
ABSTRACT
We sought to characterize overdose and non-overdose mortality among PLWH amidst the illicit drug toxicity crisis in British Columbia, Canada. A population-based analysis of PLWH (age ≥19) in British Columbia accessing healthcare from April 1996 to March 2017 was conducted using data from the Seek and Treat for Optimal Prevention of HIV/AIDS (STOP HIV/AIDS) cohort linkage. Underlying causes of deaths were stratified into overdose and non-overdose causes. We compared (bivariate analysis) health-related characteristics and prescription history between PLWH died of overdose and non-overdose causes between April 2009 and March 2017. Among 9,180 PLWH, we observed 962 deaths (142 [14.7%] overdoses; 820 [85.2%] other causes). Compared to those who died from other causes, those who died of overdose were significantly younger (median age [Q, Q3]: 46 years [42, 52] vs. 54 years [48, 63]); had an indication of chronic pain (35.9% vs. 27.1%) and hepatitis C virus (64.8% vs. 50.4%), but fewer experienced hospitalization in the year before death. PLWH who died were most likely to be prescribed with opioids (>50%) and least likely with opioid agonist therapy (<10%) in a year before death. These findings highlight the syndemic of substance use, HCV, and chronic pain, and how the crisis is unqiuely impacting females and younger people.
Introduction
The introduction of highly effective combination antiretroviral therapy (cART) has marked a paradigm shift in HIV care. Evidence overwhelmingly indicates that early access to and retention on cART has led to a drastic decline in acquired immunodeficiency syndrome (AIDS) related diseases and a near-normal life expectancy for people living with HIV (PLWH) (May et al., Citation2014; Kholoud Porter et al., Citation2003; Mocroft et al., Citation2003). Notwithstanding, PLWH are increasingly experiencing complex comorbidities and social inequities that may impact survival gains achieved by cART (Salters et al., Citation2021; St-Jean et al., Citation2021).
Growing evidence suggests a recent change in mortality trends among PLWH dominated by non-HIV causes, with accidental overdoses, non-AIDS related cancers, and infections of the upper respiratory system such as tuberculosis and pneumonia, being the main drivers of deaths in the last decade (Eyawo et al., Citation2017; Gheibi et al., Citation2019; Paula et al., Citation2020; Yazdani et al., Citation2022). A British Columbian study of underserved PLWH, between 2007 and 2010, reported that over a quarter of deaths were attributed to overdose and drug toxicity (Salters et al., Citation2021).
The illicit drug toxicity crisis has been documented as a major public health challenge in British Columbia, Canada since 2009 (Illicit Drug Toxicity Deaths in British Columbia, Citation2021). In response to the rise in overdose deaths due to the toxic drug supply (Cooper et al., Citation2020), the province declared a public health emergency in 2016 (British Columbia Centre for Disease Control, Citation2018). More than 10,000 British Columbians have died in the six years following the declaration (Legislative Assembly of British Columbia, Citation2022).
The relationship between HIV and substance use disorders (SUD) is complex, and PLWH may be at a greater risk of dying from an overdose due to pre-existing comorbid conditions associated with an elevated risk of overdose (e.g., respiratory distress, liver impairment) and difficulty accessing healthcare and treatment (Green et al., Citation2012). In British Columbia, the overdose mortality has reduced the gains in life expectancy of PLWH achieved by virtue of cART, where, on average, cART was associated with 3.3 years of potential gain in life expectancy for those aged 20 in 2014–2017 compared to 8.7 years in 2002–2013 (St-Jean et al., Citation2021).
The objective of the present study was to further evaluate the impact of the illicit drug toxicity crisis among PLWH in British Columbia, where cART is free-of-charge and Treatment as Prevention programs have been running for more than a decade. Our objectives were (i) to characterize underlying causes of deaths due to overdose and non-overdose related causes, and (ii) to examine differences in health-related characteristics and medication prescribing histories between those who died of overdose versus (vs.) non-overdose causes.
