
ABSTRACT
Internalized stigma is common among individuals with sexually transmitted infections such as HIV and among those with mental health conditions such as major depressive disorder (MDD). As part of a cluster randomized trial, we investigated the prevalence and correlates of internalized stigma among adults living with comorbid HIV and MDD in rural Malawi (n = 339). We found heightened stigma toward HIV and mental illness among those in the cohort: more than half of respondents (54%) endorsed negative perceptions associated with each health condition. Internalized HIV-related stigma was higher among those with no education (p = 0.04), younger adults (p = 0.03), and those with less social support (p = 0.001). Mental illness-related stigma was elevated among those with no source of income (p = 0.001), and it was also strongly associated with HIV-related stigma (p < 0.001). Our findings highlight potential avenues for reducing internalized stigma associated with high-prevalence health conditions in Malawi.
Trial registration: ClinicalTrials.gov identifier: NCT04777006.
Introduction
Stigma – defined as a lack of respect or negative opinion of persons because of their affiliation with something society disapproves (Goffman, Citation1963) – is common across cultures for two major categories of health conditions: sexually transmitted infections and mental illnesses. Among those with sexually transmitted infections such as HIV, negative perceptions commonly relate to stereotypes of promiscuity, lack of cleanliness, and impurity (Lau & Tsui, Citation2005). For people with mental health conditions like major depressive disorder (MDD), these perceptions may be associated with idleness and lack of motivation, or else have a religious connotation of being cursed or condemned (Pederson et al., Citation2020). These negative perceptions may be magnified in low-resource settings, where individuals have lower levels of education and where there is limited access to health messaging that combats stereotypes (Lo et al., Citation2021; Teshale & Tesema, Citation2022).
HIV and mental illness are also interconnected. HIV diagnosis is associated with social isolation, which can contribute to heightened levels of depression and anxiety (Nanni et al., Citation2015). These negative effects on mental health may be exacerbated in circumstances where intimate partners, family members, and friends learn of an individual’s HIV diagnosis and hold negative perceptions about HIV (Brandt, Citation2009). Depression has, in turn, been associated with lower adherence to antiretroviral therapy (Abas et al., Citation2014) and elevated HIV viral load (Meffert et al., Citation2019). Furthermore, the HIV virus and medications such as antiretroviral therapy can produce neurological changes that further amplify depressive symptoms (Bronshteyn et al., Citation2021; Philippi et al., Citation2020).
This adverse dynamic between having a diagnosis of HIV and elevated depressive symptoms appears most pronounced in the presence of internalized stigma – the process by which individuals cognitively and emotionally absorb negative stereotypes to which they are subjected (Boyd et al., Citation2014a). Prior studies have documented that internalized HIV stigma is associated with depression severity and social isolation (Turan et al., Citation2016), lower antiretroviral therapy adherence (Rice et al., Citation2017), elevated viral load (Christopoulos et al., Citation2020), lower retention in HIV care (Pearson et al., Citation2021), reduced employment seeking behavior (Lightner et al., Citation2021), and elevated suicidal ideation (Hua et al., Citation2014). These trends have also been observed in sub-Saharan African settings (Ashaba et al., Citation2018; Earnshaw et al., Citation2018; Hargreaves et al., Citation2020). Meanwhile, internalized stigma for mental illness is correlated with heightened psychological distress, lower self-esteem and self-efficacy (Drapalski et al., Citation2013; Oexle et al., Citation2018), reducing care seeking behavior, and heightened unemployment (Gomes et al., Citation2021; Kaushik et al., Citation2016). Although there is limited research on internalized stigma for mental illness and sub-Saharan African, available studies have shown similar trends (Bedaso et al., Citation2022; Dubreucq et al., Citation2021; Shumet et al., Citation2021; Sorsdahl et al., Citation2012).
Malawi is a landlocked, low-income country in southeastern sub-Saharan Africa. With a population of roughly 20 million individuals living on an average of $US 635 per annum, the country has a high HIV prevalence (8% as of 2020 (The World Bank, Citation2022)) and a significant treatment gap for mental health conditions (Kauye et al., Citation2014). The estimated lifetime prevalence of MDD is estimated about 18% (Kauye et al., Citation2014; Nakimuli-Mpungu et al., Citation2012), and the estimated treatment gap for MDD in Malawi is greater than 90% (Kauye et al., Citation2014; Udedi, Citation2014). Past research has documented negative stereotypes associated with both HIV (Malawi Network of People Living with HIV, Citation2016) and mental illness (Crabb et al., Citation2012) throughout Malawi, despite these conditions representing a large proportion of the overall burden of disease (Institute for Health Metrics and Evaluation, Citation2015). In this study, we examine internalized stigma pertaining to HIV and mental illness among adults living with comorbid HIV and MDD in Neno District, Malawi – a rural district of Malawi. Specifically, we examined prevalence and correlates of internalized stigma, in terms of demographic and socioeconomic characteristics, as well as perceived social support. We hypothesized that greater levels of internalized stigma across both conditions would be associated with lower levels of education, income, and social support, as well as heightened depression symptom severity.
Methods
Study design and setting
The Integrated Chronic Care Clinics – Depression study represents a randomized controlled trial that is expanding services for non-communicable diseases into Malawi’s HIV platform. Specifically, patients with chronic health conditions – such as HIV, diabetes, and hypertension – are enrolled in integrated chronic care clinics throughout all 14 health facilities in Neno District that routinely serve patients with HIV (Wroe et al., Citation2020). Integrated chronic care clinics serve approximately 13,000 patients and are supported by the Ministry of Health and Partners In Health, a local not-for-profit healthcare delivery organization. The trial incorporates depression screening and treatment into this model. The data presented in this study were gathered using the measures detailed below, collected at the point of enrollment prior to any depression care. Participants in the trial were enrolled between September 2021 and April 2022. Further details about the trial can be found elsewhere (McBain et al., Citation2021).
