
ABSTRACT
We conducted a mixed studies review to examine domestic violence and stigma against women affected by HIV. We searched Medline, Web of Science, PsycINFO and EMBASE databases with no starting date limit. Studies that reported on experiences of stigma, discrimination, or domestic violence against women affected by HIV in any country were included. Because the review focused on HIV stigma-related violence, we only included studies that reported violence following an HIV diagnosis or at the time of HIV testing. A total 1056 records were screened; 89 articles were assessed for full text eligibility and 49 studies were selected for evidence synthesis. A convergent approach was used and study findings were analysed thematically. Four broad themes emerged: (1) being affected by HIV increases domestic violence, (2) supportive reactions from partners, (3) HIV stigma is associated with domestic violence, and (4) domestic violence associated with HIV-stigma is gendered. Research gaps identified included the burden of intersectional stigma of domestic violence and HIV, and the mediating role of HIV stigma in domestic violence for women with HIV, highlighting the need for further research in this area to reduce violence against women living with HIV.
KEYWORDS:
Background
An estimated 38 million people globally were living with HIV in 2019. Nineteen million were women, of whom 300,000 died of AIDS-related causes (WHO, Citation2019). People living with HIV face social stigma and discrimination (Parker & Aggleton, Citation2003), stemming from moral judgement and fear of contagion and often resulting in discrimination from family, friends, neighbours, healthcare providers, and others (Ekstrand et al., Citation2012). Goffman defined stigma as a process through which someone is discredited based on an undesirable attribute (Goffman, Citation1963). Stigma has been categorized into four dimensions: enacted stigma (acts of discrimination), anticipated stigma (expectation of discrimination), perceived stigma (normative or felt stigma), and internalized stigma (stigma against the self) (Turan & Nyblade, Citation2013).
For women living with HIV (WLHIV), the experience of stigma is intertwined with gender discrimination and is often violent (Logie et al., Citation2011). The World Health Organization (WHO) estimates that almost 30% of women have experienced intimate partner physical or sexual violence in their lifetime (WHO, Citation2017). The link between HIV and domestic violence against women is bi-directional: domestic violence increases the risk of acquiring HIV and HIV increases the risk of domestic violence (Maman et al., Citation2000). The WHO defines domestic violence as physical, sexual, or psychological abuse committed by an intimate partner (Kalokhe et al., Citation2015; WHO, Citation2005) or other members of a woman’s shared household (Kalokhe et al., Citation2015). While HIV stigma may manifest in domestic violence against women, the stigma of domestic violence may prevent them from reporting or seeking help.
Previous reviews have examined the relationship between HIV and domestic violence (Campbell et al., Citation2008; Kennedy et al., Citation2015; Kouyoumdjian et al., Citation2013; Maman et al., Citation2000), but none has specifically examined the link between HIV stigma and domestic violence. In order to frame effective responses to both, we need to understand the effects of intersectional stigma on women’s lives. Our review aimed to synthesize the evidence on violence experienced by women affected by HIV (defined here as women living with or testing for HIV), how it is linked to HIV stigma, and how the two forms of stigma intersect.
Methods
Search strategy and terms
We conducted a mixed studies review (Pluye & Hong, Citation2014) of the literature to explore violence experienced by women affected by HIV and its link with HIV stigma. Medline, Web of Science, PsycINFO and EMBASE databases were searched to cover the biomedical, psychological, and public health literature, with no starting date limit and up to March 2020. Librarian-guided searches using keywords and MeSH (medical subject heading) terms covered HIV, stigma, and domestic violence. No limits were placed on gender, form of violence, or study design, but articles about women reporting on intimate partner and domestic violence were selected. shows the Medline search on which the other searches were based, followed by citation chaining from reference lists.
Table 1. Ovid Medline example of search strategy and terms.
Inclusion and exclusion criteria
The review included studies involving WLHIV or taking an HIV test. Domestic violence was defined as violence from intimate partners, families, or both. The broad inclusion criteria included peer-reviewed, original research articles that reported on experiences of stigma, discrimination, or domestic violence among cis and trans women affected by HIV in any country.
We excluded studies of experiences of men living with HIV, men who have sex with men, children and adolescents, studies on the physical or mental health outcomes of HIV or violence, and studies on non-domestic violence. Because the review focused on violence in relation to HIV stigma, we excluded studies that focused on reported lifetime prevalence of violence (where violence occurring before HIV diagnosis could not be distinguished from violence occurring after) or domestic violence as a risk factor for acquiring HIV. Review articles, intervention studies, conference abstracts, comments, and editorials were excluded.
Data extraction, quality, and synthesis
After screening by title and abstract, studies that met the inclusion criteria and reported findings on violence related to taking an HIV test, post-disclosure violence, non-disclosure of HIV diagnosis due to fear of violence, and violence after diagnosis, were included in full-text review. Information such as sample size, study design, location, setting, and a summary of key findings on stigma were extracted from the selected qualitative and mixed methods () and quantitative studies (). Quality of studies was assessed using the Mixed Methods Appraisal (MMAT) tool (Hong et al., Citation2018). None of the selected studies was excluded on the basis of quality.
Table 2. Summary of selected qualitative and mixed methods studies.
Table 3. Summary of selected quantitative studies.
We took a convergent approach to synthesis and analysed qualitative and quantitative data together (Gough, Citation2015; Pluye & Hong, Citation2014). A narrative synthesis approach analysed all study types thematically (Grant & Booth, Citation2009; Pluye & Hong, Citation2014). Patterns in findings across studies were analysed inductively and iteratively to develop broad conceptual themes (Popay et al., Citation2006).
Results
The initial search yielded 1056 records from which 637 duplicates were removed (). After title and abstract screening, 548 records did not meet the inclusion criteria. Eighty-nine full text articles were reviewed for eligibility, of which 40 were excluded for reasons described in . The analysis included 49 studies, of which 18 used qualitative, 7 mixed-methods, and 24 quantitative methods. summarises their locations.
Figure 1. PRISMA diagram for data extraction.
