
ABSTRACT
We conducted a multicentre observational study in people living with HIV (PLHIV) on antiretroviral therapy in Alicante (Spain) from 2019 to 2020 aiming to analyse the prevalence of abuse and assess treatment adherence according to this variable. We used the Abuse Assessment Screen tool, the simplified medication adherence questionnaire and the medication possession ratio to assess outcomes.. Of the 161 included PLHIV, 53 (32.9%) had suffered abuse (27 emotional abuse, 6 physical abuse, 3 sexual abuse, 13 emotional and physical abuse, 4 unknown type). Seven (4.3%) had suffered abuse in the last year (5 emotional, 2 physical). Abuse had lasted a median of 48 months (interquartile range 12–81). HIV status was considered as a cause of violence by 9.4% of victims. In the multivariable analysis, only abuse was independently associated with non-adherence [adjusted odds ratio (aOR) 3.92; 95% confidence interval (CI) 1.80–8.84; p = 0.0007]. Abuse (aOR 6.14; 95% CI 1.63–27.70; p = 0.001) and previous incarceration (aOR 15.08 95% CI 2.71–104.71; p = 0.003) were associated with detectable viral load. In conclusion, the prevalence of abuse is high in PLHIV, hampering adherence and virological success. Abuse screening tools should be incorporated into routine HIV care.
Introduction
Both domestic violence and HIV infection are major public health problems. In Spain, there are an estimated 130,000–160,000 people living with HIV (PLHIV), with a rate of new diagnoses of 7.46 per 100,000 inhabitants in 2019, higher than the European Union average (Área de Vigilancia de VIH y Comportamientos de Riesgo, Citationn.d.).
Domestic violence (DV) is any form of violence inflicted by people in the family environment and is generally directed at the most vulnerable members of the family. DV is often used as a synonym for intimate partner violence (IPV), which is committed by a spouse, partner or ex-partner in an intimate relationship. But in its broadest sense, DV encompasses violence against children, parents and the elderly. It takes a number of forms, including physical aggression, sexual coercion, psychological abuse and controlling behaviours.
Globally, the victims of domestic violence are overwhelmingly women, and women also tend to experience more severe forms of violence. According to Spanish law, gender-based violence (GBV) is defined as “specific violence against women, used as an instrument to maintain discrimination, inequality and power relations of men over women and that is exercised by the spouses or those who have been linked to women by emotional relationships”. It can, therefore, be exercised not only by the partner or ex-partner, but also by uncles, brothers, children or other relatives. The prevalence of GBV in women is high worldwide. Global estimates published by the World Health Organization (WHO) indicate that about 1 in 3 (35%) women worldwide have experienced either physical and/or sexual intimate partner violence or non-partner sexual violence in their lifetime (WHO et al., Citation2013). In a study carried out in Spain in 10,322 women at primary care centres, the prevalence of GBV was 24.8% and increased in women with the poorest educational level and lower incomes (Ruiz-Pérez et al., Citation2017). In 2020 alone, there were 150,804 complaints in Spanish courts for GBV, and 45 women died at the hands of a man they knew (Government Delegation against Gender Violence, Citation2020).
On the other hand, DV appears to be at least as prevalent in the collective of men who have sex with men (MSM) as in heterosexual women (Rebollo & Gómez, Citation2011). However, there is no standardised definition of DV against MSM, and it seems to be even more underdiagnosed than IPV among heterosexual couples (Rebollo & Gómez, Citation2011). One systematic review estimated a prevalence of 29.7–78.0%, with physical violence standing out as the most frequent type (11.8–45.1%), followed by sexual abuse (5.0–30.7%) (C. Finneran & Stephenson, Citation2013). Psychological violence has been much less studied, and the prevalence may be anywhere from 5.4 to 73.2% (C. Finneran & Stephenson, Citation2013). In studies carried out mainly in the United States, the risk of suffering DV appears to be higher in Black MSM and MSM with a lower educational level; living with HIV doubles the risk (Catherine Finneran & Stephenson, Citation2014).
