
ABSTRACT
Adolescent girls and young women (AGYW) engaging in sex-for-money transactions are at risk of HIV infection. A better understanding of the demographic, socio-economic factors and risks of HIV acquisition is required to guide appropriate public health interventions targeting young sex workers in South Africa. A cross-sectional survey of Female Sex Workers (FSWs), using a chain referral sampling method, was conducted across 12 sites in South Africa in 2019. Three thousand and five participants were enrolled and interviewed assessing demographic characteristics, sexual behaviour, substance use and HIV testing and treatment. Of 3005 women, 13.3% were ≤24 years old (young FSWs); of these, 60.0% entered sex work aged ≤19 years. Economic factors were the primary drivers of entry into sex work. HIV prevalence amongst young FSWs was 40.4%, with 12.4% recently infected. Younger FSWs were significantly less likely to know they were HIV positive (87.6% versus 92.1%), to report any ART exposure (75.2% versus 87.6%) and to be virally suppressed (58.1% versus 75.2%) compared to older FSWs. Our findings highlight that many FSWs enter sex work at a young age. It is essential to develop tailored services and interventions that improve access to HIV prevention and treatment services addressing specific needs.
Introduction
Adolescent girls and young women (AGYW) account for a disproportionately high number of new HIV infections (UNICEF, Citation2021). HIV prevalence for young women aged 15–24 years old remains two to three times higher than amongst their male peers (Simbayi etal., Citation2019; UNICEF, Citation2021). Aspects driving the HIV gender difference include age-disparate relationships, transactional sex and sex work, gender-based violence and high-risk behaviours such as early sexual debut, inconsistent condom use, multiple sexual partners, and socio-economic factors (poverty, level of education) (Dunkle etal., Citation2004; Jewkes etal., Citation2012; Li etal., Citation2014; Wilson etal., Citation1999).
Based on a sub-analysis of the South African Human Science Research Council (2017) report, as many as 35% of AGYW described engaging in intergenerational relationships (Simbayi etal., Citation2019). Evidence has shown that young women engage in such relationships for material gain, often driven by socio-economic factors (Kyegombe etal., Citation2020; Nguyen, Citation2017). These relationships are frequently predicated on power differentials underpinned by a patriarchal society (Chatterji etal., Citation2005; Hensen etal., Citationn.d.; Nguyen etal., Citation2019) which prevent women from negotiating safer sex practices, resulting in unplanned pregnancies. Unplanned pregnancies are a major barrier to completing secondary education (Becker etal., Citation2018) and impact on employment opportunities. Young women, who are less employable (Statistics South Africa [Stats SA], Citation2020), are thus driven towards engaging in further transactional relationships grounded in “survival sex”. For a subset of these women, sex work becomes a means to provide for both themselves and their families. Thus, the overlap between AGYW and sex work is established, and the risk of HIV acquisition increases substantively.
Studies from across South Africa have shown that HIV prevalence amongst sex workers (SWs) ranges from 40% to 90%, and that 30% to 40% are under 25 years of age – with an elevated HIV risk profile (UCSF etal., Citation2015; Coetzee etal., Citation2017a). This paper argues for the overlap between young women and sex work in order to inform program implementation to achieve better public health outcomes for this population. These associations have become increasingly important given the impact that the COVID-19 pandemic has had on schooling, access to healthcare and unemployment (Espi etal., Citation2021).
Evidence shows that the gaps in prevention among sub-populations most at risk of acquiring and transmitting HIV can sustain an epidemic (Formson & Hilhorst, Citation2016). Traditional approaches to HIV prevention and treatment have often assumed a one size fits all approach, ignoring subset key populations with differing transmission and acquisition dynamics (Formson & Hilhorst, Citation2016). Thus, understanding the association of youth and sex work is essential for epidemic control in countries such as South Africa, where the boundaries between transactional sex and sex work are often blurred. Additionally, there is a clear trajectory for young, uneducated and impoverished women who begin transacting in sex towards more informal and formal methods of sex work.