Study participants
Individuals were eligible for trial participation if they were: (1) an active care recipient at integrated chronic care clinics, (2) a resident of Neno District, (3) ≥ 18 years old, and (4) received a diagnosis of moderate or severe depression, based on the Patient Health Questionnaire-9. Individuals identified with active psychosis or at imminent risk of harm to themselves (or others) were excluded from trial participation and referred to specialized services for immediate care. For the purposes of this manuscript, we restricted our sample to those with a comorbid diagnosis of HIV, representing the preponderance of enrollees: 339 of 487 individuals (70%).
Measures
Measures included surveys, laboratory assays, pharmacy information, and clinical information abstracted from client electronic medical records. These are described below.
Depression Prevalence and Severity. Depression symptoms were measured with the Patient Health Questionnaire (both Patient Health Questionnaire-2 and Patient Health Questionnaire-9) (Kroenke et al., Citation2001), previously translated into Chichewa (the local language) and validated in Malawi (Udedi et al., Citation2019). A Patient Health Questionnaire-9 score of 10–14 indicates moderate depression, while a score of 15 or greater indicates severe depression.
Daily Functioning. We assessed individual impairments in daily functioning using the 12-item WHO Disability Assessment Schedule 2.0 (World Health Organization, Citation2012), which has been validated in various sub-Saharan African contexts, including Malawi (Cresswell et al., Citation2020) and covers topics like completing household chores, concentration, and maintaining relationships. Respondents answered questions about their general level of impairment, rather than specific to HIV or depression.
Perceived Social Support. Social support was assessed by the Multidimensional Scale of Perceived Social Support (Zimet et al., Citation1988), previously validated in Malawi (Stewart et al., Citation2014). The survey comprises 12 items on a seven-point ordinal scale from “very strongly disagree” to “very strongly agree” and includes different types of support available from family and friends, such as emotional help, talking about problems, and sharing in joys and sorrows.
Demographic Characteristics. Participants were asked to provide basic demographic information, including their gender, age, marital status, level of education, and employment status. Based on the low levels of education and employment observed within the sample, we dichotomized these measures: any formal education (yes/no), and any current source of employment (yes/no).
Internalized Stigma: HIV. To measure HIV internalized stigma, we employed the AIDS-Related Stigma Scale, which has been specifically designed to quantify HIV-related stigma in community-based settings in sub-Saharan Africa (Kalichman et al., Citation2005). This constitutes a six-item survey of yes/no responses on topics such as feelings of guilt, shame, and uncleanliness associated with HIV diagnosis (Kalichman et al., Citation2005).
Internalized Stigma: Mental Illness. To measure internalized stigma for mental illness, we employed the Internalizing Stigma of Mental Illness Scale (Boyd et al., Citation2014b), which has also been employed in community-based settings throughout sub-Saharan Africa (Assefa et al., Citation2012; Brooke-Sumner et al., Citation2018). The scale examines perceptions such as “mentally-ill people tend to be violent”, and “mental illness might make me look or behave weird”.
Statistical analyses
Descriptive statistics were generated to characterize the sample and the two dependent variables of interest: prevalence of internalized stigma associated with HIV, and prevalence of internalized stigma associated with mental illness. This included means and standard deviations for continuous variables and frequencies and percentages for discreet variables.
Following this, we conducted multivariable linear regression analysis, incorporating the independent variables as described above to examine their relationships with mental illness-related stigma. We also conducted multivariable ordered logistic regression analysis to examine the relationship between independent variables and HIV-related stigma. We elected to include these independent variables based on prior literature indicating demographic characteristics (Loutfy et al., Citation2012; Tsai, Citation2015), depression severity (Turan et al., Citation2016), perceived social support (Takada et al., Citation2014; Turan et al., Citation2016), and daily functioning (Habtamu et al., Citation2018) are predictive of internalized stigma in other settings. For the linear regression model, we documented an F-test for overall significance and the associated R-squared value. For the ordered logistic regression model, we reported McFadden’s Pseudo R-squared value. All analyses were conducted in Stata 17.0, with a two-sided alpha threshold of α = 0.05 specified.
To examine normality of residuals from the linear regression, we conducted the skewness and kurtosis test for normality (sktest). We did not find evidence the normality assumption was violated (p > 0.05). To test multicollinearity, we also examined the variance inflation factor of independent variables. No variance inflation factor was above 1.35 for any variable. Typically, a variance inflation factor below 5 is deemed acceptable.
Ethical approval
The trial protocol can be found on ClinicalTrials.gov (NCT04777006). The study received ethics approval from the RAND Human Subjects Protection Committee as well as the National Health Science Research Committee of Malawi (20/11/2626). We obtained either written or verbal informed consent from all participants in the study. The funder had no role in study design, implementation of activities, data analysis and interpretation, writing, or the decision to submit the paper.
Results
Sample characteristics
Participant demographics are shown in . While 64% of individuals reported having a source of income, average weekly income was low: $US 12 per week. The mean Patient Health Questionnaire-9 score was 13.1 (SD: 2.8) and median value was 12. Internalized stigma associated with HIV had the mean score of 3.4 (SD: 2.3) and median of 4. The mean score on the internalized stigma associated with mental illness scale was 24.3 (SD: 4.9), and the median value was 24. Levels of internalized stigma were high (see next section for details), and patients indicated moderate levels of disability and social support as indexed by the WHO Disability Assessment Schedule 2.0 and Multidimensional Scale of Perceived Social Support, respectively.
Table 1. Descriptive characteristics of the sample.
