ABSTRACT
AHEAD feasibility trial assessed the feasibility and acceptability of an 8-session group drumming programme aiming to improve executive function, depression and anxiety symptoms, and perceived social support in adolescents living with HIV in a rural low-income South African setting. Sixty-eight 12- to 19-year-old adolescents participated. They were individually randomised. The intervention arm (n = 34) received weekly hour-long group drumming sessions. Controls (n = 34) received no intervention. Feasibility and acceptability were assessed using rates of: enrolment; retention; attendance; logistical problems; adolescent-reported acceptability. Secondary measures included: five Oxford Cognitive Screen-Executive Function (OCS-EF) tasks; two Rapid Assessment of Cognitive and Emotional Regulation (RACER) tasks; the Self-Reporting Questionnaire-20 (SRQ-20) measuring depression and anxiety symptoms; the Multidimensional Scale of Perceived Social Support (MSPSS). All feasibility criteria were within green progression limits. Enrolment, retention, and acceptability were high. There was a positive effect on adolescent depressed mood with signal for a working memory effect. There were no significant effects on executive function or socio-emotional scales. Qualitative findings suggested socio-emotional benefits including: group belonging; decreased internalised stigma; improved mood; decreased anxiety. Group drumming is a feasible and acceptable intervention amongst adolescents living with HIV in rural South Africa. A full-scale trial is recommended.
Introduction
Need for intervention
Executive function (EF) is a group of control processes which regulates cognition and behaviour. The core EF components are working memory (storing and manipulating information held in mind); inhibition (inhibiting automatic responses or ignoring a distracting stimulus); set-shifting (switching from a previously learned rule to a new one) (Baddeley, Citation2010; Diamond, Citation2013; Li et al., Citation2015; Miyake et al., Citation2000; Miyake & Friedman, Citation2012). These core components contribute to complex EF such as planning, sequencing, problem-solving and adapting behaviour in response to new information (Diamond, Citation2013). EF is still developing during adolescence (Poon, Citation2017).
Adolescents living with HIV (ALHIV), particularly those with perinatally acquired HIV, have an increased risk of EF deficits (Nichols et al., Citation2013; Phillips et al., Citation2016; Rowe et al., Citation2021). The aetiology is likely multifactorial with biological, psychological, and social factors playing a role (Crowell et al., Citation2014). HIV can have a direct neurological impact by triggering neuroinflammation. This may persist despite antiretroviral therapy (ART) and result in excitotoxic neuronal injury with impaired synaptogenesis (Clifford & Ances, Citation2013; Crowell et al., Citation2014; Saylor et al., Citation2016). ALHIV also experience multiple psychosocial risk factors increasing their risk for depression and poorer EF (Ashaba et al., Citation2018; Betancourt et al., Citation2014; Cluver et al., Citation2008; Hermetet-Lindsay et al., Citation2017; Hochhauser et al., Citation2008; Kamau et al., Citation2012; Kim et al., Citation2014; Mburu et al., Citation2014; Mellins & Malee, Citation2013; Nabunya & Ssewamala, Citation2014; Ramaiya et al., Citation2016; Rubin & Maki, Citation2019; Semkovska et al., Citation2019). Caregiver mental health in HIV-affected households may also predict child EF with caregiver depression being associated with EF deficits (Elkington et al., Citation2011; Familiar et al., Citation2020).
EF is important because it may be associated with an array of important outcomes including physical and mental health, adherence to treatment, academic achievement, socio-economic outcomes, and risky behaviour (Agoston & Rudolph, Citation2016; Best et al., Citation2011; Davidovich et al., Citation2016; Koike et al., Citation2015; Mellins et al., Citation2009; Miller et al., Citation2012; Moffitt et al., Citation2011; Murphy, Durako, et al., Citation2001; Murphy, Wilson, et al., Citation2001; Schlam et al., Citation2013). Depression and anxiety have also been associated with poorer ART adherence, high-risk sexual behaviour, and substance use (Pozuelo et al., Citation2021).
Interventions to improve EF and mental health in ALHIV, particularly in HIV-endemic sub-Saharan Africa, are limited but urgently needed (Bhana et al., Citation2020; Vreeman et al., Citation2017). Although biological interventions (e.g., antiretrovirals) that may improve EF (Brahmbhatt et al., Citation2017) are available in many contexts, psychosocial and behavioural interventions are lacking. It has been shown to be possible to enhance EF development in children through a variety of non-pharmacological interventions including classroom curricula (Diamond et al., Citation2007), computerised cognitive training (Holmes et al., Citation2009; Thorell et al., Citation2009), aerobic physical activity (Alvarez-Bueno et al., Citation2017; Kamijo et al., Citation2011), martial arts (Lakes & Hoyt, Citation2004), mindfulness practices (Smalley et al., Citation2010) and musical training (Bergman Nutley et al., Citation2014; Moreno et al., Citation2011). Some similar interventions have also been used to improve EF in children with EF deficits (Bangirana et al., Citation2009; Cerrillo-Urbina et al., Citation2015; Klingberg et al., Citation2005), but interventions have rarely targeted ALHIV (Boivin et al., Citation2016; Webb et al., Citation2017) and those that have (computerised cognitive training; mindfulness-based stress reduction), may not be sustainable or culturally relevant in an African context.
Group drumming
Musical training places demands on EF. It has been associated with higher EF. Playing a musical instrument places demands on phonological working memory through memorisation, recital, and error monitoring with correction. It requires selective attention on specific auditory components while inhibiting distracting components and the impulse to copy others’ parts (inhibition) and switching between parts as attentional foci (set-shifting). Group musical training in school-aged children (≥6 years old) and adolescents have been found to improve verbal working memory (Flaugnacco et al., Citation2015; Guo et al., Citation2018), inhibition (D'Souza & Wiseheart, Citation2018; Fasano et al., Citation2019; Jaschke et al., Citation2018), visuospatial working memory (Portowitz et al., Citation2014), planning, and set-shifting in some studies (Abrahams & van Dooren, Citation2018; D'Souza & Wiseheart, Citation2018; Guo et al., Citation2018; Habibi et al., Citation2018). Group drumming was chosen as the musical intervention for this study because of its potential efficacy and likely acceptability and feasibility in an African context. Group drumming may be able to improve EF through direct EF training by placing demands on EF, and indirectly through enhancing psychosocial wellbeing (Diamond & Ling, Citation2016). Group drumming has been associated with an improved concentration in various populations (Flores, Citation2011; Ho et al., Citation2011; Newman et al., Citation2015). Available data support an association between superior inhibition and playing a percussive instrument (Slater et al., Citation2017, Citation2018). Drum training has been associated with increased functional connectivity between key brain regions (including the prefrontal cortices) in both healthy and clinical populations (Amad et al., Citation2017; Metzler-Baddeley et al., Citation2014).
Group drumming may also improve mood. It has been associated with improved socio-emotional health in healthy populations and those with or at high risk for mental health difficulties. Benefits have included: increased group cohesion, belonging and “connectedness” (Ascenso et al., Citation2018; Bensimon et al., Citation2008; Davis-Craig, Citation2009; Hannigan & McBride, Citation2011; Kaplan, Citation2000; Longhofer & Floersch, Citation1993; Mackinlay, Citation2014; Newman et al., Citation2015; Stone, Citation2005; Venkit et al., Citation2013; Watson et al., Citation2015; Winkelman, Citation2003); improved mood (Ascenso et al., Citation2018; Bittman et al., Citation2003, Citation2004, Citation2009; Davis-Craig, Citation2009; Fancourt, Perkins, Ascenso, Atkins, et al., Citation2016; Fancourt, Perkins, Ascenso, Carvalho, et al., Citation2016; Flores, Citation2011; Ho et al., Citation2011; Kaplan, Citation2000; Mackinlay, Citation2014; Newman et al., Citation2015; Silverman & Marcionetti, Citation2004; Watson et al., Citation2015; Winkelman, Citation2003); decreased anxiety (Bensimon et al., Citation2008; Blackett & Payne, Citation2005; Fancourt, Perkins, Ascenso, Carvalho, et al., Citation2016; Hannigan & McBride, Citation2011; Ho et al., Citation2011; Newman et al., Citation2015; Smith et al., Citation2014; Snow & D'Amico, Citation2010; Venkit et al., Citation2013); and improved self-esteem (Bittman et al., Citation2009; Flores, Citation2011; Longhofer & Floersch, Citation1993; Mackinlay, Citation2014; Silverman & Marcionetti, Citation2004; Snow & D'Amico, Citation2010; Wood et al., Citation2013). Group drumming may also increase oxytocin (related to social bonding) (Yuhi et al., Citation2017), and decrease salivary cortisol and certain pro-inflammatory cytokines (Fancourt, Perkins, Ascenso, Atkins, et al., Citation2016).