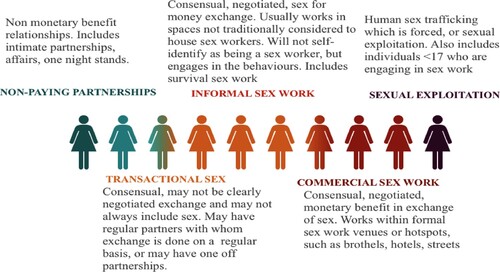
The literature highlights challenges to drawing a clear distinction between sex work and transactional sex, with multiple terms used to define each practice (Stats SA, Citation2020). This includes the practice of Ukuphanda in South Africa, which enables women to engage in sex for money exchanges within a social framework while allowing women to remain respected within the broader community (Stoebenau etal., Citation2016; Wojcicki, Citation2002). Evidence suggests that the frequency of such sex for money transactions has increased dramatically (Plan International and the African Child Policy Forum [ACPF], Citation2020). We propose that the behaviour of engaging in sex for money to survive is far more widespread than previously thought, and has transformed from minimal such sexual encounters into a form of “transactional sex work” which takes place on a regular basis. Through retaining one’s identity as a non-SW, women are better able to retain their identity as respectable women within their communities. Thus, we propose that sex work should be understood to function on a behavioural continuum (). Across this continuum, terms like sex work and transactional sex are used interchangeably to describe a set of behaviours which increase or decrease the risk profile of individuals and/or populations who engage in them, but who may not self-identify with the identity label.
Figure 1. Understanding the continuum of sex for money transactions: from transactional to commercial sex work behaviours.
While there are a number of interventions geared towards AGYW (Gibbs etal., Citation2020; Gichane etal., Citation2020; Saul etal., Citation2018; Scorgie etal., Citation2018) few exist which target extremely high risk AGYW who may not self-identify as engaging in sex work nor in transactional sex, but who are engaging in the behaviours associated with each. Within impoverished communities, sex and money are inextricably linked.
Understanding the overlap of young women and sex work is a vital step in developing an intervention package and a central tenet to epidemic control in South Africa. This is especially important within the context of highly targeted funding mechanisms which may inadvertently overlook high risk AGYW at risk of entering sex work (Pyett & Warr, Citation1997). This paper aims to describe the association between women entering sex work as AGYW, or as adults to highlight the gap in current interventions.
Methods
A cross-sectional national survey of FSWs, using a chain referral sampling method, was conducted across 12 randomly selected districts that housed sex work programs, from all nine provinces in South Africa, February–July 2019. A detailed description of the study methodology has been published (Milovanovic etal., Citation2021). The study analysed data for 3005 FSW participants: ≥18 years of age, actively engaged in the sale/transaction of sex for financial benefit at the time of the study, had sold/transacted in sex in the six months preceding the study and were cis-gender female.
After screening and signing of consent, participants completed a 40-minute survey assessing: demographics, HIV testing and treatment history, substance use, stigma, sexual behaviours, and exposure to violence. Participants underwent HIV testing and had blood draw for viral load testing, positives only. All data collection procedures were done in a private room to ensure participant confidentiality. Survey data were captured on a real-time basis, directly into tablets using the REDCap mobile phone application and the data was centrally collated using the REDCap management system (Harris etal., Citation2009).
After completing data collection, each FSW was issued with three coupons with which to recruit other potential FSWs into the study. Participants were asked to distribute the coupons to randomly selected women they knew and who knew them, who like themselves sold sex in the same district. This continued until the sample size per site was achieved. Site-specific information was used to adapt recruitment in line with site dynamics and staff and participant safety (Milovanovic etal., Citation2021).
Measures
Socio-demographic characteristics were scored as single items. Questions included: home language, place of birth and immigration status. Participants were asked their age and dichotomized into two groups based on Global Fund categorization (The Global Fund, Citation2020): younger SWs were defined as those currently ≤24 years old, and older women (>24 years). This allowed us to understand the varying risk profiles between age at entry into sex work and current age, with the 24-year cut-off being the standard for defining young women. We also asked questions around the participant’s highest level of education achieved (secondary complete or incomplete), food security, and pregnancy information.
To assess sexual behaviour and sex work, questions included: age of sexual debut, age of entry into sex work, and circumstances around entry into sex work. Participants were asked whether their family knew that they sold sex, usual place where they slept, venue where sex was sold, and number of clients and daily earning. This allowed us to calculate the earning potential per client. Additional variables explored alcohol use to help sell sex and condom use over the past year (consistently or inconsistently).
