
ABSTRACT
Injectable antiretroviral treatment (ART) represents a new effective and potentially more convenient alternative to oral ART for people living with HIV (PLWH). This study assessed preferences of PLWH for long-acting injectable compared with oral ART in the Netherlands. A labelled discrete choice experiment presented 12 choice sets of long-acting injectable and oral ART. PLWH were asked to select their preferred ART, described by six attributes: location of administration, dosing frequency, risk of short-term side effects, drug–drug interaction, forgivability, and food and mealtime restrictions. Random parameters logit and latent class models were used to estimate preferences of PLWH. 98.6% of 76 respondents were experienced oral ART users that had taken ART for a median of 12 years (Q1–Q3: 7.0–20.0). 30 (39.5%) respondents chose long-acting injectable ART in all choice tasks and 22 (28.9%) always chose oral ART. The random parameter model showed that, on average, respondents significantly favoured long-acting injectable ART over oral ART, preferred administration of the long-acting injectable ART at home, and a less frequent regimen. The latent class model confirmed one class strongly preferring long-acting injectable ART and one class slightly preferring oral ART. This study highlights the value for both long-acting injectable and oral ART.
Introduction
Care for people living with HIV (PLWH) in the Netherlands has exceeded the 90-90-90 goal set by the United Nations Programme on HIV/AIDS and World Health Organization (Joint United Nations Programme on HIV/AIDS (UNAIDS), Citation2014). As of 2018, 92% of people diagnosed with HIV and aware of their status are receiving care, 93% of these people start antiretroviral treatment (ART) and in 96% of these people viral suppression is achieved (van Sighem et al., Citation2019). Consequently, 82% of the total estimated number of PLWH in the Netherlands are successfully treated with ART, and efforts continue to improve the number of people receiving optimal care (van Sighem et al., Citation2019). Strict adherence to ART by PLWH is required for successful sustained suppression of viral load (Paterson et al., Citation2000). Barriers to ART adherence include treatment-related factors, for example, complex regimens or the number of pills required (Iacob et al., Citation2017; Katz et al., Citation2013; Mills et al., Citation2006; Nachega et al., Citation2014). Increased availability of simpler ART regimens or new ART are important reasons for switching ART (van Sighem et al., Citation2019). Up to recently, available ART treatments were orally administrated on a daily basis only, but long-acting injectable ART treatments are now approved for clinical use too (Aschenbrenner, Citation2021; Flexner et al., Citation2021; Markham, Citation2020). Injectable ART could be considered less complex in administration by PLWH since, for example, no food and meal restrictions and people do not need to take their treatments on a daily basis when receiving injectable ART. Two large, randomised clinical trials (ATLAS and FLAIR) showed switching to monthly long-acting injectable ART to be non-inferior to continuing oral ART (Orkin et al., Citation2020; Swindells et al., Citation2020). Both studies also revealed high treatment satisfaction and preference for the injectable versus the daily oral therapy (Murray et al., Citation2020). Results from the ATLAS-2M trial comparing long-acting injections every 8 weeks to injections every 4 weeks showed similar antiretroviral efficacy and safety profiles, supporting the option of less frequent dosing (Overton et al., Citation2020). Injectable ART therefore represents a new effective and potentially more convenient treatment for PLWH.
Information about how patients value various aspects of a healthcare intervention can be useful for policy decision makers when assessing these interventions (Bridges et al., Citation2011), and has already been used in reimbursement and pricing decisions (Marsh et al., Citation2020). Moreover, a better understanding of patient preferences for treatment (attributes) and investigating patient profiles with a preference for certain types of medication can facilitate healthcare professionals (HCPs) in making shared decisions and improving adherence.