Hypothesis
We hypothesised that a group drumming programme would be a feasible and acceptable intervention amongst ALHIV in rural South Africa, and be able to improve their EF, reduce depression and anxiety symptoms, and increase perceived social support.
Objectives
The primary objective was to assess intervention feasibility and acceptability in the context. Secondary objectives were to assess the proof-of-concept of an effect on EF, depression and anxiety symptoms, and perceived social support.
Materials and methods
Intervention development
The intervention was developed by a multidisciplinary team using a Theory of Change framework (Rowe et al., Citation2023).
Study design and participants
The study was embedded in the MRC/Wits Rural Public Health and Health Transitions (Agincourt) Research Unit’s Health and Socio-demographic Surveillance System (HDSS), near the Mozambican border. The setting is rural with poor infrastructure and high levels of poverty, unemployment and outmigration (Sartorius et al., Citation2014). The feasibility study was an individually randomised controlled trial (RCT) with a non-blind, parallel group, two-arm design with 1:1 allocation ratio and passive controls (registration number: PACTR201804003332337). Ethics approval was provided by the University of Oxford Tropical Research Ethics Committee (REC), the University of Witwatersrand Human REC (Medical) and the Mpumalanga Provincial Health REC. The target sample size was at least 50 participants so that we could estimate an enrolment rate of 80% within a 95% confidence interval of ±10%. We recruited male and female 12- to 19-year-old adolescents with chronic diseases (including HIV) and their caregivers at four primary care facilities (clinics) within the Agincourt HDSS. Participants required a known HIV status (positive or tested negative within the last three months) and willingness to share their status with the study team. Exclusion criteria included: profound hearing loss; current severe infective illness; another uncontrolled medical condition; cerebral palsy; known intellectual disability due to a non-HIV cause; uncontrolled epilepsy; recent central nervous system infections; current or previous brain malignancies; a previous stroke; a history of a significant head injury; or currently more than four months’ pregnant. Informed consent was obtained from all adult participants and caregivers of minors. Minors assented. Participants were allocated to the intervention and control arms by means of simple random sampling.
Intervention
Controls received no intervention. Those randomised to the intervention received weekly hour-long sessions in a private community hall or clinic (public primary care facility) room led by a trained facilitator for 8 weeks. Participants also received weekly telephonic reminders.
The first intervention session involved introductions (using a rhythmical game), joint group norm setting, and learning the posture and technique for playing the three basic tones with associated vocalisations: bass (“du”), high (“ke”) and slap (“pa”). The participants learned a rhythmic accompaniment, melody, and lyrics for a greeting song. Finally, participants were taught a farewell song and encouraged to practise the rhythms at home.
The basic structure of sessions 2–8 was: greeting song; musical game; three group songs chosen by the adolescents in sessions 1–2; farewell song. The facilitator gradually introduced 1–3 core rhythms (sequences comprising the three basic tones) of increasing complexity to accompany each song. Initially, these rhythms were played in series; later they were played by subgroups in parallel with switching.
The EF demands were increased progressively by:
Increasing working memory load through an increasing number, length and complexity of rhythms played in each session.
Increasing inhibitory demands by introducing competing subgroup rhythm/s within the circle, initially splitting the group into two halves, and later having subgroups interspersed within the circle.
Increasing set-shifting demands by increasing the frequency of subgroup rhythmic switching.
Outcomes and outcome measures
All participants and caregivers completed baseline and endline tablet-based assessments in the Tsonga language facilitated by a local fieldworker according to their familiarity with mobile technology. All questions and task instructions were translated by Agincourt HDSS staff or fieldworkers with cross-checks.
Primary outcome measures
Feasibility: rates of enrolment and retention, attendance, and logistical problems based on logs kept by the field supervisor.
Acceptability: attendance rates and acceptability ratings from the early study exit and endline acceptability questionnaires (including qualitative open-ended questions used for qualitative data analysis and reasons for non-attendance).
We defined our progression criteria for progression from a feasibility trial through to a full-scale RCT () using a red/amber/green traffic light system (Avery et al., Citation2017).
Table 1. Primary outcome progression criteria for progression to a full-scale randomised controlled trial.
Secondary outcome measures
Research Electronic Data Capture (REDCap) electronic socio-demographic and behavioural questionnaires (Harris et al., Citation2009), five Oxford Cognitive Screen – Executive Function (OCS-EF) (Rowe, Duta et al., Citation2021) and two Rapid Assessment of Cognitive and Emotional Regulation (RACER) cognitive tasks (Ford et al., Citation2019) were administered. After each cognitive task, the fieldworker selected a testing condition from a pre-defined list (including the categories: no issue; participant-related issues; technical issues; fieldworker issues; other). Task data were only included if the testing condition was “no issue”.
The difference between the intervention and control groups on the endline mean scores (controlling for baseline scores, the highest level of education attained, and socio-economic status [asset index]) for the following cognitive task and questionnaire measures were used as secondary outcomes.
Seven cognitive tasks, all designed to tap complementary EFs, were used:
▪ Five OCS-EF tasks, validated for use amongst adolescents in the Agincourt HDSS (Rowe, Duta et al., Citation2021):
trails (set-shifting)
Iowa Gambling Task (affective decision-making)
rule-finding (set-shifting)
emotional go/no-go (affective inhibition)
digit recall backwards (verbal working memory).
▪ Two RACER tasks, tablet-based tasks designed for and used in various low – and middle-income countries (LMICs) by trained laypeople (Ford et al., Citation2019) but not yet validated in South Africa:
dot location recall (visuospatial working memory)
Simon task (non-affective inhibition)
Two questionnaires were used:
World Health Organisation’s Self-Reporting Questionnaire 20 (SRQ-20), a 20-item questionnaire screening for depression and anxiety symptoms (administered to both adolescents and caregivers), including an item examining depressed mood. It was developed for use in primary care settings by workers with limited mental health training (Ali et al., Citation2016; Beusenberg & Orley, Citation1994). It has been validated in South Africa (Cherian et al., Citation1998; van der Westhuizen et al., Citation2016).
Multidimensional Scale of Perceived Social Support (MSPSS), a 12-item questionnaire that assesses perceived support from three sources: family, friends, and a significant other (Zimet et al., Citation1988). It has been validated for use amongst adolescents in South Africa (Bruwer et al., Citation2008).
Fieldworker recruitment, training, and supervision
Three assessment fieldworkers and 1 intervention fieldworker were trained. All fieldworkers received a 10-day training. The intervention fieldworker practised drumming daily during the study.
Statistical analysis
Data analysis was performed in Stata 14 by an independent analyst. Feasibility and acceptability were analysed by comparing the following rates with the progression criteria: enrolment, attendance, attrition, positivity towards the intervention, and mean satisfaction. Intervention participant data were analysed using a per-protocol analysis with the minimum dose being six sessions (i.e., 75% attendance). Confidence intervals are reported with these rates, calculated using the Clopper–Pearson method. Cognitive and socio-emotional scale outcomes were analysed using linear regression controlling for baseline scores, highest education level attained, and socio-economic status (Berthelsen et al., Citation2017; Noble et al., Citation2013). Qualitative data from the acceptability questionnaire was analysed using reflexive thematic analysis with an inductive, semantic approach in which coding and theme development were directed by the explicit data content. The study was not powered to do a formal efficacy analysis.
Results
Sample characteristics
All participants were African Tsonga-speakers. See CONSORT diagram () and tables for participant sociodemographic characteristics and musical experience (), clinical characteristics (), perinatal and psychiatric history () and caregiver sociodemographic and clinical data (). The sample had a low median CD4 cell count and low rates of virological suppression. Cognitive testing conditions were valid for ≥90% of participants for all baseline and endline tasks (Appendix 2, Tables A1 and A2). Interruptions were the main cause for invalid testing conditions. Baseline cognitive and socioemotional scale scores are summarised in . The baseline internal consistency coefficients were acceptable (Cronbach’s alpha > 0.70) for the adolescent self-reported MSPSS (α = 0.71) and SRQ-20 (α = 0.72), and the caregiver SRQ-20 (α = 0.89) (Tavakol & Dennick, Citation2011).
Figure 1. AHEAD Study CONSORT flow diagram.
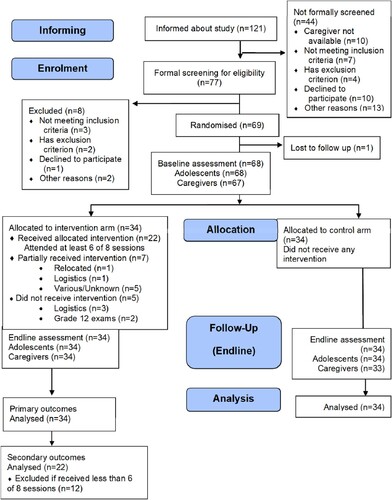
Table 2. Participant baseline sociodemographic characteristics.
