
ABSTRACT
Depression is a common cause of morbidity globally and can impact adherence to medications, posing challenges to medication-based HIV prevention. The objectives of this work are to describe the frequency of depression symptoms in a cohort of 499 young women in Kampala, Uganda and to determine the association of depression symptoms with use of HIV pre-exposure prophylaxis (PrEP). Mild or greater depression, assessed by the patient health questionnaire (PHQ-9), was experienced by 34% of participants at enrollment. Participants with mild depression symptoms tended to uptake PrEP, request PrEP refills, and adhere to PrEP with similar frequency to women with no/minimal signs of depression. These findings highlight opportunities to leverage existing HIV prevention programs to identify women who may benefit from mental health services and may not otherwise be screened.
Trial registration: ClinicalTrials.gov identifier: NCT03464266..
Introduction
Depression is the most common cause of disability and morbidity globally (Depression and Other Common Mental Disorders: Global Health Estimates, Citation2017). The World Health Organization Global Burden of Disease report estimated depression to disproportionately impact women across all global regions and all age groups (Depression and Other Common Mental Disorders: Global Health Estimates, Citation2017). In some settings, gendered power dynamics, including women’s experiences with less health decision making power and access to financial resources, may limit women’s ability to seek and receive care for depression (Morgan et al., Citation2017). In addition, there is severe lack of funding for global mental health care. Data focusing on mental health in Africa are scarce (Molodynski et al., Citation2017; Sankoh et al., Citation2018) and studies from Uganda have described the prevalence of depression among fishing communities and sex workers (Fischer et al., Citation2019; Nabunya et al., Citation2021; Ssebunnya et al., Citation2019; Vancampfort et al., Citation2019), but depression among Ugandan adolescents and young adults has not been well characterized.
HIV is also a concern for adolescent girls and young women (AGYW) in many African locations and HIV prevention is a priority for public health programming. In Uganda, young cisgender women are disproportionately affected by HIV (Uganda Population-Based HIV Impact Assessment, Citation2017). While oral HIV pre-exposure prophylaxis (PrEP) medication is highly effective in preventing new HIV infections and is available in many health facilities, its effectiveness depends on daily adherence, a challenge for a preventive therapy. People experiencing depression symptoms have greater challenges adhering to medications (Mehrotra et al., Citation2016; Miller et al., Citation2021; Nakimuli-Mpungu et al., Citation2012, Citation2013; Rael et al., Citation2021; Velloza et al., Citation2018, Citation2021), owing to negative cognitive biases that result in loss of motivation (Beck, Citation2008), and depression can be exacerbated by social withdrawal, heavy alcohol use, drug use, and/or intimate partner violence (IPV) (Beck, Citation2008; Kiene et al., Citation2017; Velloza et al., Citation2018; Velloza, Kemp, et al., Citation2020). Together, these factors can deter someone from taking steps toward beneficial health interventions, such as PrEP.
While several studies have described the mental health status among women initiating PrEP, there are limited data from AGYW, particularly from Uganda. The objectives of this paper are to describe mental health status in a large cohort of young women in Kampala, Uganda initiating PrEP and to determine whether PrEP initiation, interruption, and adherence are associated with depression symptoms.
Materials and methods
Women aged 16–25 years were enrolled from May 2018 to March 2020 into the Kampala Women’s Bone Study (KWBS), an observational study of bone health among users of concurrent oral PrEP and injectable depot medroxyprogesterone acetate (DMPA, ClinicalTrials.gov #NCT03464266). Women seeking DMPA or condoms for contraception at recruiting family planning clinics, youth-based centers, and higher learning institutions were assessed for HIV risk and referred to study staff for study eligibility assessments. Women were ineligible if they were living with HIV, pregnant, using oral contraceptives, an intrauterine device (IUD), or implants, or had recently used PrEP or DMPA. Women used PrEP, DMPA, both or neither according to their preferences.
Following eligibility assessment and the informed consent process, women were enrolled, issued a unique study ID, and completed their first study visit (Heffron et al., Citation2022). Subsequent follow up visits occurred 1 month after enrollment and quarterly thereafter. During all study visits, women received individualized counseling on HIV prevention, family planning, and PrEP adherence by trained study counselors and nurses based on national guidelines. Oral PrEP, as emtricitabine/tenofovir disoproxil fumarate (FTC/TDF), was dispensed per Ugandan national guidelines (Consolidated Guidelines for Prevention and Treatment of HIV in Uganda, Citation2016). Interviewer-administered questionnaires assessed medical history, sexual behavior, sexual relationship power (Pulerwitz et al., Citation2000), contraceptive use, PrEP adherence, HIV risk self-perception and salience, physical activity and diet, alcohol and drug use, social harm, and mental health. On March 20, 2020, the Ugandan government enacted multiple restrictions to combat the COVID-19 pandemic and participants were encouraged to continue study visits over the phone until restrictions eased.