Prevalence of internalized stigma
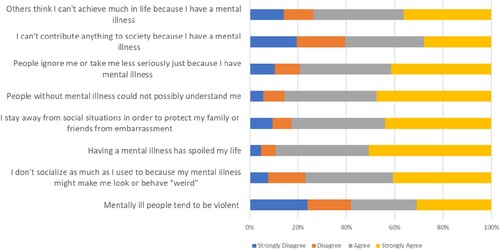
More than half of the respondents endorsed each of the six items on HIV-related stigma (see ). The most frequently endorsed items were: “I sometimes feel worthless because I am HIV positive” (yes: 61%) and “I feel guilty that I am HIV positive” (yes: 59%). Likewise, most respondents stated that they “agreed” or “strongly agreed” with all eight statements on mental illness stigma (see ). For six of eight items, “strongly agreed” was the most frequently endorsed response category. Across items, respondents most frequently agreed with the statements: “Having a mental illness has spoiled my life” (agreed: 89%) and “people without mental illness could not possibly understand me” (agreed: 85%).
Figure 1. Prevalence of Internalized Stigma for HIV.
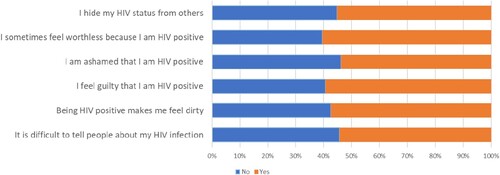
Figure 2. Prevalence of Internalized Stigma for Mental Illness.
Correlates of internalized stigma
Based on multivariable regression analysis, higher levels of internalized HIV-related stigma were associated with having no formal education (OR = 0.51; SE = 0.16; p = 0.04, 95% CI: 0.27, 0.95) and being younger (OR = 0.98; SE = 0.01; p = 0.03; 95% CI: 0.96, 1.00). In addition, we found that lower levels of perceived social support corresponded to higher levels of HIV-related stigma (OR = 0.98; SE = 0.01; p = 0.00; 95% CI: 0.97, 0.99) (see ). No other differences were statistically significant (p > 0.05). The pseudo-R-squared value for this model was 0.04.
Table 2. Correlates of internalized stigma.
Regarding internalized stigma for mental illness, higher levels were associated with having no source of income (β = −2.23; SE = 0.55; p < 0.01, 95% CI: −3.31, −1.15) (see ). Furthermore, we found that mental illness-related stigma was positively associated with HIV-related stigma (β = 0.48; SE = 0.11; p = 0.00, 95% CI: 0.25, 0.70). The F-test statistic for the model was 4.67 (p < 0.001) and R-squared value was 0.12.
Discussion
This study examined the prevalence and correlates of internalized stigma for HIV and mental illness. To our knowledge, this is the first study to explore internalized stigma among adults with a dual diagnosis living in a low-resource setting like rural Malawi. We observed high rates of internalized stigma for HIV, with more than half of respondents reporting they felt ashamed and guilty because of their HIV infection. These levels are roughly equivalent to those observed in other African settings, such as Morocco, Cameroon and South Africa (dos Santos et al., Citation2014; Jacobi et al., Citation2013; Moussa et al., Citation2021). We also observed high rates of internalized stigma of mental illness, with 89% of the respondents agreeing that “mental illness has spoiled my life” and 85% agreeing that “people without mental illness could not possibly understand me”. These rates are higher than those found in settings such as Ethiopia or Malaysia (Alemayehu et al., Citation2020; Woon et al., Citation2020) but roughly comparable to findings in settings such as China (Ran et al., Citation2018a).
Internalized stigma for HIV was associated with lack of formal education. Previous studies have found that education may have a countervailing effect on HIV-related stigma (Loutfy et al., Citation2012; Moradzadeh & Zamanian, Citation2021; Sayles et al., Citation2008), indicating that education boosts individuals’ self-esteem and dispels myths and serotypes. Direct educational campaigns targeting HIV stigma reduction have yielded benefits in reducing negative attitudes and beliefs (Mak et al., Citation2017) – offering a potential avenue that could be considered in Malawian settings like Neno District.
Consistent with other studies, stigma was lower among older adults (Armoon et al., Citation2021; Li et al., Citation2018). One explanation for this is that older age is typically associated with more social and family support, which corresponds with less stigma. Other studies have argued that overall internalization of stigmatizing attitudes may lessen with age as maturation provides resilience against stigma (Emlet et al., Citation2015; Peltzer & Pengpid, Citation2019). It has also been argued that older people develop ways to manage their lives with HIV, and this in turn reduces negative perceptions about their condition (Peltzer & Pengpid, Citation2019; Subedi et al., Citation2019).
High levels of internalized HIV-related stigma were associated with low social support, corroborating studies with similar findings in Uganda (Takada et al., Citation2014) and South Africa (Simbayi et al., Citation2007), as well as in Kenya among pregnant women living with HIV (Yator et al., Citation2021). Here, evidence suggests that social support – particularly emotional support from friends and family – tends to counter negative thoughts and perceptions that individuals hold (Takada et al., Citation2014) and may explain the relationship between HIV, depression and self-perceived quality of life (Rao et al., Citation2012). In countries ranging from Kenya to India, social group interventions have promoted adherence to antiretroviral therapy by focusing on emotional support, among other areas (Ma et al., Citation2019).
Internalized stigma of mental illness was associated with a lack of income. Previous studies have found low levels of income to be associated with internalized stigma (Ran et al., Citation2018b; Tesfaye et al., Citation2020; Werner et al., Citation2009) – including poor self-esteem that may be exacerbated by individuals’ inability to make financial contributions to their household. The converse might also hold: that income and motivation to work could also influenced by one’s self-efficacy and internalized mental health stigma (Mills et al., Citation2020; Sardá Jr et al., Citation2009). Interventions that seek to address depression symptoms while also helping capacitate individuals for employment opportunities could, theoretically, address both issues at once (Tandon et al., Citation2015). This framing could be particularly relevant in low-resource settings like Neno District, where employment rates are low and rates of untreated mental health conditions are high (Bukenya et al., Citation2022).