Methods
Data sources
Data were obtained from the population-based Seek and Treat for Optimal Prevention of HIV/AIDS (STOP HIV/AIDS) linkage cohort study, comprising de-identified individual-level data on all adults diagnosed with HIV between 01 April 1996 and 31 March 2017, in British Columbia. The STOP HIV/AIDS cohort, as described in depth previously, was formed through the linkage of provincial treatment, surveillance, and administrative databases (Heath et al., Citation2014; Nosyk et al., Citation2013). Entry into cohort was defined as the later of 01 April 1996 or earliest HIV-related record for individuals, considering all data resources. Demographics and laboratory data were identified through the provincial HIV Drug Treatment Program (DTP), which contains immunologic, virologic, and cART-related data (British Columbia Centre for Excellence. Drug Treatment Program, Citation2020). Comorbidities of interests and hospitalization episodes were identified from two main databases: (i) Medical Services Plan (MSP), and (ii) Discharge Abstract Database (DAD), using their respective International Classification Disease Codes versions 9 and 10 (ICD-9/10) (World Health Organization. International Classification of Diseases 9th Revisions, Clinical Modifications, Citation2009; World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revisions., Citation2019). The MSP data comprise of all practitioner claims with one ICD-9 diagnostic code representing the reason for each visit (British Columbia Ministry of Health. Medical Services Plan, Citation2018). The DAD data include all hospital admissions with 25 diagnostic codes (ICD-9: April 1996–March 2001; ICD-10 April 2001 onwards) per hospitalization representing either the primary reason for admission or complications during hospitalization, as well as 20 procedure codes (Canadian Institute for Health Information. Discharge Abstract Database, Citation2018). Information on assessed prescriptions in the study was retrieved from PharmaNet data that include all prescription medications dispensed by BC pharmacies, using Drug/Product Identification Number (DINPIN) (British Columbia Ministry of Health. PharmaNet, Citation2018). Over-the-counter medications are not captured in this dataset. Data on underlying causes of deaths were identified through Vital Statistic Deaths derived from death certificates, using ICD-10 codes (British Columbia Vital Statistics Agency. Vital Statistics Deaths, Citation2016; Mattson et al., Citation2021).
Study setting
Eligible participants for this study were ≥19 years of age, with a minimum of 12 months of follow-up from HIV cohort entry, and were alive at study entry (as of 01 April 2009). Participants with unknown sex were excluded from this analysis (n = 2) (Appendix 1). The end of the observation period for this study was defined as either the date of death, date of last health care encounter (i.e., latest patient record in either of DTP, MSP, DAD, or PharmaNet databases), or end of follow-up (i.e., 31 March 2017), whichever occurred first.
Outcome assessment
The outcome of interest was underlying cause of death, defined as the disease or injury that initiated train of morbid events leading directly to death (British Columbia Vital Statistics Agency. Vital Statistics Deaths, Citation2016). We characterized all deaths as caused by overdose, other causes (non-overdose), or an unknown cause of death between 01 April 2009 and 31 March 2017. The time-period for this analysis captures both the modern era of HIV Treatment as Prevention in British Columbia (Heath et al., Citation2014; Nosyk et al., Citation2014), as well as the illicit drug toxicity crisis. Fatal overdoses either due to illicit or licit drug use were further identified using ICD-10 codes X40-X44 (unintentional), and X60-X64 (intentional/suicidal) (StatisticsCanada, Citation2005a, Citation2005b). Details on ICD codes and the ascertainment of underlying causes of deaths are described in Appendix 2.
Covariate assessment
Selected continuous covariates associated with the risk of fatal overdose were age and HIV viral load, measured at death as median (25th percentile [Q1], 75th percentile [Q3]). Categorical covariates were measured at relevant time points: (1) time-independent: sex at birth (male, female), lifetime diagnosis of hepatitis C virus (HCV) (yes, no); (2) at death: CD4 cell count (≥350, 200–349, <200 cells/mm3); (3) a year before death: depression (yes, no), SUD (yes, no), chronic pain (yes, no); and (4) ≤4, 4–12, and 13–48 weeks before death: ≥1 hospitalization episode (yes, no); ≥1 prescription (yes, no) of five medication classes including opioid agonist therapy (OAT), non-OAT opioids, neuropathic pain relievers (NPR), antidepressants (selective serotonin reuptake inhibitors/serotonin norepinephrine reuptake inhibitors [SSRI/SNRI] and sedatives), respectively. Of note, British Columbia ministry of health guidelines (Chronic Disease Information Working Group, Citation2018) ascertained SUD cases including alcohol dependence syndrome and alcohol-induced mental disorders, drug dependence syndrome and drug-induced disorder, and nondependent use of drug, while the US Centres for Disease Control and Prevention guidelines (Centres for Disease Control and Prevention, Citation2013) ascertained the presence of chronic pain. Detailed case definition of depression, SUD, and chronic pain with their respective ICD codes are presented in Appendix 3. Medication DINPINs are presented in a supplementary excel file.
Statistical analysis
Individuals who died were dichotomized into two groups: those who died of an overdose and those died of other (non-overdose) causes. Mortality rates were standardized by age and sex, using direct method and applying the 2016 Canadian population as reference (Statistics Canada. Census of Population, Citation2016). The annual age-standardized mortalities (per fiscal year) with 95% confidence intervals (CI) were calculated to assess the mortality trend over time. Prescription history was stratified by sex to adequately characterize differences in drug-related risks between males and females. Demographic variables, comorbidities, and prescribing histories were compared between PLWH who died of overdose versus other causes (non-overdose), using t-test/Wilcoxon-Man Whitney test for continuous variables, and chi-square/Fisher’s exact test for categorical variables. The significance level was set at 5%. All statistical analyses were performed using Statistical Analysis System (SAS) software version 9.4 (SAS, Cary, NC, U.S.A.).
