
ABSTRACT
Posttraumatic growth (PTG) among people living with HIV (PLWH) remains an understudied and controversial topic, and several research gaps need to be filled. In our study, we focused on one such gap by implementing parallel assessment of positive (PTG) and negative changes (posttraumatic depreciation [PTD]) following trauma related to HIV diagnosis, along with measurement of resilience and HIV/AIDS stigma and socio-medical data. The study sample comprised 509 PLWH, which completed the standardized psychometric inventories measuring the study variables. The results showed an unexpected positive relationship between PTG and PTD among participants. In addition, following the person-centered approach, we observed specific PTG/PTD clusters in the study sample with different resilience and HIV/AIDS stigma levels. Our study may shed some light on understanding PTG/PTD processes among PLWH and inspire planning for effective psychological help adjusted to patients’ specific needs.
Introduction
Posttraumatic growth (PTG) is an expanding area of research for more than 20 years (Jayawickreme & Blackie, Citation2014; Tedeschi & Calhoun, Citation1996, Citation2004). Still, theoretical and methodological limitations continue to hinder progress in the field (Jayawickreme et al., Citation2021). Firstly, the use a self-report, retrospective, and one-faceted PTG scales focusing on positive changes (e.g., personal strength, quality relationships or spiritual growth) pose a risk of positive response bias (Park & Lechner, Citation2006). The answer to this issue may be bipolar PTG items allowing parallel assessment in a positive or a negative direction (Baker et al., Citation2008). This negative reflection of PTG was called posttraumatic depreciation (PTD; Cann et al., Citation2010) – a set of negative changes, such as a reduced sense of psychological adjustment, cognitive functioning, and emotional awareness (Barrington & Shakespeare-Finch, Citation2013). Paradoxically, studies indicate the independence of PTG and PTD constructs, linking them to different psychological processes with other predictors and outcomes (Barrington & Shakespeare-Finch, Citation2013; Taku et al., Citation2020). Consequently, the link between PTG and PTD is still not fully known, especially in complex trauma of chronic illness (Edmondson, Citation2014), where the initial reports of growth may be illusory or overlapping with PTD (see Kroemeke et al., Citation2017; Kunz, Joseph, et al., Citation2019, Kunz, Fellinghauer, et al., Citation2019).
The HIV diagnosis and its consequences can be classified as a traumatic event and a potential trigger of posttraumatic stress disorder (PTSD; see Neigh et al., Citation2016; Sherr et al., Citation2011). Edmondson’s model (Citation2014) can be used to describe living with HIV as a continuous process of coping with a potentially life-threatening condition. Furthermore, besides health problems PLWH face social stressors like HIV/AIDS stigma (Rueda et al., Citation2016). Although HIV infection is now a well-controlled medical condition, PLWH are invariably stigmatized and internalize the negative self-image that impairs their social functioning (Greenhalgh et al., Citation2016; Rueda et al., Citation2016; Smith et al., Citation2019). Still, despite its disadvantages, living with HIV is observed to be associated with positive changes, which comprise PTG (e.g., Cieślak et al., Citation2009; Milam, Citation2004; Ogińska-Bulik & Kraska, Citation2017). Studies linked PTG among PLWH to better mental health and treatment adherence (Garrido-Hernansaiz et al., Citation2017; Murphy & Hevey, Citation2013). Nevertheless, PTG research among PLWH shares the limitations described earlier (Rzeszutek & Gruszczyńska, Citation2018).