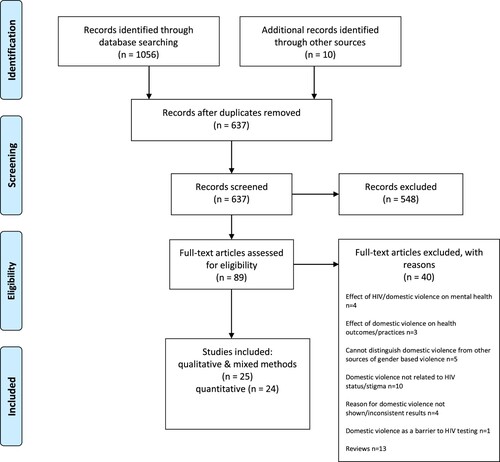
Table 4. Geographic location of selected studies.
Being affected by HIV increases domestic violence
The risk of domestic violence against women affected by HIV can increase at every stage of the trajectory, from taking an HIV test to disclosing status to living with HIV. Three studies described how HIV testing could increase the risk of domestic violence and how anticipation of violence could cause women to refrain from disclosing positive test results (Pool et al., Citation2001; Shamu et al., Citation2014; Turan et al., Citation2016). Although nearly one-third of US women declined to take an HIV test, this was not strongly associated with fear of partner violence (Maher et al., Citation2000).
Thirty-one studies found that disclosure of positive HIV test results could increase the risk of actual violence or that fear of violence could lead to non-disclosure. Twelve quantitative (Abuogi et al., Citation2019; Ezechi et al., Citation2009; Hardy et al., Citation2020; Iliyasu et al., Citation2011; Koenig et al., Citation2002; Malaju & Alene, Citation2013; Maman et al., Citation2016; Ojikutu et al., Citation2016; Olowookere et al., Citation2015; Onono et al., Citation2014; Shamu et al., Citation2014; Turan et al., Citation2011), twelve qualitative (Arrey et al., Citation2015; Ashaba et al., Citation2017; Colombini et al., Citation2016; Derose et al., Citation2017; Gielen et al., Citation1997; Hatcher et al., Citation2014; Hatcher et al., Citation2016; Mulrenan et al., Citation2015; Pool et al., Citation2001; Rujumba et al., Citation2012; Zamudio-Haas et al., Citation2012; Zunner et al., Citation2015), and seven mixed methods (Adeniyi et al., Citation2017; Gielen et al., Citation2000; Knettel et al., Citation2019; Mepham et al., Citation2011; Odiachi et al., Citation2018; Orza et al., Citation2015; Turan et al., Citation2011) studies reported on actual or anticipated post-disclosure violence. Generally, women were afraid to disclose positive test results for fear of violent backlash and women who disclosed largely experienced violence. Fears of disclosure were greater for women in polygamous marriages as a positive diagnosis could lead to the husband returning to another wife (Rujumba et al., Citation2012). Fifteen studies described how domestic violence started or worsened following HIV diagnosis and provided the strongest evidence that having HIV increases women’s risk of violence (Aryal et al., Citation2012; Emusu et al., Citation2009; Ezeanochie et al., Citation2011; Ezechi et al., Citation2009; Gielen et al., Citation2000; Hardy et al., Citation2020; Hatcher et al., Citation2016; Hyginus et al., Citation2012; Iliyasu et al., Citation2011; Marais et al., Citation2019; Mulrenan et al., Citation2015; Olowookere et al., Citation2015; Orza et al., Citation2015; Shamu et al., Citation2014; Zunner et al., Citation2015). One study from South Africa described how violence started or worsened immediately after HIV testing, while another reported worsening of abuse due to HIV status (Hatcher et al., Citation2016; Marais et al., Citation2019). Similar findings of violence commencing or escalating after disclosure were reported from Ghana, Uganda, Zimbabwe, Kenya, and Nigeria (Emusu et al., Citation2009; Ezeanochie et al., Citation2011; Ezechi et al., Citation2009; Hardy et al., Citation2020; Hyginus et al., Citation2012; Iliyasu et al., Citation2011; Olowookere et al., Citation2015; Shamu et al., Citation2014; Zunner et al., Citation2015) A third of participants in a global survey reported violence because of HIV (Orza et al., Citation2015), while a small proportion of US women reported similar findings (Gielen et al., Citation2000). Women in Nepal reported a sharp rise in domestic violence, with economic violence starting only after diagnosis (Aryal et al., Citation2012) and, in India, WLHIV reported more “quarrels,” with almost a third of them attributed it to HIV status (Chakraborty et al., Citation2016).
Supportive reactions from partners
There were, however, fourteen studies that reported supportive reactions from partners (Abuogi et al., Citation2019; Adeniyi et al., Citation2017; Ashaba et al., Citation2017; Derose et al., Citation2017; Gielen et al., Citation1997; Gielen et al., Citation2000; Hershow et al., Citation2017; Iliyasu et al., Citation2011; Kabwama et al., Citation2019; Mulrenan et al., Citation2015; Odiachi et al., Citation2018; Rujumba et al., Citation2012; Shamu et al., Citation2014; Zamudio-Haas et al., Citation2012), and some showed that violence was a function of behavioural or relationship characteristics rather than HIV status. A South African study found no association between disclosure of HIV status and domestic violence, but non-disclosure was associated with a greater likelihood of experiencing violence, suggesting that non-disclosure could be a marker for a violent relationship (Maman et al., Citation2016). In a US study, violence was present in abusive and non-abusive partnerships and did not differ by serostatus (Koenig et al., Citation2002). A Ugandan study indicated that, although WLHIV experienced high levels of domestic violence, they were similar to those experienced in the general population (Kabwama et al., Citation2019). Vietnamese women who reported infection from their husbands did not experience or anticipate violence upon disclosure of positive status, mainly because their spouses were injection drug users and presumptive sources of infection (Hershow et al., Citation2017), and women from Western Kenya using couples testing and counselling services had a greater likelihood of reporting positive male partner reactions upon disclosure (Abuogi et al., Citation2019).