People living with HIV/AIDS are especially vulnerable to DV (Warren-Gash et al., Citation2016). Moreover, DV can be a direct cause of acquiring HIV infection. Women living with HIV carry a particularly high risk of suffering GBV. In a multicentre study of 945 HIV-positive women from 94 countries, 89.0% of the 480 women who completed the questionnaire had suffered or feared GBV (Narasimhan et al., Citation2016). In a study conducted in Scotland, the frequency was somewhat lower, with 50% of HIV-positive women experiencing GBV at some point and 13.5% suffering it at the time of screening; only 15.7% of the cohort had previously been questioned about GBV (Wielding & Scott, Citation2017). A recent review by Pantalone et al. on the prevalence of IPV in PLHIV estimated the lifetime frequency of physical violence at 26–62% in women and 15–39% in MSM. For sexual violence, the figures were 22–44% and 8–33%, respectively, and for psychological abuse, 55 and 22–73% (Pantalone et al., Citation2014). The review found strong and consistent associations with poor mental health, risk behaviours for health and non-adherence to antiretroviral medication in both groups (Pantalone et al., Citation2014).
Despite the existing evidence, screening for IPV is not routinely performed in HIV clinics. In Spain, to the best of our knowledge, there are no data on the prevalence of IPV or DV in people living with HIV or on its association with ART adherence and virological control.
Our aim was to describe the 12-month and lifetime prevalence of gender-based and domestic violence in people living with HIV in Spain and to assess the association between current or past gender-based and domestic violence and virological failure or ART adherence. The overarching objective is to understand and raise the visibility of this problem, support people who suffer from abuse, improve their health, and inform the design of prevention and early detection programmes adapted to this group.
Methods
Study design and participants
This multicentre, cross-sectional study was based on a systematic abuse screening programme in people living with HIV who attended the outpatient HIV clinics of three hospitals in the province of Alicante, Spain (Hospital Vega Baja, Hospital General Universitario de Elche y Hospital General Universitario de Elda) from February 2019 to January 2020. The centres collectively covered a catchment area of about 650,000 inhabitants and followed around 1300 HIV-positive patients.
Inclusion criteria were: aged 18 years or older, confirmed HIV infection (Western blot and/or PCR positive), and under antiretroviral treatment for at least 12 months. All participants agreed to take part and signed informed consent. Patients were excluded if they refused to answer the questions about gender-based and domestic violence or if they were incarcerated.
This is an exploratory study, as prevalence of abuse in the HIV population in Spain is unknown. Therefore, we did not specify a sample size and decided to include patients consecutively for a year.
The Abuse Assessment Screen (AAS) questionnaire (Rabin et al., Citation2009) was used to screen participants (Supplemental Material). An electronic form of the questionnaire was available at the clinics (SIVIO: Information System for the detection and action against gender/domestic violence in adults) of the Valencian Health Agency. If the patient screened positive, the Danger Assessment questionnaire (Supplemental Material) was completed for risk assessment, and the regional protocol for healthcare assistance to gender violence was followed (Escribá Agüir et al., Citation2009). For the Danger Assessment questionnaire, a score ≥4 points was considered as an extreme danger of homicide or suicide. In addition, all participants were asked additional questions about the serological status of the abuser and their opinion about whether their HIV serostatus was a motivating factor in the abuse. Adherence was evaluated using two tools: first, every participant was asked to complete a Simplified Medication Adherence Questionnaire (SMAQ) (Supplemental Material); patient was considered as non-adherent if answered non-adherently to any of the questions. Secondly, a pharmacist reviewed the dispensing record of each patient in the year prior to inclusion to calculate the medication possession rate (MPR), that is, the number of days of medication dispensed divided by the number of days between dispensations per hundred (Gross et al., Citation2006). Patient was considered as non-adherent if MPR was below 95%.
Variables
Clinical and epidemiological variables collected were age, sex assigned at birth (male/female/intersexual), gender (men/women/non-binary), pregnancy, date and place of birth, migration status, alcohol and tobacco consumption, date of HIV diagnosis, CD4 nadir, baseline viral load, ART start date, transmission group, imprisonment, educational level, and employment status. Screening results for past or present abuse (in the last 12 months) were registered as negative, possible or positive. We also recorded the type of abuse (emotional, physical, sexual or other), person committing abuse and their serological status, time suffering violence, the survivor’s perception of whether their serological status was a motivator of violence, and previous abuse screenings in the SIVIO application. For positive cases, results of the Danger Assessment questionnaire (Campbell et al., Citation2009) score were also registered.