Mental health screening
Study counselors and clinicians screened women for probable depression using the patient health questionnaire (PHQ-9) administered in English or Luganda (Nakku et al., Citation2016). The PHQ-9 has been validated in many settings, including among young women in East Africa (Carroll et al., Citation2020; Kaggwa et al., Citation2022). Based on previously validated cut-offs, the PHQ-9 scores were summed and probable depression severity categories were calculated as follows: scores 0–4 are considered no/minimal, 5–9 are mild, 10–14 are moderate, 15–19 are moderately severe, and 20–27 are severe (Kroenke et al., Citation2001). For the purposes of this analysis, we combined scores of 10 or higher in a single category of moderate/severe depression. In the validation of the PHQ-9 in Luganda, the Cronbach’s alpha suggested modest to excellent validity (0.68–0.94) and a score of 5 was found to be the optimal cutoff in distinguishing probable depression (Kaggwa et al., Citation2022; Nakku et al., Citation2016). Women were referred for further counseling with an onsite psychologist if their results indicated moderate or severe depression.
PrEP adherence
In addition to self-report, we used electronic pill box devices (Wisepill Technologies, South Africa) and blood quantification of tenofovir diphosphate (TFV-DP) levels to determine PrEP adherence. Wisepill devices were provided to each woman when she initiated PrEP and women were trained to transfer pills into the pill box (Guidelines for the Use of Antiretroviral Drugs for the Treatment and Prevention of HIV in Kenya, Citation2018). These devices create a date-time stamp with each opening recorded on a web-based platform. We defined high PrEP adherence as having >80% of expected openings detected since last visit (each day was expected to have one opening) for those dispensed PrEP. Wisepill data from women who never logged pill use were included as non-adherent. Dried blood spots (DBS) were collected from PrEP users at each visit and a random sample of 10% of women were selected to have TVF-DP quantified from DBS. TFV-DP concentration >1500 fmol/punch was used as a cutoff to denote high adherence as this concentration is approximately 6–7 doses/week of FTC/TDF to correspond with the Wisepill cutoff (Castillo-Mancilla et al., Citation2013; Ibrahim et al., Citation2021).
Statistical analysis
Baseline participant characteristics were summarized for all participants, stratified by depression severity. Using the date the Ugandan government enacted COVID restrictions, we assessed the impact of COVID-19 on depression symptoms by comparing PHQ-9 scores at visits before and subsequent to the lockdown. For our primary analysis, logistic regression was used to estimate the association of declining PrEP at enrollment and depression severity. Separate models assessed the association of alcohol use, drug use, and IPV and declining PrEP at enrollment, as different exposures that may be related to mental health. To interpret the relationship between PrEP uptake and baseline alcohol use, drug use, and IPV experiences, the unadjusted odds ratio was preferable because it described the relationship of PrEP uptake with each exposure without controlling away the context of all others.
Participant-driven PrEP interruption was defined as declining PrEP refills at a follow-up visit due to participant preference, as opposed to safety determined by a clinician or other reasons. Participants who chose to stop PrEP because they became pregnant or started to breastfeed were excluded from this analysis. Separate logistic regression models with generalized estimating equations (GEE) were constructed to assess the relationship between time-dependent depression and PrEP interruption and adherence, assessed during initial 12 and 24 months after initiation. Models for PrEP adherence used Wisepill data and DBS results, separately. GEE included cumulative logit models and a multinomial distribution. Potential confounders known from previous literature to be associated with mental health and/or PrEP continuation and adherence (age, income, relationship status, years of education, DMPA dispensing at visit, having any partner who is living with HIV or of unknown HIV status, new partners, and recent condom use) (Velloza et al., Citation2018, Citation2021; HPT 067/ADAPT Study Team et al., Citation2020) were assessed for their influence on the odds ratio and retained in the adjusted model if they resulted in a ≥10% change. Follow-up data were censored at the first PrEP interruption. We assessed sensitivity and specificity of Wisepill detected adherence, using DBS as the gold-standard. SAS version 9.4 (Cary, NC) and R Studio version 1.2.1335 were used for analysis.
Ethical considerations
The study protocol was approved by the National HIV/AIDS Research Committee of Uganda (ARC 202), the Uganda National Council for Science and Technology (SS4505), and the University of Washington (STUDY00001451). All participants provided written informed consent, and those aged 16–17 years either provided assent with a consenting guardian or qualified to provide consent based on their status as an emancipated or mature minor according to local guidelines (National Guidelines for Research involving Humans as Research Participants, Citation2014).