Internal stigma was assessed using an adaptation of the People Living with HIV Stigma Index (NAPAW SA, Citation2012) including eight questions (Milovanovic etal., Citation2021). Higher scores indicated more reported internalized stigma. External stigma was evaluated by asking if participants had been verbally, physically or sexually harassed, threatened or discriminated against by healthcare workers or police due to their being a sex worker.
Sexual violence was assessed using the adapted World Health Organization (Citation2002) violence against women questionnaire. The questionnaire was modified to ask about violence specific to various perpetrator types. A new variable was created that grouped all perpetrator types indicating either “none” or “some” sexual violence. Additionally, participants were also asked whether they had ever been forced into sex by more than one man at the same time (gang rape).
Treatment cascade and health outcomes were assessed by asking questions around previous HIV testing history and known HIV status (newly diagnosed or a known positive). HIV status was based on study confirmed testing and blood collected for assessment of viral suppression (VL < 1000 cp/ml). An STI screening questionnaire was implemented which also explored whether or not participants received treatment for STI symptoms. Self-report ART exposure including PEP/PrEP/PMTCT was assessed using a guided chart. All participants were referred for further care as required.
Statistical analysis
Data were analysed and results were presented overall and stratified by age groups: ≤24 years (young women), and those currently aged >24 years. Frequencies and percentages were determined for categorical variables. Medians and interquartile ranges (IQR) were determined for continuous measures overall and by age group.
Categorical variables were compared by the Chi-square test whereas medians between the two groups were compared non-parametrically using the Kruskal–Wallis Test. All statistical analyses assumed a 5% level of significance and were run using SAS Enterprise Guide 7.15, SAS Institute Inc., Cary, NC, USA.
Ethical considerations
All participants received oral and written information regarding the conduct of the study, voluntary participation and the risks and benefits, in the appropriate language of choice. Ethics approval was provided by the Human Research Ethics Committee (HREC) (Medical) of the University of the Witwatersrand (Ref number: 180809).
Results
Demographic characteristics
The study enrolled 3005 participants of which 399 (13.3%) were 24 years old or younger. presents the demographic characteristics of the two groups.
Table 1. Demographic characteristics by age-group.
Younger SWs were more likely to be local (295/399, 73.9% vs. 1646/2606, 63.2%, p < .0001) and less likely to be internal migrants (55/399, 13.8% vs. 496/2606, 19.0%, p = 0.0116) or external migrants (49/399, 12.3% vs. 464/2606, 17.8%, p < 0.0063) compared with older women. Younger SWs were also significantly more likely to have been pregnant between the ages 15–19 years compared to older women (202/268, 75.4% vs. 1208/2298, 52.6%, p < .0001). Amongst those who had children, younger SWs were less likely to have two (63/398, 15.8% vs. 777/2599, 29.9%, p < 0.0001) or more than two children (10/398, 2.5% vs. 825/2599, 31.7%, p < 0.0001) compared to their older counterparts.
Sex work-related characteristics
presents the sex-related characteristics and behaviours by age group. Younger SWs were more likely to have had an earlier sexual debut with significantly more young women reporting first coitus before 14 years of age (93/391, 23.8% vs. 457/2528, 18.1%, p = 0.0072) compared to older women. Among the younger group, 60.0% (235/392) entered sex work aged ≤19 years compared to 16.8% (435/2586) of older women – amongst whom almost half entered into sex work before the age of 25 (1151/2586, 44.5%). Younger women were less likely to report being homeless or sleeping in abandoned buildings (55/398, 13.8% vs. 553/2604, 21.2%, p = 0.0006) but more likely to report sleeping in sex work venues (141/398, 35.4% vs. 768/2604, 29.5%, p = 0.0164) compared with their older counterparts.
Table 2. Sex-related characteristics and behaviours by age-group.
Younger women were more likely to report selling sex in a tavern/shebeen (172/399, 43.1% vs. 919/2606, 35.3%, p = 0.0024). Across both groups, there was no significant difference in the median number of clients in the last working day and their earning potential. Younger women reported drinking more alcohol to help them do sex work compared to their older counterparts (144/398, 36.2% vs. 707/2594, 27.3%, p = 0.0002). There were no significant differences by age category for inconsistency in condom use over the past year (20/393, 5.1% vs. 91/2571, 3.5%, p = 0.1318). The median internalized and externalized stigma was not significantly different between younger and older women.