Plasma viral load and CD4 lymphocyte count at the time of screening were included, as were previous or current virological failures (two consecutive determinations of plasma viral load of more than 50 copies/mL more than 24 weeks after the start of ART), ART abandonment (voluntary ART interruption by the patient for more than one month) and the number of missed visits.
Data collection
Study data were collected and managed using REDCap electronic data capture tools hosted at the Seimc Gesida Foundation server. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources.
Statistical analysis
Data were analysed using R statistical software (R Core Team, Citation2019). Categorical data were compared using the χ2 test and Fisher’s exact test when necessary. Continuous variables were compared using the Mann-Whitney U test for non-parametric data and the student’s t test for variables following a normal distribution. A multivariable analysis was carried out using logistic regression. P values of less than 0.05 were considered to be statistically significant.
The performance and reporting of the study comply with STROBE guidelines (von Elm et al., Citation2007).
Ethical aspects/protection of the participating subjects
The study was approved by the Clinical Research Ethics Committees of both the Elda and Elche General University Hospitals.
All doctors and nurses participating in the study received prior training on gender and domestic violence to ensure good knowledge of the protocol and intervention plan, as well as the resources available for the possible or confirmed cases detected.
The study was carried out in accordance with the Declaration of Helsinki, the rules of Good Clinical Practice and the Spanish legislation regarding this type of study. Clinical information was anonymised. All participants signed their informed consent prior to their inclusion in the study.
Results
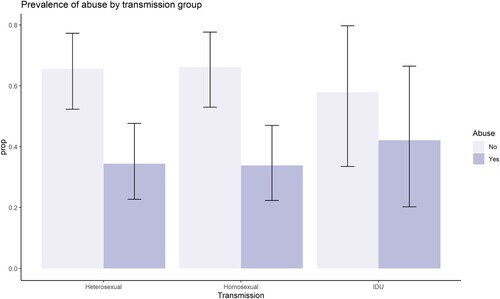
Of the 164 HIV-infected adults invited to participate, 161 accepted and were included (104 men and 57 women). Fifty-three patients (32.9%) had suffered abuse in their lifetime (27 emotional abuse, 6 physical abuse, 3 sexual abuse, 13 emotional and physical abuse, 4 unknown type). Seven (4.3%) had suffered abuse in the last year (5 emotional, 2 physical), and three (1.9%) were being abused at the time of enrolment, one considered at high risk according to the Danger Assessment questionnaire. Two other patients were screened as possible cases because health staff suspected abuse, but patients did not admit to/recognise it. In total, 42.1% of women had suffered abuse [95% confidence interval (CI) 28.1–55%] compared to 25.9% of men (95% CI 17.8–35.5%). shows the prevalence of abuse according to the HIV transmission risk group.
Figure 1. Prevalence of abuse according to HIV transmission risk group. IDU: injection drug users.
The median duration of abuse was 48 months [interquartile range (IQR) 12–81]. The serological status of the abuser was positive in eight cases, negative in 30 and unknown in 15 The victim’s HIV status was perceived as a motivator of violence by 9.4% (5/53) of the survivors. There were 66 perpetrators: 59 men and 7 women. The types of abuse and perpetrators are shown in .
Table 1. Types of abuse and perpetrators according to victims’ gender and sexual orientation.
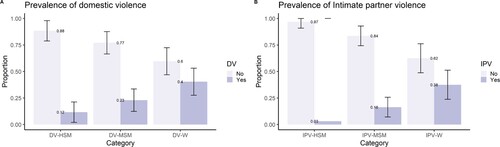
In women, the prevalence of GBV was 35.1% (95% CI 22.91–48.9%) and of DV, 40.4% (95% CI 27.6–53.1%). The overall prevalence of IPV in all participants was 19.3% (95% CI 13.5–26.2%). Among MSM, the prevalence of DV was 23.0% (95% CI 12.4–33.5%), and in heterosexual men, 11.6% (95% CI 2.0–21.2%) ().
Figure 2. Prevalence of domestic violence (2a) and intimate partner violence (2b), by gender and sexual orientation. DV: domestic violence; IPV: intimate partner violence; HSM: heterosexual men; MSM: men who have sex with men; W: women.