HIV stigma is associated with domestic violence
Violence was rarely described in the literature in terms of HIV-related stigma. It was described instead as physical, sexual, or emotional abuse due to HIV serostatus (Adeniyi et al., Citation2017; Aryal et al., Citation2012; Ashaba et al., Citation2017; Chakraborty et al., Citation2016; Chilemba et al., Citation2014; Emusu et al., Citation2009; Ezeanochie et al., Citation2011; Ezechi et al., Citation2009; Gielen et al., Citation1997; Gielen et al., Citation2000; Hardy et al., Citation2020; Hatcher et al., Citation2014; Hershow et al., Citation2017; Hyginus et al., Citation2012; Iliyasu et al., Citation2011; Kabwama et al., Citation2019; Koenig et al., Citation2002; Maher et al., Citation2000; Maman et al., Citation2016; Mepham et al., Citation2011; Moreno, Citation2007; Mulrenan et al., Citation2015; Odiachi et al., Citation2018; Olowookere et al., Citation2015; Orza et al., Citation2015; Osinde et al., Citation2011; Rujumba et al., Citation2012; Shamu et al., Citation2014; Zamudio-Haas et al., Citation2012; Zunner et al., Citation2015). Studies reported fears or acts of physical violence, blame, and abandonment due to suspicions of infidelity rather than conceiving them as the result of enacted stigma. For instance, a qualitative study in Malawi described women’s experiences of humiliation, abandonment, and blame as forms of emotional abuse due to HIV status rather than forms of enacted stigma (Chilemba et al., Citation2014). Studies described feelings of hopelessness, diminished self-worth, and guilt as emotional problems rather than consequences of internalized stigma (Chilemba et al., Citation2014; Zunner et al., Citation2015).
Eighteen studies did, however, explicitly show that HIV-related stigma was associated with domestic violence (Abuogi et al., Citation2019; Arrey et al., Citation2015; Colombini et al., Citation2016; Derose et al., Citation2017; Fiorentino et al., Citation2019; Hatcher et al., Citation2016; Jiwatram-Negron et al., Citation2018; Knettel et al., Citation2019; Logie et al., Citation2011; Marais et al., Citation2019; Matseke et al., Citation2016; Mehta et al., Citation2019; Ojikutu et al., Citation2016; Onono et al., Citation2014; Pool et al., Citation2001; Ramlagan et al., Citation2019; Turan et al., Citation2011; Turan et al., Citation2016). Women were afraid to take an HIV test or disclose their status because of HIV stigma-related violence or fears of it (anticipated stigma). Two Kenyan and one Ugandan studies described how fear of HIV stigma and discrimination was associated with avoiding testing (Pool et al., Citation2001; Turan et al., Citation2011; Turan et al., Citation2016). Five studies described how anticipated stigma and internalized stigma were important reasons for non-disclosure of status to avoid domestic violence (Abuogi et al., Citation2019; Arrey et al., Citation2015; Knettel et al., Citation2019; Ojikutu et al., Citation2016; Onono et al., Citation2014), while one study reported that disclosure increased risk of stigma and abuse from male partners (Colombini et al., Citation2016).
Nine studies considered stigma-related domestic violence in the everyday lives of WLHIV in a range of geographic settings (Derose et al., Citation2017; Fiorentino et al., Citation2019; Hatcher et al., Citation2016; Jiwatram-Negron et al., Citation2018; Logie et al., Citation2011; Marais et al., Citation2019; Matseke et al., Citation2016; Mehta et al., Citation2019; Ramlagan et al., Citation2019). In Cameroon, HIV-related stigma was associated with double the risk of frequent physical domestic violence, which was associated in turn with interruption of antiretroviral therapy (ART) (Fiorentino et al., Citation2019). A South African study reported that higher levels of internalized stigma and depression were associated with physical or psychological violence (Matseke et al., Citation2016). Another showed that women who survived domestic violence were more likely to experience personalized HIV stigma (Ramlagan et al., Citation2019). Two studies from South Africa reported briefly on the dual burden of HIV and domestic violence stigma, leading to reduced ability of WLHIV to seek support (Hatcher et al., Citation2016; Marais et al., Citation2019). The enacted HIV stigma experienced by women in the Dominican Republic contributed to food insecurity, while internalized stigma led to social isolation (Derose et al., Citation2017). Canadian WLHIV discussed how the combination of HIV stigma and gender discrimination trapped them in abusive relationships (Logie et al., Citation2011). Women reporting HIV-related stigma in Kazakhstan had almost twice the risk of experiencing intimate partner violence, with about one-tenth experiencing HIV-specific abuse (Jiwatram-Negron et al., Citation2018). In India, domestic violence associated with perceived and enacted HIV stigma was associated with unsafe sex (Mehta et al., Citation2019).
Domestic violence associated with HIV is gendered
Although all people living with HIV may face violence, the experiences of men and women may differ, often due to unequal social structures that position women as inferior to men (Boesten & Poku, Citation2013; Greig et al., Citation2008; Mitra & Sarkar, Citation2011). Disclosure of serostatus is often the first trigger for violence against women affected by HIV. Women usually test for HIV during pregnancy and this can result in disclosure asymmetry or serodiscordance when male partners have not been tested. Both can trigger domestic violence (Abuogi et al., Citation2019; Colombini et al., Citation2016; Ezechi et al., Citation2009; Hatcher et al., Citation2014; Mulrenan et al., Citation2015; Turan et al., Citation2016; Zunner et al., Citation2015). WLHIV experienced multiple forms of violence from different sources after disclosure. For instance, they were humiliated by partners and in-laws who publicized their serostatus and labelled them as prostitutes (Chilemba et al., Citation2014; Zunner et al., Citation2015). Family members and neighbours encouraged men to abandon their wives due to suspicions of infidelity and HIV reflecting badly on the family and community (Chilemba et al., Citation2014; Turan et al., Citation2016; Zamudio-Haas et al., Citation2012; Zunner et al., Citation2015). Children testing positive for HIV also sparked violence from male partners (Ezeanochie et al., Citation2011; Marais et al., Citation2019; Mulrenan et al., Citation2015).
Controlling behaviours and male partners deliberately infecting women were other forms of abuse. A qualitative study with Latina WLHIV in the US described how men did not want to be with women who had HIV and it became a factor in the quality of their relationships, giving men an excuse for controlling behaviours (Moreno, Citation2007). Women also reported being deliberately infected with HIV by their husbands or partners as a form of abuse (Emusu et al., Citation2009; Moreno, Citation2007).