Number of studies have indicated the role of personality traits as predictors of PTG (see Prati & Pietrantoni, Citation2009). One such predictors is resilience defined as one’s ability to bounce back from or adapt to adversity (Smith et al., Citation2008). Still, in HIV/AIDS literature, the relationship between resilience and PTG is described as positive, negative or is not observed at all (Garrido-Hernansaiz et al., Citation2017; Garrido-Hernansaiz & Alonso-Tapia, Citation2017; Murphy & Hevey, Citation2013). To resolve this ambiguity, environmental variables, like stigmatization, need to be included in the association (Zhao et al., Citation2019). Among others, HIV/AIDS stigma may counteract adaptation by preventing, i.e., positive HIV disclosure (Greenhalgh et al., Citation2016; Smith et al., Citation2019). It was found that positive disclosure may support PTG, while negative disclosure seems to foster PTD (Taku et al., Citation2020). Finally, as the adoption of a PTG vs. PTD model may shed some light on the inconsistencies in PTG research among PLWH (Rzeszutek & Gruszczyńska, Citation2018), the person-centered perspective (O’Donnell et al., Citation2017) may allow seeing PLWH as diverse and heterogenous in the context of the analyzed variables and their predictors. This research novelty includes our study methodology may allow us to discern PTG/PTD clusters that can be differently linked to the studied variables (Pięta & Rzeszutek, Citation2021).
Current study
The first aim of our study was to explore the existence of different clusters within the sample of PLWH with respect to PTG and PTD. In other words, following the person-centered approach (O’Donnell et al., Citation2017), we wanted to identify subgroups of participants that differ regarding the perceived intensity of both PTG and PTD. The existing studies point to important differences in growth and depreciation levels in populations that experienced various traumatic events (Baker et al., Citation2008; Barrington & Shakespeare-Finch, Citation2013; Kroemeke et al., Citation2017; Taku et al., Citation2020). To find out how PTG and PTD are experienced in the sample of PLWH, we formulated the following hypothesis:
Hypothesis 1. Several subgroups of PLWH can be found that differ within perceived PTG and PTD levels. In addition, PTG and PTD are not related with each other in our sample of participants.
Hypothesis 2. Distinct clusters of PTG and PTD among PLWH can be observed, which are differently related to resilience level and HIV/AIDS stigma intensity among participants after controlling for socio-medical factors. Participants belonging to clusters with high PTG and low PTD were characterized by high levels of resilience and low levels of perceived HIV/AIDS stigma. The opposite trend can be seen for clusters with high PTD and low PTG.
The data analysis plan is represented by .
Figure 1. Data analysis plan.
Methods
Participants and procedure
In total, 509 participants with medical HIV diagnoses were recruited from the Hospital for Infectious Diseases in Warsaw by the authors of the study. The study participation was voluntary, without remuneration and required informed consent in writing. The patients could preserve their anonymity, and confidentiality was assured to the volunteers for future participation in the study project. The research proposal was approved by the local ethics committee. Also, the participants were informed about the availability of psychological care services in the institution where the study was held and were presented with the means of obtaining the summary results from the study.
The participants completed a paper-and-pencil version of the inventories along with the questionnaire for socio-medical data (see ) in the space provided by the hospital and returned the questionnaires immediately after filling that took around 20 minutes. About 85% of participants returned valid questionnaires. The study’s eligibility criteria were 18 years or more, a medical HIV infection diagnosis, and receiving antiretroviral treatment (ART). The exclusion criteria included HIV-related cognitive disorders, screened by medical doctors working in the hospital.
Table 1. Socio-demographic variables in the studied sample (N = 509).
Measures
Expanded version of the PTG and PTD Inventory (PTGDI-X; Taku et al., Citation2020)
To assess PTG and PTD levels among participants, the 50-item PTGDI-X questionnaire was used in the Polish adaptation by Zięba (see: Taku et al., Citation2020). PTGDI-X comprises positively worded items measuring domains of PTG (personal strength, relationships, possibilities, appreciation of life, spiritual change, e.g., I am more willing to express my emotions) along with the same items, but worded negatively and assessing PTD (e.g., I am less willing to express my emotions; Tedeschi et al., Citation2017). Responses were provided on a 6-point scale, ranging from 0 (I did not experience this change) to 5 (I experienced this change to a great degree). Higher scores reflected higher PTG or PTD levels. We based our study on the global PTG and PTD scores (Taku et al., Citation2020). The participants were instructed to focus on the positive or negative changes following the HIV diagnosis. The Cronbach’s alphas for the global PTG and PTD scores were satisfactory (see ).