Results
Of 9180 PLWH who met the eligibility criteria for this study, the median age at cohort entry was 37 years (31, 46) and 79.4% of the participants were male. In total, 962 deaths were observed between 01 April 2009 and 31 March 2017, of which 14.7% (n = 142) were due to overdose, (unintentional [14.2%, n = 137]; intentional [0.5%, n = 5]). The unintentional overdose deaths were largely caused by exposure to narcotics and psychodysleptics (52.5%, n = 72). Main drivers of non-overdose deaths were HIV-related causes (22.4%, n = 184), non-AIDS cancer (21.3%, n = 175), and cardiovascular diseases (11.3%, n = 93) ().
Table 1. Mortality due to overdose and non-overdose causes among PLWH in BC (n = 9180) from 2009/2010 to 2016/2017.
Crude mortality rates for overdose deaths were significantly higher among females than males (3.74 deaths per 1000 PY [95% CI: 2.77, 5.04] vs. 2.20 [1.81, 2.68], respectively) (). Similarly, crude mortality rates for non-overdose deaths were also higher among females 16.16 (95% CI: 14.0, 18.66) compared to 14.11 (95% CI: 13.06, 15.26) among males. The highest rate of overdose deaths was observed within age groups 30–49 (2.84 [95% CI: 2.30, 3.51]) and 50–64 (2.59 [95% CI: 1.96, 3.41]), whereas the risk of non-overdose deaths increased with age, with those aged >65 experiencing 48.10 deaths per 1000 PY (95% CI: 41.58, 55.64). Standardized rates were 2.91 (95% CI: 2.28, 3.53) for overdose deaths, and 17.20 (95% CI: 15.59, 18.82) for non-overdose deaths.
Table 2. Mortality rates among PLWH in BC from 2009/2010 to 2016/2017.
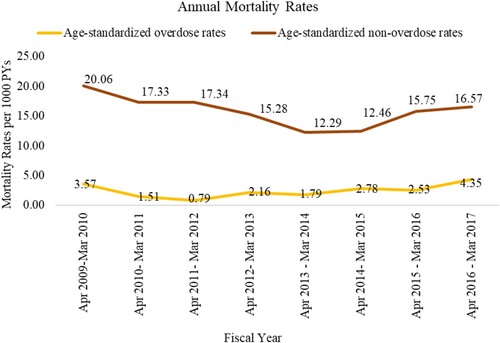
When assessing the age-standardized trends (), we observed about 2-fold increase in overdose deaths in 2016/2017. The age-standardized trend for non-overdose deaths indicates a 60% decline in 2009/2010–2013/2014, followed by 30% increase in 2014/2015–2016/2017.
Figure 1. Age-standardized annual mortality trends from 2009/2010 to 2016/2017, divided by overdose versus non-overdose deaths. Note: Fiscal year is the period between 01 April of the previous year and March 31 of the year indicated in the y-axis, e.g., year 2017 indicates the period from 01 April 2016 to 31 March 2017. Note: Standardization was performed using direct method and based on the 2016 Canadian population as a reference. Note: Counts of overdose deaths for age categories <30 and 65+ were sparse. Therefore, age categories <30 and 30–49, and, separately, 50–64 and 65+ were combined, i.e., age-adjusted categories for the purpose of annual trend were defined as <50 and 50+. Abbreviations: PYs: person-years.
Comparing PLWH who died from overdose and non-overdose causes (), the median age (Q1, Q3) at death was significantly lower for those who died of overdose (46 years [42, 52] vs. 54 years [48, 63], respectively). Males died less due to overdose vs. non-overdose causes (69.7% vs. 77.3%), whereas females were more likely to die of overdose (30.2 vs. 22.6%), p = 0.04. Compared to people who died of non-overdose causes, people who died of overdose were more likely to have indication of chronic pain (35.9% vs. 27.1%) and HCV (64.8% vs. 50.4%). Those who died of non-overdose deaths were more likely to have the lowest category of CD4 cell count, i.e.,<200 cells/mm3 at death (26.9% vs. 14.1%). Diagnoses of SUD and depression in the year before death were not statistically different between people dying of overdose versus non-overdose causes. Of note, prevalence of SUD diagnosis in our sample was over 50% within a year prior to death (overdose: 58.4% vs. non-overdose: 50.1%). At all assessed time windows up to 48 weeks before death, hospitalization episodes were less likely for overdose deaths (p < .0001). For instance, in a month prior to death, only 19.7% of those died of overdose, compared to 63.6% of those who died of non-overdose, were hospitalized.
Table 3. Comparison of health-related characteristics among people who died of overdose versus non-overdose causes from 2009/2010 to 2016/2017.