Table 3. Participant clinical characteristics.
Table 4. Participant perinatal and psychiatric history.
Table 5. Caregiver baseline sociodemographic and clinical characteristics.
Table 6. Baseline summary statistics of cognitive and socio-emotional scale scores of participants in both trial arms with adequate conditions of test.
Primary outcomes: feasibility and acceptability
Enrolment and retention
Seventy-seven adolescents underwent formal eligibility screening. Seventy-two adolescents were eligible for inclusion. Sixty-nine adolescents (96% [95% CI 88–99]) enrolled and underwent randomisation to the intervention (n = 34) and control (n = 35) arms. There was one early loss to follow-up (1% [95% CI 0–8]) with no further study attrition; the study retention rate was 99% [95% CI 92–100].
Attendance (intervention arm adherence)
In the intervention arm, 22 (65% [95% CI 46–80]) participants (“compliers”) attended 6–8 drumming sessions (75% attendance; data analysed). 12 (35% [95% CI 20–54]) participants (“non-compliers”) attended <75% of sessions: four (12%) attended 4 or 5 sessions, three (9%) attended 1 or 2 sessions, five (15%) attended none. Average weekly attendance was 66% (95% CI 53–79) (). Reasons reported for non-attendance were logistical (e.g., distance and transport issues or other academic, childcare, or extracurricular commitments) or personal (e.g., acute illness, fatigue). No adverse events were reported. After baseline screening, five caregivers and three adolescents were identified requiring referral to local outpatient health/social services (clinic professional nurse, clinic social worker or district hospital psychiatric medical officer) for further management for high SRQ-20 scores. Non-compliers were more likely to have behaviourally acquired HIV and not be school-enrolled ().
Figure 2. Plot of drumming session attendance rate with 95% confidence intervals in Weeks 1–8.
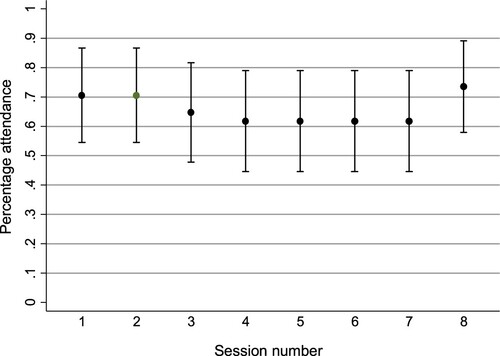
Table 7. Comparison of baseline characteristics of intervention arm compliers (attended 75% or more) versus non-compliers (attended < 75%).
Logistical problems
The drumming facilitation trainer travelled from another province. The limited availability of trainers locally is a potential constraint for scalability and sustainability; however, it would be possible for a trainer to equip local drumming facilitators to train other facilitators through longer, more intensive training so the process could become locally self-sustainable. Furthermore, drumming is already popular in local communities and incorporated in traditional rituals. There were 25 logistical problems recorded by the field supervisor. Most issues were minor and potentially avoidable. The drumming venues had basic amenities, fans, and were accessible by public transport. Transport fare reimbursement facilitated attendance, particularly for participants from low-income households. Distance to the venue was a barrier to participation for some when venues were in neighbouring villages. Having a venue in each village would likely facilitate attendance and reduce travel costs and safety concerns in a full-scale RCT. Intervention sessions were held on weekdays after school. Attendance rates dropped slightly during school examinations and vacation periods.
Acceptability and qualitative outcomes based on endline acceptability survey
Post-intervention, 94% (95% CI 80–99) of intervention arm participants felt positive towards the programme, 82% (95% CI 65–93) would recommend it to others, and 97% (95% CI 85–100) would participate again. Satisfaction ratings on a visual analogue scale (1–10) were high (mean 8.7 [95% CI 8.4–9.1]). Perceived programme effects were generally positive with most feeling that participation helped to some extent with their ability to concentrate at school (91% [95% CI 76–98]), and overall mood (97% [95% CI 85–100]).
The coding tree for the intervention arm participants’ qualitative data appears in below.
Figure 3. Intervention arm qualitative data coding tree.
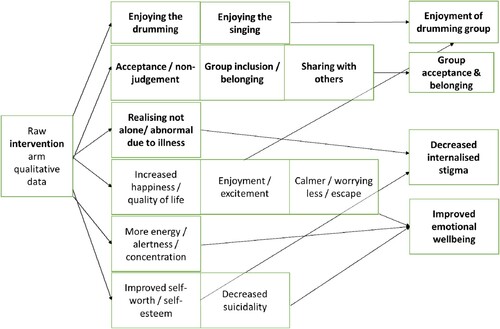
The following recurring themes emerged from the intervention participants’ qualitative data:
(1) Enjoyment of the drumming group: Enjoyment of the musical elements was a common theme.It’s like waiting for Christmas. The excitement and looking forward to it. It’s nice to have something to look forward to. It feels good to be here. – Participant #1.
(2) Finding acceptance and belonging in the circle: Many mentioned finding the circle to be non-judgemental and a space where they felt accepted. It was a space for solidarity and friendship.I enjoy being here with all the girls. I believe it is improving my self-esteem. It makes me happy to be with the group. I was struggling to make friends before but now I feel like I have friends. It makes me happy. I enjoy the sessions. – Participant #2.I am very happy to be part of the group. It makes me feel good about myself being around people that don’t judge me. – Participant #3.“It is nice to finally find a group of friends that accept me as I am.” – Participant #4.
(3) Decreased internalised stigma with improvements in self-esteem was another common theme.[I] give thanks to the study for giving me courage to keep going and not to commit suicide which I was considering before. I did not value myself before the study because of my status but now I value myself more. I’m not alone with this chronic disease. There are many other people living with the disease. – Participant #5.
Improving emotional wellbeing: Many described feelings of happiness and improved quality of life, with others describing less anxiety in general or relating to their HIV status. One participant (Participant #1) explained: “It helps us forget about other things going on in our lives.” Others felt more energised since taking part. A few mentioned decreased suicidality.
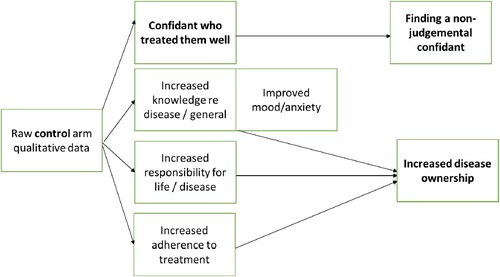
Some control group participants also reported perceived benefits from study participation with the following themes emerging from the study acceptability questionnaire:
(1) Finding a non-judgemental confidant (through routine study visits): As one participant (Participant #6) described: “I was given a chance to talk to someone.” Another participant (Participant #7) explained: “I found people that spoke to me in a good way despite my situation.”
(2) Disease ownership: Some participants mentioned increased disease knowledge and ownership and treatment adherence.
The coding tree for the control arm participants’ qualitative data appears in below.
Figure 4. Control arm qualitative data coding tree.
Progression criteria
See for the summarised primary outcome results compared to progression criteria to a full-scale RCT.
Table 8. Primary outcome results compared to progression criteria for progression to a full-scale randomised controlled trial.
Secondary outcome measures
The study had approximately 82% power (calculated using G*Power 3.1.9.4) (Faul et al., Citation2009) to detect a large effect size (Cohen’s d = 0.8); 43% to detect a medium effect size (Cohen’s d = 0.5) and 11% (i.e., insufficient) to detect a small effect size (Cohen’s d = 0.2). Although there was no significant intervention effect on EF (inhibition, working memory or set-shifting tasks), adolescent total SRQ-20 (depression and anxiety symptoms), or MSPSS (perceived social support) scores in multivariable regression analyses comparing the intervention arm to the control arm (), effects were in the predicted direction, but small: working memory (digit recall backwards mean difference 0.28 (95% CI −0.61, 1.16); P = 0.532; dot recall mean difference 6.78 (95% CI −15.22, 28.78); P = 0.537), and adolescent depression and anxiety symptoms (SRQ-20) (SRQ-20 mean difference −0.44 (95% CI −1.94, 1.06); P = 0.556). There was an intervention effect on adolescent depressed mood (beta = −0.15; 95% CI −0.29, −0.02; P = 0.030) and a marginal effect on caregiver total depression and anxiety symptoms (beta = −2.33; 95% CI −4.82, 0.17; P = 0.067) ().
Table 9. Comparison of cognitive and socio-emotional scale outcomes using multivariable regression models (controlling for baseline score, education level, socio-economic status) of intervention arm compliers (attended 75% or more of intervention) versus control arm.