Across both groups, women reported being gang raped (95/395, 23.9% younger and 605/2597, 23.3% older women) and experiencing some sexual violence (252/399, 63.2% younger and 1609/2592, 62.1% older women) – with no significant difference by age categorization.
Treatment cascade and health outcomes
Younger women were less likely to report receiving treatment for STI symptoms in the past six months (110/177, 62.1% vs. 968/1213 79.8%, p < 0.0001) and less likely to be HIV infected (161/399, 40.4% vs. 1701/2600, 65.4%, p < 0.0001) compared to their older counterparts (). They were more likely to be newly diagnosed HIV positive (20/161, 12.4% vs. 134/1701, 7.9%; p = 0.0454), less likely to self-report ART exposure (121/161, 75.2% vs. 1490/1701, 87.6%, p = 0.0001) and less likely to be virally suppressed (61/105, 58.1% vs. 963/1280, 75.2%; p = 0.0001) compared to older women.
Table 3. Treatment cascade and health outcomes by age-group.
Discussion
The current study offers the unique opportunity to understand some of the characteristics of women who had begun selling sex at an early age. While sex work programs in South Africa had made exceptional headway (prior to the COVID-19 pandemic) in reaching the 90:90:90 targets (Jaffer etal., Citation2022; UNAIDS, Citation2014), current AGYW had poorer health outcomes. This highlights an important gap in South Africa’s key population programs which needs to be urgently addressed. At risk AGYW in South Africa, are unlikely to self-identify as engaging in any form of sex work (Ranganathan etal., Citation2017) and consequently, they are less likely to access the standard package of sex work-specific services. Therefore, targetted programs will need to be innovative when thinking about how best to identify youth engaging in sex work in order to provide additional support services, without creating greater stigma.
While we found that there was no major difference amongst the two age groups in internalized and externalized stigma, the impact of stigma continues to massively influence young women, especially those who are transacting or engaging in any method of formal or informal sex work (Ranganathan etal., Citation2017).
AGYW and their older counterparts reported equal levels of exposure to sexual violence, and lifetime exposure to gang rape. However, younger SWs are reporting high exposure to violence from a younger age and by implication are likely to experience greater levels of violence across their lifetime (Jewkes etal., Citation2021). Suggesting that while fewer young SWs were HIV positive in our sample, the higher prevalence of violence across their lifetimes (Coetzee etal., Citation2017b) would likely impact on the rate of seroconversion.
Our study reports that economic factors drive entry and retention in sex work. Economic factors, including not having enough to eat, needing to add to the family income, and needing to feed a child after dropping out of school are all reasons given for selling sex (Wilson etal., Citation1999). While younger SWs were less likely to have been pregnant, a higher proportion of them had been pregnant when compared to their same age adolescent counterparts in the general population (68% vs 12%, respectively) (National Department of Health etal., Citation2019).
Findings from a 2017 study suggested that adolescent girls and young women from impoverished backgrounds have an elevated risk of school drop-out (Jewkes etal., Citation2012) or to be withdrawn from school to aid in the financial sustainability of their families (Stoebenau etal., Citation2016). Girls are also more likely to miss a week of schooling every month due to menstruation (Gibbs etal., Citation2020). All of these factors increase the risk of incomplete high school, lowering the likelihood of employability and increasing the need to engage in sex for money transactions.
Given the continuum of sex work presented, women are able to recursively move along this continuum based upon their life circumstances, economic situation and needs. The sex work continuum is not predicated on age categories, and when compared to the general population, young women entering this continuum have a fundamentally different risk profile. While being a young woman is not contingent upon being a sex worker, it is frequently the case that SWs are either AGYW, or have entered into the sex work continuum during their youth. Through broadening our understanding of the overlap between these two population groups, we are better empowered to develop effective interventions, and to ensure we minimize the risk of a sub-population slipping through the gaps, especially as these may represent a high risk subset of AGYW. Some of these services may well overlap with those already provided through SW and AGYW programs. This creates opportunities for cost-sharing and learnings. Thus enabling us to develop effective and sustainable interventions for AGYW that ensure they are retained in school, avoiding unplanned pregnancies, improving job-readiness, proactively engaged in health seeking behaviours, and are empowered to make healthy sexual choices.
