
ABSTRACT
There is an urgent need for greater provision of mental health services to people living with HIV. HIV testing and counselling (HTC) sessions diagnose HIV and offer appropriate psychosocial support and behavioural messages to support people to link into HIV care. It is not known to what extent HTC currently addresses mental health. We examined transcriptions of 116 audio-recorded HTC sessions delivered in Uganda against a checklist of mental health techniques. Hierarchical cluster analysis explored co-occurrence of techniques. Core counselling skills were very commonly present, and co-occurred. Assessment techniques were not commonly seen. Specific therapy techniques to treat anxiety or depression were not present. HTC staff are a resource for delivering mental health care for people with HIV, owing to their strong fundamental counselling skills. However, training is needed in assessment and evidence-based therapies. Provision of fuller assessment and interventions may increase detection and signposting for mental health and alcohol use, both of which may affect linkage into care. HTC staff have fundamental skills that could also be developed to train and supervise other staff to provide much needed mental health support to people living with HIV. Future research should develop brief mental health interventions for delivery by HTC staff.
Introduction
There is a well-documented lack of access to mental health services globally, and a particular need for services for people living with HIV (PLWH) (Abas et al., Citation2014; Remien et al., Citation2019). A paucity of mental health policy, systems, context-appropriate interventions, and trained staff underpin low service provision for mental health in HIV (Wainberg et al., Citation2017). This is relevant to HIV as better assessment and intervention for mental health can address the challenge of linking people into their HIV care (Bhatia et al., Citation2011; Ruzagira et al., Citation2017). In many countries, there is an existing infrastructure for HIV services, which could be utilised to support the delivery of mental health care, in an integrated package (Chamie et al., Citation2020). HIV testing and counselling (HTC) is often a person’s first contact with HIV-related services and represents an opportunity to assess and offer either brief intervention or linkage into other mental health services.
Given the opportunity to contact with patients during HTC sessions represents and the lack of mental health provision for people living with HIV, there is a need for research examining if and how HTC can be developed to meet mental health needs. This is vital in its own right and to support that linkage into HIV care. There is inconsistency about what should be in the “counselling” component of HTC sessions, with recommendations for only brief information and behavioural advice conflicting with a recognition of the need to provide psychosocial support to help link people into HIV treatment (WHO, Citation2019). The meaning of “counselling” then covers advice and instruction, as well as psychological support and intervention. Some countries’ HTC guidelines include the need to assess for depression, as in Uganda for example (Ministry of Health, Citation2018).
In common with other areas in mental health (Fairburn & Cooper, Citation2011), there has been little research into the competence and actual practice of HTC staff. The HTC staff are trained in some behaviour change techniques and communication skills. These staff may have an important contribution to make to improving mental health care for PLWH, as a potentially unrecognised human resource with existing mental health skills. Options for HTC staff’s contribution to global mental health include assessment, brief intervention provision, signposting to other appropriate mental health services and/ or provision of mental health intervention directly to clients. There may also be a role to train and supervise lay health workers, who are commonly used in mental health interventions (Wainberg et al., Citation2017). First, however, it is vital to understand the extent of the existing resource by exploring what mental health techniques they are currently using, and therefore what mental health skills they currently possess and what services they are already providing.
Methods
Setting and participants
Data were collected from staff providing HIV testing and counselling (HTC) sessions at “The AIDS Support Organisation” (TASO), a large non-governmental organisation providing HIV testing and care throughout Uganda. Four sites across Uganda were chosen to give a range of sites and remain accessible for researchers: Jinja (Eastern region), Entebbe (Central), Mulago in Kampala (Central) and Mbarara (Western). HTC staff employed full-time to provide services to adults were invited to take part. We aimed to recruit around 6–8 participants from each centre, and for them to record around four sessions.
Data collection
For each HTC counsellor, up to four HTC sessions were audio-recorded. We gained informed consent from both the client and the counsellor. This was recorded by a local research assistant also in attendance. Convenience sampling was used. Sessions were included regardless of a positive or negative HIV testing result. Audio-recording was transcribed verbatim. As per usual practice by the counsellors, most sessions were conducted in English. Those that were not in English were translated from the local language at transcription. Data were collected from January 2016 until July 2016.