Five women had been previously screened for abuse (3.1%): four at their health centre and one at the hospital. Three were classified as positive cases and two as negative.
compares participants who had versus had not suffered abuse. Abused patients had significantly worse adherence (56.7 vs 25.9% were considered as non-adherent by MPR, p < 0.001), and a higher proportion presented a detectable viral load [20.8 vs 4.6%; odds ratio (OR) 5.33, 95% CI 1.59–20.81; p = 0.003].
Table 2. Bivariable analysis of factors associated with abuse.
In multivariable analysis, baseline patient characteristics associated with abuse were woman gender [adjusted odds ratio (aOR) 3.91, 95% CI 1.42–12.23; p = 0.01] and illicit drug use (aOR 2.35, 95% CI 1.02–5.57; p = 0.046) (). The only factor associated with non-adherence to ART (according to medication possession rate) was abuse (aOR 3.92, 95% CI 1.80–8.84; p < 0.001), while the detectable viral load was associated with both abuse (aOR 6.14, 95% CI 1.63–27.70; p = 0.001) and previous incarceration (aOR 15.08, 95% CI 2.71–104.71; p = 0.003).
Table 3. Multivariable analysis of factors associated with abuse, non-adherence to antiretroviral therapy, and detectable viral load.
Discussion
A third of the HIV patients followed up routinely in our hospitals are survivors of abuse in their lifetime, and one in twenty had suffered from it in the previous year. Despite these numbers, only a few had ever been screened.
The acceptability of abuse screening was high in this population; only three patients declined participation. An attitude of empathy, careful listening and counselling from health staff is needed to generate the confidence that patients need to share a situation of abuse [Grupo de expertos de la Secretaría del Plan Nacional sobre el Sida (SPNS), Grupo de Estudio de Sida (GeSIDA), Citation2020]. We believe that the close, trusting relationship between HIV patients and their doctors and nurses in the HIV units creates the perfect environment to facilitate these encounters. However, better health staff training on screening approaches and case management is needed. Indeed, the WHO has highlighted the urgent need to integrate issues related to violence into clinical training so all healthcare providers understand the relationship between exposure to violence and patients’ ill health and can respond appropriately (WHO, Citation2020).
Violence against women is a global public health problem that violates the rights of women and girls, limits their participation in society, and damages their health and well-being (WHO et al., Citation2013). Globally, the prevalence of IPV and/or non-partner sexual violence among women is the lowest in the WHO European region (27.2%) and the highest in Africa and Southeast Asia. Most studies addressing GBV in HIV-positive women have been conducted in Africa, but information in Europe or North America is scarcer. In our study, 35.1% of HIV-positive women are GBV survivors, similar to a macro-survey done in our region (Subdirectorate General for Awareness Raising, Prevention and Studies on Gender Violence, Citation2020) but higher than the prevalence reported in the general population of Spanish (Ruiz-Pérez et al., Citation2017) or European women (WHO et al., Citation2013). This finding probably reflects the greater prevalence of abuse in people living with HIV. Other studies have found a bidirectional association between IPV and positive HIV serology (Durevall & Lindskog, Citation2015; Li et al., Citation2014). Although not statistically significant, in our study abuse was more frequent among migrants living with HIV, particularly women (of whom 53.3% had suffered some abuse). Detecting and addressing gender violence in this population poses special challenges and needs socially, culturally and gender-based tailored approaches.
IPV in MSM was not infrequent in our cohort, as 16% of MSM had suffered from it. However, the few studies that have tackled the problem of IPV in MSM in Spain, have reported a somehow higher prevalence (26.56–45%) (Alisesa, Citation2021) Compared to women, MSM are less frequently screened for IPV and there are fewer resources available for abuse victims. Greater visibility for this problem, combined with specific, tailored screening programmes, prevention strategies and survivors assistance programmes are needed. In a study conducted in the United States in 56 HIV-positive persons, 73% reported DV at some point in their life, 29% of whom believed it was related to their serological status (Ramachandran et al., Citation2010). Other studies on IPV in MSM emphasise that survivors of violence are more likely to suffer depression, consume addictive substances, be HIV-positive, or have unprotected anal intercourse, suggesting the need for preventive as well as early detection programmes (Buller et al., Citation2014).