Limitations
There is limited, reliable data available in South Africa on mortality rates amongst SWs although we know that SWs are vulnerable to higher rates of violence than found in the general non-sex worker population. Mortality may be impacting the declines we see amongst the oldest age category. Due to ethical, time and financial constraints, FSWs under 18 years of age were not eligible for enrolment into the study, which may be impacting our estimates of the number of SWs in each age category. We do not include data from a matched sample of women drawn from the general population as a comparison.
Conclusion
By outlining the overlap between young women and sex work, this study provides further evidence of the urgent need to address the gap in current programing for AGYW and sex work to ensure no one is left behind. Using the national study data, we were able to retrospectively explore the continuum of vulnerability that AGYW experience, and outline the drivers of entry into sex work. Understanding these drivers, vulnerabilities and poor health outcomes is crucial to the development and implementation of evidence-driven interventions that should aim to increase HIV prevention and treatment services.
Acknowledgement
We would like to acknowledge all the study participants and the staff that ensured the successful conduct of this multi-site study. MM facilitated the design, and oversaw the implementation and scientific aspects of the study and led the writing of the paper; RJ assisted with data analysis and interpretation and manuscript preparation and review; MM assisted with study oversight and manuscript preparation; KD assisted with data analysis and interpretation and manuscript preparation and review; KH monitored and analyse the data and contributed to writing; LV technical input and manuscript review; NS technical input and manuscript review; MJ oversaw the clinical aspects of the study and provided technical review; VM assisted with study oversight and manuscript preparation; FA provided technical and scientific oversight and manuscript review; KO monitored and analyse the data and contributed to writing; GG provided technical and scientific oversight and manuscript review; JC, oversaw the design, implementation and scientific aspects of the study and led the writing of the paper. All co-authors have provided their consent for publication
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Becker, M., Bhattacharjee, P., Blanchard, J., Cheuk, E., Isac, S., Musyoki, H., Gichangi, P., Aral, S., Pickles, M., Sandstrom, P., Ma, H., & Mishra, S. (2018). Vulnerabilities at first sex and their association with lifetime gender-based violence and HIV prevalence among adolescent girls and young women engaged in sex work, transactional sex, and casual sex in Kenya. Journal of Acquired Immune Deficiency Syndrome, 79(3), 296–304. https://doi.org/10.1097/QAI.0000000000001826
- Chatterji, M., Murray, N., London, D., & Anglewiez, P. (2005). The factors influencing transactional sex among young men and women in 12 sub-Saharan African countries. Social Biology, 52(1–2), 56–72. https://doi.org/10.1080/19485565.2002.9989099
- Coetzee, J., Jewkes, R., & Gray, G. (2017a). Cross-sectional study of female sex workers in Soweto, South Africa: Factors associated with HIV infection. PLoS One, 12(10), Article e0184775. https://doi.org/10.1371/journal.pone.0184775
- Coetzee, J., Jewkes, R., & Gray, G. (2017b). Prevalence and patterns of victimization and polyvictimization among female sex workers in Soweto, a South African township: A cross-sectional, respondent-driven sampling study. Global Health Action, 10(1), Article 1403815. https://doi.org/10.1080/16549716.2017.1403815
- Dunkle, K., Jewkes, R., Brown, H., Gray, G., McIntryre, J., & Harlow, S. (2004). Transactional sex among women in Soweto, South Africa: Prevalence, risk factors and association with HIV infection. Social Science and Medicine, 59(8), 1581–1592. https://doi.org/10.1016/j.socscimed.2004.02.003