Ethical considerations
Counsellors were recruited by local research assistants, who clarified their data would not be shared with anyone, including their managers. Written consent was gained from counsellors, and verbal consent from clients, recorded by the research assistant. All counsellors and clients were aware that participation was entirely voluntary, that the purpose of the study was to explore behaviours of the counsellor, and that they had the opportunity only at the end of the recording to withdraw their data. Neither personal information was transcribed about clients nor counsellors, and audio-recordings were destroyed once transcriptions were checked. The University of Bath, Ugandan National Council for Science and Technology (UNCST) and the Uganda Virus Research Institute Research Ethics Committee gave ethical approvals for the research.
Data analysis
Transcribed data were analysed with quantitative content analysis, to code for the presence or absence of different mental health techniques (Krippendorff, Citation2018). First, it was necessary to create a checklist of techniques. The backbone for this checklist was the Enhancing Assessment of Common Therapeutic Factors (ENACT) rating scale on therapist competence (Kohrt et al., Citation2015). This scale is intended for use in low-middle income settings and covers common techniques that are shared across psychological treatments and are non-specialist (i.e., Do not require specialist training in any form of psychological therapy). The first item on this scale, relating to non-verbal behaviours, was not used owing to our use of audio-recordings. The remaining eighteen were included. Several of the items on the scale include multiple observable techniques, for example Item 2 covers open questions, summarising, and clarifying statements. Here, we divided these into individual items.
Similar to the ENACT list, Murray et al (Murray et al., Citation2014) compiled a list of techniques present in evidence-based therapies that could not require highly trained staff. Their “Common Elements Treatment Approach” (CETA) includes techniques relevant to depression, anxiety and trauma-related difficulties. There is an unsurprisingly substantial overlap with the ENACT scale, and we included CETA’s more advanced, formal cognitive–behavioural therapy (CBT) techniques, such as teaching relaxation and exposure-based interventions, in our checklist. Finally, we inspected core HTC training manual’s checklists to assess counselling (I-TECH, Citation2006) and included items relating to mental health support.
The resulting checklist of techniques to support mental health contained 48 items across 18 themes: verbal communication skills; rapport building; emotion focussed work; use of empathy; assessment of function; exploration of explanatory models; coping; assessment of circumstances; assessment of health; involvement of family/social network; goal setting; promotion of hope; psychoeducation; problem solving; eliciting feedback; confidentiality; risk assessment; and specific CBT techniques covering relaxation, activation, cognitive change and exposure techniques. Across the themes, there are ten techniques focusing on different types of assessment.
Transcripts were analysed for the presence of each technique. As it was not often possible to tell when one occurrence of a technique began and ended, coding was simply for presence/absence in entire transcribed session. Cohen’s kappa was calculated on the transcripts scored by two authors (EC and FM) to address inter-rater reliability, requiring at least 0.8 equating to “good” (McHugh, Citation2012). Simple counts and percentage of sessions a technique was observed in are reported.
To address whether techniques tended to occur in any pattern, hierarchical cluster analysis was conducted. Checklist techniques appearing in at least 10% of the transcripts (and therefore were not rare), were subjected to unweighted group method with arithmetic mean (UPGMA) cluster analysis, based on the Jaccard Similarity Coefficient (Sokal, Citation1958). The UPGMA cluster analysis is a distance-matrix method, employing sequential clustering to build a dendrogram. First, all sequences were compared via pairwise alignment to compute the Jaccard Similarity Coefficient matrix. The two sequences with the minimum distance were identified and clustered as a singular pair. Subsequently, the distance between this pair and all other sequences was recalculated to form a new matrix. Then, the sequence that was closest to the first pair was identified and clustered. This process was repeated until all sequences were incorporated into the cluster. The height of the link joining observations on the dendrogram was joined was assessed using the Jaccard Similarity Coefficient, to demonstrate the similarity between two clusters. Briefly, where similarity approaches the maxima, “1”, this indicates items occurred together 100% of the time, whilst at the minima, “0”, items occurred together 0% of the time (Saraçli et al., Citation2013). All data analyses were conducted using R (R Core Team), and dendrogram was drawn using PAleontological Statistics (Hammer et al., Citation2001).
Results
Across the four sites, 29 counsellors were recruited and provided 116 transcripts that were analysed (19 analysed by both FM and EC, 8 by FM alone and 89 by EC alone). Inter-rater reliability was kappa = 0.91, meaning percentage agreement is within the 82–100% range and are thus inter-rater reliability is “almost perfect” (McHugh, Citation2012). The overall cluster analysis cophenetic distance ratio for 0.97, indicating a reliable and robust analysis.
provides the simple counts of the number of occurrences (number of transcripts in which techniques are observed) and the percentage of transcripts in which the techniques occur.