When assessing prescribing practices before death (irrespective of the death cause), among selected class of medications, opioids were most likely to be prescribed to females or males PLWH (>50%), whereas OATs were least likely (<20%) (). Prescription of OAT and sedatives are significantly different between male PLWH who died of overdose vs. non-overdose (12.1% vs. 6.3%, and 21.2% vs. 31.7%, respectively). Among females, prescription difference between those who died of overdose vs. non-overdose was only observed for NPR (53.4% vs. 33.8%). Note that in the four-week period before death, opioids were prescribed to a lesser extent (≤35% of either males or females). When assessed at different time windows, males who died of overdose experienced little to no change in OAT prescription (≤4 weeks before death: 9.1%; 5–12 weeks before death: 10.1%; 13–48 weeks before death: 9.1%), while a noticeable drop in OAT prescription was observed among females dying of overdose, 4.6% of whom were prescribed OAT in the four-week period prior to death (5–12 weeks before death: 11.6%; 13–48 weeks before death: 18.6%) (Appendix 4, Supplementary Figure).
Table 4. Comparison of prescription history between PLWH who died of overdose versus non-overdose from 2009/2010 to 2016/2017, stratified by sex.
Discussion
In this population-based study using cohort of PLWH in BC, we examined the dynamics of overdose and non-overdose deaths amidst the illicit drug toxicity and the later era of cART (2009–2017). The vast majority of fatal overdoses were unintentional. Common other causes of deaths in this analysis included HIV-related causes, non-AIDS cancer, and cardiovascular diseases. Female and younger PLWH had higher rates of fatal overdoses in our setting (compared to males and older people). PLWH died of overdose were disproportionately affected by HCV and chronic pain, yet were less hospitalized in the year before death (an indication perhaps of greater hospital-based care for people dying from other causes).
The syndemic of HIV, HCV, and overdose calls for multi-level responses that reduce structural vulnerability and create a health-enabling environment, particularly for women and younger people (Perlman & Jordan, Citation2018). Evidence supports implementation of broader HCV and HIV care and treatment, substance use screening, therpaeutic interventions (i.e. OAT, safe supply), and harm reduction programs to control the syndemic and enhance effectiveness of public health responses to toxic drug supply and prevent overdose deaths among PLHW (Braveman et al., Citation2011; Perlman & Jordan, Citation2018).
Our results suggest that PLWH who died were more likely to have been prescribed opioids in the year before death than other assessed medications. Prescription opioids have been prominently featured in long-term management of chronic pain among PLWH (R. D. Bruce et al., Citation2017). Chronic pain is an important and multifactorial comorbidity that reportedly occurs in 85% of PLWH (Merlin et al., Citation2018). Long-term opioid use, particularly when prescribed at high dose is shown to be associated with an increased risk of overdose (R. D. Bruce et al., Citation2017). New evidence suggests that opioids may further accelerate HIV disease progression by impairing immune function (Roy et al., Citation2011), increasing virologic failure (Flores et al., Citation2018), and disrupting gut homeostasis (Meng et al., Citation2015).
Given these findings, current pain guidelines do not recommend opioid analgesics as a first-line treatment for the long-term management of chronic pain in PLWH (R. Douglas Bruce et al., Citation2017). Therefore, it is important to offer PLWH with chronic pain more effective treatment pathways that best address their chronic pain, reduce their risk of overdose, and ensures retention in care. An interesting clustered randomized clinical trial by Samet and Colleagues suggests that Targeting Effective Analgesia in Clinic for HIV (TEACH) improves adherence to chronic opioid therapy guidelines for the management of chronic pain (Samet et al., Citation2021).
Although no difference in opioid prescription use was observed, chronic pain was disproportionately higher in males dying of overdose vs. non-overdose a year before death (36.6% vs. 25.8%; p = 0.02). This is while the occurrence of chronic pain among females dying of overdose was similar to that of individuals who died from other causes (non-overdose). However, the proportion of individuals with chronic pain is still above 30% (34.8% vs. 31.1%; p = 0.6), which suggests an overall higher indication of chronic pain among female PLWH, indicating that more research may be needed to identify effective supports and interventions.
Inadequate management of chronic pain among PLWH can have widespread negative consequences and may affect not only their clinical care, but also their social and psychosical health (Madden et al., Citation2020). Therefore, greater clinical effort and research attention are required to address chronic pain issues among PLWH, especially in higher-risk settings and according to sex differences.
Furthermore, Vold et al. reported that an increased dispensation of opioid analgesic was associated with dispensed OAT below half of the recommended dose or OAT discontinuation (Citation2020). It was not within the scope of this study to assess the relationship between opioid and OAT prescribing practices; however, we observed a low frequency of OAT prescriptions within a year before a fatal overdose. Smolina and colleagues also found that fewer than 10% of people who died of an opioid-related overdose in BC had a prescription for OAT at the time of overdose (Citation2019). While we could not determine the role of opioid use in our analysis, the lack of OAT use among PLWH who died due to overdose may indicate missed opportunities for clinical interventions in this setting. These data indicate the need for future studies examining the impact of OAT prescribing practices among PLWH at risk of opioid overdose. Additionally, it is necessary to implement effective OAT programs in coordination with safe supply interventions, HCV care and treatment, and management of chronic pain among PLWH.