- Espi, G., Leibbrandt, M., & Ranchhod, V. (2021). The relationship between employment history and COVID-19 employment outcomes in South Africa. NIDS-CRAM. https://cramsurvey.org/wp-content/uploads/2020/09/6.-Espi-G.-Leibbrandt-M.-_-Ranchhod-V.-2020-The-relationship-between-employment-history-and-COVID-19-employment-outcomes-in-South-Africa.pdf
- Formson, C., & Hilhorst, D. (2016). The many faces of transactional sex: Women's agency, livelihood and risk factors in humanitarian contexts: A literature review. WageningenUniversity. https://assets.publishing.service.gov.uk/media/57a0896440f0b64974000060/WP41-transactionalsex.pdf
- Gibbs, A., Washington, L., Abdelatif, N., Chirwa, E., Willan, S., Shai, N., Sikweyiya, Y., Mkhwanazi, S., Ntini, N., & Jewkes, R. (2020). Stepping stones and creating futures intervention to prevent intimate partner violence among young people: Cluster randomized controlled trial. Journal of Adolescent Health, 66(3), 323–335. https://doi.org/10.1016/j.jadohealth.2019.10.004
- Gichane, M. W., Wamoyi, J., Atkins, K., Balvanz, P., Maman, S., Majani, E., & Pettifor, A. (2020). The influence of cash transfers on engagement in transactional sex and partner choice among adolescent girls and young women in northwest Tanzania. Culture, Health & Sexuality, 16, 1–15. https://doi.org/10.1080/13691058.2020.1811890
- Harris, P., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. (2009). Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Information, 42(2), 377–381. https://doi.org/10.1016/j.jbi.2008.08.010
- Hensen, B., Floyd, S., Chabata, S., Chiyaka, T., Busza, J., Mushati, P., Birdthistle, I., Hargreaves, J., & Cowan, F. (n.d.). Charactersitics of male sexual partners and knowledge of male partner's HIV status among young women who sell sex enrolled in an evaluation of DREAMS in Zimbabwe, 2017. London School of Hygiene and Tropical Medicine. https://www.lshtm.ac.uk/files/characteristics-of-male-sexual-partners.pdf
- Jaffer, M., Christofides, N., Hlongwane, K., Otwombe, K., Milovanovic, M., Hopkins, K. L., Matuludi, M., Mbowane, V., Abdullah, F., Gray, G., Jewkes, R., & Coetzee, J. (2022). The HIV cascade of care and service utilisation at sex work programmes among female sex workers in South Africa. AIDS and Behavior, https://doi.org/10.1007/s10461-022-03616-6
- Jewkes, R., Dunkle, K., Nduna, M., & Shai, N. (2012). Transactional sex and HIV incidence in a cohort of young women in the stepping stones trial. Journal of AIDS and Clinical Research, 3(5). https://doi.org/10.4172/2155-6113.1000158
- Jewkes, R., Otwombe, K., Dunkle, K., Milovanovic, M., Hlongwane, K., Jaffer, M., Matuludi, M., Mbowane, V., Hopkins, K., Hill, N., Gray, G., & Coetzee, J. (2021). Sexual IPV and non-partner rape of female sex workers: Findings of a cross-sectional community-centric national study in South Africa. SSM - Mental Health, 1. https://doi.org/10.1016/j.ssmmh.2021.100012
- Kyegombe, N., Meiksin, R., Wamoyi, J., Heise, L., Stoebenau, K., & Buller, A. M. (2020). Sexual health of adolescent girls and young women in central Uganda: Exploring perceived coercive aspects of transactional sex. Sex Reprod Health Matters, 28(1), 1700770. https://doi.org/10.1080/26410397.2019.1700770
- Li, Y., Marshall, C. M., Rees, H. C., Nunez, A., Ezeanolue, E. E., & Ehiri, J. E. (2014). Intimate partner violence and HIV infection among women: A systematic review and meta-analysis. Journal of The international Aids Society, 17(1), 18845. https://doi.org/10.7448/IAS.17.1.18845
- Milovanovic, M., Jewkes, R., Otwombe, K., Jaffer, M., Hopkins, K., Hlongwane, K., Matuludi, M., Mbowane, V., Gray, G., Dunkle, K., Hunt, G., Welte, A., Kassanjee, R., Slingers, N., Vanleeuw, L., Puren, A., Kinghorn, A., Martinson, N., Abdullah, F., & Coetzee, J. (2021). Community-led cross-sectional study of social and employment circumstances, HIV and associated factors amongst female sex workers in South Africa: Study protocol. Global Health Action, 14(1), Article 1953243. https://doi.org/10.1080/16549716.2021.1953243
- National Department of Health, Statistics South Africa, South African Medical Research Council, & ICF. (2019). South Africa demographic and Health Survey 2016. NDoH, Stats SA, SAMRC, ICF.