Results
A total of 499 women were enrolled in the KWBS. The median age was 20 years (interquartile range (IQR): 18.5–21.0), 86% were single with a steady partner, 91% were not living with a partner, and 62% were unsure of their partner’s HIV status (). At the time of enrollment, most women had no/minimal (66.1%) or mild depression (24.4%). A smaller number had moderate (8.6%) or moderately severe depression (0.8%), and none had severe depression. The median PHQ-9 score was 3 (IQR: 1–3) at enrollment and 2 (IQR: 0–4) across 3756 follow-up visits, and 9 clients were missing one of the PHQ-9 items. The patterns of depression symptoms over time were dynamic for most young women (). Of the women who had no/minimal depression at baseline, 75% continued to have no/minimal detectable depression through the initial 12 months of PrEP use. Of the women who had mild depression at baseline, 55.8% of subsequent visits indicated minimal, 40.1% indicated mild, and 4.1% indicated severe depression (4% experienced mild depression consistently across their visits). All women with moderate/severe depression at baseline experienced a less severe depression category at least once over follow-up, and 37.9% of subsequent visits indicated no/minimal, 36.6% indicated mild, and 25.5% indicated moderate/severe depression. In terms of COVID-19, PHQ-9 scores among women in this cohort were on average 3.52 (median: 3, IQR: 1–5) before and 1.84 (median: 1, IQR: 1–3) after the pandemic began (Wilcoxon ranked sum p-value: < 0.0001). A total of 303 (7.1%) visits occurred telephonically during the lockdown.
Figure 1. Distribution of PHQ-9 categories over time.
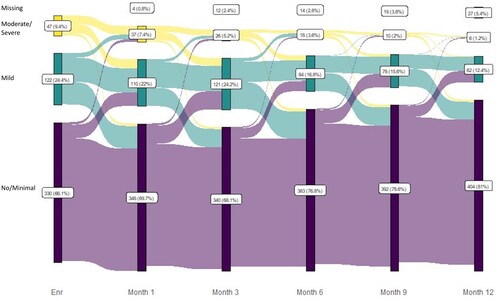
Table 1. Baseline characteristics of women in the Kampala Women’s Bone Study, by PHQ-9 depression score category and overall.
Associations of PrEP initiation
Of those enrolled, 88% chose to initiate PrEP at enrollment (431/499) and an additional 9 initiated PrEP at a later follow-up visit. PrEP uptake was similar among women with mild depression (8.2% vs. 16.7%, odds ratio (OR): 0.45, 95% Confidence Interval (CI): 0.22–0.91, ) and women with moderate/severe depression (6.4% vs. 16.7%, OR: 0.34, 95% CI: 0.10–1.14) compared with no/minimal depression along with women who did or did not report drug use (6.2% vs. 13.9%, OR: 0.39, 95% CI: 0.05–3.19). PrEP decline was lower among women who drank alcohol (6.8% vs. 15.7%, OR: 0.39, 95% CI: 0.18–0.85). IPV was uncommonly reported (5.6%, 28/499) and only among women who chose to initiate PrEP at baseline. Women who reported IPV were less likely to decline PrEP than those who did not experience IPV (0.0% vs. 14.5%, OR = 0.13, 95% CI: 0.01–0.57).
Table 2. Association of depression with declining PrEP at enrollment.
Depression and PrEP interruption
Among 440 women using PrEP, a total of 18 participant-driven PrEP interruptions occurred during the first 12 months of the study and 46 participant-driven interruptions occurred during the full 24 months of follow-up. During the initial 12 months, women reporting mild depression were similarly likely to choose to interrupt PrEP (0.8% vs. 1.0%, adjusted OR (aOR): 0.99, 95% CI: 0.38–2.56) than those with no/minimal depression, adjusted for partner’s HIV status and whether the participant had new partners in past 3 months (). Across 24 months of PrEP use, women reporting mild depression were similarly likely to interrupt PrEP (0.7% vs. 1.7%, aOR: 0.54, 95% CI: 0.22, 1.29) than those with no/minimal depression. None of the PrEP interruptions occurred at visits where the participant reported moderate/severe depression.
Table 3. Association of depression with participant-driven PrEP interruption.
Depression and PrEP adherence
In the initial 12 months of the study, low PrEP adherence (<80% openings within previous 7 days) was detected via Wisepill 73.4% of the time and low PrEP adherence was similar among women with mild or no/minimal depression (76.9% vs. 72.4%, aOR: 1.21, 95% CI: 0.87–1.69; ). During 24 months of the study, low PrEP adherence was detected via Wisepill 76.4% of the time and low PrEP adherence was similar among across depression categories. Depression symptoms were not associated with PrEP adherence across 12 and 24 months of follow-up.
Table 4. Association of depression with lower PrEP adherence detected via Wisepill and DBS during follow-up.
TFV-DP was quantified via DBS collected during 311 visits that corresponded with available Wisepill data. When comparing Wisepill adherence to DBS as the gold standard, we found a 5.7% sensitivity and 100% specificity (). Indication of low adherence via TFV-DP was more common among women with mild depression (3.3% vs. 0.7%) but not statistically different (aOR: 1.03, 95% CI: 0.98–1.08, ) from those no/minimal depression. Low TFV-DP levels were uncommon among women with moderate/severe depression and those with no/minimal depression (0.0% vs. 0.7%, aOR: 0.98, 95% CI: 0.97–1.00).