It is worth noting that female PLWH who died of overdose were prescribed more frequently with antidepressants that could reflect higher prevalence of depression and anxiety (Salk et al., Citation2017; VanHouten et al., Citation2019). Higher rates of overdose deaths and co-occurring mental health concerns among females in our setting suggest that the current overdose crisis has produced important differences by sex. Therefore, to effectively prevent overdose deaths among PLWH, interventions that consider women’s risks and needs as they relate to opioid use disorder and co-occurring conditions are critical (Barbosa-Leiker et al., Citation2021).
Limitations of this study include those inherent to observational studies using administrative data. First, we expect underestimation of overdose deaths given that only confirmed cases of overdose were captured and ≥50% of undetermined causes of death in BC are likely drug-related (Ye et al., Citation2018). Second, we were not able to examine overdose mortality specific to substances due to the use of predefined ICD categories attributed to underlying cause of deaths and unavailability of information on toxicology testing in our administrative data. Third, our data were limited to 31 March 2017, thus our cohort does not reflect the increasing detrimental effect of the overdose crisis post-2017. Fourth, our administrative data do not contain information on community-based health care interactions where people with opioid use disorder are more likely to receive OAT; therefore, underestimation of OAT prescription using solely these administrative data was possible. However, we used the powerful PharmaNet database, which captures dispensed medications from all pharmacies in BC. Fifth, we did not have access to emergency care data. A high proportion of the population experiencing concurrent disorders present to emergency care as the first point of contact. We assessed hospitalization episodes using DAD where we captured primary reasons for admission or complications arising during hospitalization. Therefore, our hospitalization events exclude emergency care.
Conclusion
In our setting, PLWH, particularly females and younger people are disproportionately affected by the illicit drug toxicity crisis. The syndemic of substance use disorder, HCV co-infection, and the often overlooked issue of chronic pain may be exacerbating the crisis among PLWH in British Columbia. Implementation of an integrated approach and a multi-level response is required to identify areas of vulnerability, enhance effectiveness of public health policies, and ultimately reduce overdose deaths among PLWH.
Authors contributions
KY, ND, and KS contributed to the research conceptualization, development, and design of methodology, data analysis, and data interpretation. KS oversaw project administration. KY was responsible for the original draft preparation and project coordination. MY, JT contributed to data cleaning, statistical analysis, and computer code implementation and statistical interpretation. AT, CS, N.GA, TM, VL, RB, RH, and JM contributed to the paper’s data interpretation and critical review. All authors contributed to manuscript development.
Ethics
The British Columbia Centre for Excellence in HIV/AIDS received approval for this study from the University of British Columbia Ethics Review Committee at St. Paul’s Hospital, Providence Health Care Site (H08-02095).
Supplemental Material
Download MS Word (2 MB)Supplemental Material
Download MS Word (156 KB)Acknowledgements
We would like to acknowledge with gratitude the people living with HIV and the health care practitioners in the province. We honour those we have lost due to the toxic drug crisis. We are grateful to the BC Ministry of Health of British Columbia for providing access to the administrative data and ongoing support. We also acknowledge the support of Scott Emerson and Amanda Yonkman and the STOP HIV/AIDS research group.