Discussion
Main findings
A short-term group drumming intervention was feasible and acceptable amongst ALHIV in rural South Africa. All feasibility criteria were within the green progression limits. There were high enrolment and retention rates. Although there was a 24% initial drop-off in attendance overall attendance rates remained within the required limits and were relatively stable throughout the programme suggesting acceptability. Adolescent acceptability and satisfaction ratings were overwhelmingly positive. This feasibility study supports the progression to a formal pilot and full-scale RCT. There was a signal for a small effect on working memory but not set-shifting or inhibition. EF would be the primary outcome analysing efficacy in a full-scale RCT. This was a feasibility trial, and therefore not powered to detect smaller group differences. Possible reasons for the lack of a notable effect include an insufficient dose (too few hours). Longer EF training interventions over many months or years have shown better results (Diamond & Ling, Citation2016; Jaeggi et al., Citation2008). Short-term musical training alone may be insufficient to improve EF in adolescents in a context with multiple threats to EF development, including poor nutrition, low-quality education, etc.
There was a positive effect on depressed mood, supported by the qualitative data. Interestingly while there were no significant differences in total depression and anxiety scores (SRQ-20), there was a trend for improved caregiver scores in the intervention group compared to controls, suggesting possible positive family effects. There were various perceived socio-emotional benefits, including finding acceptance and belonging, decreased internalised stigma, and improved emotional well-being with improved mood and decreased anxiety (Cohen & Wills, Citation1985; Collishaw et al., Citation2016). Despite these qualitative findings, there were no significant changes in the quantitative measure of perceived social support, possibly because the intervention only improved perceived social support in a small proportion or because the measure was insensitive to small changes in perceived peer social support.
Qualitative data suggested that control arm participants also experienced non-specific effects from participation, with perceived benefits of having the fieldworker as a confidant and experiencing increased disease ownership. This suggests that this population of ALHIV seem to benefit from increased confidential individual contact time.
Strengths and limitations
To our knowledge, this was the first feasibility study assessing an intervention aiming to improve EF exclusively focused on ALHIV in a LMIC. It tested an intervention widely popular in Africa. It included a comprehensive EF battery, including affective tasks.
There were study limitations. Firstly, the small sample size entailed in a feasibility study meant it was underpowered to detect intervention effects. Secondly, there were a few limitations related to measures. There were no measures of EF in real-life contexts or positive affective states. The Tsonga versions of questionnaires were not all validated. Field-based cognitive testing may have more measurement error versus laboratory testing. Finally, the study used a health facility-based sampling frame which may not be representative of ALHIV not linked to care.
Scalability and sustainability
Certain intervention components (e.g., norms and rhythms) are easier to standardise and replicate across contexts. Other components (e.g., specific melodies and lyrics) would need adaptation to make the intervention more engaging and acceptable in the particular population and context. It will be challenging to maintain intervention quality at scale without skilled oversight. It will require skilled trainers, supervisors, and fieldworkers with the key characteristics to be good drum group facilitators.
Ten local schoolteachers, rehabilitation, and non-government organisation (NGO) staff received drum group facilitation training alongside the fieldworkers. The drums were donated to their institutions for use post-study. The NGO planned to use the drums for adolescent support groups at the local clinics. Potential implementation barriers in government facilities include human resource constraints and the lack of facilitating factors (e.g., snacks, transport fare and session reminders) without additional funding. A potential path to sustainability would be to train adolescents to run groups as a voluntary peer-led programme (Maticka-Tyndale & Barnett, Citation2010).
Conclusions
Executive function difficulties, depression, and anxiety are relatively common amongst adolescents with HIV (ALHIV) in sub-Saharan Africa, yet to date there is limited research on interventions to address these challenges. This feasibility study adds useful evidence to the literature on interventions aiming to improve executive function, as well as depression and anxiety symptoms in ALHIV in sub-Saharan Africa Group drumming is a feasible and acceptable intervention amongst ALHIV in rural South Africa with subjective socio-emotional benefits and an improvement in depressed mood. There was signal for a small effect on working memory and set-shifting and total caregiver depression and anxiety symptoms; however, there were no significant effects on executive function, self-report total depression and anxiety symptoms, or perceived social support scales in this feasibility trial. Skilled human resource and financial constraints will likely be the main challenges to scalability. The high rates of enrolment, attendance, retention, and acceptability, and the promising socio-emotional effects suggest that this intervention should be considered for progression to a formal pilot with subsequent full-scale randomised controlled trial; however, the primary outcome would likely shift to depression. Further research is required to assess effects on executive function, e.g., a more intensive intervention could be tested.
Supplemental Material
Download MS Word (18.7 KB)Supplemental Material
Download MS Word (85 KB)Acknowledgements
Thank you to the staff at the MRC/Wits Rural Public Health and Health Transitions (Agincourt) Research Unit for making this study possible. A particular thank you to Rhian Twine, Simon Khoza, Floidy Wafawanaka, Xavier Gómez-Olivé, Khanyisa Ngobeni, Nkosinathi Masilela, Walter Ndlovu, and Weekend Khoza. Thanks to the members of the community advisory board. Thank you to the fieldworkers who implemented this study protocol and Unathi Khosa, the drumming group facilitator. Finally, thanks to the adolescents and caregivers who participated.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Abrahams, T. P., & van Dooren, J. C. (2018). Musical attention control training (MACT) in secure residential youth care: A randomised controlled pilot study. The Arts in Psychotherapy, 57, 80–87. https://doi.org/10.1016/j.aip.2017.10.008
- Agoston, A. M., & Rudolph, K. D. (2016). Interactive contributions of cumulative peer stress and executive function deficits to depression in early adolescence. The Journal of Early Adolescence, 36(8), 1070–1094. https://doi.org/10.1177/0272431615593176
- Ali, G.-C., Ryan, G., & De Silva, M. J. (2016). Validated screening tools for common mental disorders in Low and middle income countries: A systematic review. PLoS One, 11(6), e0156939. https://doi.org/10.1371/journal.pone.0156939
- Alvarez-Bueno, C., Pesce, C., Cavero-Redondo, I., Sanchez-Lopez, M., Martinez-Hortelano, J. A., & Martinez-Vizcaino, V. (2017). The effect of physical activity interventions on children’s cognition and metacognition: A systematic review and meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 56(9), 729–738. https://doi.org/10.1016/j.jaac.2017.06.012
- Amad, A., Seidman, J., Draper, S. B., Bruchhage, M. M. K., Lowry, R. G., Wheeler, J., Robertson, A., Williams, S. C. R., & Smith, M. S. (2017). Motor learning induces plasticity in the resting brain—Drumming up a connection. Cerebral Cortex, 27(3), 2010–2021. https://doi.org/10.1093/cercor/bhw048
- Ascenso, S., Perkins, R., Atkins, L., Fancourt, D., & Williamon, A. (2018). Promoting well-being through group drumming with mental health service users and their carers. International Journal of Qualitative Studies on Health and Well-being, 13(1), 1484219. https://doi.org/10.1080/17482631.2018.1484219
- Ashaba, S., Cooper-Vince, C., Maling, S., Rukundo, G. Z., Akena, D., & Tsai, A. C. (2018). Internalized HIV stigma, bullying, major depressive disorder, and high-risk suicidality among HIV-positive adolescents in rural Uganda. Global Mental Health, 5, e22. https://doi.org/10.1017/gmh.2018.15
- Avery, K. N. L., Williamson, P. R., Gamble, C., O'Connell Francischetto, E., Metcalfe, C., Davidson, P., Williams, H., & Blazeby, J. M. (2017). Informing efficient randomised controlled trials: Exploration of challenges in developing progression criteria for internal pilot studies. BMJ Open, 7(2), e013537. https://doi.org/10.1136/bmjopen-2016-013537
- Baddeley, A. (2010). Working memory. Current Biology, 20(4), R136–R140. https://doi.org/10.1016/j.cub.2009.12.014
- Bangirana, P., Giordani, B., John, C. C., Page, C., Opoka, R. O., & Boivin, M. J. (2009). Immediate neuropsychological and behavioral benefits of computerized cognitive rehabilitation in Ugandan pediatric cerebral malaria survivors. Journal of Developmental and Behavioral Pediatrics, 30(4), 310–318. https://doi.org/10.1097/DBP.0b013e3181b0f01b
- Bensimon, M., Amir, D., & Wolf, Y. (2008). Drumming through trauma: Music therapy with post-traumatic soldiers. The Arts in Psychotherapy, 35(1), 34–48. https://doi.org/10.1016/j.aip.2007.09.002
- Bergman Nutley, S., Darki, F., & Klingberg, T. (2014). Music practice is associated with development of working memory during childhood and adolescence. Frontiers in Human Neuroscience, 7, 926. https://doi.org/10.3389/fnhum.2013.00926
- Berthelsen, D., Hayes, N., White, S. L. J., & Williams, K. E. (2017). Executive function in adolescence: Associations with child and family risk factors and self-regulation in early childhood. Frontiers in Psychology, 8, 903. https://doi.org/10.3389/fpsyg.2017.00903
- Best, J. R., Miller, P. H., & Naglieri, J. A. (2011). Relations between executive function and academic achievement from ages 5 to 17 in a large, representative national sample. Learning and Individual Differences, 21(4), 327–336. https://doi.org/10.1016/j.lindif.2011.01.007
- Betancourt, T., Scorza, P., Kanyanganzi, F., Fawzi, M. C., Sezibera, V., Cyamatare, F., Beardslee, W., Stulac, S., Bizimana, J. I., Stevenson, A., & Kayiteshonga, Y. (2014). HIV and child mental health: A case-control study in Rwanda. Pediatrics, 134(2), e464–e472. https://doi.org/10.1542/peds.2013-2734
- Beusenberg, M., & Orley, J. (1994). A user’s guide to the Self Reporting Questionnaire (SRQ). WHO. http://apps.who.int/iris/bitstream/10665/61113/1/WHO_MNH_PSF_94.8.pdf
- Bhana, A., Abas, M. A., Kelly, J., van Pinxteren, M., Mudekunye, L. A., & Pantelic, M. (2020). Mental health interventions for adolescents living with HIV or affected by HIV in low- and middle-income countries: Systematic review. BJPsych Open, 6(5), e104–e104. https://doi.org/10.1192/bjo.2020.67
- Bittman, B., Bruhn, K. T., Stevens, C., Westengard, J., & Umbach, P. O. (2003). Recreational music-making: A cost-effective group interdisciplinary strategy for reducing burnout and improving mood states in long-term care workers. Advances in Mind-body Medicine, 19(3-4), 4–15. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc4&AN=2003-10365-002
- Bittman, B., Dickson, L., & Coddington, K. (2009). Creative musical expression as a catalyst for quality-of-life improvement in inner-city adolescents placed in a court-referred residential treatment program. Advances in Mind-Body Medicine, 24(1), 8–19. https://pubmed.ncbi.nlm.nih.gov/20671333/
- Bittman, B. B., Snyder, C., Bruhn, K. T., Liebfreid, F., Stevens, C. K., Westengard, J., & Umbach, P. O. (2004). Recreational music-making: An integrative group intervention for reducing burnout and improving mood states in first year associate degree nursing students: Insights and economic impact. International Journal of Nursing Education Scholarship, 1(1), 12. https://doi.org/10.2202/1548-923x.1044.