Table 2. Descriptive statistics for the analyzed variables.
The Brief Resilience Scale (BRS)
We used the Polish adaptation of the BRS scale (Smith et al., Citation2008) by Konaszewski et al. (Citation2020) to assess resilience levels among participants. BRS consists of six items with a 5-point Likert response scale, ranging from 1 (strongly disagree) to 5 (strongly agree) (i.e., I tend to bounce back quickly after hard times). The Cronbach’s alpha for the total resilience score was satisfactory (see ).
The Berger HIV Stigma Scale (HSS)
To assess the level of HIV/AIDS stigma with the HSS inventory (Berger et al., Citation2001), the Polish adaptation by Van Damme-Ostapowicz and Sobolewski (Citation2015) was used. HSS contains 40 items to assess the degree of various aspects of HIV/AIDS stigma experienced (i.e., It is easier to avoid new friendships that worry about telling someone that I have HIV). Answers are provided on a Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). In this study, the total HIV/AIDS score was used. The Cronbach’s alpha for the total resilience score was satisfactory (see ).
Data analysis
The analysis consisted of three stages. First, descriptive statistics (skewness and kurtosis) for the analyzed variables were calculated to assess the distributions. The relationship between PTG and PTD was analyzed with Pearson correlation analysis. Second, to extract possible PTG/PTD levels, a profile cluster analysis based on the k-means method was applied (Garsons, Citation2014). The number of clusters to extract was determined based on two guidelines. The first was to extract a maximum number of clusters. The second one was not two extract clusters containing less than 5% of the current sample. The extracted clusters were evaluated in terms of socio-medical data with the use of Pearson’s chi-squared test and one-way ANOVA. Third, to assess the relationships between levels of resilience and stigma and PTG/PTD profiles, discriminant analysis based on enter method was performed. Resilience and stigma were analyzed as predictors of PTG/PTD profiles. Significance of discriminant functions was assessed with the use of Wilk’s lambda test.
Results
presents the descriptive statistics for the analyzed variables. The distribution of PTD was positively skewed and leptokurtic, while the distribution of PTG was platykurtic. However, the values of measures and kurtosis were close to the range [−1; 1] characteristic for the normal distribution. The distributions of stigma and resilience did not differ from the normal distribution in terms of skewness and kurtosis.
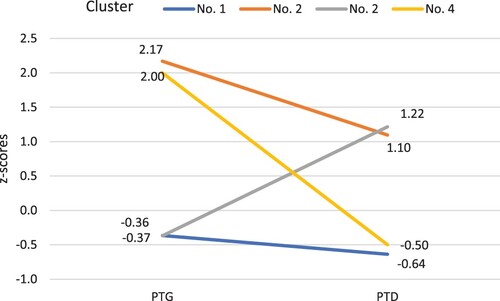
The correlation between PTG and PTD in the current study was significant and positive, but very weak, r (507) = .14, p < .01. The PTG and PTD levels were analyzed using cluster analysis based on the k-means method. Four distinct clusters were extracted. presents the standardized values of PTG and PTD in the extracted clusters. The first cluster consisted of participants (n = 256) with average levels of PTG and PTD. The second cluster consisted of participants (n = 29) with high levels of PTG and PTD. The third cluster consisted of participants (n = 125) with an average level of PTG and a high level of PTD. The fourth cluster consisted of participants (n = 36) with high levels of PTG and average levels of PTD. In total results of 446 participants were included in the cluster analysis. Participants with missing data on PTG or PTD were excluded.
Figure 2. Profiles of PTG and PTD in extracted clusters.
Note: The figure presents the standardized values of PTG and PTD in the extracted clusters.
presents the significant relationships between the sociodemographic variables and the extracted clusters.
Table 3. Statistically significant relationships between extracted clusters and socio-medical data.