Disclaimer: All inferences, opinions, and conclusions drawn in this publication are those of the authors, and do not reflect the opinions or policies of the Data Stewards. The BC-CfE is prohibited from making individual-level data available publicly due to provisions in our service contracts, institutional policy, and ethical requirements. In order to facilitate research, we make such data available via individual data access requests. Some BC-CfE data are not available externally due to prohibitions in service contracts with our funders or data providers. Institutional policies stipulate that all external data requests require collaboration with a BC-CfE researcher. For more information or to make a request, please contact [email protected]. All data relevant to the analysis are included in the tables or supplementary materials. The underlying analytical codes are available from the authors on request.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Barbosa-Leiker, C., Campbell, A. N. C., McHugh, R. K., Guille, C., & Greenfield, S. F. (2021). Opioid use disorder in women and the implications for treatment. Psychiatric Research and Clinical Practice, 3(1), 3–11. https://doi.org/10.1176/appi.prcp.20190051
- Braveman, P., Egerter, S., & Williams, D. R. (2011). The social determinants of health: Coming of age. Annual Review of Public Health, 32(1), 381–398. https://doi.org/10.1146/annurev-publhealth-031210-101218
- British Columbia Center for Excellence. (2020). Drug Treatment Program. http://bccfe.ca/drug-treatment-program
- British Columbia Centre for Disease Control. (2018). http://www.bccdc.ca/PublishingImages/opioid-overdose-emergency-snapshot.pdf
- British Columbia Ministry of Health. (2018). Medical Services Plan. Population Data BC. Payment Information File. V2. http://www.popdata.bc.ca/data
- British Columbia Ministry of Health. (2018). PharmaNet. Data Stewardship Committee. V2. http://www.popdata.bc.ca/data
- British Columbia Vital Statistics Agency. (2016). Vital Statistics Deaths. Data Stewardship Committee. V2. http://www.popdata.bc.ca/data
- Bruce, R. D., Merlin, J., Lum, P. J., Ahmed, E., Alexander, C., Corbett, A. H., Foley, K., Leonard, K., Treisman, G. J., & Selwyn, P. (2017). 2017 HIVMA of IDSA clinical practice guideline for the management of chronic pain in patients living With HIV. Clinical Infectious Diseases, 65(10), e1–e37. https://doi.org/10.1093/cid/cix636
- Canadian Institute for Health Information. Discharge Abstract Database. (2018). Population Data BC. V2. http://www.popdata.bc.ca/data
- Centres for Disease Control and Prevention. (2013). Prescription Drug Overdose Data and Statistics Guide to ICD-9-CM and ICD-10 Codes Related to Poisoning and Pain https://www.cdc.gov/drugoverdose/pdf/PDO_Guide_to_ICD-9-CM_and_ICD-10_Codes-a.pdf
- Chronic Disease Information Working Group. (2018). BC Chronic Disease and Selected Procedure Case Definitions http://www.bccdc.ca/health-professionals/data-reports/chronic-disease-dashboard#Case–Definitions
- Cooper, L., Thompson, R., Edgerton, J., Watson, R., MacMaster, J., Kalliny, S. A., Huffman, M., Juarez, M. M., Mathews-Juarez, P., Tabatabai, P., Singh, M., & P, K. (2020). Modeling dynamics of fatal opioid overdose by state and across time. Preventive Medicine Reports, 20, 101184–101184. https://doi.org/10.1016/j.pmedr.2020.101184
- Eyawo, O., Franco-Villalobos, C., Hull, M. W., Nohpal, A., Samji, H., Sereda, P., Lima, V. D., Shoveller, J., Moore, D., Montaner, J. S. G., Hogg, R. S., Montaner, J., Hogg, R., Eyawo, O., Hull, M., Shoveller, J., Moore, D., Sereda, P., Lima, V., for the Comparative, O., & Service Utilization Trends, s. (2017). Changes in mortality rates and causes of death in a population-based cohort of persons living with and without HIV from 1996 to 2012. BMC Infectious Diseases, 17(1), 174. https://doi.org/10.1186/s12879-017-2254-7
- Flores, J., Liang, Y., Ketchum, N. S., Turner, B. J., Bullock, D., Villarreal, R., Potter, J. S., & Taylor, B. S. (2018). Prescription opioid use is associated with virologic failure in people living with HIV. AIDS and Behavior, 22(4), 1323–1328. https://doi.org/10.1007/s10461-017-1842-2
- Gheibi, Z., Shayan, Z., Joulaei, H., Fararouei, M., Beheshti, S., & Shokoohi, M. (2019). Determinants of AIDS and non-AIDS related mortality among people living with HIV in Shiraz, southern Iran: A 20-year retrospective follow-up study. BMC Infectious Diseases, 19(1), 1094. https://doi.org/10.1186/s12879-019-4676-x
- Green, T. C., McGowan, S. K., Yokell, M. A., Pouget, E. R., & Rich, J. D. (2012). HIV infection and risk of overdose: A systematic review and meta-analysis. AIDS (London, England), 26(4), 403–417. https://doi.org/10.1097/QAD.0b013e32834f19b6
- Heath, K., Samji, H., Nosyk, B., Colley, G., Gilbert, M., Hogg, R. S., & Montaner, J. S. (2014). Cohort profile: Seek and treat for the optimal prevention of HIV/AIDS in British Columbia (STOP HIV/AIDS BC). International Journal of Epidemiology, 43(4), 1073–1081. https://doi.org/10.1093/ije/dyu070