Discrete choice experiments (DCEs) elicit patient preferences in healthcare by quantifying the relative importance of various attributes that characterise a treatment and trade-offs that respondents make between these attributes (Clark et al., Citation2014). A number of DCEs have been conducted to assess preferences for HIV prevention (Beckham et al., Citation2021), HIV care, and oral ART (Humphrey et al., Citation2019), but there is a paucity of studies focusing on preferences for long-acting injectable and oral ART, and no such studies have been conducted in the Netherlands. One study among PLWH in the US found modest acceptability of hypothetical injectable ART but did not explicitly elicit preferences for long-acting injectable or oral ART or their attributes (Simoni et al., Citation2020). Moreover, preference data could differ between populations or countries, suggesting the need for national data to support policy makers with understanding the potential value of long-acting injectable and oral treatment. This DCE aims to elicit preferences of PLWH in the Netherlands for long-acting injectable compared with oral ART, and to assess the importance of treatment attributes beyond the regimen itself in the patients’ choice for an ART.
Methods
A DCE consists of several choice sets describing two or more alternative options according to a list of attributes. In each choice set, the levels of each attribute vary, resulting in different hypothetical alternative options. Respondents choose their preferred option in each choice set. This DCE was developed according to the guidelines provided by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Good Research Practice for Conjoint Analysis Task Force (Bridges et al., Citation2011). A labelled DCE was used, with two hypothetical treatment options categorised as long-acting injectable ART or oral ART, to specifically look at preference for administration method of ART and how other ART attributes affect this preference. Labelled designs offer less abstract choices to respondents adding more validity to the results (Kruijshaar et al., Citation2009). An opt-out option was not allowed as no treatment does not represent a viable option for PLWH.
Attributes and levels
A three-step approach was used to select relevant attributes and levels for inclusion in the DCE. First, a literature review via a systematic database search identified attributes used in earlier studies on preferences (conjoint analysis or willingness-to-pay assessment) of PLWH for ART in general and specifically for long-acting injectable and oral ART.
Thereafter, individual interviews with PLWH identified any missing ART attributes and prioritised the most important attributes for inclusion in the DCE using an a priori compiled interview guide. Adults ≥18 years of age living with HIV with knowledge about ART were invited to participate via a social media platform, hosted by the Dutch Association for PLWH. From 27 May 2020 until 10 June 2020, 15 interviews were performed until data saturation was reached. Based on the interviews, attributes reported most often as important were selected and described using the definitions provided by the participants. Five attributes were initially selected by the research team for inclusion in the DCE: common side effects, frequency of administration, location of administration, drug–drug interaction (DDI) and forgivability of missing doses (i.e., delay allowed after a missed dose). Criteria for inclusion required that the attributes were (1) important in the interviews, (2) conceptually different from each other, (3) would differentiate between long-acting injectable and oral ART, and (4) relevant for the objective of the study. In the absence of differences in effectiveness and long-term side effects or safety profile between long-acting injectable and oral ART (Orkin et al., Citation2020; Swindells et al., Citation2020), no attributes about these aspects were included.
The selected attributes were validated by an expert group, which included a Dutch HCP specialised in the treatment of PLWH and a patient advocate. The comprehensiveness and definitions of the attributes on the final lists were discussed with the expert group, based on which an additional attribute was added: “food and mealtime restrictions”. Then, attribute levels were identified by the researchers based on existing literature reporting on ART and discussed with experts. The final list of attributes and levels is found in . Further details on the methods and results of attributes and level selection are provided in the Supplemental Material.
Table 1. Attributes and levels of oral and long-acting injectable ART.
Questionnaire/data collection and recruitment
A Bayesian efficient experiment design with Ngene software (version 1.1.1) (Reed Johnson et al., Citation2013) was used to determine a subset of all possible ART profiles based on the selected attributes to present to respondents in the DCE. This experimental design maximises the precision of estimated parameters by maximising the D efficiency – a summary measure of the variance covariance matrix, for a given number of choice questions. Three different versions were compiled, each consisting of 12 choice tasks. Respondents were randomly presented with one of the three versions of the DCE. In each choice set, respondents chose either the long-acting injectable or oral ART. provides an example of a choice set.