In the next step of the data analysis, the levels of resilience and HIV/AIDS stigma were analyzed as predictors of distinctive PTG/PTD profiles. The analysis was based on discriminant analysis, which was used to assess the significance of possible relationships. Two significant discriminant functions were extracted. Tests for statistical significance were equal to λ = .90, χ2 (6) = 46.54, p < .001 for the first function, and to λ = .98, χ2 (2) = 7.91, p < .05 for the second function. The first function correlated highly with resilience, r = .91, p < .001, and the second one with stigma, r = .76, p < .001. The values of the discriminant function in the group centroids are depicted in .
Figure 3. Standardized values of discriminant functions representing stigma and resilience in extracted clusters.
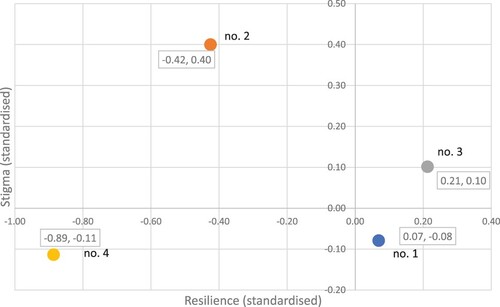
The values of resilience and stigma were average in cluster 1 (PTG-avg, PTD-avg). The participants from cluster 2 (PTG-H, PTD-H) were characterized by the highest level of stigma and the lowest level of resilience. The participants from cluster 3 (PTG-avg., PTD-H) were characterized by the highest level of resilience and an average level of stigma. The participants from cluster 4 (PTG-H, PTD-avg.) wwere characterized by a low level of resilience and an average level of stigma.
Discussion
The results were consistent with the first hypothesis up to a point. On the one hand, we observed four clusters with various levels of PTG/PTD, which may speak for the coexistence of positive and negative changes (Kroemeke et al., Citation2017). Also, the notion that PLWH is heterogenous population with respect to sociodemographic and medical characteristics was supported and can be explained by multiple social and health obstacles, i.e., belonging to a sexual minority or a substance misuse problem, that may prevent them from experiencing growth (Rzeszutek & Gruszczyńska, Citation2018).
Importantly, we failed to identify the independence of PTG and PTD. This result can be specific for health-related stress, as the positive correlation between PTG and PTD was also observed by Kunz et al.’s (Citation2017) amongst patients with spinal cord injury. Kunz, Fellinghauer, et al. (Citation2019) also showed that the PTG/PTD relationship may diminish with time. Still, PTG and PTD may be viewed as separate constructs rather than as ends of the same continuum, though this dynamic process could not be captured by a cross-sectional study.
The second hypothesis was supported to a greater extent. Clusters of PTG and PTD related differently to resilience and HIV/AIDS stigma levels after controlling for socio-medical data. We found the following clusters of participants: cluster 1 (average PTG and average PTD) with average resilience and average HIV/AIDS stigma levels; cluster 2 (high PTG and high PTD) with low resilience and high stigma levels; cluster 3 (average PTG and high PTD) with high resilience and average stigma levels; and finally, in cluster 4 (high PTG and average PTD), participants declared low resilience and average stigma levels. Our results showed complex and heterogenous patterns of adaptation to living with HIV. High PTG levels in cluster 2 coexisted with low resilience and high stigma levels and in cluster 4 with low levels of resilience and average stigma. This may point to an increased need for positive reframing among people with lower levels of overall ability to bounce back from adversity. Simultaneously, high PTD levels coexisted with low resilience and high stigma levels in cluster 2 and high resilience and average stigma levels in cluster 3, which may speak for a significant role of stigma in enhancing PTD and resistance to positively reframe the HIV diagnosis in participants with high level of resilience. In general, our results are in line with the understanding of PTG and resilience as rather different theoretical constructs (see Westphal & Bonanno, Citation2007) or even speaking for a negative relationship between PTG and resilience among PLWH (Garrido-Hernansaiz et al., Citation2017). However, coexistence of high PTG and PTD in some clusters of patients with low resilience may raise questions about the possibility of viewing PTG as reflecting positive illusions instead of real growth (Zoellner & Maercker, Citation2006). High PTD levels observed in cluster 2 could indicate the devastating effects of HIV-related stigmatization (Rueda et al., Citation2016) and are in line with more general results linking PTD and negative disclosure (Taku et al., Citation2020). Due to the social reception of HIV infection and low HIV testing rates in Poland, PLWH can be exposed to multiple losses in various areas of life (Rosińska et al., Citation2016; Skonieczna, Citation2013; Van Damme-Ostapowicz & Sobolewski, Citation2015). This situation can also be reflected in cluster 3 participants, who despite their high resilience levels, regard HIV infection as a significant burden to their lives.
