., Mutale, J., Duran-Frigola, M., Duran-Frigola, M., Savory, T., & Herce, M. E. (2020). Patient-reported reasons for declining same-day antiretroviral therapy initiation in routine HIV care settings in Lusaka, Zambia: Results from a mixed-effects regression analysis. Journal of the International AIDS Society, 23(7), e25560. https://doi.org/10.1002/JIA2.25560
- Ruria, E. C., Masaba, R., Kose, J., Woelk, G., Mwangi, E., Matu, L., Ng’eno, H., Bikeri, B., & Rakhmanina, N. (2017). Optimizing linkage to care and initiation and retention on treatment of adolescents with newly diagnosed HIV infection. Aids (london, England), 31(May), S253–S260. https://doi.org/10.1097/QAD.0000000000001538
- Shroufi, A., Gunguwo, H., Dixon, M., Nyathi, M., Ndebele, W., Saint-Sauveur, J. F., Taziwa, F., Ferreyra, C., Viñoles, M.-C., & Ferrand, R. A. (2013). HIV-infected adolescents in Southern Africa can achieve good treatment outcomes: Results from a retrospective cohort study. Aids (london, England), 27(12), 1971–1978. https://doi.org/10.1097/QAD.0b013e32836149ea
- Skovdal, M., Campbell, C., Madanhire, C., Mupambireyi, Z., Nyamukapa, C., & Gregson, S. (2011). Masculinity as a barrier to men’s use of HIV services in Zimbabwe. Globalization and Health, 7(1), 13. https://doi.org/10.1186/1744-8603-7-13
- Slogrove, A. L., Mahy, M., Armstrong, A., & Davies, M. A. (2017). Living and dying to be counted: What we know about the epidemiology of the global adolescent HIV epidemic. Journal of the International AIDS Society, 20(Suppl 3), 4–15. https://doi.org/10.7448/IAS.20.4.21520
- Toska, E., Laurenzi, C. A., Roberts, K. J., Cluver, L., & Sherr, L. (2020). Adolescent mothers affected by HIV and their children: A scoping review of evidence and experiences from sub-Saharan Africa. Global Public Health, 15(11), 1655–1673. https://doi.org/10.1080/17441692.2020.1775867/FORMAT/EPUB
- UNAIDS. (2014). UNAIDS issues new fast-track strategy to end AIDS by 2030. https://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_en.pdf
- Vonasek, B., Kay, A., Devezin, T., Bacha, J. M., Kazembe, P., Dhillon, D., Dlamini, S., Haq, H., Thahane, L., Simon, K., Matshaba, M., Sanders, J., Minde, M., Wanless, S., Nyasulu, P., & Mandalakas, A. (2021). Tuberculosis symptom screening for children and adolescents living with HIV in six high HIV / TB burden countries in Africa. Aids (london, England), 35, 73–79. https://doi.org/10.1097/QAD.0000000000002715
- Woollett, N., Cluver, L., Bandeira, M., & Brahmbhatt, H. (2017). Identifying risks for mental health problems in HIV positive adolescents accessing HIV treatment in Johannesburg. Journal of Child & Adolescent Mental Health, 0583(March), 1–17. https://doi.org/10.2989/17280583.2017.1283320
- World Health Organization. (2011). Retention in HIV programmes: Defining the challenges and identifying solutions. World Health Organization. https://doi.org/10.1016/j.trstmh.2010.01.007
- Wyk, B. V., Kriel, E., & Mukumbang, F. (2020). Retention in care for adolescents who were newly initiated on antiretroviral therapy in the Cape Metropole in South Africa. Southern African Journal of HIV Medicine, 21(1), 1–8. https://doi.org/10.4102/sajhivmed.v21i1.1077