Lastly, we found that internalized stigma associated with mental illness and HIV were strongly correlated. We expect there are two underlying reasons for this. First, low levels of education among those with MDD and HIV may jointly contribute to facile interpretations of disease epidemiology, including those grounded in stereotypes. Second, exposure to cultural beliefs held by family and friends is likely to be consistent across health conditions: i.e., Families and communities who hold negative cultural beliefs about HIV may be more likely to hold negative cultural beliefs about MDD. Similar findings have been observed in other settings (Crabb et al., Citation2012; Pederson et al., Citation2020; Saliu & Akintunde, Citation2014; Sano et al., Citation2016). This raises the possibility that addressing mechanisms that underpin internalized stigma more generally – such as education, functional capacity and/or social support – could yield benefits for both sets of conditions. The depression treatment intervention associated with this study focuses on strengthening social support to improve health and social wellbeing. Upon conclusion of the trial, we intend to evaluate whether changes in social support mediate effects of depression treatment on internalized stigma.
This study contains four main limitations. First, measures of stigma and depression were self-reported. The extent to which participants felt comfortable sharing their perceptions of stigma could be influenced by social desirability bias on the part of patients or observer expectancy effects on the part of interviewers. Second, we are unable to determine whether the measures employed in the study captured internalized HIV stigma and mental illness stigma as two separate constructs, or as one underlying construct. Third, the study population was predominantly female, limiting generalizability of findings. Lastly, our examination is correlational and cannot comment on whether our observed relationships are causative in one direction or influenced by unmeasured confounders. However, the patterns we observed are consistent with prior literature and offer potential avenues for intervention.
Conclusion
Overall, this study indicates the high prevalence of internalized stigma among those with HIV and MDD in rural Malawi. Furthermore, the pattern of associations we observed underscores the importance of social support, education, and income-generating activities when considering ways to address internalized stigma within this population. Subsequent research in the Malawian context might explore the intersectionality of stigma for multiple health conditions, as well as pilot interventions that address modifiable factors that could alleviate stigma as documented in this study.
Ethics approval
The study has received ethics approval from the RAND Human Subjects Protection Committee as well as the National Health Science Research Committee of Malawi (20/11/2626).
Consent for participation and publication
We obtained either written informed consent from all participants to participate in the study. Patients signed informed consent regarding publishing their data.
Code availability statement
Code available upon request.
Author contributions
Kondwani Mpinga, Owen Mwale, and Ryan McBain contributed to study conception and design. Data collection was performed by Kondwani Mpinga, Owen Mwale, Myrrah Kamwiyo, and Waste Kayira. Data preparation and analysis were performed by Ryan McBain, Kondwani Mpinga, and Sarita D. Lee. The first draft of the manuscript was written by Ryan McBain, Kondwani Mpinga, and Sarita D. Lee. All authors commented on versions of the manuscripts. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to extend appreciation to study participants and clinic staff for their assistance in collecting the data. Without them, none of this research would be possible.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Deidentified data available upon request (email: [email protected]).
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Abas, M., Ali, G.-C., Nakimuli-Mpungu, E., & Chibanda, D. (2014). Depression in people living with HIV in sub-Saharan Africa: Time to act. Tropical Medicine & International Health, 19(12), 1392–1396. https://doi.org/10.1111/tmi.12382
- Alemayehu, Y., Demilew, D., Asfaw, G., Asfaw, H., Alemnew, N., & Tadesse, A. (2020). Internalized stigma and associated factors among patients with major depressive disorder at the outpatient department of amanuel mental specialized hospital, Addis Ababa, Ethiopia, 2019: A cross-sectional study. Psychiatry Journal, 2020, e7369542. https://doi.org/10.1155/2020/7369542
- Armoon, B., Higgs, P., Fleury, M.-J., Bayat, A.-H., Moghaddam, L. F., Bayani, A., & Fakhri, Y. (2021). Socio-demographic, clinical and service use determinants associated with HIV related stigma among people living with HIV/AIDS: A systematic review and meta-analysis. BMC Health Services Research, 21(1), 1004. https://doi.org/10.1186/s12913-021-06980-6
- Ashaba, S., Cooper-Vince, C., Maling, S., Rukundo, G. Z., Akena, D., & Tsai, A. C. (2018). Internalized HIV stigma, bullying, major depressive disorder, and high-risk suicidality among HIV-positive adolescents in rural Uganda. Global Mental Health (Cambridge, England), 5, e22. https://doi.org/10.1017/gmh.2018.15
- Assefa, D., Shibre, T., Asher, L., & Fekadu, A. (2012). Internalized stigma among patients with schizophrenia in Ethiopia: A cross-sectional facility-based study. BMC Psychiatry, 12(1), 239. https://doi.org/10.1186/1471-244X-12-239
- Bedaso, A., Workie, K., Gobena, M., & Kebede, E. (2022). The magnitude and correlates of internalized stigma among people with mental illness attending the outpatient department of Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia. Heliyon, 8(5), https://doi.org/10.1016/j.heliyon.2022.e09431