Table 5. Comparison between adherence detected via DBS and Wisepill.
Discussion
The prevalence of moderate to severe depression symptoms detected via standardized PHQ-9 questionnaire in this study was 9% at enrollment and an additional 24% of women had scores consistent with mild depression. During follow-up, 34% of young women reported at least mild depression symptoms, which highlights the need for more mental health services, training for clinical staff to utilize screening tools, and opportunities to leverage existing HIV prevention programs to integrate mental health services (Velloza et al., Citation2021).
In this cohort, depression did not significantly impact PrEP uptake, continuation, or adherence. Overall, a high percentage of women, regardless of depression status, chose to uptake (>83%) and continue receiving refills of (>98%) PrEP, but had low adherence (>72%). These data were collected during COVID-19-related public health restrictions, which limited access to public services, including reproductive health and mental health care (Sadinsky et al., Citation2020). Our study, however, found a lower PHQ-9 score in the period after the pandemic began. Although some women experienced acute or worsening depression symptoms, the overall prevalence of depression symptoms decreased over time which could reflect the clinical research setting and availability of an onsite psychologist. In addition, anecdotal accounts from study staff highlight that many participants moved from boarding schools and universities to their family home during the lockdown and this would have reduced opportunities for peer pressure, financial stress, and provided greater social support – all factors that could contribute to the unexpected finding of improved mental health and lack of statically significant effect on PrEP use.
Our data demonstrate that young women in Kampala have dynamic patterns of depression symptoms over 2 years. The PHQ-9 depression scale is one of many mental health assessment tools used globally to screen for probable depression in clinical and research settings (Costantini et al., Citation2021; Kroenke et al., Citation2001; Spitzer et al., Citation2000). Tools to measure depression symptoms are highly specific to cultural and regional underpinnings, and tool validity is not geographically universal. This caveat makes comparison of depression prevalence difficult across studies in different regions, within various subpopulations, or utilizing different measurement tools. In Uganda, one cross-sectional study that found an 18.2% prevalence of depression among teenagers at a reproductive health center (Kyohangirwe et al., Citation2020). The prevalence of moderate to severe depression at baseline (9%) was lower for women in this study as compared to women in other East Africa studies (12–33%) (Larsen et al., Citation2020; Lundberg et al., Citation2011; Osok et al., Citation2018). However, the cross-sectional measurement in other studies is insufficient to characterize the dynamic nature of depression symptoms and our study provides greater longitudinal description of symptoms.
Results from studies of depression and PrEP initiation from other settings in Africa suggest women with depression symptoms are amenable to initiating PrEP but struggle with adherence. Women with depression symptoms may have higher HIV risk and be open to taking PrEP, as found in other studies (Larsen et al., Citation2020). In addition, our research further supports literature that women with a history of IPV and alcohol use are more likely to accept PrEP; and other studies have found these subpopulations may struggle with PrEP adherence and continuation (Kiene et al., Citation2017; Roberts et al., Citation2016; Velloza et al., Citation2021), including studies of Ugandan women (Cabral et al., Citation2018; Roberts et al., Citation2016). IPV may be interrelated with both the depression pathways that exacerbate negative cognitive biases and the gendered power dynamics that underlie both IPV and barriers to seeking care for depression symptoms.
In our study, participant-driven PrEP interruption, which excludes instances where PrEP was accepted but not taken, was similar among women with and without depression. Additionally, depression symptoms were not associated with PrEP adherence captured via WisePill, which is likely an overestimate of high adherence. Poor measurement of adherence via WisePill and loss-to-follow-up over 24 months may underlie these findings. When assessing PrEP adherence through TFV-DP levels in a small subset of PrEP users (n = 311), our findings align with other studies in the region showing that women with depression symptoms trend towards lower adherence over time (Velloza et al., Citation2018, Citation2021; HPTN 067/ADAPT Study Team, et al., Citation2020).
Limitations of this study include the use of adherence data from electronic pill boxes, which are large, cumbersome, and often disliked by research participants (Haberer et al., Citation2020; Musiimenta et al., Citation2018; Velloza, Khoza, et al., Citation2020) and data may be inaccurate because women choose not to use them or not to carry them when traveling. Another limitation is that the PHQ-9 is structured to capture clinical depression and is therefore unable to contextualize the experiences of mild and moderate depression symptoms, particularly among populations unaccustomed to mental health screening. As such, PHQ-9 salience may not emphasize and fully capture the impact of depression, regardless of severity and day-to-day patterns, on a young person’s life (Helmich et al., Citation2020). COVID-19 public health measures in Uganda also impacted study retention and PrEP discontinuation rates when there were restrictions on public transportation and participants could not connect with study personnel for PrEP medication. Additionally, in prior PrEP studies, young women have cited preferences for the quality of care and counseling available at research clinics as compared to public clinics, and our study findings may not be fully generalizable to routine HIV prevention clinic with more limited resources for PrEP and mental health counseling (Magazi et al., Citation2014). Lastly, our findings are limited to a small group of women with moderate depression and may not be generalizable to routine HIV prevention clinic settings.