Finally, regarding the role of socio-medical data, non-heterosexual participants were the most numerous in cluster 1 (neutral response to HIV), while were outnumbered in cluster 3 (least valuable; see high PTD). Presumably, this result may reflect no “stigma accumulation” among non-heterosexual PLWH (Slenders et al., Citation2014). Second, most participants with higher education were found in cluster 1 (neutral), while the least were in cluster 3 (least valuable), which may be associated with the role of social status (O’Leary et al., Citation2014).
Third, an interesting trend was associated with employment, as full employment was associated with lower PTD. However, most participants without full-time jobs were found in cluster 4 (high PTG, average PTD). This may reflect PLWHs’ tendency to switch to freelance jobs or own businesses to avoid workplace discrimination (Conyers et al., Citation2005). Finally, of the medical variables, only the time since diagnosis and ARV treatment time were associated with PTG/PTD clusters. With the more recent HIV diagnosis, we observed higher PTG and lower PTD (see cluster 3) may reflect the illusory nature of PTG change after living with HIV for a short period of time (Sawyer et al., Citation2010).
Our study has limitations, though it indicates perspectives for future research. First, the cross-sectional design precludes cause-and-effect conclusions between variables. Also, we did not measure the resilience levels of the participants before diagnosis, and they had different times since diagnosis and starting ARV treatment. Further, as a retrospective measure of PTG/PTD was implemented, received PTG/PTD scores were susceptible to biases, as is common in the PTG literature (Infurna & Jayawickreme, Citation2019).
Despite limitations, our study adds to an understanding of psychological functioning of PLWH by pointing to coexistence of positive and negative changes following diagnosis. Our study is the first to explore PTG/PTD interactions in such a large sample with control of a range of psychological and socio-medical variables. Finally, the use of the person-centered perspective is significant for planning effective psychological help and adjusting the healthcare system to PLWHs’ individual characteristics and needs (Rzeszutek & Gruszczyńska, Citation2018). Firstly, HIV/AIDS stigma may be a major source of distress for PLWH, irrespectively of individual characteristics. Secondly, it seems that interventions focused on avoiding depreciation may be of use for PLWH high in resilience, who adapt to adverse situations, rather than view them as an opportunity for growth. On the contrary, in PLWH low in resilience, it is crucial to make sure that the reported PTG is a genuine process supporting psychological well-being rather than a positive illusion that may constitute a nonadaptive way of coping with distress.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Baker, J., Kelly, C., Calhoun, L., Cann, A., & Tedeschi, R. (2008). An examination of posttraumatic growth and posttraumatic depreciation: Two exploratory studies. Journal of Loss and Trauma, 13(5), 450–465. https://doi.org/10.1080/15325020802171367
- Barrington, A., & Shakespeare-Finch, J. (2013). Working with refugee survivors of torture and trauma: An opportunity for vicarious post-traumatic growth. Counselling Psychology Quarterly, 26(1), 89–105. https://doi.org/10.1080/09515070.2012.727553
- Berger, B., Ferrans, C., & Lashley, F. R. (2001). Measuring stigma in people with HIV: Psychometric assessment of the HIV stigma scale. Research in Nursing & Health, 24(6), 518–529. https://doi.org/10.1002/nur.10011