- Boyd, J. E., Adler, E. P., Otilingam, P. G., & Peters, T. (2014a). Internalized stigma of mental illness (ISMI) scale: A multinational review. Comprehensive Psychiatry, 55(1), 221–231. https://doi.org/10.1016/j.comppsych.2013.06.005
- Boyd, J. E., Otilingam, P. G., & Deforge, B. R. (2014b). Brief version of the Internalized Stigma of Mental Illness (ISMI) scale: Psychometric properties and relationship to depression, self esteem, recovery orientation, empowerment, and perceived devaluation and discrimination. Psychiatric Rehabilitation Journal, 37(1), 17–23. https://doi.org/10.1037/prj0000035
- Brandt, R. (2009). The mental health of people living with HIV/AIDS in Africa: A systematic review. African Journal of AIDS Research, 8(2), 123–133. https://doi.org/10.2989/AJAR.2009.8.2.1.853
- Bronshteyn, M., Yang, F. N., Shattuck, K. F., Dawson, M., Kumar, P., Moore, D. J., Ellis, R. J., & Jiang, X. (2021). Depression is associated with hippocampal volume loss in adults with HIV. Human Brain Mapping, 42(12), 3750–3759. https://doi.org/10.1002/hbm.25451
- Brooke-Sumner, C., Selohilwe, O., Mazibuko, M. S., & Petersen, I. (2018). Process evaluation of a pilot intervention for psychosocial rehabilitation for service users with schizophrenia in north west province, South Africa. Community Mental Health Journal, 54(7), 1089–1096. https://doi.org/10.1007/s10597-018-0318-9
- Bukenya, B., Kasirye, R., Lunkuse, J., Kinobi, M., Vargas, S. M., Legha, R., Tang, L., & Miranda, J. (2022). Depression, anxiety, and suicide risk among Ugandan youth in vocational training. Psychiatric Quarterly, 93(2), 513–526. https://doi.org/10.1007/s11126-021-09959-y
- Christopoulos, K. A., Neilands, T. B., Dilworth, S., Lisha, N., Sauceda, J., Mugavero, M. J., Crane, H. M., Fredericksen, R. J., Mathews, W. C., Moore, R. D., Mayer, K. H., Napravnik, S., & Johnson, M. O. (2020). Internalized HIV stigma predicts subsequent viremia in US HIV patients through depressive symptoms and antiretroviral therapy adherence. AIDS (London, England), 34(11), 1665–1671. https://doi.org/10.1097/QAD.0000000000002595
- Crabb, J., Stewart, R. C., Kokota, D., Masson, N., Chabunya, S., & Krishnadas, R. (2012). Attitudes towards mental illness in Malawi: A cross-sectional survey. BMC Public Health, 12(1), 541. https://doi.org/10.1186/1471-2458-12-541
- Cresswell, J. A., Barbour, K. D., Chou, D., McCaw-Binns, A., Filippi, V., Cecatti, J. G., Barreix, M., Petzold, M., Kostanjsek, N., Cottler-Casanova, S., & Say, L. (2020). Measurement of maternal functioning during pregnancy and postpartum: Findings from the cross-sectional WHO pilot study in Jamaica, Kenya, and Malawi. BMC Pregnancy and Childbirth, 20(1), 518. https://doi.org/10.1186/s12884-020-03216-z
- dos Santos, M. M., Kruger, P., Mellors, S. E., Wolvaardt, G., & van der Ryst, E. (2014). An exploratory survey measuring stigma and discrimination experienced by people living with HIV/AIDS in South Africa: The People Living with HIV Stigma Index. BMC Public Health, 14(1), 80. https://doi.org/10.1186/1471-2458-14-80
- Drapalski, A. L., Lucksted, A., Perrin, P. B., Aakre, J. M., Brown, C. H., DeForge, B. R., & Boyd, J. E. (2013). A model of internalized stigma and its effects on people with mental illness. Psychiatric Services (Washington, D.C.), 64(3), 264–269. https://doi.org/10.1176/appi.ps.001322012
- Dubreucq, J., Plasse, J., & Franck, N. (2021). Self-stigma in serious mental illness: A systematic review of frequency, correlates, and consequences. Schizophrenia Bulletin, 47(5), 1261–1287. https://doi.org/10.1093/schbul/sbaa181
- Earnshaw, V. A., Bogart, L. M., Laurenceau, J.-P., Chan, B. T., Maughan-Brown, B. G., Dietrich, J. J., Courtney, I., Tshabalala, G., Orrell, C., Gray, G. E., Bangsberg, D. R., & Katz, I. T. (2018). Internalized HIV stigma, ART initiation and HIV-1 RNA suppression in South Africa: Exploring avoidant coping as a longitudinal mediator. Journal of the International AIDS Society, 21(10), e25198. https://doi.org/10.1002/jia2.25198
- Emlet, C. A., Brennan, D. J., Brennenstuhl, S., Rueda, S., Hart, T. A., & Rourke, S. B. (2015). The impact of HIV-related stigma on older and younger adults living with HIV disease: Does age matter? AIDS Care, 27(4), 520–528. https://doi.org/10.1080/09540121.2014.978734
- Goffman, E. (1963). Stigma: Notes on the management of spoiled identity. Simon & Schuster.
- Gomes, D. R. A. S., Zanetti, A. C. G., Miasso, A. I., Castro, F. F. S., & Vedana, K. G. G. (2021). Internalized stigma in people with mood disorders: Predictors and associated factors. Journal of Nervous & Mental Disease, 209(1), 54–58. https://doi.org/10.1097/NMD.0000000000001257
- Habtamu, K., Alem, A., Medhin, G., Fekadu, A., & Hanlon, C. (2018). Functional impairment among people with severe and enduring mental disorder in rural Ethiopia: A cross-sectional study. Social Psychiatry and Psychiatric Epidemiology, 53(8), 803–814. https://doi.org/10.1007/s00127-018-1546-6
- Hargreaves, J. R., Pliakas, T., Hoddinott, G., Mainga, T., Mubekapi-Musadaidzwa, C., Donnell, D., Piwowar-Manning, E., Agyei, Y., Mandla, N. F., Dunbar, R., Macleod, D., Floyd, S., Bock, P., Fidler, S., Hayes, R. J., Seeley, J., Stangl, A., Bond, V., Ayles, H., & HPTN 071 (PopART) Study Team. (2020). Hiv stigma and viral suppression Among people living With HIV in the context of universal test and treat: Analysis of data from the HPTN 071 (PopART) trial in Zambia and South Africa. Journal of Acquired Immune Deficiency Syndromes, 85(5), 561–570. https://doi.org/10.1097/QAI.0000000000002504
- Hua, J., Emrick, C. B., Golin, C. E., Liu, K., Pan, J., Wang, M., Wan, X., Chen, W., & Jiang, N. (2014). Hiv and stigma in liuzhou, China. AIDS and Behavior, 18(2), 203–211. https://doi.org/10.1007/s10461-013-0637-3
- Institute for Health Metrics and Evaluation. (2015, September 9). Malawi. Institute for Health Metrics and Evaluation. https://www.healthdata.org/malawi.