Forceful interruption of treatment was another form of violence. Women who were currently on ART were three times more likely to report domestic violence, which could make it difficult for them to adhere to treatment (Osinde et al., Citation2011). Women who did not disclose hid their medication for fear of violent reprisals if male partners found out (Hatcher et al., Citation2014; Marais et al., Citation2019; Mepham et al., Citation2011; Zunner et al., Citation2015). Controlling partners became suspicious during clinic visits, becoming physically abusive and actively stopping women from collecting medication (Ashaba et al., Citation2017; Hatcher et al., Citation2016; Marais et al., Citation2019), or interfered with ART intake (Hardy et al., Citation2020; Zunner et al., Citation2015). Frequent physical violence was associated with ART interruption of greater than one month (Fiorentino et al., Citation2019). Finally, internalization of abuse led to hopelessness, which made it burdensome for women to engage in HIV care (Hatcher et al., Citation2016; Marais et al., Citation2019; Zunner et al., Citation2015), and caused some to contemplate suicide (Chilemba et al., Citation2014; Hardy et al., Citation2020; Hatcher et al., Citation2016; Zunner et al., Citation2015).
Withdrawal of financial support after an HIV diagnosis was yet another form of abuse reported by women in multiple studies (Aryal et al., Citation2012; Ashaba et al., Citation2017; Chilemba et al., Citation2014; Colombini et al., Citation2016; Derose et al., Citation2017; Hardy et al., Citation2020; Hyginus et al., Citation2012; Malaju & Alene, Citation2013; Odiachi et al., Citation2018; Turan et al., Citation2016; Zunner et al., Citation2015), and fearing withdrawal of financial support was a barrier to disclosure (Knettel et al., Citation2019; Odiachi et al., Citation2018; Pool et al., Citation2001; Rujumba et al., Citation2012; Turan et al., Citation2016). Women were also forced to tolerate their partners’ risky behaviours and abuse due to their financial dependence on them (Arrey et al., Citation2015; Chilemba et al., Citation2014; Emusu et al., Citation2009; Marais et al., Citation2019; Moreno, Citation2007; Orza et al., Citation2015). Lack of financial support could lead to food scarcity (Chilemba et al., Citation2014; Colombini et al., Citation2016; Derose et al., Citation2017; Zunner et al., Citation2015) and interruption of treatment (Odiachi et al., Citation2018).
Negotiation of safe sex was associated with higher risk of domestic violence against women, irrespective of cultural setting. Since WLHIV are more likely to negotiate safe sex, they are at greater risk of violence (Chakraborty et al., Citation2016; Chilemba et al., Citation2014; Colombini et al., Citation2016; Emusu et al., Citation2009; Gielen et al., Citation1997; Hatcher et al., Citation2014; Marais et al., Citation2019; Mehta et al., Citation2019; Mepham et al., Citation2011; Moreno, Citation2007; Mulrenan et al., Citation2015; Zamudio-Haas et al., Citation2012; Zunner et al., Citation2015). Latina women in the US found it difficult to find partners who would be willing to use condoms (Moreno, Citation2007). Traditional gender norms set expectations around childbearing, forcing women to engage in condomless sex (Emusu et al., Citation2009; Mulrenan et al., Citation2015; Ojikutu et al., Citation2016; Zunner et al., Citation2015), and studies from India found associations between domestic violence and negotiation of safe sex (Chakraborty et al., Citation2016; Mehta et al., Citation2019).
Women also reported being trapped in abusive relationships due to their HIV status (Derose et al., Citation2017; Logie et al., Citation2011; Marais et al., Citation2019; Moreno, Citation2007). Two African studies showed that women were afraid to report violence for fear of making their status public (Ezechi et al., Citation2009; Hardy et al., Citation2020). One study found that almost half of women did not report violence (Iliyasu et al., Citation2011) and another that WLHIV were more likely to report violence to formal and informal sources, although the reasons for such behaviours were not explored (Hyginus et al., Citation2012). WLHIV feared not finding another partner due to their serostatus (Derose et al., Citation2017; Logie et al., Citation2011). Internalization of emotional abuse from partners was another reason for women to remain in abusive relationships (Marais et al., Citation2019).
Discussion
Although previous reviews have examined HIV and domestic violence, ours is the first, to our knowledge, to examine the evidence around stigma and domestic violence in the lives of women affected by HIV. The evidence that being affected by HIV increases violence confirms the findings from previous reviews (Campbell et al., Citation2008; Kennedy et al., Citation2015; Kouyoumdjian et al., Citation2013; Maman et al., Citation2000), and this review adds evidence on how violence is linked to HIV stigma and the additional burden of the intersectional stigma of domestic violence and HIV.
Although most studies came from Africa, our findings held across high- and low-income countries. Some studies drew explicit links between violence and HIV stigma, but most only considered how violence was related to being affected by HIV. Several studies showed supportive reactions from partners, which highlighted the importance of interventions such as couples counselling in reducing violence following an HIV diagnosis. The review also captured how violence in the lives of women with HIV was gendered. Women were often blamed for bringing HIV into the relationship as they were usually the first to get tested during pregnancy – in itself not a biological necessity, but a manifestation of gender norms that medicalize women’s life processes, particularly reproduction (Conrad, Citation1992). Once known to have HIV, women were at increased risk of multiple forms of violence from male partners and their families.
The review also identified two important gaps in the literature. First, although both HIV and domestic violence are stigmatized, few studies have reported on the intersectional stigma of the two. This is important because, as shown in studies with women with multiple marginalized identities, the interaction of stigmas can amplify the stigma experience (Logie et al., Citation2011; Rice et al., Citation2018). Only three studies showed that WLHIV were unlikely to report violence due to fears of making their HIV status public, although the association with stigma was not explored (Ezechi et al., Citation2009; Hardy et al., Citation2020; Hyginus et al., Citation2012). HIV stigma may also worsen domestic violence stigma, as WLHIV who survive domestic violence may not be able to seek support after an episode due to the compounded shame of HIV and facing domestic violence. Two qualitative studies from South Africa reported this lack of social support (Hatcher et al., Citation2016; Marais et al., Citation2019), one highlighting the additional HIV shame created by abusive partners (Marais et al., Citation2019). Partners exploit the stigma of HIV, which when internalized may entrap women in abusive relationships (Logie et al., Citation2011; Marais et al., Citation2019).