Few studies have described depression over time among young women seeking HIV prevention services in Uganda. We found that depression symptoms were frequent and fluid over time. Participants with depression symptoms tended to uptake PrEP, request PrEP refills, and adhere to PrEP with similar frequency to women with no/minimal signs of depression. The patterns of depression over time suggest that women can move into periods with more depression symptoms, and PrEP products that do not require daily adherence may be optimal for those whose depression symptoms manifest in this way. Our findings also demonstrate the opportunity for HIV prevention services to incorporate mental health screening tools and link patients to counseling services and care. As PrEP scale-up continues globally, integration of mental health screening can be considered and incorporated when provider skills and referral systems are present to support people found to have depression symptoms.
Authors’ contributions
RH TRM and AM led the Kampala Women’s Bone Study in its formulation and implementation with consultation from CW MY FM. JB and SM assisted with study coordination and safety monitoring. AN MB ON RN RS TM TS AM collected the data for the study. LM and RS conceptualized and developed the analysis plan. YZ refined and conducted the analysis, and YZ and RH drafted the manuscript. All authors have reviewed and approved of this manuscript.
Acknowledgements
We are grateful to the participants who gave of their time, energy, and dedication. We are also grateful to the study team for their careful work.
The Kampala Women’s Bone Study Team
University of Washington: Renee Heffron (protocol chair), Jade Boyer, Susan Morrison, Gabrielle Stein, Katherine Thomas, Elena A Rechkina, Kenneth Mugwanya, Jared M. Baeten, Andrew Hoofnagle
Infectious Diseases Institute: Andrew Mujugira (site investigator), Timothy Muwonge, Timothy Ssebuliba, Felix Bambia, Josephine Badaru, Monica Bagaya, Oliver Sapiri, Rogers Nsubuga, Agnes Nakyanzi, Lydia Valarie Nambala, Florence Nambi, Olivia Nampewo, Robert Nyanzi, Miriam Nampala Ryder, Mary Nakayiza
Makerere University-Johns Hopkins University Research Collaboration, Kampala, Uganda: Flavia Matovu Kiweewa, Andrew Kateregga, Stephen Bule
Columbia University: Mike Yin
Duke University: Christina Wyatt
Johns Hopkins University: Mark Marzinke
University of Colorado: Peter Anderson
Gilead Sciences: FTC/TDF donation
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data are available upon request from [email protected].
Additional information
Funding
References
- National Guidelines for Research involving Humans as Research Participants. (2014). Uganda National Council for Science and Technology.
- Consolidated Guidelines for Prevention and Treatment of HIV in Uganda. (2016). Uganda Ministry of Health.
- Depression and Other Common Mental Disorders: Global Health Estimates. (2017). World Health Organization.
- Uganda Population-Based HIV Impact Assessment. (2017). Ministry of Health Government of Uganda. https://www.afro.who.int/sites/default/files/2017-08/UPHIA%20Uganda%20factsheet.pdf
- Guidelines for the Use of Antiretroviral Drugs for the Treatment and Prevention of HIV in Kenya. (2018). Kenya Ministry of Health. http://cquin.icap.columbia.edu/wp-content/uploads/2017/04/ICAP_CQUIN_Kenya-ARV-Guidelines-2018-Final_20thAug2018.pdf
- Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. American Journal of Psychiatry, 165(8), 969–977. https://doi.org/10.1176/appi.ajp.2008.08050721
- Cabral, A., Baeten, J., Ngure, K., Velloza, J., Odoyo, J., Haberer, J., Celum, C., Muwonge, T., Asiimwe, S., & Heffron, R. (2018). Intimate partner violence and self-reported pre-exposure prophylaxis interruptions among HIV-negative partners in HIV serodiscordant couples in Kenya and Uganda. JAIDS Journal of Acquired Immune Deficiency Syndromes, 77(2), 154–159. https://doi.org/10.1097/QAI.0000000000001574
- Carroll, H. A., Hook, K., Perez, O. F. R., Denckla, C., Vince, C. C., Ghebrehiwet, S., Ando, K., Touma, M., Borba, C. P. C., Fricchione, G. L., & Henderson, D. C. (2020). Establishing reliability and validity for mental health screening instruments in resource-constrained settings: Systematic review of the PHQ-9 and key recommendations. Psychiatry Research, 291, 113236. https://doi.org/10.1016/j.psychres.2020.113236