Figure 1. Example of a choice task in the discrete choice experiment.
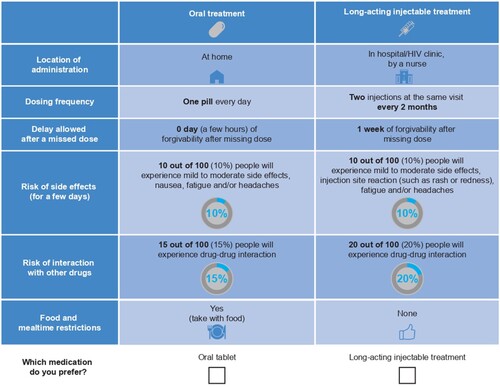
The DCE questionnaire consisted of (1) an information leaflet and informed consent form; (2) a description of the exercise and an example of the choice set, completed; (3) questions about the experience of completing the choice tasks, and (4) questions about the respondent’s demographic, disease-specific and other characteristics that could affect willingness to take long-acting injectable or oral ART (i.e., willingness to switch, ease of visiting and distance to clinics, experience with injections, injection anxiety). To answer frequently asked questions raised by participants in the interviews, we included a general description about oral and injectable ART in the introduction of the questionnaire. Oral ART was described as: “For oral ART you need to pick up a receipt at the pharmacy regularly, store the ART at home and pack the ART while traveling”. Injectable ART was described as:
For injectable ARTs you need to visit the hospital or HIV clinic monthly or bimonthly. You do not need to take additional oral medication to treat the HIV. Most people experience mild pain from administrating the injection. Soreness can last up to three days. Most patients expressed the pain of administrating the injection as “completely” or “very” acceptable.
Respondents for the DCE questionnaire were recruited via an invitation on the website and social media platforms of the Dutch Association for PLWH from July to August 2020. PLWH who were ≥18 years of age were eligible.
The study design of the interviews and online questionnaire with PLWH was approved by the Research Ethics Committee of the Faculty of Health, Medicine and Life Sciences of Maastricht University (FHML-REC/2020/057). Respondents provided informed consent before participation in the study.
Data analysis
Questionnaires were included in the analysis if a respondent completed all choice sets. Respondent characteristics were analysed using descriptive statistics. For continuous variables, median and interquartile ranges (IQRs) were described because of the deviations from normal distribution, and frequency and percentages for discrete variables. Normality of continuous variables were checked using four methods: Shapiro–Wilks test, quantile-quantile plot, histograms, and comparison of the mean and median.
First, the number of respondents who consistently chose oral ART in all choice sets, who consistently chose long-acting injectable ART in all choice sets and whose choice varied across the choice sets was determined. Heterogeneity in differences between the three groups in terms of their demographic and disease-specific characteristics were then explored using a Kruskal–Wallis test for continuous variables, and a Chi-squared test for categorical data with IBM SPSS 24 (IBM Corp, Armonk, NY). Respondents always choosing oral ART compared with those always choosing long-acting injectable ART was analysed using a Mann–Witney U test for continuous variable, and a Chi-squared test or a Fisher’s exact test for categorical variables.
Data derived from the choice sets were analysed using Nlogit software (version 6) to assess preference for attributes and levels, and to reveal heterogeneity in respondents’ preferences. A random parameter model was first applied, which allows for the capture of heterogeneity in preferences by estimating the standard deviation (SD) of parameter distribution (Hauber et al., Citation2016). All attributes were categorical variables and translated into effect coding. Using effect coding, estimated coefficients for each level indicate the magnitude of the preference and whether the preference is positive or negative compared with the mean of the attribute. If significantly different from zero, the SD shows the magnitude of the heterogeneity in preference for the ART attributes and levels in the sample (Hauber et al., Citation2016). For the estimation of the parameter values, 250 Halton draws were conducted.