Interpersonal violence has been associated with diminished access to health care and poorer health outcomes when accessed (Hawcroft et al., Citation2019; Massetti et al., Citation2018). In our study, we found an association between abuse history and poor ART outcomes, driven by suboptimal ART adherence. A systematic review and meta-analysis found that women who experienced IPV presented lower ART use, half the odds of self-reported ART adherence and significantly worsened viral suppression compared to women who did not suffer abuse (Hatcher et al., Citation2015). Recent studies have also shown how GBV worsens HIV care and antiretroviral treatment (ART) results (Biomndo et al., Citation2021; Hatcher et al., Citation2021; Mendoza et al., Citation2016) and may also hamper access to PrEP (Leddy et al., Citation2019; O’Malley et al., Citation2021). Moreover, a recent study found an association between severe IPV and all-cause mortality in HIV-positive women (Closson et al., Citation2020).
Less studied are the consequences of IPV in HIV-positive men. An observational study in 251 patients, predominantly men, found IPV to be an independent predictor of having CD4 counts of less than 200 cells/µl and a detectable viral load, while being threatened by a partner was also predictive of a high rate of missed visits (Schafer et al., Citation2012). In a Canadian study in 687 HIV-positive MSM, IPV was associated with a higher rate of clinically relevant interruptions in care, a higher incidence of AIDS among patients presenting early to care and an increased rate of HIV-related hospitalisations (Siemieniuk et al., Citation2013). A recent longitudinal study in the same country found that people living with HIV who had experienced any interpersonal violence were 36% more likely to discontinue care, 81% more likely to experience viremia, 47% more likely to experience a drop in CD4 counts below 200/µl, and 65% more likely to die compared to patients not reporting interpersonal violence over nine years of follow-up (Budd et al., Citation2021).
Our study has some limitations. It is a cross-sectional study and, as such, is subject to some bias. By its very nature, it cannot prove causation. Moreover, we did not specifically ask about sexual orientation, so the transmission risk group was used as a proxy, with the assumption that injection drug users were heterosexual. We also did not specifically address childhood abuse, which has been identified as an independent factor for bad HIV care outcomes (Budd et al., Citation2021). Another limitation derived from the study design is that it leaves a fundamental question unanswered: the interval at which screening should be performed. Longitudinal studies are necessary for assessing the incidence of abuse, the length of screening intervals and the efficacy of preventive measures. Finally, our study only included people living with HIV and therefore a direct comparison with lifetime abuse rates in the general population is not possible. We have tried to overcome this by comparing our results with those published in general Spanish population (Alisesa, Citation2021; Ruiz-Pérez et al., Citation2017). Nevertheless, we believe that a prevalence study such as ours is a necessary first step to understand the magnitude of the problem and inform the design of intervention and prevention strategies aimed at this group.
Specific abuse screening protocols and survivors assistance programmes should be designed, with a special focus on people living with HIV (Pantalone et al., Citation2012). In Spain, great progress has been made at the level of policies against gender and domestic violence, but other aspects such as the provision of services and, above all, promotion and prevention, are lagging (Goicolea et al., Citation2014). Social determinants of both health and violence must be taken into account when designing those programmes, now more than ever in light of the concurrent COVID-19 and IPV pandemics (Evans et al., Citation2020).
In conclusion, despite being frequent targets of violence, most people living with HIV followed at our clinics had never been screened for abuse. A lifetime history of abuse is associated with worse ART adherence and virological failure among HIV patients. There is an urgent need to incorporate abuse screening tools and integrate violence assessment and prevention into our routine HIV care.