- Castillo-Mancilla, J. R., Zheng, J.-H., Rower, J. E., Meditz, A., Gardner, E. M., Predhomme, J., Fernandez, C., Langness, J., Kiser, J. J., Bushman, L. R., & Anderson, P. L. (2013). Tenofovir, emtricitabine, and tenofovir diphosphate in dried blood spots for determining recent and cumulative drug exposure. AIDS Research and Human Retroviruses, 29(2), 384–390. https://doi.org/10.1089/aid.2012.0089
- Costantini, L., Pasquarella, C., Odone, A., Colucci, M. E., Costanza, A., Serafini, G., Aguglia, A., Belvederi Murri, M., Brakoulias, V., Amore, M., Ghaemi, S. N., & Amerio, A. (2021). Screening for depression in primary care with patient health questionnaire-9 (PHQ-9): A systematic review. Journal of Affective Disorders, 279, 473–483. https://doi.org/10.1016/j.jad.2020.09.131
- Fischer, M., Ramaswamy, R., Fischer-Flores, L., & Mugisha, G. (2019). Measuring and understanding depression in women in Kisoro, Uganda. Culture, Medicine, and Psychiatry, 43(1), 160–180. https://doi.org/10.1007/s11013-018-9604-9
- Haberer, J. E., Garrison, L., Tumuhairwe, J. B., Baijuka, R., Tindimwebwa, E., Tinkamanyire, J., Burns, B. F., & Asiimwe, S. (2020). Factors affecting the implementation of electronic antiretroviral therapy adherence monitoring and associated interventions for routine HIV care in Uganda: Qualitative study. Journal of Medical Internet Research, 22(9), e18038. https://doi.org/10.2196/18038
- Heffron, R., Muwonge, T. R., Boyer, J., Matovu, F., Zia, Y., Bagaya, M., Ssebuliba, T., Morrison, S., Bambia, F., Nsubuga, R., Badaru, J., Stein, G., Mugwanya, K. K., Wyatt, C., Baeten, J. M., Yin, M. T., Mujugira, A., Thomas, K., Rechkina, E., … Anderson, P. (2022). Bone mineral density, nutrient intake, and physical activity among young women from Uganda. Archives of Osteoporosis, 17(1), 134. https://doi.org/10.1007/s11657-022-01155-0
- Helmich, M. A., Wichers, M., Olthof, M., Strunk, G., Aas, B., Aichhorn, W., Schiepek, G., & Snippe, E. (2020). Sudden gains in day-to-day change: Revealing nonlinear patterns of individual improvement in depression. Journal of Consulting and Clinical Psychology, 88(2), 119–127. https://doi.org/10.1037/ccp0000469
- Ibrahim, M. E., Castillo-Mancilla, J. R., Yager, J., Brooks, K. M., Bushman, L., Saba, L., Kiser, J. J., MaWhinney, S., & Anderson, P. L. (2021). Individualized adherence benchmarks for HIV pre-exposure prophylaxis. AIDS Research and Human Retroviruses, 37(6), 421–428. https://doi.org/10.1089/aid.2020.0108
- Kaggwa, M. M., Najjuka, S. M., Ashaba, S., & Mamun, M. A. (2022). Psychometrics of the patient health questionnaire (PHQ-9) in Uganda: A systematic review. Frontiers in Psychiatry, 13, 781095. https://doi.org/10.3389/fpsyt.2022.781095
- Kiene, S. M., Lule, H., Sileo, K. M., Silmi, K. P., & Wanyenze, R. K. (2017). Depression, alcohol use, and intimate partner violence among outpatients in rural Uganda: Vulnerabilities for HIV, STIs and high risk sexual behavior. BMC Infectious Diseases, 17(1), 88. https://doi.org/10.1186/s12879-016-2162-2
- Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
- Kyohangirwe, L., Okello, E., Namuli, J. D., Ndeezi, G., & Kinyanda, E. (2020). Prevalence and factors associated with major depressive disorder among adolescents attending a primary care facility in Kampala, Uganda. Tropical Doctor, 50(1), 30–36. https://doi.org/10.1177/0049475519879586
- Larsen, A., Kinuthia, J., Lagat, H., Sila, J., Abuna, F., Kohler, P., John-Stewart, G., & Pintye, J. (2020). Depression and HIV risk behaviors among adolescent girls and young women seeking family planning services in Western Kenya. International Journal of STD & AIDS, 31(7), 652–664. https://doi.org/10.1177/0956462420920423
- Lundberg, P., Rukundo, G., Ashaba, S., Thorson, A., Allebeck, P., Östergren, P.-O., & Cantor-Graae, E. (2011). Poor mental health and sexual risk behaviours in Uganda: A cross-sectional population-based study. BMC Public Health, 11(1), 125. https://doi.org/10.1186/1471-2458-11-125
- Magazi, B., Stadler, J., Delany-Moretlwe, S., Montgomery, E., Mathebula, F., Hartmann, M., & van der Straten, A. (2014). Influences on visit retention in clinical trials: Insights from qualitative research during the VOICE trial in Johannesburg, South Africa. BMC Women’s Health, 14(1), 88. https://doi.org/10.1186/1472-6874-14-88
- Mehrotra, M. L., Glidden, D. V., McMahan, V., Amico, K. R., Hosek, S., Defechereux, P., Mayer, K. H., Veloso, V. G., Bekker, L.-G., Avelino-Silva, V. I., Schechter, M., & Grant, R. M. (2016). The effect of depressive symptoms on adherence to daily oral PrEP in men who have sex with men and transgender women: A marginal structural model analysis of the iPrEx OLE study. AIDS and Behavior, 20(7), 1527–1534. https://doi.org/10.1007/s10461-016-1415-9