- Blackett, P. S., & Payne, H. L. (2005). Health rhythms: A preliminary inquiry into group-drumming as experienced by participants on a structured day services programme for substance-misusers. Drugs: Education, Prevention and Policy, 12(6), 477–491. https://doi.org/10.1080/09687630500342881
- Boivin, M. J., Nakasujja, N., Sikorskii, A., Opoka, R. O., & Giordani, B. (2016). A randomized controlled trial to evaluate if computerized cognitive rehabilitation improves neurocognition in Ugandan children with HIV. AIDS Research and Human Retroviruses, 32(8), 743–755. https://doi.org/10.1089/aid.2016.0026
- Brahmbhatt, H., Boivin, M., Ssempijja, V., Kagaayi, J., Kigozi, G., Serwadda, D., Violari, A., & Gray, R. H. (2017). Impact of HIV and antiretroviral therapy on neurocognitive outcomes Among school-aged children. Jaids-Journal of Acquired Immune Deficiency Syndromes, 75(1), 1–8. <Go to ISI>://WOS:000399376500008.
- Bruwer, B., Emsley, R., Kidd, M., Lochner, C., & Seedat, S. (2008). Psychometric properties of the multidimensional scale of perceived social support in youth. Comprehensive Psychiatry, 49(2), 195–201. https://doi.org/10.1016/j.comppsych.2007.09.002
- Cerrillo-Urbina, A. J., Garcia-Hermoso, A., Sanchez-Lopez, M., Pardo-Guijarro, M. J., Santos Gomez, J. L., & Martinez-Vizcaino, V. (2015). The effects of physical exercise in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis of randomized control trials. Child: Care, Health and Development, 41(6), 779–788. https://doi.org/10.1111/cch.12255
- Cherian, V. I., Peltzer, K., & Cherian, L. (1998). The factor-structure of the self reporting questionnaire (SRQ-20) in South Africa. East African Medical Journal, 75(11), 654–656. https://pubmed.ncbi.nlm.nih.gov/10065179/
- Clifford, D. B., & Ances, B. M. (2013). HIV-associated neurocognitive disorder [review]. The Lancet Infectious Diseases, 13(11), 976–986. https://doi.org/10.1016/S1473-3099(13)70269-X
- Cluver, L. D., Gardner, F., & Operario, D. (2008). Effects of stigma on the mental health of adolescents orphaned by AIDS. Journal of Adolescent Health, 42(4), 410–417. https://doi.org/10.1016/j.jadohealth.2007.09.022
- Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357. https://psycnet.apa.org/doi/10.1037/0033-2909.98.2.310
- Collishaw, S., Hammerton, G., Mahedy, L., Sellers, R., Owen, M. J., Craddock, N., Thapar, A. K., Harold, G. T., Rice, F., & Thapar, A. (2016). Mental health resilience in the adolescent offspring of parents with depression: A prospective longitudinal study. The Lancet Psychiatry, 3(1), 49–57. https://doi.org/10.1016/S2215-0366(15)00358-2
- Crowell, C. S., Malee, K. M., Yogev, R., & Muller, W. J. (2014). Neurologic disease in HIV-infected children and the impact of combination antiretroviral therapy. Reviews in Medical Virology, 24(5), 316–331. https://doi.org/10.1002/rmv.1793
- Davidovich, S., Collishaw, S., Thapar, A. K., Harold, G., Thapar, A., & Rice, F. (2016). Do better executive functions buffer the effect of current parental depression on adolescent depressive symptoms? Journal of Affective Disorders, 199, 54–64. https://doi.org/10.1016/j.jad.2016.03.049
- Davis-Craig, A.-L. (2009). Building community: African dancing and drumming in the little village of tallahassee. Florida State University.
- Diamond, A. (2013). Executive functions. Annual Review of Psychology, 64, 135–168. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4084861/pdf/nihms-602706.pdf
- Diamond, A., Barnett, W. S., Thomas, J., & Munro, S. (2007). Preschool program improves cognitive control. Science, 318(5855), 1387–1388. https://doi.org/10.1126/science.1151148
- Diamond, A., & Ling, D. S. (2016). Conclusions about interventions, programs, and approaches for improving executive functions that appear justified and those that, despite much hype, do not. Developmental Cognitive Neuroscience, 18, 34–48. https://doi.org/10.1016/j.dcn.2015.11.005
- D'Souza, A. A., & Wiseheart, M. (2018). Cognitive effects of music and dance training in children. Archives of Scientific Psychology, 6(1), 178–192. https://doi.org/10.1037/arc0000048
- Elkington, K. S., Robbins, R. N., Bauermeister, J. A., Abrams, E. J., McKay, M., & Mellins, C. A. (2011). Mental health in youth infected with and affected by HIV: The role of caregiver HIV. Journal of Pediatric Psychology, 36(3), 360–373. https://doi.org/10.1093/jpepsy/jsq094
- Familiar, I., Chernoff, M., Ruisenor-Escudero, H., Laughton, B., Joyce, C., Fairlie, L., Vhembo, T., Kamthunzi, P., Barlow-Barlow, L., Zimmer, B., McCarthy, K., & Boivin, M. J. (2020). Association between caregiver depression symptoms and child executive functioning. Results from an observational study carried out in four sub-saharan countries. AIDS Care, 32(4), 486–494. https://doi.org/10.1080/09540121.2019.1659917
- Fancourt, D., Perkins, R., Ascenso, S., Atkins, L., Kilfeather, S., Carvalho, L., Steptoe, A., & Williamon, A. (2016). Group drumming modulates cytokine response in mental health services users: A preliminary study. Psychotherapy and Psychosomatics, 85(1), 53–55. https://doi.org/10.1159/000431257
- Fancourt, D., Perkins, R., Ascenso, S., Carvalho, L. A., Steptoe, A., & Williamon, A. (2016). Effects of group drumming interventions on anxiety, depression, social resilience and inflammatory immune response among mental health service users [empirical study; quantitative study; treatment outcome]. PLoS One, 11(3), e0151136. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc13&AN=2016-13301-001
- Fasano, M. C., Semeraro, C., Cassibba, R., Kringelbach, M. L., Monacis, L., de Palo, V., Vuust, P., & Brattico, E. (2019). Short-Term orchestral music training modulates hyperactivity and inhibitory control in school-Age children: A longitudinal behavioural study. Frontiers in Psychology, 10, 750–750. https://doi.org/10.3389/fpsyg.2019.00750
- Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*power 3.1: Tests for correlation and regression analyses [journal article]. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/brm.41.4.1149
- Flaugnacco, E., Lopez, L., Terribili, C., Montico, M., Zoia, S., & Schon, D. (2015). Music training increases phonological awareness and Reading skills in developmental dyslexia: A randomized control trial. PLoS ONE, 10(9), e0138715. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc12&AN=2016-03408-001
- Flores, K. (2011). African drumming as a medium to promote emotional and social well-being of children aged 7 to 12 in residential care. University of Pretoria.