- Jacobi, C. A., Atanga, P. N. J. I., Bin, L. K., Mbome, V. N., Akam, W., Bogner, J. R., Kropf, S., & Malfertheiner, P. (2013). HIV/AIDS-related stigma felt by people living with HIV from Buea, Cameroon. AIDS Care, 25(2), 173–180. https://doi.org/10.1080/09540121.2012.701715
- Kalichman, S. C., Simbayi, L. C., Jooste, S., Toefy, Y., Cain, D., Cherry, C., & Kagee, A. (2005). Development of a brief scale to measure AIDS-related stigma in South Africa. AIDS and Behavior, 9(2), 135–143. https://doi.org/10.1007/s10461-005-3895-x
- Kaushik, A., Kostaki, E., & Kyriakopoulos, M. (2016). The stigma of mental illness in children and adolescents: A systematic review. Psychiatry Research, 243, 469–494. https://doi.org/10.1016/j.psychres.2016.04.042
- Kauye, F., Jenkins, R., & Rahman, A. (2014). Training primary health care workers in mental health and its impact on diagnoses of common mental disorders in primary care of a developing country, Malawi: A cluster-randomized controlled trial. Psychological Medicine, 44(3), 657–666. https://doi.org/10.1017/S0033291713001141
- Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
- Lau, J. T. F., & Tsui, H. Y. (2005). Discriminatory attitudes towards people living with HIV/AIDS and associated factors: A population based study in the Chinese general population. Sexually Transmitted Infections, 81(2), 113–119. https://doi.org/10.1136/sti.2004.011767
- Li, Z., Morano, J. P., Khoshnood, K., Hsieh, E., & Sheng, Y. (2018). HIV-related stigma among people living with HIV/AIDS in rural Central China. BMC Health Services Research, 18(1), 453. https://doi.org/10.1186/s12913-018-3245-0
- Lightner, J. S., Rajabiun, S., Cabral, H. J., Flaherty, J., Shank, J., & Brooks, R. (2021). Associations of internalized and anticipated HIV stigma with returning to work for persons living with HIV. PLoS One, 16(6), e0252783. https://doi.org/10.1371/journal.pone.0252783
- Lo, L. L. H., Suen, Y. N., Chan, S. K. W., Sum, M. Y., Charlton, C., Hui, C. L. M., Lee, E. H. M., Chang, W. C., & Chen, E. Y. H. (2021). Sociodemographic correlates of public stigma about mental illness: A population study on Hong Kong’s Chinese population. BMC Psychiatry, 21(1), 274. https://doi.org/10.1186/s12888-021-03301-3
- Loutfy, M. R., Logie, C. H., Zhang, Y., Blitz, S. L., Margolese, S. L., Tharao, W. E., Rourke, S. B., Rueda, S., & Raboud, J. M. (2012). Gender and ethnicity differences in HIV-related stigma experienced by people living with HIV in Ontario, Canada. PLOS ONE, 7(12), e48168. https://doi.org/10.1371/journal.pone.0048168
- Ma, P. H. X., Chan, Z. C. Y., & Loke, A. Y. (2019). Self-Stigma reduction interventions for people living with HIV/AIDS and their families: A systematic review. AIDS and Behavior, 23(3), 707–741. https://doi.org/10.1007/s10461-018-2304-1
- Mak, W. W. S., Mo, P. K. H., Ma, G. Y. K., & Lam, M. Y. Y. (2017). Meta-analysis and systematic review of studies on the effectiveness of HIV stigma reduction programs. Social Science & Medicine, 188, 30–40. https://doi.org/10.1016/j.socscimed.2017.06.045
- Malawi Network of People Living with HIV. (2016). The people living with HIV stigma index—Malawi report April 2016. Global Network of People Living with HIV. https://www.stigmaindex.org/wp-content/uploads/2022/04/Malawi-SI-report-2016.pdf.
- McBain, R. K., Mwale, O., Ruderman, T., Kayira, W., Connolly, E., Chalamanda, M., Kachimanga, C., Khongo, B. D., Wilson, J., Wroe, E., Raviola, G., Smith, S., Coleman, S., Kelly, K., Houde, A., Tebeka, M. G., Watson, S., Kulisewa, K., Udedi, M., & Wagner, G. (2021). Stepped care for depression at integrated chronic care centers (IC3) in Malawi: Study protocol for a stepped-wedge cluster randomized controlled trial. Trials, 22(1), 630. https://doi.org/10.1186/s13063-021-05601-1
- Meffert, S. M., Neylan, T. C., McCulloch, C. E., Maganga, L., Adamu, Y., Kiweewa, F., Maswai, J., Owuoth, J., Polyak, C. S., Ake, J. A., & Valcour, V. G. (2019). East African HIV care: Depression and HIV outcomes. Global Mental Health (Cambridge, England), 6, e9. https://doi.org/10.1017/gmh.2019.6
- Mills, H., Mulfinger, N., Raeder, S., Rüsch, N., Clements, H., & Scior, K. (2020). Self-help interventions to reduce self-stigma in people with mental health problems: A systematic literature review. Psychiatry Research, 284, 112702. https://doi.org/10.1016/j.psychres.2019.112702
- Moradzadeh, R., & Zamanian, M. (2021). HIV-Related stigma Among people living With HIV in Iran: A cross-sectional study. Journal of the Association of Nurses in AIDS Care, 32(5), 610–618. https://doi.org/10.1097/JNC.0000000000000251
- Moussa, A. B., Delabre, R. M., Villes, V., Elkhammas, M., Bennani, A., Ouarsas, L., Filali, H., Alami, K., Karkouri, M., & Castro, D. R. (2021). Determinants and effects or consequences of internal HIV-related stigma among people living with HIV in Morocco. BMC Public Health, 21(1), 163. https://doi.org/10.1186/s12889-021-10204-1