- Miller, S. J., Harrison, S. E., & Sanasi-Bhola, K. (2021). A scoping review investigating relationships between depression, anxiety, and the PrEP care continuum in the United States. International Journal of Environmental Research and Public Health, 18(21), 11431. https://doi.org/10.3390/ijerph182111431
- Molodynski, A., Cusack, C., & Nixon, J. (2017). Mental healthcare in Uganda: Desperate challenges but real opportunities. BJPsych International, 14(4), 98–100. https://doi.org/10.1192/s2056474000002129
- Morgan, R., Tetui, M., Muhumuza Kananura, R., Ekirapa-Kiracho, E., & George, A. S. (2017). Gender dynamics affecting maternal health and health care access and use in Uganda. Health Policy and Planning, 32(suppl_5), v13–v21. https://doi.org/10.1093/heapol/czx011
- Musiimenta, A., Atukunda, E. C., Tumuhimbise, W., Pisarski, E. E., Tam, M., Wyatt, M. A., Ware, N. C., & Haberer, J. E. (2018). Acceptability and feasibility of real-time antiretroviral therapy adherence interventions in rural Uganda: Mixed-method pilot randomized controlled trial. JMIR MHealth and UHealth, 6(5), e122. https://doi.org/10.2196/mhealth.9031
- Nabunya, P., Byansi, W., Damulira, C., Bahar, O. S., Jennings Mayo-Wilson, L., Tozan, Y., Kiyingi, J., Nabayinda, J., Braithwaite, R., Witte, S. S., & Ssewamala, F. M. (2021). Predictors of depressive symptoms and post traumatic stress disorder among women engaged in commercial sex work in Southern Uganda. Psychiatry Research, 298, 113817. https://doi.org/10.1016/j.psychres.2021.113817
- Nakimuli-Mpungu, E., Bass, J. K., Alexandre, P., Mills, E. J., Musisi, S., Ram, M., Katabira, E., & Nachega, J. B. (2012). Depression, alcohol use and adherence to antiretroviral therapy in sub-Saharan Africa: A systematic review. AIDS and Behavior, 16(8), 2101–2118. https://doi.org/10.1007/s10461-011-0087-8
- Nakimuli-Mpungu, E., Mojtabai, R., Alexandre, P. K., Musisi, S., Katabira, E., Nachega, J. B., Treisman, G., & Bass, J. K. (2013). Lifetime depressive disorders and adherence to anti-retroviral therapy in HIV-infected Ugandan adults: A case-control study. Journal of Affective Disorders, 145(2), 221–226. https://doi.org/10.1016/j.jad.2012.08.002
- Nakku, J. E. M., Rathod, S. D., Kizza, D., Breuer, E., Mutyaba, K., Baron, E. C., Ssebunnya, J., & Kigozi, F. (2016). Validity and diagnostic accuracy of the Luganda version of the 9-item and 2-item Patient Health Questionnaire for detecting major depressive disorder in rural Uganda. Global Mental Health (Cambridge, England), 3, e20. https://doi.org/10.1017/gmh.2016.14
- Osok, J., Kigamwa, P., Stoep, A. V., Huang, K.-Y., & Kumar, M. (2018). Depression and its psychosocial risk factors in pregnant Kenyan adolescents: A cross-sectional study in a community health Centre of Nairobi. BMC Psychiatry, 18(1), 136. https://doi.org/10.1186/s12888-018-1706-y
- Pulerwitz, J., Gortmaker, S. L., & DeJong, W. (2000). Measuring sexual relationship power in HIV/STD research. Sex Roles, 42(7/8), 637–660. https://doi.org/10.1023/A:1007051506972
- Rael, C. T., Roberts, S., Ibitoye, M., Gorbach, P. M., Palanee-Phillips, T., Harkoo, I., Mbilizi, Y., Panchia, R., Siva, S., Tembo, T., Agwau Akello, C., Balkus, J., Riddler, S., & Carballo-Diéguez, A. (2021). Likely clinical depression and HIV-related decline in antiretroviral therapy untreated women who seroconverted during participation in microbicide trials in sub-Saharan Africa. International Journal of STD & AIDS, 32(7), 620–628. https://doi.org/10.1177/0956462420975935
- Roberts, S. T., Haberer, J., Celum, C., Mugo, N., Ware, N. C., Cohen, C. R., Tappero, J. W., Kiarie, J., Ronald, A., Mujugira, A., Tumwesigye, E., Were, E., Irungu, E., & Baeten, J. M. (2016). Intimate partner violence and adherence to HIV pre-exposure prophylaxis (PrEP) in African women in HIV serodiscordant relationships: A prospective cohort study. JAIDS Journal of Acquired Immune Deficiency Syndromes, 73(3), 313–322. https://doi.org/10.1097/QAI.0000000000001093
- Sadinsky, S., Jarandilla Nuñez, A., Nabulega, S., Riley, T., Ahmed, Z., & Sully, E. (2020). From bad to worse: The COVID-19 pandemic risks further undermining adolescents’ sexual and reproductive health and rights in many countries. Guttmacher Institute.