Supplemental Material
Download MS Word (95.5 KB)Acknowledgments
The authors are grateful to the Seimc Gesida Foundation, and especially to Marta de Miguel Montero, for their assistance with REDCap electronic data capture tools. The authors are in debt to all VIHOLETA study participants and all staff at the Infectious Diseases Clinics of our hospitals
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Alisesa, C. (2021). Violencia intragénero Guía práctica de atención a las víctimas (pp. 1–81). Consejería de Igualdad, Políticas Sociales y Conciliación. Dirección General de Violencia de Género, Igualdad de Trato y Diversidad. https://www.juntadeandalucia.es/sites/default/files/2021-09/ViolenciaIntragénero.pdf
- Área de Vigilancia de VIH y Comportamientos de Riesgo. Vigilancia Epidemiológica del VIH y sida en España: Sistema de Información sobre Nuevos Diagnósticos de VIH y Registro Nacional de Casos de Sida. Plan Nacional sobre el Sida. (n.d.). S.G. de Promoción de la Salud y Epidemiología/Centro Nacional de Epidemiología – ISCIII. Retrieved November 21, 2017, from https://www.msssi.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/vigilancia/InformeVIH_SIDA_2016.pdf
- Biomndo, B. C., Bergmann, A., Lahmann, N., & Atwoli, L. (2021). Intimate partner violence is a barrier to antiretroviral therapy adherence among HIV-positive women: Evidence from government facilities in Kenya. PLoS ONE, 16(4), e0249813. https://doi.org/10.1371/journal.pone.0249813
- Budd, A. S., Krentz, H. B., Rubin, L. H., Power, C., Gill, M. J., & Fujiwara, E. (2021). Long-term consequences of interpersonal violence experiences on treatment engagement and health status in people living with HIV. AIDS, 35(5), 801–809. https://doi.org/10.1097/QAD.0000000000002798
- Buller, A. M., Devries, K. M., Howard, L. M., & Bacchus, L. J. (2014). Associations between intimate partner violence and health among men who have sex with men: A systematic review and meta-analysis. PLoS Medicine, 11(3), e1001609. https://doi.org/10.1371/journal.pmed.1001609
- Campbell, J. C., Webster, D. W., & Glass, N. (2009). The danger assessment: Validation of a lethality risk assessment instrument for intimate partner femicide. Journal of Interpersonal Violence, 24(4), 653–674. https://doi.org/10.1177/0886260508317180
- Closson, K., McLinden, T., Parry, R., Lee, M., Gibbs, A., Kibel, M., Wang, L., Trigg, J., Braitstein, P., Pick, N., Parashar, S., Montaner, J. S. G., Kaida, A., & Hogg, R. S. (2020). Severe intimate partner violence is associated with all-cause mortality among women living with HIV. AIDS, 34(10), 1549–1558. https://doi.org/10.1097/QAD.0000000000002581
- Durevall, D., & Lindskog, A. (2015). Intimate partner violence and HIV in ten sub-Saharan African countries: What do the demographic and health surveys tell us? The Lancet Global Health, 3(1), e34–e43. https://doi.org/10.1016/S2214-109X(14)70343-2
- Escribá Agüir, V., Royo Marqués, M., Mas Pons, R., Fullana Montoro, A., & Moreno Alonso, M. (2009). Protocolo para la atención sanitaria de la violencia de género (PDA). Generalitat. http://www.violenciagenero.msssi.gob.es/profesionalesInvestigacion/protocolosAmbitoAutonomico/sanitario/docs/Protocolo_atencion_sanitaria_Valencia.pdf
- Evans, M. L., Lindauer, M., & Farrell, M. E. (2020). A pandemic within a pandemic – intimate partner violence during COVID-19. New England Journal of Medicine, 383(24), 2302–2304. https://doi.org/10.1056/nejmp2024046
- Finneran, C., & Stephenson, R. (2013). Intimate partner violence among men who have sex with men: A systematic review. Trauma, Violence, & Abuse, 14(2), 168–185. https://doi.org/10.1177/1524838012470034
- Finneran, C., & Stephenson, R. (2014). Intimate partner violence, minority stress, and sexual risk-taking among U.S. men who have sex with men. . Journal of Homosexuality, 61(2), 288–306. https://doi.org/10.1080/00918369.2013.839911