- Ford, C. B., Kim, H. Y., Brown, L., Aber, J. L., & Sheridan, M. A. (2019). A cognitive assessment tool designed for data collection in the field in low- and middle-income countries. Research in Comparative and International Education, 14(1), 141–157. https://doi.org/10.1177/1745499919829217
- Guo, X., Ohsawa, C., Suzuki, A., & Sekiyama, K. (2018). Improved digit span in children after a 6-week intervention of playing a musical instrument: An exploratory randomized controlled trial. Frontiers in Psychology, 8, 2303. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc14&AN=2018-02029-001
- Habibi, A., Damasio, A., Ilari, B., Elliott Sachs, M., & Damasio, H. (2018). Music training and child development: A review of recent findings from a longitudinal study. Annals of the New York Academy of Sciences, 1423(1), 73–81. https://doi.org/10.1111/nyas.13606
- Hannigan, P. D., & McBride, D. L. (2011). Drumming with intimate partner violence clients: Getting into the beat; therapists’ views on the use of drumming in family violence treatment groups. Canadian Art Therapy Association Journal, 24(1), 2–9. https://doi.org/10.1080/08322473.2011.11434787
- Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381. https://doi.org/10.1016/j.jbi.2008.08.010
- Hermetet-Lindsay, K. D., Correia, K. F., Williams, P. L., Smith, R., Malee, K. M., Mellins, C. A., Rutstein, R. M., & Pediatric, H. I. V. A. C. S. (2017). Contributions of disease severity, psychosocial factors, and cognition to behavioral functioning in US youth perinatally exposed to HIV. AIDS and Behavior, 21(9), 2703–2715. https://doi.org/10.1007/s10461-016-1508-5
- Ho, P., Tsao, J. C., Bloch, L., & Zeltzer, L. K. (2011). The impact of group drumming on social-emotional behavior in low-income children. Evidence-Based Complementary and Alternative Medicine, 2011, 250708. https://doi.org/10.1093/ecam/neq072
- Hochhauser, C., Gaur, S., Marone, R., & Lewis, M. (2008). The impact of environmental risk factors on HIV-associated cognitive decline in children [empirical study; longitudinal study; retrospective study; quantitative study]. AIDS Care, 20(6), 692–699. https://doi.org/10.1080/09540120701693982
- Holmes, J., Gathercole, S. E., & Dunning, D. L. (2009). Adaptive training leads to sustained enhancement of poor working memory in children. Developmental Science, 12(4), F9–15. https://doi.org/10.1111/j.1467-7687.2009.00848.x
- Jaeggi, S. M., Buschkuehl, M., Jonides, J., & Perrig, W. J. (2008). Improving fluid intelligence with training on working memory. Proceedings of the National Academy of Sciences, 105(19), 6829–6833. https://doi.org/10.1073/pnas.0801268105
- Jaschke, A. C., Honing, H., & Scherder, E. J. A. (2018). Longitudinal analysis of music education on executive functions in primary school children [article]. Frontiers in Neuroscience, 12(11), 103. https://doi.org/10.3389/fnins.2018.00103
- Kamau, J. W., Kuria, W., Mathai, M., Atwoli, L., & Kangethe, R. (2012). Psychiatric morbidity among HIV-infected children and adolescents in a resource-poor Kenyan urban community. AIDS Care, 24(7), 836–842. https://doi.org/10.1080/09540121.2011.644234
- Kamijo, K., Pontifex, M. B., O'Leary, K. C., Scudder, M. R., Wu, C.-T., Castelli, D. M., & Hillman, C. H. (2011). The effects of an afterschool physical activity program on working memory in preadolescent children. Developmental Science, 14(5), 1046–1058. https://doi.org/10.1111/j.1467-7687.2011.01054.x
- Kaplan, C. D. (2000). The short term effects of small group hand drumming on mood, group cohesiveness and rhythm perception [Dissertation Empirical Study]. PsycINFO. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc3&AN=2000-95010-126
- Kim, M. H., Mazenga, A. C., Devandra, A., Ahmed, S., Kazembe, P. N., Yu, X., Nguyen, C., & Sharp, C. (2014). Prevalence of depression and validation of the beck depression inventory-II and the children’s depression inventory-short amongst HIV-positive adolescents in Malawi. Journal of the International AIDS Society, 17(1), 18965. https://doi.org/10.7448/ias.17.1.18965
- Klingberg, T., Fernell, E., Olesen, P. J., Johnson, M., Gustafsson, P., Dahlstrom, K., Gillberg, C. G., Forssberg, H., & Westerberg, H. (2005). Computerized training of working memory in children with ADHD–a randomized, controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 44(2), 177–186. https://doi.org/10.1097/00004583-200502000-00010
- Koike, S., Hardy, R., & Richards, M. (2015). Adolescent self-control behavior predicts body weight through the life course: A prospective birth cohort study [original article]. International Journal Of Obesity, 40(1), 71–76. https://doi.org/10.1038/ijo.2015.213
- Lakes, K. D., & Hoyt, W. T. (2004). Promoting self-regulation through school-based martial arts training. Journal of Applied Developmental Psychology, 25(3), 283–302. https://doi.org/10.1016/j.appdev.2004.04.002
- Li, J. J., Chung, T. A., Vanyukov, M. M., Scott Wood, D., Ferrell, R., & Clark, D. B. (2015). A hierarchical factor model of executive functions in adolescents: Evidence of gene-environment interplay. Journal of the International Neuropsychological Society, 21(1), 62–73. https://doi.org/10.1017/s1355617714001039
- Longhofer, J., & Floersch, J. (1993). African drumming and psychiatric rehabilitation [empirical study]. Psychosocial Rehabilitation Journal, 16(4), 3–10. https://doi.org/10.1037/h0095656
- Ma, D. S., Correll, J., & Wittenbrink, B. (2015, December). The Chicago face database: A free stimulus set of faces and norming data. Behav Res Methods, 47(4), 1122–1135. https://doi.org/10.3758/s13428-014-0532-5
- Mackinlay, E. (2014). An ABC of drumming: Children’s narratives about beat, rhythm and groove in a primary classroom [empirical study; qualitative study]. British Journal of Music Education, 31(2), 209–230. https://doi.org/10.1017/S0265051714000114
- Maticka-Tyndale, E., & Barnett, J. P. (2010). Peer-led interventions to reduce HIV risk of youth: A review. Evaluation and Program Planning, 33(2), 98–112. https://doi.org/10.1016/j.evalprogplan.2009.07.001
- Mburu, G., Ram, M., Oxenham, D., Haamujompa, C., Iorpenda, K., & Ferguson, L. (2014). Responding to adolescents living with HIV in Zambia: A social–ecological approach. Children and Youth Services Review, 45, 9–17. https://doi.org/10.1016/j.childyouth.2014.03.033
- Mellins, C. A., Elkington, K. S., Bauermeister, J. A., Brackis-Cott, E., Dolezal, C., McKay, M., Wiznia, A., Bamji, M., & Abrams, E. J. (2009). Sexual and drug use behavior in perinatally HIV-infected youth: Mental health and family influences. Journal of the American Academy of Child and Adolescent Psychiatry, 48(8), 810–819. https://doi.org/10.1097/CHI.0b013e3181a81346
- Mellins, C. A., & Malee, K. M. (2013). Understanding the mental health of youth living with perinatal HIV infection: Lessons learned and current challenges [mental health, psychiatric disorders, emotional and behavioral problems, perinatal HIV infection, adolescence, pediatric HIV]. Journal of the International AIDS Society, 16(1), 18593. http://www.jiasociety.org/index.php/jias/article/view/18593.