The second gap is a lack of studies that recognize the mediating role of stigma in domestic violence against WLHIV. The theoretical literature recognises HIV stigma as a form of violence: physical violence against people living with HIV has been described as a form of enacted stigma and fear of it as anticipated stigma (Earnshaw & Chaudoir, Citation2009; Herek, Citation1999; Holzemer et al., Citation2007). Over a third of studies described violence experienced by WLHIV as related to HIV stigma, while the rest framed it as a function of HIV serostatus. Domestic violence in the lives of WLHIV may start or escalate upon HIV diagnosis and violence has been shown to be greater for WLHIV than for others (Kouyoumdjian et al., Citation2013). This means that, although all women may experience domestic violence, WLHIV may experience abuse solely due to their HIV serostatus. HIV, with its associated fears of transmission and blame for poor moral character (Herek, Citation2002), makes the violence happen. This is HIV stigma and it drives the violence that occurs in women’s lives. Knowing this is crucial to designing violence reduction interventions for WLHIV, because applying domestic violence interventions without accompanying HIV stigma reduction may make them ineffective.
Limitations
One reviewer screened articles due to resource constraints. The selected articles included diverse populations and study designs and comparability was limited. Most of the quantitative studies were cross-sectional, some with small sample sizes, which limited causal inference. The search terms captured the broad concepts of domestic violence, HIV, and stigma, but studies often reported violence as an outcome of HIV status (rather than HIV stigma) and some may have been missed. Hand-searches of reference lists minimized this limitation as far as possible. Finally, a broader search of HIV stigma could have included studies on violence such as controlling behaviours by partners and in-laws.
Conclusion
Our review synthesized the evidence on domestic violence and HIV stigma. The findings suggest that testing for or living with HIV increases the risk of domestic violence (although some women do get support from partners), that this violence is associated with HIV stigma, and that HIV-related domestic violence is gendered. The review identified important research gaps on the intersectional stigma of domestic violence and HIV and the need to recognize the mediating role of HIV stigma in domestic violence against women. The implications include (1) a need for empirical studies to understand the burden of intersecting HIV and domestic violence stigma in women’s lives and (2) the importance of the role of HIV stigma in domestic violence experienced by WLHIV, so that appropriate violence reduction interventions can be designed for them.
Acknowledgements
We thank Hattie Lowe for her careful reading and valuable input on this manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abuogi, L., Hampanda, K., Odwar, T., Helova, A., Odeny, T., Onono, M., Bukusi, E., & Turan, J. (2019). HIV status disclosure patterns and male partner reactions among pregnant women with HIV on lifelong ART in western Kenya. AIDS Care, 858–868. https://doi.org/10.1080/09540121.2019.1659915
- Adeniyi, O. V., Ajayi, A. I., Selanto-Chairman, N., Goon, D. T., Boon, G., Fuentes, Y. O., Hofmeyr, G. J., Avramovic, G., Carty, C., & Lambert, J. (2017). Demographic, clinical and behavioural determinants of HIV serostatus nondisclosure to sex partners among HIV-infected pregnant women in the eastern cape, South Africa. PLoS ONE, 12(8), e0181730. https://doi.org/10.1371/journal.pone.0181730
- Arrey, A. E., Bilsen, J., Lacor, P., & Deschepper, R. (2015). “It’s My secret”: Fear of disclosure among Sub-Saharan African migrant women living with HIV/AIDS in belgium. PLoS ONE, 10(3), e0119653. https://doi.org/10.1371/journal.pone.0119653
- Aryal, N., Regmi, P. R., & Mudwari, N. R. (2012). Violence against women living with HIV: A cross sectional study in Nepal. Global Journal of Health Science, 4(3), 117. https://doi.org/10.5539/gjhs.v4n3p117
- Ashaba, S., Kaida, A., Coleman, J. N., Burns, B. F., Dunkley, E., O'Neil, K., Kastner, J., Sanyu, N., Akatukwasa, C., Bangsberg, D. R., Matthews, L. T., & Psaros, C. (2017). Psychosocial challenges facing women living with HIV during the perinatal period in rural Uganda. PLoS ONE, 12(5), e0176256. https://doi.org/10.1371/journal.pone.0176256
- Boesten, J., & Poku, N. K. (2013). Gender and HIV/AIDS: Critical perspectives from the developing world. Ashgate Publishing, Ltd.
- Campbell, J. C., Baty, M., Ghandour, R. M., Stockman, J. K., Francisco, L., & Wagman, J. (2008). The intersection of intimate partner violence against women and HIV/AIDS: A review. International Journal of Injury Control and Safety Promotion, 15(4), 221–231. https://doi.org/10.1080/17457300802423224
- Chakraborty, H., Patted, S., Gan, A., Islam, F., & Revankar, A. (2016). Determinants of intimate partner violence among HIV-positive and HIV-negative women in India. Journal of Interpersonal Violence, 31(3), 515–530. https://doi.org/10.1177/0886260514555867
- Chilemba, W., van Wyk, N., & Leech, R. (2014). Experiences of emotional abuse Among women living With HIV and AIDS in Malawi. Health Care for Women International, 35(7-9), 743–757. https://doi.org/10.1080/07399332.2014.926901
- Colombini, M., James, C., Ndwiga, C., Team, I., & Mayhew, S. H. (2016). The risks of partner violence following HIV status disclosure, and health service responses: Narratives of women attending reproductive health services in Kenya. Journal of the International Aids Society, 19(1), 20766. https://doi.org/10.7448/IAS.19.1.20766