- Goicolea, I., Vives-Cases, C., Minvielle, F., Briones-Vozmediano, E., & Ohman, A. (2014). Applying the WHO recommendations on health-sector response to violence against women to assess the Spanish health system. A mixed methods approach. Gaceta Sanitaria, 28(3), 238–241. https://doi.org/10.1016/j.gaceta.2013.08.002
- Government Delegation against Gender Violence. (2020). Statistical portal. https://estadisticasviolenciagenero.igualdad.mpr.gob.es/
- Gross, R., Yip, B., Lo Re, V., Wood, E., Alexander, C. S., Harrigan, P. R., Bangsberg, D. R., Montaner, J. S. G., & Hogg, R. S. (2006). A simple, dynamic measure of antiretroviral therapy adherence predicts failure to maintain HIV-1 suppression. The Journal of Infectious Diseases, 194(8), 1108–1114. https://doi.org/10.1086/507680
- Grupo de expertos de la Secretaría del Plan Nacional sobre el Sida (SPNS), Grupo de Estudio de Sida (GeSIDA), la Sociedad Española de Ginecología y Obstetricia. (SEGO) y la Sociedad Española de Infectología Pediátrica. (SEIP). (2020). Documento de consenso sobre la asistencia en el ámbito sanitario a las mujeres con infección por el VIH (Actualizacion Agosto 2020) (pp. 1–92). https://www.mscbs.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/documentos/Mujer_y_VIH_DEFI.pdf
- Hatcher, A. M., Brittain, K., Phillips, T. K., Zerbe, A., Abrams, E. J., & Myer, L. (2021). Longitudinal association between intimate partner violence and viral suppression during pregnancy and postpartum in South African women. AIDS, 35(5), 791–799. https://doi.org/10.1097/QAD.0000000000002796
- Hatcher, A. M., Smout, E. M., Turan, J. M., Christofides, N., & Stöckl, H. (2015). Intimate partner violence and engagement in HIV care and treatment among women: A systematic review and meta-analysis. AIDS, 29(16), 2183–2194. https://doi.org/10.1097/QAD.0000000000000842
- Hawcroft, C., Hughes, R., Shaheen, A., Usta, J., Elkadi, H., Dalton, T., Ginwalla, K., & Feder, G. (2019). Prevalence and health outcomes of domestic violence amongst clinical populations in Arab countries: A systematic review and meta-analysis. BMC Public Health, 19(1), 1. https://doi.org/10.1186/s12889-019-6619-2
- Leddy, A. M., Weiss, E., Yam, E., & Pulerwitz, J. (2019). Gender-based violence and engagement in biomedical HIV prevention, care and treatment: A scoping review. BMC Public Health, 19(1), 1. https://doi.org/10.1186/s12889-019-7192-4
- Li, Y., Marshall, C. M., Rees, H. C., Nunez, A., Ezeanolue, E. E., & Ehiris, J. E. (2014). Intimate partner violence and HIV infection among women: A systematic review and meta-analysis. Journal of the International AIDS Society, 17(1), 18845. https://doi.org/10.7448/IAS.17.1.18845
- Massetti, G. M., Townsend, J. S., Thomas, C. C., Basile, K. C., & Richardson, L. C. (2018). Healthcare access and cancer screening among victims of intimate partner violence. Journal of Women’s Health, 27(5), 607–614. https://doi.org/10.1089/jwh.2017.6402
- Mendoza, C., Barrington, C., Donastorg, Y., Perez, M., Fleming, P., Decker, M., & Kerrigan, D. (2016). Violence from a sexual partner is significantly associated with poor HIV care and treatment outcomes among female sex workers in the Dominican republic. JAIDS Journal of Acquired Immune Deficiency Syndromes, 1(3), 273–278. https://doi.org/10.1097/QAI.0000000000001250
- Narasimhan, M., Orza, L., Welbourn, A., Bewley, S., Crone, T., & Vazquez, M. (2016). Sexual and reproductive health and human rights of women living with HIV: A global community survey. Bulletin of the World Health Organization, 94(4), 243–249. https://doi.org/10.2471/BLT.14.150912
- O’Malley, T. L., Egan, J. E., Hawk, M. E., Krier, S. E., & Burke, J. G. (2021). Intimate partner violence, HIV pre-exposure prophylaxis (PrEP) acceptability, and attitudes about use: Perspectives of women seeking care at a family planning clinic. AIDS and Behavior, 25(2), 427–437. https://doi.org/10.1007/s10461-020-03003-z