- Metzler-Baddeley, C., Cantera, J., Coulthard, E., Rosser, A., Jones, D. K., & Baddeley, R. J. (2014). Improved executive function and callosal white matter microstructure after rhythm exercise in huntington’s disease. Journal of Huntington's Disease, 3(3), 273–283. https://doi.org/10.3233/jhd-140113
- Miller, M., Nevado-Montenegro, A. J., & Hinshaw, S. P. (2012). Childhood executive function continues to predict outcomes in young adult females with and without childhood-diagnosed ADHD. Journal of Abnormal Child Psychology, 40(5), 657–668. https://doi.org/10.1007/s10802-011-9599-y
- Miyake, A., & Friedman, N. P. (2012). The nature and organization of individual differences in executive functions: Four general conclusions. Current Directions in Psychological Science, 21(1), 8–14. https://doi.org/10.1177/0963721411429458
- Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognitive Psychology, 41(1), 49–100. https://doi.org/10.1006/cogp.1999.0734
- Moffitt, T. E., Arseneault, L., Belsky, D., Dickson, N., Hancox, R. J., Harrington, H., Houts, R., Poulton, R., Roberts, B. W., Ross, S., Sears, M. R., Thomson, W. M., & Caspi, A. (2011). A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the National Academy of Sciences, 108(7), 2693–2698. https://doi.org/10.1073/pnas.1010076108
- Moreno, S., Bialystok, E., Barac, R., Schellenberg, E., Cepeda, N. J., & Chau, T. (2011). Short-term music training enhances verbal intelligence and executive function. Psychological Science, 22(11), 1425–1433. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc8&AN=2011-26192-013
- Murphy, D. A., Durako, S. J., Moscicki, A. B., Vermund, S. H., Ma, Y., Schwarz, D. F., & Muenz, L. R. (2001). No change in health risk behaviors over time among HIV infected adolescents in care: Role of psychological distress. The Journal of Adolescent Health, 29(3 Suppl), 57–63. https://www.jahonline.org/article/S1054-139X(01)00287-7/fulltext
- Murphy, D. A., Wilson, C. M., Durako, S. J., Muenz, L. R., & Belzer, M. (2001). Antiretroviral medication adherence among the REACH HIV-infected adolescent cohort in the USA. AIDS Care, 13(1), 27–40. https://doi.org/10.1080/09540120020018161
- Nabunya, P., & Ssewamala, F. M. (2014). The effects of parental loss on the psychosocial wellbeing of AIDS-orphaned children living in AIDS-impacted communities: Does gender matter? Children and Youth Services Review, 43, 131–137. https://doi.org/10.1016/j.childyouth.2014.05.011
- Newman, G. F., Maggott, C., & Alexander, D. G. (2015). Group drumming as a burnout prevention initiative among staff members at a child and adolescent mental health care facility [empirical study; longitudinal study; retrospective study; qualitative study]. South African Journal of Psychology, 45(4), 439–451. https://doi.org/10.1177/0081246315581346
- Nichols, S. L., Bethel, J., Garvie, P. A., Patton, D. E., Thornton, S., Kapogiannis, B. G., Ren, W., Major-Wilson, H., Puga, A., & Woods, S. P. (2013). Neurocognitive functioning in antiretroviral therapy-naive youth with behaviorally acquired human immunodeficiency virus. Journal of Adolescent Health, 53(6), 763–771. https://doi.org/10.1016/j.jadohealth.2013.07.006
- Noble, K. G., Korgaonkar, M. S., Grieve, S. M., & Brickman, A. M. (2013). Higher education is an age-independent predictor of white matter integrity and cognitive control in late adolescence. Developmental Science, 16(5), 653–664. https://doi.org/10.1111/desc.12077
- O'Leary, M. J., & Barber, P. J. (1993). Interference effects in the Stroop and Simon paradigms. Journal of Experimental Psychology: Human Perception and Performance, 19(4), 830–844. https://doi.org/10.1037/0096-1523.19.4.830
- Phillips, N., Amos, T., Kuo, C., Hoare, J., Ipser, J., Thomas, K. G. F., & Stein, D. J. (2016). HIV-Associated Cognitive impairment in perinatally infected children: A meta-analysis. Pediatrics, 138(5), e20160893. https://doi.org/10.1542/peds.2016-0893
- Poon, K. (2017). Hot and cool executive functions in adolescence: Development and contributions to important developmental outcomes. Frontiers in Psychology, 8, 2311–2311. https://doi.org/10.3389/fpsyg.2017.02311
- Portowitz, A., Peppler, K. A., & Downton, M. (2014). In harmony: A technology-based music education model to enhance musical understanding and general learning skills. International Journal of Music Education, 32(2), 242–260. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc11&AN=2014-16064-009
- Pozuelo, J. R., Desborough, L., Stein, A., & Cipriani, A. (2021). Systematic review and meta-analysis: Depressive symptoms and risky behaviors Among adolescents in Low- and middle-income countries. Journal of the American Academy of Child and Adolescent Psychiatry, 61(2), 255–276. https://doi.org/10.1016/j.jaac.2021.05.005
- Ramaiya, M. K., Sullivan, K. A., O’ Donnell, K., Cunningham, C. K., Shayo, A. M., Mmbaga, B. T., & Dow, D. E. (2016). A qualitative exploration of the mental health and psychosocial contexts of HIV-positive adolescents in Tanzania. PLoS One, 11(11), e0165936. https://doi.org/10.1371/journal.pone.0165936
- Rowe, K., Buivydaite, R., Heinsohn, T., Rahimzadeh, M., Wagner, R. G., Scerif, G., & Stein, A. (2021). Executive function in HIV-affected children and adolescents: A systematic review and meta-analyses. AIDS Care, 33(7), 833–857. https://doi.org/10.1080/09540121.2021.1873232
- Rowe, K., Duta, M., Demeyere, N., Wagner, R. G., Pettifor, A., Kahn, K., Tollman, S., Scerif, G., & Stein, A. (2021). Validation of Oxford cognitive screen: Executive function (OCS-EF), a tablet-based executive function assessment tool amongst adolescent females in rural South Africa. International Journal of Psychology, 56(6), 895–907. https://doi.org/10.1002/ijop.12764
- Rowe, K., Nkosi, A. D., Dos Santos, A., Kahn, K., Tollman, S., Wagner, R. G., Scerif, G., & Stein, A. (2023). The development of a group drumming intervention aiming to improve executive function and socio-emotional wellbeing in adolescents with HIV in rural South Africa (under review).
- Rubin, L. H., & Maki, P. M. (2019). HIV, depression, and cognitive impairment in the Era of effective antiretroviral therapy [article]. Current HIV/AIDS Reports, 16(1), 82–95. https://doi.org/10.1007/s11904-019-00421-0
- Sartorius, K., Sartorius, B. K., Collinson, M. A., & Tollman, S. M. (2014). The dynamics of household dissolution and change in socio-economic position: A survival model in a rural South Africa. Development Southern Africa, 31(6), 775–795. https://doi.org/10.1080/0376835X.2014.951991
- Saylor, D., Dickens, A. M., Sacktor, N., Haughey, N., Slusher, B., Pletnikov, M., Mankowski, J. L., Brown, A., Volsky, D. J., & McArthur, J. C. (2016). HIV-associated neurocognitive disorder — Pathogenesis and prospects for treatment [review article]. Nature Reviews Neurology, 12(4), 234. https://doi.org/10.1038/nrneurol.2016.27
- Schlam, T. R., Wilson, N. L., Shoda, Y., Mischel, W., & Ayduk, O. (2013). Preschoolers’ delay of gratification predicts their body mass 30 years later. The Journal of Pediatrics, 162(1), 90–93. https://doi.org/10.1016/j.jpeds.2012.06.049
- Semkovska, M., Quinlivan, L., O'Grady, T., Johnson, R., Collins, A., O'Connor, J., Knittle, H., Ahern, E., & Gload, T. (2019). Cognitive function following a major depressive episode: A systematic review and meta-analysis. The Lancet Psychiatry, 6(10), 851–861. https://doi.org/10.1016/S2215-0366(19)30291-3
- Silverman, M. J., & Marcionetti, M. J. (2004). Immediate effects of a single music therapy intervention with persons who are severely mentally ill. The Arts in Psychotherapy, 31(5), 291–301. https://doi.org/10.1016/j.aip.2004.06.008
- Simon, J. R., & Rudell, A. P. (1967). Auditory S-R compatibility: The effect of an irrelevant cue on information processing. Journal of Applied Psychology, 51(3), 300–304. https://doi.org/10.1037/h0020586
- Slater, J., Ashley, R., Tierney, A., & Kraus, N. (2018). Got rhythm? Better inhibitory control Is linked with more consistent drumming and enhanced neural tracking of the musical beat in adult percussionists and nonpercussionists. Journal of Cognitive Neuroscience, 30(1), 14–24. https://doi.org/10.1162/jocn_a_01189
- Slater, J., Azem, A., Nicol, T., Swedenborg, B., & Kraus, N. (2017). Variations on the theme of musical expertise: Cognitive and sensory processing in percussionists, vocalists and non-musicians. European Journal of Neuroscience, 45(7), 952–963. https://doi.org/10.1111/ejn.13535
- Smalley, S. L., Kitil, M. J., Galla, B. M., Kaiser-Greenland, S., Locke, J., Ishijima, E., & Kasari, C. (2010). Effects of mindful awareness practices on executive functions in elementary school children AU - flook, lisa. Journal of Applied School Psychology, 26(1), 70–95. https://doi.org/10.1080/15377900903379125
- Smith, C., Viljoen, J. T., & McGeachie, L. (2014). African drumming: A holistic approach to reducing stress and improving health? Journal of Cardiovascular Medicine, 15(6), 441–446. https://doi.org/10.2459/jcm.0000000000000046
- Snow, S., & D'Amico, M. (2010). The drum circle project: A qualitative study with at-risk youth in a school setting [empirical study; qualitative study]. Canadian Journal of Music Therapy, 16(1), 12–39. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=psyc7&AN=2012-07278-002
- Stone, N. N. (2005). Hand-drumming to build community: The story of the whittier drum project. New Directions for Youth Development, 2005(106), 73–83, 76. https://doi.org/10.1002/yd.120.