- Conrad, P. (1992). Medicalization and social control. Annual Review of Sociology, 18(1), 209–232. https://doi.org/10.1146/annurev.so.18.080192.001233
- Derose, K. P., Payan, D. D., Fulcar, M. A., Terrero, S., Acevedo, R., Farias, H., & Palar, K. (2017). Factors contributing to food insecurity among women living with HIV in the Dominican Republic: A qualitative study. PLoS ONE, 12(7), e0181568. https://doi.org/10.1371/journal.pone.0181568
- Earnshaw, V. A., & Chaudoir, S. R. (2009). From conceptualizing to measuring HIV stigma: A review of HIV stigma mechanism measures. Aids and Behavior, 13(6), 1160–1177. https://doi.org/10.1007/s10461-009-9593-3
- Ekstrand, M. L., Bharat, S., Ramakrishna, J., & Heylen, E. (2012). Blame, symbolic stigma and HIV misconceptions are associated with support for coercive measures in urban India. Aids and Behavior, 16(3), 700–710. https://doi.org/10.1007/s10461-011-9888-z
- Emusu, D., Ivankova, N., Jolly, P., Kirby, R., Foushee, H., Wabwire-Mangen, F., Katongole, D., & Ehiri, J. (2009). Experience of sexual violence among women in HIV discordant unions after voluntary HIV counselling and testing: A qualitative critical incident study in Uganda. AIDS Care, 21(11), 1363–1370. https://doi.org/10.1080/09540120902883077
- Ezeanochie, M. C., Olagbuji, B. N., Ande, A. B., Kubeyinje, W. E., & Okonofua, F. E. (2011). Prevalence and correlates of intimate partner violence against HIV-seropositive pregnant women in a Nigerian population. Acta Obstetricia et Gynecologica Scandinavica, 90(5), 535–539. https://doi.org/10.1111/j.1600-0412.2011.01083.x
- Ezechi, O. C., Gab-Okafor, C., Onwujekwe, D. I., Adu, R. A., Amadi, E., & Herbertson, E. (2009). Intimate partner violence and correlates in pregnant HIV positive Nigerians. Archives of Gynecology and Obstetrics, 280(5), 745–752. https://doi.org/10.1007/s00404-009-0956-9
- Fiorentino, M., Sagaon-Teyssier, L., Ndiaye, K., Suzan-Monti, M., Mengue, M. T., Vidal, L., Kuaban, C., March, L., Laurent, C., Spire, B., Boyer, S., Kuaban, C., Vidal, L., Maradan, G., Ambani, A., Ndalle, O., Momo, P., Tong, C., Boyer, V., … Grp, E. V. S. (2019). Intimate partner violence against HIV-positive Cameroonian women: Prevalence, associated factors and relationship with antiretroviral therapy discontinuity—results from the ANRS-12288 EVOLCam survey. Women's Health, (15), 1–15. https://doi.org/10.1177/1745506519848546
- Gielen, A. C., McDonnell, K. A., Burke, J. G., & O'Campo, P. (2000). Women's lives after an HIV-positive diagnosis: Disclosure and violence. Maternal and Child Health Journal, 4(2), 111–120. https://doi.org/10.1023/A:1009522321240
- Gielen, A. C., O'Campo, P., Faden, R. R., & Eke, A. (1997). Women's disclosure of HIV status: Experiences of mistreatment and violence in an urban setting. Women & Health, 25(3), 19–31. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=9273981 https://doi.org/10.1300/J013v25n03_02
- Goffman, E. (1963). Stigma: Notes on the management of spoiled identity. Prentice Hall.
- Gough, D. (2015). Qualitative and mixed methods in systematic reviews. Systematic Reviews, 4(1), 1–3. https://doi.org/10.1186/s13643-015-0151-y
- Grant, M. J., & Booth, A. (2009). A typology of reviews: An analysis of 14 review types and associated methodologies. Health Information & Libraries Journal, 26(2), 91–108. https://doi.org/10.1111/j.1471-1842.2009.00848.x
- Greig, A., Peacock, D., Jewkes, R., & Msimang, S. (2008). Gender and AIDS: Time to act. Aids (london, England), 22(Suppl 2(Suppl 2)), S35–S43. https://doi.org/10.1097/01.aids.0000327435.28538.18
- Hardy, Y. O., Antwi, P. K., Agbeno, E. K., Yifieyeh, A. C., Enimil, A., & Afful, B. A. (2020). Determinants of post-disclosure violence among women living with HIV in sero-discordant unions in kumasi, Ghana: A cross-sectional study. AIDS Care, 187–191. https://doi.org/10.1080/09540121.2020.1724256
- Hatcher, A. M., Stockl, H., Christofides, N., Woollett, N., Pallitto, C. C., Garcia-Moreno, C., & Turan, J. M. (2016). Mechanisms linking intimate partner violence and prevention of mother-to-child transmission of HIV: A qualitative study in South Africa. Social Science & Medicine, 168, 130–139. https://doi.org/10.1016/j.socscimed.2016.09.013
- Hatcher, A. M., Woollett, N., Pallitto, C. C., Mokoatle, K., Stockl, H., MacPhail, C., Delany-Moretlwe, S., & Garcia-Moreno, C. (2014). Bidirectional links between HIV and intimate partner violence in pregnancy: Implications for prevention of mother-to-child transmission. Journal of the International Aids Society, 17(1), 19233. https://doi.org/10.7448/IAS.17.1.19233
- Herek, G. M. (1999). Aids and stigma. American Behavioral Scientist, 42(7), 1106–1116. https://doi.org/10.1177/0002764299042007004
- Herek, G. M. (2002). Thinking about AIDS and stigma: A psychologist's perspective. Journal of Law, Medicine & Ethics, 30(4), 594–607. https://doi.org/10.1111/j.1748-720X.2002.tb00428.x
- Hershow, R. B., Bhadra, M., Mai, N. V. T., Sripaipan, T., Ha, T. V., & Go, V. F. (2017). A qualitative study With women living With HIV on perceived gender norms and experiences of intimate partner violence in northern Vietnam. Journal of Interpersonal Violence, 5905. https://doi.org/10.1177/0886260517724834
- Holzemer, W. L., Uys, L., Makoae, L., Stewart, A., Phetlhu, R., Dlamini, P. S., Greeff, M., Kohi, T. W., Chirwa, M., & Cuca, Y. (2007). A conceptual model of HIV/AIDS stigma from five African countries. Journal of Advanced Nursing, 58(6), 541–551. https://doi.org/10.1111/j.1365-2648.2007.04244.x
- Hong, Q. N., Pluye, P., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P., Gagnon, M.-P., Griffiths, F., & Nicolau, B. (2018). Mixed methods appraisal tool (MMAT), version 2018. Registration of Copyright, 10, 1148552.