- Cann, A., Calhoun, L. G., Tedeschi, R. G., & Solomon, D. (2010). Posttraumatic growth and depreciation as independent experiences and predictors of well-being. Journal of Loss and Trauma, 15(3), 151–166. https://doi.org/10.1080/15325020903375826
- Cieślak, R., Benight, C., Schmidt, N., Luszczynska, A., Curtin, E., Clark, R. A., & Kissinger, P. (2009). Predicting post-traumatic growth among Hurricane Katrina survivors living with HIV: The role of self-efficacy, social support, and PTSD symptoms. Anxiety, Stress and Coping, 22(4), 449–463. https://doi.org/10.1080/10615800802403815
- Conyers, L., Boomer, K. B., & McMahon, B. T. (2005). Workplace discrimination and HIV/AIDS: the national EEOC ADA research project. Work, 25(1), 37–48. https://pubmed.ncbi.nlm.nih.gov/16006674/
- Edmondson, D. (2014). An enduring somatic threat model of post-traumatic stress disorder due to acute life-threatening medical events. Social and Personality Psychology Compass, 8(3), 118–134. https://doi.org/10.1111/2Fspc3.12089
- Garrido-Hernansaiz, H., & Alonso-Tapia, J. (2017). Associations among resilience, posttraumatic growth, anxiety, and depression and their prediction from stress in newly diagnosed people living with HIV. The Journal of the Association of Nurses in AIDS Care: JANAC, 28(2), 289–294. https://doi.org/10.1016/j.jana.2016.12.005
- Garrido-Hernansaiz, H., Murphy, P., & Alonso-Tapia, J. (2017). Predictors of resilience and posttraumatic growth among people living with HIV: A longitudinal study. AIDS and Behavior, 21(11), 3260–3270. https://doi.org/10.1007/s10461-017-1870-y
- Garsons, G. (2014). Cluster analysis. Statistical.
- Greenhalgh, C., Evangeli, M., Frize, G., Foster, C., & Fidler, S. (2016). Intimate relationships in young adults with perinatally acquired HIV: A qualitative study of strategies used to manage HIV disclosure. AIDS Care, 28(3), 283–288. https://doi.org/10.1080/09540121.2015.1093594
- Infurna, F., & Jayawickreme, E. (2019). Fixing the growth illusion: New directions for research in resilience and posttraumatic growth. Current Directions in Psychological Science, 28(2), 152–158. https://doi.org/10.1177/0963721419827017
- Jayawickreme, E., & Blackie, L. (2014). Post-traumatic growth as positive personality change: Evidence, controversies, and future directions. European Journal of Personality, 28(4), 312–331. https://doi.org/10.1002/per.1963
- Jayawickreme, E., Infurna, F., Alajak, K., Blackie, L., Chopik, W., Chung, J., Dorfman, A., Fleeson, W., Forgeard, M., Frazier, P., Furr, R. M., Grossmann, I., Heller, A. S., Laceulle, O. M., Lucas, R. E., Luhmann, M., Luong, G., Meijer, L., McLean, K. C., … Zonneveld, R. (2021). Post-traumatic growth as positive personality change: Challenges, opportunities, and recommendations. Journal of Personality, 89(1), 145–165. https://doi.org/10.1111/jopy.12591
- Konaszewski, K., Niesiobędzka, M., & Surzykiewicz, J. (2020). Validation of the Polish version of the brief resilience scale (BRS). PloS One, 15(8), e0237038. https://doi.org/10.1371/journal.pone.0237038
- Kroemeke, A., Bargiel-Matusiewicz, K., & Kalamarz, M. (2017). Mixed psychological changes following mastectomy: Unique predictors and heterogeneity of post-traumatic growth and post-traumatic depreciation. Frontiers in Psychology, 8, 1245. https://doi.org/10.3389/fpsyg.2017.01245
- Kunz, S., Fellinghauer, C., & Peter, C. (2019). Measuring posttraumatic growth and depreciation after spinal cord injury: A Rasch analysis. Rehabilitation Psychology, 64(4), 407–424. https://doi.org/10.1037/rep0000288
- Kunz, S., Joseph, S., Geyh, S., & Peter, C. (2017). Posttraumatic growth and adjustment to spinal cord injury: Moderated by posttraumatic depreciation? Psychological Trauma: Theory, Research, Practice, and Policy, 9(4), 434–444. https://doi.org/10.1037/tra0000164