- Tavakol, M., & Dennick, R. (2011). Making sense of cronbach’s alpha. International Journal of Medical Education, 2, 53–55. https://doi.org/10.5116/ijme.4dfb.8dfd
- Thorell, L. B., Lindqvist, S., Bergman Nutley, S., Bohlin, G., & Klingberg, T. (2009). Training and transfer effects of executive functions in preschool children. Developmental Science, 12(1), 106–113. https://doi.org/10.1111/j.1467-7687.2008.00745.x
- van der Westhuizen, C., Wyatt, G., Williams, J. K., Stein, D. J., & Sorsdahl, K. (2016). Validation of the self reporting questionnaire 20-item (SRQ-20) for Use in a Low- and middle-income country emergency centre setting. International Journal of Mental Health and Addiction, 14(1), 37–48. https://doi.org/10.1007/s11469-015-9566-x
- Venkit, V. R., Godse, A. A., & Godse, A. S. (2013). Exploring the potentials of group drumming as a group therapy for young female commercial sex workers in mumbai, India. Arts & Health: An International Journal of Research, Policy and Practice, 5(2), 132–141. https://doi.org/10.1080/17533015.2012.698629
- Vreeman, R. C., McCoy, B. M., & Lee, S. (2017). Mental health challenges among adolescents living with HIV. Journal of the International AIDS Society, 20(Suppl 3), 21497–21497. https://doi.org/10.7448/IAS.20.4.21497
- Watson, J., Washington, G., & Stepteau-Watson, D. (2015). Umoja: A culturally specific approach to mentoring young African American males. Child & Adolescent Social Work Journal, 32(1), 1–10. https://doi.org/10.1007/s10560-014-0367-z
- Webb, L., Perry-Parrish, C., Ellen, J., & Sibinga, E. (2017). Mindfulness instruction for HIV-infected youth: A randomized controlled trial. AIDS Care, 30(6), 688–695. https://doi.org/10.1080/09540121.2017.1394434
- Winkelman, M. (2003). Complementary therapy for addiction: “drumming out drugs”. American Journal of Public Health, 93(4), 647–651. https://doi.org/10.2105/ajph.93.4.647
- Wood, L., Ivery, P., Donovan, R., & Lambin, E. (2013). “To the beat of a different drum”: improving the social and mental wellbeing of at-risk young people through drumming. Journal of Public Mental Health, 12(2), 70–79. https://doi.org/10.1108/JPMH-09-2012-0002
- Yuhi, T., Kyuta, H., Mori, H. A., Murakami, C., Furuhara, K., Okuno, M., Takahashi, M., Fuji, D., & Higashida, H. (2017). Salivary oxytocin concentration changes during a group drumming intervention for maltreated school children. Brain Sciences, 7(11), 152. https://doi.org/10.3390/brainsci7110152
- Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. https://doi.org/10.1207/s15327752jpa5201_2
Appendices
Appendix 1 – Cognitive tasks.
AHEAD RACER cognitive task descriptions
RACER (Rapid Assessment of Cognitive and Emotional Regulation) is a touch-screen tablet-based application which was developed by Margaret Sheridan and Amar Hamoudi to assess cognitive function, including executive function (EF), in the field in large samples of children in LMICs. It is designed to be easy to administer by trained lay people or fieldworkers and suitable for use in children with low literacy levels. The tasks use simple shapes and do not rely on content knowledge. The two EF tasks are both quick to administer (1–4 min). They are administered with the tablet in landscape orientation with the examiner seated next to the participant so that the stimuli and on-screen instructions are upright for both the examiner and the participant. Input is with the dominant hand’s index or middle finger for both the examiner and the participant. The examiner has a separate set of standardised written instructions, translated into the local language, Tsonga in the AHEAD Study, to ensure that administration is standardised. Each task has practice rounds built in during which task comprehension can be assured prior to the “test” itself. They include baseline trials with minimal or no EF demands and more challenging EF trials. The outcome measure for each is task is the comparison between performance on the EF trials and baseline trials.
Task 1: Dot location recall
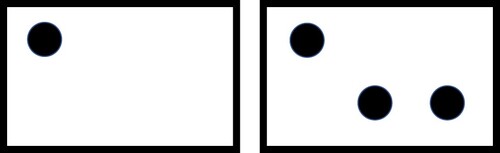
This visuospatial working memory task has 52 trials. In each trial, participants are shown one, two or three stimuli (black dots on the screen). Each dot appears in one of nine locations on an invisible 3 x 3 grid. The stimuli appear on the screen for 2000 milliseconds during which time participants should memorise their locations. After this period, the screen goes blank for 100 milliseconds (short-delay trials) or 3000 milliseconds (long-delay trials). There were 26 short-delay trials and 26 long-delay (working memory) trials. After the delay, participants are asked to touch the screen exactly where they remember the dots to have appeared. Trials with only one dot are low-load trials whereas trials with two or three dots are high-load trials because they contain a greater amount of spatial information to memorise. Long-delay trials also place greater demands on the working memory than short-delay trials because the mental rehearsal needs to occur for a longer period of time. See Figure A1 for an example of the configuration of stimuli on the screen. Response accuracy is measured as the Euclidean distance (in pixels) from the recorded touch location to the centre of nearest stimulus. These distances are recorded automatically by the tablet. The final working memory outcome variable is the difference between the mean accuracy on low-load short-delay trials and the mean accuracy on high-load long-delay trials: working memory score = [mean distance from target on low-load short-delay trials] – [mean distance from target on high-load long-delay trials]. The degree to which a longer delay impairs performance is taken to be an estimate of working memory. A higher score indicates better working memory performance.
Figure A1. AHEAD Study RACER dot recall spatial working memory task: examples of stimulus configurations in low-load (left) and high-load (right) trials.
Task 2: Simon task
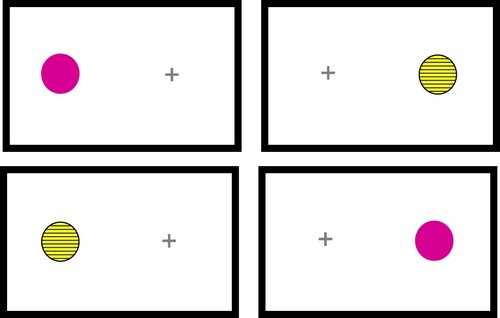
The Simon task is a measure of cool or non-affective inhibitory control based on the Simon or stimulus-response compatibility effect. This effect describes the phenomenon of higher accuracy and lower response times when there is congruence between stimuli and the expected response, and decreased accuracy and slower reaction times when there is incongruence or a mismatch between features of the stimulus and the required response (e.g., Response required on the opposite side to the stimulus) (O'Leary & Barber, Citation1993; Simon & Rudell, Citation1967). In this version of the task, there were 60 same-side (congruent) trials and 60 opposite-side (incongruent) trials. Stimuli with different colours and patterns appear one at a time on either the left or right side of the screen. For same-side trials, participants are instructed to touch the centre of the dot (i.e., the same side) as quickly as possible. For opposite-side trials, participants are instructed to touch the centre of the opposite side of the screen, which is marked with a small cross sign, as quickly as possible. This incongruence between the side of the stimulus and the side of the response requires inhibition of the prepotent tendency to touch the same side as the stimulus and thus assesses inhibitory control. See Figure A2 for the on-screen appearance of different trial types. Reaction times on each trial is recorded automatically by the tablet. The final inhibitory control outcome variable is the difference between the mean reaction time on same-side (congruent) trials and opposite-side (incongruent) trials: inhibitory control score = [mean congruent trial reaction time] – [mean incongruent trial reaction time]. The degree to which the requirement of inhibition slows performance is taken as an estimate of the individual’s inhibitory control performance. A higher score indicates better inhibitory control performance.
Figure A2. AHEAD Study RACER Simon inhibitory control task: examples of same-side trials with purple-pink dot stimuli and opposite-side trials with striped yellow-and-black dot stimuli.