Table 1. List of techniques and number of transcripts in which they were observed.
The most commonly used techniques are related to active listening skills. There were five techniques that were never observed as present: Begins with less intimidating or less sensitive issues; Problem solving: solution generation and action planning; Imaginal Exposure – complete desensitisation; Live exposure – face triggers and reminders; and Live exposure – complete desensitisation. Formal therapy techniques were used less commonly overall. The most commonly used items relate to verbal communication skills and the use of empathy.
Assessment items were not all commonly used. Overall assessment of problems a client presented occurred in 82.8% of interactions, however more detailed assessment was rarer including assessment of physical health (31%), harm to self/others (28%), alcohol use (17%), recent events and their impact (5%), mental health issues beyond what described in the presenting problem (3%), social and family support (3%), and functioning (1%).
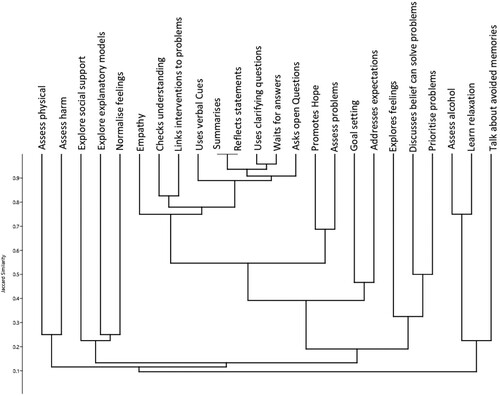
provides the results of the cluster analysis. Empathy, checking understanding, linking intervention to problems, use of verbal cues, summarising, reflecting, clarifying questions, waiting for answers and using open questions are core skills that show high co-occurrence: the techniques were frequently done and mostly done together. shows there is no clustering of the assessment items, showing that there is no pattern of how these co-occur in the data.
Figure 1. Dendrogram showing linkage. Including all items used in at least 10% of the transcripts.
Discussion
This study aimed to examine the mental health techniques HTC staff use in their sessions, to explore their existing skills and service provision. The data show that although formal therapy components were not commonly used, many core communication skills were evidenced and used in the vast majority of the sessions. The HTC staff had a coherent set of active listening skills. These verbal communication and empathy techniques can be considered as essential, core skills, that underlie all further therapeutic work. The core skills are shared principles across many different therapeutic traditions (Lundh, Citation2014). It is clear then that this HTC workface has the foundation skills to provide further psychological support.
Normalising and exploring feelings did not form part of the cluster with other core skills. These two techniques were also not linked together. This suggests that focused attention to emotions is less common. This supports qualitative findings that HIV counsellors in Uganda tend to focus more on behaviours than on exploration of emotions to understand mental health (Martin et al., Citation2020). Attention is needed to improve practice in this area. The emotional impact of a HIV diagnosis is linked to denial and lack of linkage into care (Horter et al., Citation2017). Support and encouragement from health care providers is an important facilitator of linkage into care (Sanga et al., Citation2019). Culturally appropriate strategies for providing emotional support at diagnosis should be developed and implemented.
Another area for further development is assessment techniques. Assessment techniques were not all commonly used, and there was no clear pattern in how they were used together. This is potentially problematic, given the context is of physical health here, and the strong links between mental health, HIV, social support and alcohol use (Nyoni et al., Citation2020; Pantalone et al., Citation2020; Velloza et al., Citation2019). This may reflect pressures HTC staff are under to see larger numbers of people, or a need for further training and supervision (Martin et al., Citation2020). Greater training on assessment and provision of a full assessment protocol may address this, and lead to greater detection of potential barriers to linkage into care and risks of poor health outcomes.
Specific CBT therapy techniques of exposure (relevant to anxiety difficulties), problem solving and action planning were never observed. This may be due to many reasons, including lack of need, lack of skill or the HTC sessions being too short or pressured with other tasks (Martin et al., Citation2020). Techniques relating to therapy components, such as goal setting, promotion of hope, and relaxation were used but not frequently. They were no clear associations between these therapy component techniques to the use of other techniques. These techniques could usefully be included in a relatively brief format. Techniques such as goal setting are core components in self-management interventions (Crowley & Rohwer, Citation2021).
Two clusters were found including items that can be thought of as components of therapy were (1) assessment of problems often used alongside promotion of hope, and (2) assessment of alcohol use often used alongside helping clients learn relaxation. The suggests that when these elements were assessed for, a linked intervention component was provided. The foundations are there to develop more nuanced application of therapy components.