- Pantalone, D. W., Rood, B. A., Morris, B. W., & Simoni, J. M. (2014). A systematic review of the frequency and correlates of partner abuse in HIV-infected women and men who partner with men. Journal of the Association of Nurses in AIDS Care, 25(1), S15–S35. https://doi.org/10.1016/j.jana.2013.04.003
- Pantalone, D. W., Schneider, K. L., Valentine, S. E., & Simoni, J. M. (2012). Investigating partner abuse among HIV-positive men who have sex with men. AIDS and Behavior, 16(4), 1031–1043. https://doi.org/10.1007/s10461-011-0011-2
- Rabin, R. F., Jennings, J. M., Campbell, J. C., & Bair-Merritt, M. H. (2009). Intimate partner violence screening tools. American Journal of Preventive Medicine, 36(5), 439–445.e4. https://doi.org/10.1016/j.amepre.2009.01.024
- Ramachandran, S., Yonas, M. A., Silvestre, A. J., & Burke, J. G. (2010). Intimate partner violence among HIV-positive persons in an urban clinic. AIDS Care, 22(12), 1536–1543. https://doi.org/10.1080/09540121.2010.482199
- R Core Team. (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.r-project.org/
- Rebollo, J., & Gómez, B. (2011). Informe sobre la situación de la violencia entre parejas del mismo sexo. In FELGTB. Federación Estatal de Lesbianas, Gais, Transexuales y Bisexuales. www.felgtb.org/ … /informe-2011-sobre-violencia-intragenero.pdf
- Ruiz-Pérez, I., Escribà-Agüir, V., Montero-Piñar, I., Vives-Cases, C., Rodríguez-Barranco, M., Plazaola-Castaño, J., Jiménez-Gutiérrez, E., Fuentes-Pujol, M., Rohlfs-Barbosa, I., Blanco-Prieto, P., Gil-González, D., Ojuel-Solsona, J., Ruiz-Jarabo Quemada, C., Millán-Susinos, R., García-Miranda, L., & Mosquera-Tenreiro, C. (2017). Prevalence of intimate partner violence in Spain: A national cross-sectional survey in primary care. Atención Primaria, 49(2), 93–101. https://doi.org/10.1016/j.aprim.2016.03.006
- Schafer, K. R., Brant, J., Gupta, S., Thorpe, J., Winstead-Derlega, C., Pinkerton, R., Laughon, K., Ingersoll, K., & Dillingham, R. (2012). Intimate partner violence: A predictor of worse HIV outcomes and engagement in care. AIDS Patient Care and STDs, 26(6), 356–365. https://doi.org/10.1089/apc.2011.0409
- Siemieniuk, R. A. C., Miller, P., Woodman, K., Ko, K., Krentz, H. B., & Gill, M. J. (2013). Prevalence, clinical associations, and impact of intimate partner violence among HIV-infected gay and bisexual men: A population-based study. HIV Medicine, 14(5), 293–302. https://doi.org/10.1111/hiv.12005
- Subdirectorate General for Awareness Raising, Prevention and Studies on Gender Violence. (2020). Government delegation against gender violence. Macro-survey on violence against women 2019 (pp. 1–341). https://ncdc.gov.ng/themes/common/docs/protocols/96_1577798337.pdf
- von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., & Vandenbroucke, J. P. (2007). The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet, 370(9596), 1453–1457. https://doi.org/10.1016/S0140-6736(07)61602-X
- Warren-Gash, C., Bartley, A., Bayly, J., Dutey-Magni, P., Edwards, S., Madge, S., Miller, C., Nicholas, R., Radhakrishnan, S., Sathia, L., Swarbrick, H., Blaikie, D., & Rodger, A. (2016). Outcomes of domestic violence screening at an acute London trust: Are there missed opportunities for intervention? BMJ Open, 6(1), e009069. https://doi.org/10.1136/bmjopen-2015-009069
- WHO. (2020). WHO | Health care for women subjected to intimate partner violence or sexual violence. WHO. http://www.who.int/reproductivehealth/publications/violence/vaw-clinical-handbook/en/
- WHO, Medicine, L. S. of H. and T., & South African Medical Research Council. (2013). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence (pp. 1–58). https://www.who.int/iris/bitstream/10665/85239/1/9789241564625_eng.pdf
- Wielding, S., & Scott, A. (2017). What women want: Social characteristics, gender-based violence and social support preferences in a cohort of women living with HIV. International Journal of STD & AIDS, 28(5), 486–490. https://doi.org/10.1177/0956462416654046