- Nakimuli-Mpungu, E., Bass, J. K., Alexandre, P., Mills, E. J., Musisi, S., Ram, M., Katabira, E., & Nachega, J. B. (2012). Depression, alcohol use and adherence to antiretroviral therapy in sub-Saharan Africa: A systematic review. AIDS and Behavior, 16(8), 2101–2118. https://doi.org/10.1007/s10461-011-0087-8
- Nanni, M. G., Caruso, R., Mitchell, A. J., Meggiolaro, E., & Grassi, L. (2015). Depression in HIV infected patients: A review. Current Psychiatry Reports, 17(1), 530. https://doi.org/10.1007/s11920-014-0530-4
- Oexle, N., Müller, M., Kawohl, W., Xu, Z., Viering, S., Wyss, C., Vetter, S., & Rüsch, N. (2018). Self-stigma as a barrier to recovery: A longitudinal study. European Archives of Psychiatry and Clinical Neuroscience, 268(2), 209–212. https://doi.org/10.1007/s00406-017-0773-2
- Pearson, C. A., Johnson, M. O., Neilands, T. B., Dilworth, S. E., Sauceda, J. A., Mugavero, M. J., Crane, H. M., Fredericksen, R. J., Mathews, W. C., Moore, R. D., Napravnik, S., Mayer, K. H., & Christopoulos, K. A. (2021). Internalized HIV stigma predicts suboptimal retention in care Among people living with HIV in the United States. AIDS Patient Care and STDs, 35(5), 188–193. https://doi.org/10.1089/apc.2020.0244
- Pederson, A. B., Burnett-Zeigler, I., Fokuo, J. K., Wisner, K. L., Zumpf, K., & Oshodi, Y. (2020). Mental health stigma among university health care students in Nigeria: A cross-sectional observational study. Pan African Medical Journal, 37, 5. https://doi.org/10.11604/pamj.2020.37.5.24898
- Peltzer, K., & Pengpid, S. (2019). Prevalence and associated factors of enacted, Internalized And anticipated stigma Among people living With HIV In South Africa: Results Of The first national survey. HIV/AIDS (Auckland, N.Z.), 11, 275–285. https://doi.org/10.2147/HIV.S229285
- Philippi, C. L., Reyna, L., Nedderman, L., Chan, P., Samboju, V., Chang, K., Phanuphak, N., Ratnaratorn, N., Hellmuth, J., Benjapornpong, K., Dumrongpisutikul, N., Pothisri, M., Robb, M. L., Ananworanich, J., Spudich, S., Valcour, V., & Paul, R. (2020). Resting-state neural signatures of depressive symptoms in acute HIV. Journal of Neurovirology, 26(2), 226–240. https://doi.org/10.1007/s13365-020-00826-3
- Ran, M.-S., Zhang, T.-M., Wong, I. Y.-L., Yang, X., Liu, C.-C., Liu, B., Luo, W., Kuang, W.-H., Thornicroft, G., & Chan, C. L.-W. (2018a). Internalized stigma in people with severe mental illness in rural China. International Journal of Social Psychiatry, 64(1), 9–16. https://doi.org/10.1177/0020764017743999
- Ran, M.-S., Zhang, T.-M., Wong, I. Y.-L., Yang, X., Liu, C.-C., Liu, B., Luo, W., Kuang, W.-H., Thornicroft, G., & Chan, C. L.-W. (2018b). Internalized stigma in people with severe mental illness in rural China. International Journal of Social Psychiatry, 64(1), 9–16. https://doi.org/10.1177/0020764017743999
- Rao, D., Chen, W. T., Pearson, C. R., Simoni, J. M., Fredriksen-Goldsen, K., Nelson, K., Zhao, H., & Zhang, F. (2012). Social support mediates the relationship between HIV stigma and depression/quality of life among people living with HIV in Beijing, China. International Journal of STD & AIDS, 23(7), 481–484. https://doi.org/10.1258/ijsa.2009.009428
- Rice, W. S., Crockett, K. B., Mugavero, M. J., Raper, J. L., Atkins, G. C., & Turan, B. (2017). Association between internalized HIV-related stigma and HIV care visit adherence. JAIDS Journal of Acquired Immune Deficiency Syndromes, 76(5), 482–487. https://doi.org/10.1097/QAI.0000000000001543
- Saliu, A., & Akintunde, B. (2014). Knowledge, attitude, and preventive practices among prison inmates in Ogbomoso prison at Oyo state, south west Nigeria. International Journal of Reproductive Medicine, 2014, 364375. https://doi.org/10.1155/2014/364375
- Sano, Y., Antabe, R., Atuoye, K. N., Hussey, L. K., Bayne, J., Galaa, S. Z., Mkandawire, P., & Luginaah, I. (2016). Persistent misconceptions about HIV transmission among males and females in Malawi. BMC International Health and Human Rights, 16(1), 16. https://doi.org/10.1186/s12914-016-0089-8
- Sardá Jr, J., Nicholas, M. K., Asghari, A., & Pimenta, C. A. M. (2009). The contribution of self-efficacy and depression to disability and work status in chronic pain patients: A comparison between Australian and Brazilian samples. European Journal of Pain, 13(2), 189–195. https://doi.org/10.1016/j.ejpain.2008.03.008
- Sayles, J. N., Hays, R. D., Sarkisian, C. A., Mahajan, A. P., Spritzer, K. L., & Cunningham, W. E. (2008). Development and psychometric assessment of a multidimensional measure of internalized HIV stigma in a sample of HIV-positive adults. AIDS and Behavior, 12(5), 748–758. https://doi.org/10.1007/s10461-008-9375-3
- Shumet, S., W/Michele, B., Angaw, D., Ergete, T., & Alemnew, N. (2021). Magnitude of internalised stigma and associated factors among people with bipolar disorder at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia: A cross-sectional study. BMJ Open, 11(4), e044824. https://doi.org/10.1136/bmjopen-2020-044824
- Simbayi, L. C., Strebel, A., Cloete, A., Henda, N., & Mqeketo, A. (2007). Internalized stigma, discrimination, and depression among men and women living with HIV/AIDS in Cape Town, South Africa. Social Science & Medicine, 64(9), 1823–1831. https://doi.org/10.1016/j.socscimed.2007.01.006