This study has several limitations. Our checklist is based on existing, validated tools, however it has not been previously used. HTC staff taking part were self-selecting and aware of the recording process, which may have altered their practice. In-depth review of case notes may provide a way to triangulate our findings. Further, it was not clear in how many cases more mental health assessment and intervention was needed given the needs of the clients. This study signals the current level of practice, however further work should start to link use of different techniques to mental health and HIV outcomes, to allow us to optimise HTC sessions.
In conclusion, HIV testing and counselling staff represent a resource for delivering mental health care for people with HIV, owing to their existing practice and fundamental counselling skills. These staff provide the HIV diagnosis and have a strong role to support linkage into HIV care. The HTC sessions themselves are currently only partly used as an opportunity to detect and begin to address mental health difficulties. Poor mental health is intertwined with poor linkage into care (Bhatia et al., Citation2011). Our data show that HTC sessions do not offer formal interventions to fully assess nor address alcohol use and mental health. This represents a missed opportunity. Further research should explore how best to use the valuable, existing resource of HTC staff who have excellent core skills to be developed further to provide interventions, or to train and supervise others. This would help address mental health difficulties amongst persons with HIV, which link to poor physical outcomes. Development of brief interventions for use by HTC staff to address mental health barriers to linkage into care could usefully leverage these skills to tackle a major health problem.
Acknowledgements
We would like to thank the staff and service users at TASO who participated in data collection, in addition to the research assistants who supported the data collection.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abas, M., Ali, G.-C., Nakimuli-Mpungu, E., & Chibanda, D. (2014). Depression in people living with HIV in sub-Saharan Africa: Time to act. Tropical Medicine & International Health, 19(12), 1392–1396. https://doi.org/10.1111/tmi.12382
- Bhatia, R., Hartman, C., Kallen, M. A., Graham, J., & Giordano, T. P. (2011). Persons newly diagnosed with HIV infection are at high risk for depression and poor linkage to care: Results from the steps study. Aids and Behavior, 15(6), 1161–1170. https://doi.org/10.1007/s10461-010-9778-9
- Chamie, G., Hickey, M. D., Kwarisiima, D., Ayieko, J., Kamya, M. R., & Havlir, D. V. (2020). Universal HIV testing and treatment (UTT) integrated with chronic disease screening and treatment: The SEARCH study. Current HIV/AIDS Reports, 17(4), 315–323. https://doi.org/10.1007/s11904-020-00500-7
- Crowley, T., & Rohwer, A. (2021). Self-management interventions for adolescents living with HIV: A systematic review. BMC Infectious Diseases, 21(1), 431–431. https://doi.org/10.1186/s12879-021-06072-0
- Fairburn, C. G., & Cooper, Z. (2011). Therapist competence, therapy quality, and therapist training. Behaviour Research and Therapy, 49(6-7), 373–378. https://doi.org/10.1016/j.brat.2011.03.005
- Hammer, Ø, Harper, D. A., & Ryan, P. D. (2001). PAST: Paleontological statistics software package for education and data analysis. Palaeontologia Electronica, 4(1), 9. https://palaeo-electronica.org/2001_1/past/past.pdf
- Horter, S., Thabede, Z., Dlamini, V., Bernays, S., Stringer, B., Mazibuko, S., Dube, L., Rusch, B., & Jobanputra, K. (2017). Life is so easy on ART, once you accept it”: Acceptance, denial and linkage to HIV care in Shiselweni, Swaziland. Social Science & Medicine, 176, 52–59. https://doi.org/10.1016/j.socscimed.2017.01.006
- I-TECH. (2006). Counseling Assessment Checklist: VCT for Nurses: Published online by International Training and Education Center for Health (I-TECH). Accessed online June 2020 https://www.go2itech.org/HTML/CM08/toolkit/tools/print/tools/skills/Coun_Assess_Check_VCT.doc
- Kohrt, B. A., Jordans, M. J. D., Rai, S., Shrestha, P., Luitel, N. P., Ramaiya, M. K., Singla, D. R., & Patel, V. (2015). Therapist competence in global mental health: Development of the ENhancing assessment of Common Therapeutic factors (ENACT) rating scale. Behaviour Research and Therapy, 69(0), 11–21. https://doi.org/10.1016/j.brat.2015.03.009
- Krippendorff, K. (2018). Content analysis. An introduction to its methodology. Sage Publications Ltd.