Finally, a latent class model was used to identify clusters of respondents with equivalent preference profiles (Zhou et al., Citation2018). To determine the number of classes, we selected the model with the best fit based on the Akaike information criterion. To investigate if the latent classes differed according to respondents’ characteristics, a Kruskal–Wallis test for continuous variables and a Chi-squared test for categorical data were then conducted with IBM SPSS 24 (IBM Corp, Armonk, NY, USA) to test whether (socio-economic and medical) characteristics significantly differed across latent classes.
Results
Respondent characteristics
Overall, 76 respondents completed all choice sets of the DCE and were included in the analysis. shows, that most respondents identified as male (84.5%), had a median age of 51.0 (IQR 43.0–58.0) years and 58.3% were higher educated. Most respondents were born in the Netherlands (82.9%) and had a median of 13.5 (IQR 7.0–25.0) years living with HIV. Almost all respondents were using ART (98.6%) for a median of 12.0 (IQR 7.0–20.0) years, and 64.8% reported to have ever missed a dose, but most respondents indicated that this was less than once a week (median 0.0 [IQR 0.0–0.3] of missed doses per week). Of the respondents, 14.5% had a low willingness to switch ARTs and 8.4% of respondents reported that visiting a HIV clinic is difficult or very difficult for them.
Table 2. Demographic and disease characteristics of respondents and comparison of the respondents always choosing oral, long-acting injectable and with variable choice in the choice tasks of the discrete choice experiment.Table Footnote†
Choice task analysis
Of the 76 respondents, 30 (39.5%) chose long-acting injectable ART in all choice tasks, while 22 (28.9%) always chose oral ART, and for 24 (31.6%) respondents the choice varied in the 12 choice tasks. Comparison of the three groups showed no statistically significant differences in demographic and disease-specific characteristics (), but the respondents always choosing oral ART reported significantly lower willingness to switch ART than respondents always choosing long-acting injectable ART (p = 0.006).
Random parameter model
Results of the random parameter model are presented in . All attributes, except for forgivability, were statistically significant. The SDs were relatively large, indicating substantial variability in the respondents’ preferences, especially for the injectable and oral administration method (SD = 12.89, 95% confidence interval 7.39, 18.38). On average, respondents favoured long-acting injectable ART over oral ART, preferred administration of the long-acting injectable ART at home by a nurse compared with administration at a hospital, and preferred two injections at the same visit every 2 months compared with every month. For oral ART, respondents favoured one compared with two pills each day. Moreover, respondents had a significant preference for ART with lower risks of side effects and DDIs, and respondents had a significant preference for taking ART with food compared with taking ART on an empty stomach.
Table 3. Results of the mixed logit model.
Latent classes
Results of the latent class analysis are presented in . Two latent classes of respondents were identified: 48.7% of respondents were allocated to class 1 and 51.3% to class 2. Respondents in class 1 had a statistically significant preference for long-acting injectable ART compared with oral ART, while the respondents in class 2 had a statistically significant, though less pronounced preference for oral ART. Respondents in class 2 were also shown to have a significant preference for administration of ART at home, for less frequent administration and for having a 10% over a 15% or 20% risk of DDIs. For class 1, similar positive preferences were found for a 10% risk on DDI compared with higher risks. Other attributes did not reach statistical significance.
Table 4. Results of the latent class analysis.
Statistically significant differences in disease characteristics at an alpha of 0.1 were found between respondents in class 1 and class 2 (Supplemental Material). Respondents in class 2 had lived longer with HIV compared with respondents in class 1 (median [IQR] of 15 [10–26] and 11 [4–19.5] years, respectively, p = 0.006) and had been on HIV medication for longer (median [IQR] of 15 [7.8–23.2] and 10 [4–15] years, respectively, p = 0.008). Respondents in class 1 were more willing to switch ART (p = 0.08), reported less anxiety for needles (p = 0.047) and regarded it easier to visit the hospital (p = 0.02) than respondents in class 2.