- Kunz, S., Joseph, S., Geyh, S., & Peter, C. (2019). Perceived posttraumatic growth and depreciation after spinal cord injury: Actual or illusory? Health Psychology, 38(1), 53–62. https://doi.org/10.1037/hea0000676
- Milam, J. (2004). Posttraumatic growth among HIV/AIDS patients. Journal of Applied Social Psychology, 34(11), 2353–2376. https://doi.org/10.1111/j.1559-1816.2004.tb01981.x
- Murphy, P., & Hevey, D. (2013). The relationship between internalized HIV-related stigma and posttraumatic growth. AIDS and Behavior, 17(5), 1809–1818. https://doi.org/10.1007/s10461-013-0482-4
- Neigh, G., Rhodes, S., Valdez, A., & Jovanovic, T. (2016). PTSD co-morbid with HIV: Separate but equal, or two parts of a whole? Neurobiology of Disease, 92, 116–123. https://doi.org/10.1016/2Fj.nbd.2015.11.012
- O’Donnell, M. L., Schaefer, I., Varker, T., Kartal, D., Forbes, D., Bryant, R. A. A., Silove, D., Creamer, M., McFarlane, A., Malhi, G., Felmingham, K., Van Hoof, M., Hadzi-Pavlovic, D., Nickerson, A., & Steel, Z. (2017). A systematic review of person-centered approaches to investigating patterns of trauma exposure. Clinical Psychology Review, 57, 208–225. https://doi.org/10.1016/j.cpr.2017.08.009
- Ogińska-Bulik, N., & Kraska, K. (2017). Posttraumatic stress disorder and posttraumatic growth in HIV-infected patients—The role of coping strategies. Health Psychology Report, 5(4), 323–332. https://doi.org/10.5114/hpr.2017.68017
- O’Leary, A., Jemmott, J. B., & Stevens, R. (2014). Optimism and education buffer the effects of syndemic conditions on HIV status among African American men who have sex with men. AIDS and Behavior, 18(11), 2080–2088. https://doi.org/10.1007/s10461-014-0708-0
- Park, C., & Lechner, S. (2006). Measurement issues in assessing growth following stressful life experiences. In L. G. Calhoun & R. G. Tedeschi (Eds.), Handbook of posttraumatic growth: Research & practice (pp. 47–67). Lawrence Erlbaum Associates Publishers.
- Pięta, M., & Rzeszutek, M. (2021). Posttraumatic growth and well-being among people living with HIV: A systematic review and meta-analysis in recognition of 40 years of HIV/AIDS. Quality of Life Research, 31(5), 1269–1288. https://doi.org/10.1007/s11136-021-02990-3
- Prati, G., & Pietrantoni, L. (2009). Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. Journal of Loss and Trauma, 14(5), 364–388. https://doi.org/10.1080/15325020902724271
- Rosińska, M., Simmons, R., Marzec-Bogusławska, A., Janiec, J., & Porter, K. (2016). Relating HIV testing patterns in Poland to risky and protective behaviour. AIDS Care, 28(4), 423–431. https://doi.org/10.1080/09540121.2015.1100702
- Rueda, S., Mitra, S., Chen, S., Gogolishvili, D., Globerman, J., Chambers, L., Wilson, M., Logie, C. H., Shi, Q., Morassaei, S., & Rourke, S. B. (2016). Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: A series of meta-analyses. BMJ Open, 6(7), e011453. https://doi.org/10.1136/bmjopen-2016-011453
- Rzeszutek, M., & Gruszczyńska, E. (2018). Posttraumatic growth among people living with HIV: A systematic review. Journal of Psychosomatic Research, 114, 81–91. https://doi.org/10.1016/j.jpsychores.2018.09.006
- Sawyer, A., Ayers, S., & Field, A. P. (2010). Post-traumatic growth and adjustment among individuals with cancer and HIV/AIDS: A meta-analysis. Clinical Psychology Review, 30(4), 436–447. https://doi.org/10.1016/j.cpr.2010.02.004
- Sherr, L., Nagra, N., Kulubya, G., Catalan, J., Clucasa, C., & Harding, R. (2011). HIV infection associated post-traumatic stress disorder and post-traumatic growth: A systematic review. Psychology, Health & Medicine, 16(5), 612–629. https://doi.org/10.1080/13548506.2011.579991
- Skonieczna, A. (2013). HIV atakuje psychikę [HIV attacks Poland]. Menedżer Zdrowia, 1, 70–72.