- Nguyen, N. (2017). Sexual partner type and risk of incident HIV infection among adolescent girls and young women in rural South Africa. [Doctoral disseration], University of North Carolina at Chapel Hill Graduate School. https://cdr.lib.unc.edu/concern/dissertations/7p88ch03c
- Nguyen, N., Powers, K., Miller, W., Howard, A., Halpern, C., Hughes, J., Wang, J., Twine, R., Gomez-Olive, F. X., MacPhail, C., Kahn, K., & Pettifor, A. (2019). Sexual partner types and incident HIV infection among rural South African adolescent girls and young women enrolled in HPTN 068: A latent class analysis. Journal of Acquired Immune Deiciency Syndrome, 82(1), 24–33. https://doi.org/10.1097/QAI.0000000000002096
- Plan International and the African Child Policy Forum (ACPF). (2020). Under Siege: Impact of COVID-19 in girls in Africa. ACPF. https://www.casemanagement.alliancecpha.org/en/system/tdf/library/attachments/under_siege-impact_of_covid-19_on_girls_in_africa.pdf?file=1&type=node&id=40325
- Pyett, P., & Warr, D. (1997). Vulnerability on the streets: Female sex workers and HIV risk. AIDS Care, 9(5), 539–547. https://doi.org/10.1080/713613193
- Ranganathan, M., MacPhail, C., Pettifor, A., Kahn, K., Khoza, N., Twine, R., Watts, C., & Heise, L. (2017). Young women's perceptions of transactional sex and sexual agency: A qualitative study in the context of rural South Africa. BMC Public Health, 17(1), Article 666. https://doi.org/10.1186/s12889-017-4636-6
- Saul, J., Bachman, G., Allen, S., Toiv, N., Cooney, C., & Beamon, T. (2018). The DREAMS core package of interventions: A comprehensive approach to preventing HIV among adolescent girls and young women. PLoS One, 13(12), Article e0208167. https://doi.org/10.1371/journal.pone.0208167
- Scorgie, F., Baron, D., & Delany-Moretlwe, S. (2018). STRIVE impact case study: Prioritising combination HIV prevention for adolescent girls and young women in South Africa. Strive. http://strive.lshtm.ac.uk/system/files/attachments/Impact%20case%20study%20-%20Combination%20HIV%20prevention%20for%20AGYW%20in%20SA.pdf
- Simbayi, L., Zuma, K., Zungu, N., Moyo, S., Marinda, E., Jooste, S., Mabaso, M., Ramlagan, S., North, A., Van Zyl, J., & Mohlabane, N. (2019). South African national HIV prevalence, incidence, behaviour and communication survey, 2017. HSRC Press.
- Statistics South Africa. (2020). Quarterly labour force survey. Quarter 4: 2019. Stats SA. https://www.statssa.gov.za/publications/P0211/P02114thQuarter2019.pdf
- Stoebenau, K., Heise, L., Wamoyi, J., & Bobrova, N. (2016). Revisting the understanding of “transactional sex” in sub-Saharan Africa: A review and synthesis of the literature. Social Science & Medicine, 168, 186–197. https://doi.org/10.1016/j.socscimed.2016.09.023
- The Global Fund. (2020, March). Technical Brief HIV programming for adolescent girls and young women in high-HIV burden settings. https://www.theglobalfund.org/media/4576/core_adolescentgirlsandyoungwomen_technicalbrief_en.pdf
- The National Association of People living with HIV and AIDS in South Africa. (2012). The people living with HIV stigma index: User guide (English). NAPWA SA.
- UCSF, Anova Health Institute, & WRHI. (2015). South African Health monitoring study (SAHMS), final report: The integrated biological and behavioural survey among female sex workers, South Africa 2013-2014.
- UNAIDS. (2014). 90-90-90: An ambitious treatment target to help end the AIDS epidemic. https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf
- UNICEF. (2021). Improving the quality of pre-exposure prophylaxis implementation for adolescent girls and young women in eastern and Southern Africa. https://www.unicef.org/esa/media/9701/file/AGYW-PrEP-Implementation-Brief-ESA-2021.pdf
- Wilson, C., Wright, P., Safrit, J., & Rudy, B. (1999). Epidemiology of HIV infection and risk in adolescents and youth. Journal of Acquired Immune Deficiency Syndrome, 54(Suppl 1), S5–S6. https://doi.org/10.1097/QAI.0b013e3181e243a1
- Wojcicki, J. (2002). Commercial sex work or ukuphanda? Sex-for-money exchange in Soweto and Hammanskraa Area, South Africa. Culture, Medicine and Psychiatry, 26(3), 339–370. https://doi.org/10.1023/a:1021291922026
- World Health Organization. (2002). WHO multi-country study on women's health and domestic violence: Core questionnaire and WHO instrument. WHO.