- Sorsdahl, K. R., Kakuma, R., Wilson, Z., & Stein, D. J. (2012). The internalized stigma experienced by members of a mental health advocacy group in South Africa. International Journal of Social Psychiatry, 58(1), 55–61. https://doi.org/10.1177/0020764010387058
- Stewart, R. C., Umar, E., Tomenson, B., & Creed, F. (2014). Validation of the multi-dimensional scale of perceived social support (MSPSS) and the relationship between social support, intimate partner violence and antenatal depression in Malawi. BMC Psychiatry, 14(1), 180. https://doi.org/10.1186/1471-244X-14-180
- Subedi, B., Timilsina, B. D., & Tamrakar, N. (2019). Perceived stigma among people living with HIV/AIDS in Pokhara, Nepal. HIV/AIDS (Auckland, N.Z.), 11, 93–103. https://doi.org/10.2147/HIV.S181231
- Takada, S., Weiser, S. D., Kumbakumba, E., Muzoora, C., Martin, J. N., Hunt, P. W., Haberer, J. E., Kawuma, A., Bangsberg, D. R., & Tsai, A. C. (2014). The dynamic relationship between social support and HIV-related stigma in rural Uganda. Annals of Behavioral Medicine, 48(1), 26–37. https://doi.org/10.1007/s12160-013-9576-5
- Tandon, S. D., Latimore, A. D., Clay, E., Mitchell, L., Tucker, M., & Sonenstein, F. L. (2015). Depression outcomes associated with an intervention implemented in employment training programs for low-income adolescents and young adults. JAMA Psychiatry, 72(1), 31–39. https://doi.org/10.1001/jamapsychiatry.2014.2022
- Tesfaye, E., Worku, B., Girma, E., & Agenagnew, L. (2020). Internalized stigma among patients with mood disorders in Ethiopia: A cross-sectional facility-based study. International Journal of Mental Health Systems, 14(1), 32. https://doi.org/10.1186/s13033-020-00365-8
- Teshale, A. B., & Tesema, G. A. (2022). Discriminatory attitude towards people living with HIV/AIDS and its associated factors among adult population in 15 sub-Saharan African nations. PloS One, 17(2), e0261978. https://doi.org/10.1371/journal.pone.0261978
- Tsai, A. C. (2015). Socioeconomic gradients in internalized stigma among 4,314 persons with HIV in sub-Saharan Africa. AIDS and Behavior, 19(2), 270–282. https://doi.org/10.1007/s10461-014-0993-7
- Turan, B., Smith, W., Cohen, M. H., Wilson, T. E., Adimora, A. A., Merenstein, D., Adedimeji, A., Wentz, E. L., Foster, A. G., Metsch, L., Tien, P. C., Weiser, S. D., & Turan, J. M. (2016). Mechanisms for the negative effects of internalized HIV-related stigma on antiretroviral therapy adherence in women. JAIDS Journal of Acquired Immune Deficiency Syndromes, 72(2), 198–205. https://doi.org/10.1097/QAI.0000000000000948
- Udedi, M. (2014). The prevalence of depression among patients and its detection by primary health care workers at Matawale Health Centre (Zomba). Malawi Medical Journal: The Journal of Medical Association of Malawi, 26(2), 34–37.
- Udedi, M., Muula, A. S., Stewart, R. C., & Pence, B. W. (2019). The validity of the patient health Questionnaire-9 to screen for depression in patients with type-2 diabetes mellitus in non-communicable diseases clinics in Malawi. BMC Psychiatry, 19(1), 81. https://doi.org/10.1186/s12888-019-2062-2
- Werner, P., Stein-Shvachman, I., & Heinik, J. (2009). Perceptions of self-stigma and its correlates among older adults with depression: A preliminary study. International Psychogeriatrics, 21(6), 1180–1189. https://doi.org/10.1017/S1041610209990470
- Woon, L. S.-C., Khoo, S. I., Baharudin, A., & Midin, M. (2020). Association between insight and internalized stigma and other clinical factors among patients with depression: A cross-sectional study. Indian Journal of Psychiatry, 62(2), 186–192. https://doi.org/10.4103/psychiatry.IndianJPsychiatry_612_19
- The World Bank. (2022). Prevalence of HIV, total (% of population ages 15-49)—Malawi. The World Bank Data. https://data.worldbank.org/indicator/SH.DYN.AIDS.ZS?locations=MW.
- World Health Organization. (2012). Measuring health and disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0) (p. 88) [Manual]. World Health Organization. https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health/who-disability-assessment-schedule
- Wroe, E. B., Kalanga, N., Dunbar, E. L., Nazimera, L., Price, N. F., Shah, A., Dullie, L., Mailosi, B., Gonani, G., Ndarama, E. P. L., Talama, G. C., Bukhman, G., Kerr, L., Connolly, E., & Kachimanga, C. (2020). Expanding access to non-communicable disease care in rural Malawi: Outcomes from a retrospective cohort in an integrated NCD–HIV model. BMJ Open, 10(10), e036836. https://doi.org/10.1136/bmjopen-2020-036836
- Yator, O., Mathai, M., Albert, T., & Kumar, M. (2021). Burden of HIV-related stigma and post-partum depression: A cross-sectional study of patients attending prevention of mother-to-child transmission clinic at kenyatta national hospital in Nairobi. Frontiers in Psychiatry, 11, https://www.frontiersin.org/articles/10.3389fpsyt.2020.532557. https://doi.org/10.3389/fpsyt.2020.532557
- Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. https://doi.org/10.1207/s15327752jpa5201_2