- Illicit Drug Toxicity Deaths in British Columbia. (2021). https://www2.gov.bc.ca/assets/gov/birth-adoption-death-marriage-and-divorce/deaths/coroners-service/statistical/illicit-drug.pdf
- Kholoud Porter, A. B., Bhaskaran Krishnan, Janet Darbyshire, Patrizio Pezzotti, Kholoud Porter, A Sarah Walker, & CASCADE Collaboration. (2003). Determinants of survival following HIV-1 seroconversion after the introduction of HAART. The Lancet, 362(9392), 1267-1274. https://doi.org/10.1016/S0140-6736(03)14570-9
- Legislative Assembly of British Columbia. (2022). Closing gaps, reducing barriers: Expanding the response to the toxic drug and overdose crisis. https://www.leg.bc.ca/content/CommitteeDocuments/42nd-parliament/3rd-session/health/report/SSC-Health-Report_42-3_2022-11-01_Final.pdf
- Madden, V. J., Parker, R., & Goodin, B. R. (2020). Chronic pain in people with HIV: A common comorbidity and threat to quality of life. Pain Management, 10(4), 253–260. https://doi.org/10.2217/pmt-2020-0004
- Mattson, C. L., Tanz, L. J., Quinn, K., Kariisa, M., Patel, P., & Davis, N. L. (2021). Trends and geographic patterns in drug and synthetic opioid overdose deaths – United States, 2013-2019. MMWR. Morbidity and Mortality Weekly Report, 70(6), 202–207. https://doi.org/10.15585/mmwr.mm7006a4
- May, M. T., Gompels, M., Delpech, V., Porter, K., Orkin, C., Kegg, S., Hay, P., Johnson, M., Palfreeman, A., Gilson, R., Chadwick, D., Martin, F., Hill, T., Walsh, J., Post, F., Fisher, M., Ainsworth, J., Jose, S., Leen, C., … Study, U. K. C. H. C. (2014). Impact on life expectancy of HIV-1 positive individuals of CD4+ cell count and viral load response to antiretroviral therapy. AIDS (London, England), 28(8), 1193–1202. https://doi.org/10.1097/QAD.0000000000000243
- Meng, J., Sindberg, G. M., & Roy, S. (2015). Disruption of gut homeostasis by opioids accelerates HIV disease progression. Frontiers in Microbiology, 6, 643. https://doi.org/10.3389/fmicb.2015.00643
- Merlin, J. S., Long, D., Becker, W. C., Cachay, E. R., Christopoulos, K. A., Claborn, K., Crane, H. M., Edelman, E. J., Harding, R., Kertesz, S. G., Liebschutz, J. M., Mathews, W. C., Mugavero, M. J., Napravnik, S. C. C. O., Saag, M. S., Starrels, J. L., & Gross, R. (2018). Brief report: The association of chronic pain and long-term opioid therapy with HIV treatment outcomes. Journal of Acquired Immune Deficiency Syndromes, 79(1), 77–82. https://doi.org/10.1097/qai.0000000000001741
- Mocroft, A., Ledergerber, B., Katlama, C., Kirk, O., Reiss, P., d’Arminio Monforte, A., Knysz, B., Dietrich, M., Phillips, A. N., & Lundgren, J. D. (2003). Decline in the AIDS and death rates in the EuroSIDA study: An observational study. The Lancet, 362(9377), 22–29. https://doi.org/10.1016/s0140-6736(03)13802-0
- Nosyk, B., Colley, G., Yip, B., Chan, K., Heath, K., Lima, V. D., Gilbert, M., Hogg, R. S., Harrigan, P. R., & Montaner, J. S. (2013). Application and validation of case-finding algorithms for identifying individuals with human immunodeficiency virus from administrative data in British Columbia, Canada. PLoS One, 8(1), e54416. https://doi.org/10.1371/journal.pone.0054416
- Nosyk, B., Montaner, J. S. G., Colley, G., Lima, V. D., Chan, K., Heath, K., Yip, B., Samji, H., Gilbert, M., Barrios, R., Gustafson, R., Hogg, R. S., & Group, S. H. A. S. (2014). The cascade of HIV care in British Columbia, Canada, 1996-2011: A population-based retrospective cohort study. The Lancet Infectious Diseases, 14(1), 40–49. https://doi.org/10.1016/S1473-3099(13)70254-8
- Paula, A. A., Pires, D. F., Alves Filho, P., Lemos, K. R. V., Veloso, V. G., Grinsztejn, B., & Pacheco, A. G. (2020). Mortality profiles among people living with HIV/AIDS: Comparison between Rio de Janeiro and other federative units between 1999 and 2015. Revista Brasileira de Epidemiologia, 23, e200017. https://doi.org/10.1590/1980-549720200017
- Perlman, D. C., & Jordan, A. E. (2018). The syndemic of opioid misuse, overdose, HCV, and HIV: Structural-level causes and interventions. Current HIV/AIDS Reports, 15(2), 96–112. https://doi.org/10.1007/s11904-018-0390-3
- Roy, S., Ninkovic, J., Banerjee, S., Charboneau, R. G., Das, S., Dutta, R., Kirchner, V. A., Koodie, L., Ma, J., Meng, J., & Barke, R. A. (2011). Opioid drug abuse and modulation of immune function: Consequences in the susceptibility to opportunistic infections. Journal of Neuroimmune Pharmacology, 6(4), 442–465. https://doi.org/10.1007/s11481-011-9292-5