- Lundh, L.-G. (2014). The search for common factors in psychotherapy. Two theoretical models, with different empirical implications. Psychology and Behavioral Sciences, 3(5), 131–150. https://doi.org/10.11648/j.pbs.20140305.11
- Martin, F., Nalukenge, W., Lazarus, O., Birungi, J., & Seeley, J. (2020). Vital”: HIV counselling and testing staff’s views of addressing mental health with HIV in Uganda. BMC Health Services Research, 20(1), 1027. https://doi.org/10.1186/s12913-020-05881-4
- McHugh, M. L. (2012). Interrater reliability: The kappa statistic. Biochem Med (Zagreb), 22(3), 276–282. https://doi.org/10.11613/BM.2012.031
- Ministry of Health. (2018). Consolidated guidelines for the prevention and treatment of HIV and AIDS in Uganda. Ministry of Health. http://library.health.go.ug/publications/hivaids/consolidated-guidelines-prevention-and-treatment-hiv-uganda-1
- Murray, L. K., Dorsey, S., Haroz, E., Lee, C., Alsiary, M. M., Haydary, A., Weiss, W. M., & Bolton, P. (2014). A common elements treatment approach for adult mental health problems in low- and middle-income countries. Cognitive and Behavioral Practice, 21(2), 111–123. https://doi.org/10.1016/j.cbpra.2013.06.005
- Nyoni, T., Sallah, Y. H., Okumu, M., Byansi, W., Lipsey, K., & Small, E. (2020). The effectiveness of treatment supporter interventions in antiretroviral treatment adherence in sub-Saharan Africa: A systematic review and meta-analysis. AIDS Care. https://doi.org/10.1080/09540121.2020.1742870.
- Pantalone, D. W., Nelson, K. M., Batchelder, A. W., Chiu, C., Gunn, H. A., & Horvath, K. J. (2020). A systematic review and meta-analysis of combination behavioral interventions co-targeting psychosocial syndemics and HIV-related health behaviors for sexual minority men. Journal of Sex Research. https://doi.org/10.1080/00224499.2020.1728514.
- Remien, R. H., Stirratt, M. J., Nguyen, N., Robbins, R. N., Pala, A. N., & Mellins, C. A. (2019). Mental health and HIV/AIDS: The need for an integrated response. Aids (London, England), 33(9), 1411–1420. https://doi.org/10.1097/QAD.0000000000002227
- Ruzagira, E., Grosskurth, H., Kamali, A., & Baisley, K. (2017). Brief counselling after home-based HIV counselling and testing strongly increases linkage to care: A cluster-randomized trial in Uganda. Journal of the International AIDS Society, 20(2), e25014. https://doi.org/10.1002/jia2.25014
- Sanga, E. S., Mukumbang, F. C., Mushi, A. K., Lerebo, W., & Zarowsky, C. (2019). Understanding factors influencing linkage to HIV care in a rural setting, Mbeya, Tanzania: Qualitative findings of a mixed methods study. BMC Public Health, 19(1), 383. https://doi.org/10.1186/s12889-019-6691-7
- Saraçli, S., Doğan, N., & Doğan, İ. (2013). Comparison of hierarchical cluster analysis methods by cophenetic correlation. Journal of Inequalities and Applications, 2013(1), 203. https://doi.org/10.1186/1029-242X-2013-203
- Sokal, M. (1958). A statistical method for evaluating systematic relationships. University of Kansas Science Bulletin, 38, 1409–1438.
- Velloza, J., Kemp, C. G., Aunon, F. M., Ramaiya, M. K., Creegan, E., & Simoni, J. M. (2019). Alcohol use and antiretroviral therapy non-adherence among adults living with HIV/aids in sub-Saharan Africa: A systematic review and meta-analysis. Aids and Behavior, https://doi.org/10.1007/s10461-019-02716-0.
- Wainberg, M. L., Scorza, P., Shultz, J. M., Helpman, L., Mootz, J. J., Johnson, K. A., Neria, Y., Bradford, J.-M. E., Oquendo, M. A., & Arbuckle, M. R. (2017). Challenges and opportunities in global mental health: A research-to-practice perspective. Current Psychiatry Reports, 19(5), 28. https://doi.org/10.1007/s11920-017-0780-z
- WHO. (2019). Consolidated guidelines on HIV testing services for a changing epidemic. World Health Organisation. https://www.who.int/publications/i/item/consolidated-guidelines-on-hiv-testing-services-for-a-changing-epidemic