- Hyginus, E., Chukwuemeka, I., Lawrence, I., & Sunday, M. (2012). HIV-related intimate partner violence among pregnant women in Nigeria. East African Journal of Public Health, 9(1), 29–32. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med9&NEWS=N&AN=23120946
- Iliyasu, Z., Abubakar, I. S., Babashani, M., & Galadanci, H. S. (2011). Domestic violence among women living with HIV/AIDS in kano, northern Nigeria. African Journal of Reproductive Health, 15(3), 41–49. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med8&NEWS=N&AN=22574491
- Jiwatram-Negron, T., El-Bassel, N., Primbetova, S., & Terlikbayeva, A. (2018). Gender-Based violence Among HIV-positive women in Kazakhstan: Prevalence, types, and associated risk and protective factors. Violence Against Women, 24(13), 1570–1590. https://doi.org/10.1177/1077801217741218
- Kabwama, S. N., Bukenya, J., Matovu, J. K. B., Gwokyalya, V., Makumbi, F., Beyeza-Kashesya, J., Mugerwa, S., Bwanika, J. B., & Wanyenze, R. K. (2019). Intimate partner violence among HIV positive women in care - results from a national survey, Uganda 2016. BMC Women's Health, 19(1), 130. https://doi.org/10.1186/s12905-019-0831-1
- Kalokhe, A. S., Potdar, R. R., Stephenson, R., Dunkle, K. L., Paranjape, A., Del Rio, C., & Sahay, S. (2015). How well does the world health organization definition of domestic violence work for India? PLoS ONE, 10(3), e0120909. https://doi.org/10.1371/journal.pone.0120909
- Kennedy, C. E., Haberlen, S., Amin, A., Baggaley, R., & Narasimhan, M. (2015). Safer disclosure of HIV serostatus for women living with HIV who experience or fear violence: A systematic review. Journal of the International Aids Society, 18, 20292. https://doi.org/10.7448/IAS.18.6.20292
- Knettel, B. A., Minja, L., Chumba, L. N., Oshosen, M., Cichowitz, C., Mmbaga, B. T., & Watt, M. H. (2019). Serostatus disclosure among a cohort of HIV-infected pregnant women enrolled in HIV care in moshi, Tanzania: A mixed-methods study. SSM - Population Health, 7, 100323. https://doi.org/10.1016/j.ssmph.2018.11.007
- Koenig, L. J., Whitaker, D. J., Royce, R. A., Wilson, T. E., Callahan, M. R., Fernandez, M. I., & Perinatal Guidelines Evaluation Project, G. (2002). Violence during pregnancy among women with or at risk for HIV infection. American Journal of Public Health, 92(3), 367–370. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=11867312 https://doi.org/10.2105/AJPH.92.3.367
- Kouyoumdjian, F. G., Findlay, N., Schwandt, M., & Calzavara, L. M. (2013). A systematic review of the relationships between intimate partner violence and HIV/AIDS. PLoS ONE, 8(11), e81044. https://doi.org/10.1371/journal.pone.0081044
- Logie, C. H., James, L., Tharao, W., & Loutfy, M. R. (2011). Hiv, gender, race, sexual orientation, and sex work: A qualitative study of intersectional stigma experienced by HIV-positive women in ontario, Canada. PLoS Medicine, 8(11), e1001124. https://doi.org/10.1371/journal.pmed.1001124
- Maher, J. E., Peterson, J., Hastings, K., Dahlberg, L. L., Seals, B., Shelley, G., & Kamb, M. L. (2000). Partner violence, partner notification, and women's decisions to have an HIV test. JAIDS Journal of Acquired Immune Deficiency Syndromes, 25(3), 276–282. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=11115959 https://doi.org/10.1097/00126334-200011010-00012
- Malaju, M. T., & Alene, G. D. (2013). Women's expectation of partner's violence on HIV disclosure for prevention of mother to child transmission of HIV in north west Ethiopia. BMC Research Notes, 6(1), 96. https://doi.org/10.1186/1756-0500-6-96
- Maman, S., Campbell, J., Sweat, M. D., & Gielen, A. C. (2000). The intersections of HIV and violence: Directions for future research and interventions. Social Science & Medicine, 50(4), 459–478. https://doi.org/10.1016/S0277-9536(99)00270-1
- Maman, S., Groves, A. K., McNaughton Reyes, H. L., & Moodley, D. (2016). Diagnosis and disclosure of HIV status: Implications for women's risk of physical partner violence in the postpartum period. JAIDS Journal of Acquired Immune Deficiency Syndromes, 72(5), 546–551. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=psyc13&NEWS=N&AN=2016-36772-012 https://doi.org/10.1097/QAI.0000000000001012
- Marais, A., Kuo, C. C., Julies, R., Stein, D. J., Joska, J. A., & Zlotnick, C. (2019). “If he’s abusing You . . . The baby Is going to Be affected”: HIV-positive pregnant women’s experiences of intimate partner violence. Violence Against Women, 25(7), 839–861. https://doi.org/10.1177/1077801218802640
- Matseke, G., Rodriguez, V. J., Peltzer, K., & Jones, D. (2016). Intimate partner violence among HIV positive pregnant women in South Africa. Journal of Psychology in Africa, 26(3), 259–266. https://doi.org/10.1080/14330237.2016.1185912
- Mehta, K. G., Baxi, R., Patel, S., Chavda, P., & Mazumdar, V. (2019). Stigma, discrimination, and domestic violence experienced by women living with HIV: A cross-sectional study from western India. Indian Journal of Community Medicine, 44(4), 373–377. https://doi.org/10.4103/ijcm.IJCM_136_19
- Mepham, S., Zondi, Z., Mbuyazi, A., Mkhwanazi, N., & Newell, M. L. (2011). Challenges in PMTCT antiretroviral adherence in northern KwaZulu-natal, South Africa. AIDS Care, 23(6), 741–747. https://doi.org/10.1080/09540121.2010.516341
- Mitra, A., & Sarkar, D. (2011). Gender inequality and the spread of HIV-AIDS in India. International Journal of Social Economics, 38(6), 557–572. https://doi.org/10.1108/03068291111131409
- Moreno, C. L. (2007). The relationship between culture, gender, structural factors, abuse, trauma, and HIV/AIDS for latinas. Qualitative Health Research, 17(3), 340–352. https://doi.org/10.1177/1049732306297387
- Mulrenan, C., Colombini, M., Howard, N., Kikuvi, J., & Mayhew, S. H. (2015). Exploring risk of experiencing intimate partner violence after HIV infection: A qualitative study among women with HIV attending postnatal services in Swaziland. BMJ Open, 5(5), e006907. https://doi.org/10.1136/bmjopen-2014-006907