- Salk, R. H., Hyde, J. S., & Abramson, L. Y. (2017). Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychological Bulletin, 143(8), 783–822. https://doi.org/10.1037/bul0000102
- Salters, K. A., Parent, S., Nicholson, V., Wang, L., Sereda, P., Pakhomova, T. E., Kibel, M., Chau, W., Closson, K., Parashar, S., Barrios, R., Montaner, J. S. G., & Hogg, R. S. (2021). The opioid crisis is driving mortality among under-served people living with HIV in British Columbia, Canada. BMC Public Health, 21(1), 680–680. https://doi.org/10.1186/s12889-021-10714-y
- Samet, J. H., Tsui, J. I., Cheng, D. M., Liebschutz, J. M., Lira, M. C., Walley, A. Y., Colasanti, J. A., Forman, L. S., Root, C., Shanahan, C. W., Sullivan, M. M., Bridden, C. L., Abrams, C., Harris, C., Outlaw, K., Armstrong, W. S., & Del Rio, C. (2021). Improving the delivery of chronic opioid therapy among people living with human immunodeficiency virus: A cluster randomized clinical trial. Clinical Infectious Diseases, 73(7), e2052–e2058. https://doi.org/10.1093/cid/ciaa1025
- Smolina, K., Crabtree, A., Chong, M., Zhao, B., Park, M., Mill, C., & Schütz, C. G. (2019). Patterns and history of prescription drug use among opioid-related drug overdose cases in British Columbia, Canada, 2015-2016. Drug and Alcohol Dependence, 194, 151–158. https://doi.org/10.1016/j.drugalcdep.2018.09.019
- StatisticsCanada. (2005a). Comparability of ICD-10 and ICD-9 for Mortality Statistics in Canada. https://www150.statcan.gc.ca/n1/pub/84-548-x/2005001/t/4078902-eng.htm
- StatisticsCanada. (2005b). Comparison of ICD-9 and ICD-10 rules for selection of underlying causes of death: Selection and modification rules https://www150.statcan.gc.ca/n1/pub/84-548-x/2005001/t/4078902-eng.htm
- Statistics Canada. Census of Population. (2016). Statistics Canada Catalogue no. 98-400-X2016007. https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/dt-td/Rp-eng.cfm?TABID = 2&LANG = E&A = R&APATH = 3&DETAIL = 0&DIM = 0&FL = A&FREE = 0&GC = 01&GL = -1&GID = 1234402&GK = 1&GRP = 1&O = D&PID = 109529&PRID = 10&PTYPE = 109445&S = 0&SHOWALL = 0&SUB = 0&Temporal = 2016&THEME = 115&VID = 0&VNAMEE = &VNAMEF = &D1 = 0&D2 = 0&D3 = 0&D4 = 0&D5 = 0&D6 = 0
- St-Jean, M., Dong, X., Tafessu, H., Moore, D., Honer, W. G., Vila-Rodriguez, F., Sereda, P., Hogg, R. S., Patterson, T. L., Salters, K., Barrios, R., Montaner, J. S. G., & Lima, V. D. (2021). Overdose mortality is reducing the gains in life expectancy of antiretroviral-treated people living with HIV in British Columbia, Canada. International Journal of Drug Policy, 103195. https://doi.org/10.1016/j.drugpo.2021.103195
- VanHouten, J. P., Rudd, R. A., Ballesteros, M. F., & Mack, K. A. (2019). Drug overdose deaths among women aged 30-64 years – United States, 1999-2017. MMWR. Morbidity and Mortality Weekly Report, 68(1), 1–5. https://doi.org/10.15585/mmwr.mm6801a1
- Vold, J. H., Skurtveit, S., Aas, C., Johansson, K. A., & Fadnes, L. T. (2020). Too much or too little opioids to patients receiving opioid agonist therapy in Norway (2013–2017): A prospective cohort study. BMC Health Services Research, 20(1), 668. https://doi.org/10.1186/s12913-020-05504-y
- World Health Organization. (2009). International Classification of Diseases 9th Revisions, Clinical Modifications. http://icd9.chrisendres.com/index.php
- World Health Organization. (2019). International Statistical Classification of Diseases and Related Health Problems 10th Revisions. https://icd.who.int/browse10/2019/en
- Yazdani, K., Salters, K., Shen, T., Dolguikh, K., Trigg, J., White, R. F., Closson, K., Nanditha, N. G. A., Honer, W. G., Vila-Rodriguez, F., Lima, V. D., Montaner, J. S. G., & Barrios, R. (2022). A 20-year population-based study of all-cause and cause-specific mortality among people with concurrent HIV and psychotic disorders. AIDS (London, England), 36(13), 1851–1860. https://doi.org/10.1097/qad.0000000000003341
- Ye, X., Sutherland, J., Henry, B., Tyndall, M., & Kendall, P. R. W. (2018). At-a-glance – impact of drug overdose-related deaths on life expectancy at birth in British Columbia [Aperçu – Impact des décès par surdose de drogue sur l’espérance de vie à la naissance en Colombie-Britannique]. Health Promotion and Chronic Disease Prevention in Canada: Research, Policy and Practice, 38(6), 248–251. https://doi.org/10.24095/hpcdp.38.6.05