- Sankoh, O., Sevalie, S., & Weston, M. (2018). Mental health in Africa. The Lancet Global Health, 6(9), e954–e955. https://doi.org/10.1016/S2214-109X(18)30303-6
- Spitzer, R. L., Williams, J. B., Kroenke, K., Hornyak, R., & McMurray, J. (2000). Validity and utility of the PRIME-MD patient health questionnaire in assessment of 3000 obstetric-gynecologic patients: The PRIME-MD patient health questionnaire obstetrics-gynecology study. American Journal of Obstetrics and Gynecology, 183(3), 759–769. https://doi.org/10.1067/mob.2000.106580
- Ssebunnya, J., Medhin, G., Kangere, S., Kigozi, F., Nakku, J., & Lund, C. (2019). Prevalence, correlates and help-seeking behaviour for depressive symptoms in rural Uganda: A population-based survey. Global Mental Health (Cambridge, England), 6, e27. https://doi.org/10.1017/gmh.2019.25
- Vancampfort, D., Byansi, P., Kinyanda, E., Namutebi, H., Nalukenge, L., Bbosa, R. S., Ward, P. B., & Mugisha, J. (2019). Associations between physical inactivity, major depressive disorder, and alcohol use disorder in people living with HIV in a Ugandan fishing community. International Journal of STD & AIDS, 30(12), 1177–1184. https://doi.org/10.1177/0956462419863924
- Velloza, J., Baeten, J. M., Haberer, J., Ngure, K., Irungu, E., Mugo, N. R., Celum, C., & Heffron, R. (2018). Effect of depression on adherence to oral PrEP among men and women in East Africa. JAIDS Journal of Acquired Immune Deficiency Syndromes, 79(3), 330–338. https://doi.org/10.1097/QAI.0000000000001821
- Velloza, J., Heffron, R., Amico, K. R., Rowhani-Rahbar, A., Hughes, J. P., Li, M., Dye, B. J., Celum, C., Bekker, L.-G., & Grant, R. M. (2020). The effect of depression on adherence to HIV pre-exposure prophylaxis among high-risk South African women in HPTN 067/ADAPT. AIDS and Behavior, 24(7), 2178–2187. https://doi.org/10.1007/s10461-020-02783-8
- Velloza, J., Hosek, S., Donnell, D., Anderson, P. L., Chirenje, M., Mgodi, N., Bekker, L.-G., Delany-Moretlwe, S., Celum, C., & HPTN 082 study group. (2021). Assessing longitudinal patterns of depressive symptoms and the influence of symptom trajectories on HIV pre-exposure prophylaxis adherence among adolescent girls in the HPTN 082 randomized controlled trial. Journal of the International AIDS Society, 24(Suppl 2), e25731. https://doi.org/10.1002/jia2.25731
- Velloza, J., Kemp, C. G., Aunon, F. M., Ramaiya, M. K., Creegan, E., & Simoni, J. M. (2020). Alcohol use and antiretroviral therapy non-adherence among adults living with HIV/AIDS in Sub-Saharan Africa: A systematic review and meta-analysis. AIDS and Behavior, 24(6), 1727–1742. https://doi.org/10.1007/s10461-019-02716-0
- Velloza, J., Khoza, N., Scorgie, F., Chitukuta, M., Mutero, P., Mutiti, K., Mangxilana, N., Nobula, L., Bulterys, M. A., Atujuna, M., Hosek, S., Heffron, R., Bekker, L.-G., Mgodi, N., Chirenje, M., Celum, C., & Delany-Moretlwe, S. (2020). The influence of HIV-related stigma on PrEP disclosure and adherence among adolescent girls and young women in HPTN 082: A qualitative study. Journal of the International AIDS Society, 23(3), Article 3. https://doi.org/10.1002/jia2.25463