- Slenders, S., Sieben, I., & Verbakel, E. (2014). Tolerance towards homosexuality in Europe: Population composition, economic affluence, religiosity, same-sex union legislation and HIV rates as explanations for country differences. International Sociology, 29(4), 348–367. https://doi.org/10.1177/0268580914535825
- Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: Assessing the ability to bounce back. International Journal of Behavioral Medicine, 15(3), 194–200. https://doi.org/10.1080/10705500802222972
- Smith, C., Cook, R., & Rohleder, P. (2019). ‘When it comes to HIV, that’s when you find out the genuinity of that love’: The experience of disclosing a HIV+ status to an intimate partner. Journal of Health Psychology, 24(8), 1011–1022. https://doi.org/10.1177/1359105317691588
- Taku, K., Tedeschi, R. G., Shakespeare-Finch, J., Krosch, D., David, G., Kehl, D., Grunwald, S., Romeo, A., Di Tella, M., Kamibeppu, K., Soejima, T., Hiraki, K., Volgin, R., Dhakal, S., Zięba, M., Ramos, C., Nunes, R., Leal, I., Gouveia, P., & Calhoun, L. (2020). Posttraumatic growth (PTG) and posttraumatic depreciation (PTD) across ten countries: Global validation of the PTG-PTD theoretical model. Personality and Individual Differences. Advance online publication. https://doi.org/10.1016/j.paid.2020.110222
- Tedeschi, R., & Calhoun, L. (1996). The posttraumatic growth inventory: Measuring the positive legacy of trauma. Journal of Traumatic Stress, 9(3), 455–471. https://doi.org/10.1007/bf02103658
- Tedeschi, R., & Calhoun, L. (2004). Post-traumatic growth: Conceptual foundations and empirical evidence. Psychological Inquiry, 15(1), 1–18. https://doi.org/10.1207/s15327965pli1501_01
- Tedeschi, R., Can, A., Taku, K., Senol-Durak, K., & Calhoun, L. (2017). The posttraumatic growth inventory: A revision integrating existential and spiritual change. Journal of Traumatic Stress, 30(1), 11–18. https://doi.org/10.1002/jts.22155
- Van Damme-Ostapowicz, K., & Sobolewski, M. (2015). Cultural adaptation to Polish conditions as an element of validation of the Berger HIV stigma scale – Preliminary report. Archives of Physiotherapy and Global Research, 19(4), 21–24.
- Westphal, M., & Bonanno, G. (2007). Posttraumatic growth and resilience to trauma: Different sides of the same coin or different coins? Applied Psychology: An International Review, 56(3), 417–427. https://doi.org/10.1111/j.1464-0597.2007.00298.x
- Zhao, M., Liu, B., Zheng, T., Xu, J., Hao, Y., Wang, J., Zhang, X., Nie, W., Wang, C., Wang, F., Jiao, M., Wu, Q., & Liang, L. (2019). Factors associated with hostility among people living with HIV/AIDS in Northeast China: A cross-sectional study. BMC Public Health, 19(1), 1189. https://doi.org/10.1186/s12889-019-7526-2
- Zoellner, T., & Maercker, A. (2006). Posttraumatic growth in clinical psychology: A critical review and introduction of a two-component model. Clinical Psychology Review, 26(5), 626–653. https://doi.org/10.1016/j.cpr.2006.01.008