- Odiachi, A., Erekaha, S., Cornelius, L. J., Isah, C., Ramadhani, H. O., Rapoport, L., & Sam-Agudu, N. A. (2018). HIV status disclosure to male partners among rural Nigerian women along the prevention of mother-to-child transmission of HIV cascade: A mixed methods study. Reproductive Health, 15(1), 36. https://doi.org/10.1186/s12978-018-0474-y
- Ojikutu, B. O., Pathak, S., Srithanaviboonchai, K., Limbada, M., Friedman, R., Li, S., Mimiaga, M. J., Mayer, K. H., Safren, S. A., Cummings, V., Dai, J. Y., Celentano, D. D., Elharrar, V., Emel, L., Gaydos, C., Hamilton, E., Hughes, J., Kelly, C., London, A., … Waller, H. (2016). Community cultural norms, stigma and disclosure to sexual partners among women living with HIV in Thailand, Brazil and Zambia (HPTN 063). PLoS ONE, 11(5), e0153600. https://doi.org/10.1371/journal.pone.0153600
- Olowookere, S. A., Fawole, O. I., Adekanle, D. A., Adeleke, N. A., & Abioye-Kuteyi, E. A. (2015). Patterns and correlates of intimate partner violence to women living With HIV/AIDS in osogbo, southwest Nigeria. Violence Against Women, 21(11), 1330–1340. https://doi.org/10.1177/1077801215594889
- Onono, M. A., Cohen, C. R., Jerop, M., Bukusi, E. A., & Turan, J. M. (2014). HIV serostatus and disclosure: Implications for infant feeding practice in rural south nyanza, Kenya. Bmc Public Health, 14(1), Article 390. https://doi.org/10.1186/1471-2458-14-390
- Orza, L., Bewley, S., Chung, C., Crone, E. T., Nagadya, H., Vazquez, M., & Welbourn, A. (2015). “Violence. Enough already”: findings from a global participatory survey among women living with HIV. Journal of the International Aids Society, 18, 20285–20273. https://doi.org/10.7448/ias.18.6.20285
- Osinde, M. O., Kaye, D. K., & Kakaire, O. (2011). Intimate partner violence among women with HIV infection in rural Uganda: Critical implications for policy and practice. BMC Women's Health, 11(1), 50. https://doi.org/10.1186/1472-6874-11-50
- Parker, R., & Aggleton, P. (2003). Hiv and AIDS-related stigma and discrimination: A conceptual framework and implications for action. Social Science & Medicine, 57(1), 13–24. https://doi.org/10.1016/S0277-9536(02)00304-0
- Pluye, P., & Hong, Q. N. (2014). Combining the power of stories and the power of numbers: Mixed methods research and mixed studies reviews. Annual Review of Public Health, 35(1), 29–45. https://doi.org/10.1146/annurev-publhealth-032013-182440
- Pool, R., Nyanzi, S., & Whitworth, J. A. (2001). Attitudes to voluntary counselling and testing for HIV among pregnant women in rural south-west Uganda. AIDS Care, 13(5), 605–615. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=11571007 https://doi.org/10.1080/09540120120063232
- Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., Britten, N., Roen, K., & Duffy, S. (2006). Guidance on the conduct of narrative synthesis in systematic reviews. A Product from the ESRC Methods Programme Version, 1, b92.
- Ramlagan, S., Sifunda, S., Peltzer, K., Jean, J., & Ruiter, R. A. C. (2019). Correlates of perceived HIV-related stigma among HIV-positive pregnant women in rural mpumalanga province, South Africa. Journal of Psychology in Africa, 29(2), 141–148. https://doi.org/10.1080/14330237.2019.1603022
- Rice, W. S., Logie, C. H., Napoles, T. M., Walcott, M., Batchelder, A. W., Kempf, M.-C., Wingood, G. M., Konkle-Parker, D. J., Turan, B., Wilson, T. E., Johnson, M. O., Weiser, S. D., & Turan, J. M. (2018). Perceptions of intersectional stigma among diverse women living with HIV in the United States. Social Science & Medicine, 208, 9–17. https://doi.org/10.1016/j.socscimed.2018.05.001
- Rujumba, J., Neema, S., Byamugisha, R., Tylleskär, T., Tumwine, J. K., & Heggenhougen, H. K. (2012). “Telling my husband I have HIV is too heavy to come out of my mouth”: pregnant women's disclosure experiences and support needs following antenatal HIV testing in eastern uganda. Journal of the International Aids Society, 15(2), 17429. https://doi.org/10.7448/IAS.15.2.17429
- Shamu, S., Zarowsky, C., Shefer, T., Temmerman, M., & Abrahams, N. (2014). Intimate partner violence after disclosure of HIV test results among pregnant women in Harare, Zimbabwe. PLoS ONE, 9(10), e109447. https://doi.org/10.1371/journal.pone.0109447
- Turan, J. M., Bukusi, E. A., Onono, M., Holzemer, W. L., Miller, S., & Cohen, C. R. (2011). HIV/AIDS stigma and refusal of HIV testing Among pregnant women in rural Kenya: Results from the MAMAS study. Aids and Behavior, 15(6), 1111–1120. https://doi.org/10.1007/s10461-010-9798-5
- Turan, J. M., Hatcher, A. M., Romito, P., Mangone, E., Durojaiye, M., Odero, M., & Camlin, C. S. (2016). Intimate partner violence and forced migration during pregnancy: Structural constraints to women's agency. Global Public Health, 11(1-2), 153–168. https://doi.org/10.1080/17441692.2015.1030684
- Turan, J. M., & Nyblade, L. (2013). HIV-related stigma as a barrier to achievement of Global PMTCT and maternal health goals: A review of the evidence. Aids and Behavior, 17(7), 2528–2539. https://doi.org/10.1007/s10461-013-0446-8
- WHO. (2005). Who multi-country study on women's health and domestic violence against women: Initial results on prevalence, health outcomes and women's responses. World Health Organization.
- WHO. (2017). Violence against women. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
- WHO. (2019). Global Health Observatory (GHO) data. https://www.who.int/gho/hiv/en/
- Zamudio-Haas, S., Mudekunye-Mahaka, I., Lambdin, B. H., & Dunbar, M. S. (2012). If, when and how to tell: A qualitative study of HIV disclosure among young women in Zimbabwe. Reproductive Health Matters, 20(SUPPL. 39), 18–26. https://doi.org/10.1016/S0968-8080(12)39637-7
- Zunner, B., Dworkin, S. L., Neylan, T. C., Bukusi, E. A., Oyaro, P., Cohen, C. R., Abwok, M., & Meffert, S. M. (2015). Hiv, violence and women: Unmet mental health care needs. Journal of Affective Disorders, 174, 619–626. doi:10.1016/j.jad.2014.12.017