Discussion
This study revealed PLWH have strong preferences regarding mode of delivery of ART, specifically long-acting injectable or oral ART. Approximately 40% of respondents preferred long-acting injectable ART, while 29% of respondents preferred oral ART, suggesting that many PLWH would welcome the availability of long-acting injectable ART. The analysis of the responses to the choice sets in the DCE confirmed, on average, a small overall preference for long-acting injectable ART. Moreover, respondents had a pronounced preference for dosing regimens with less frequent administration and lower risks of short-term side effects and DDIs. Heterogeneity in preferences within the sample was, however, substantial.
Latent class analysis confirmed the presence of two profiles within our sample. The first class strongly preferred long-acting injectable ART over oral ART, while the second class slightly preferred oral over long-acting injectable ART. The respondents in the second class had lived with HIV for significantly longer and had also been receiving ART for longer. Simoni et al. (Citation2019) reported, in a qualitative study about the acceptability of long-acting injectable ART, that daily oral ART has already been integrated into the daily routines of these people, making the dosing regimens not that burdensome. Additionally, people in the second class also had significantly more anxiety for needles and more difficulty visiting a clinic, which could also explain their lower willingness to switch from oral to long-acting injectable ART (Simoni et al., Citation2019).
To our knowledge, this study is among the first to investigate preferences for long-acting injectable versus oral ART (Humphrey et al., Citation2019). This makes it difficult to compare our results with previous studies. A study focused on eliciting preferences for targeted long-acting combination ART identified modest acceptability of injectable ART by PLWH in the US, and efficacy and dosing frequency significantly affected acceptability (Simoni et al., Citation2020). Our study did not include efficacy as an attribute as efficacy, in terms of maintaining viral suppression in already suppressed patients, of long-acting injectable and oral ART are comparable, but we noted significant preferences for lower compared with higher frequency of administration.
The information provided in the current study on the preference of PLWH for administration regimens of ART could be useful for HCPs, policy decision makers and payers. For payers and policy decision makers, this study suggests that there is a demand for both long-acting injectable and oral ART, and policy decisions could be made accordingly. As long-acting injectable ART has been approved (by the European Medicines Agency and elsewhere) (Aschenbrenner, Citation2021; Flexner et al., Citation2021; Markham, Citation2020), this could be a valuable alternative for a substantial number of PLWH. For HCPs, information about preferences of PLWH for long-acting injectable and oral ART could be relevant in clinical decision making. HCPs should be aware though that individuals could have different preferences, which warrants shared decision making to ensure choices fit well with the individual’s preferences.
A limitation that should be considered when interpreting the current results is the limited sample size including 76 respondents. Although sufficient to estimate stable and significant parameters for the attributes and levels for the total sample, the sample size was too limited for extensive subgroup analysis and understanding of differences between groups and latent classes. Another limitation is that the sample included a relatively high proportion of respondents born in the Netherlands and with a higher educational level compared with the general population of PLWH in the Netherlands (van Sighem et al., Citation2019). Certain subgroups were not adequately represented, such as women, women with children, persons with different ethnicities or less experienced ART users. Their preferences may differ from the mean preferences found in the study sample. Finally, although a description of pain and discomfort associated with long-acting ART administrated intramuscularly was provided in the introduction of the questionnaire, they were not explicitly included as a separate attribute which could have potentially impacted patients’ preferences.
Conclusions
This study revealed that PLWH have a strong preference for mode of administration. Other attributes that affect ART choice significantly are administration location, dosing frequency, risk of short-term side effects, risks of DDIs and food and mealtime restrictions. However, preferences of certain subgroups underrepresented in the study sample may deviate from the average preferences found. This study therefore highlights the value and place in practice for a long-acting injectable ART and provides information for further development of these types of ART to meet preferences of PLWH.
Supplemental Material
Download MS Word (2.6 MB)Acknowledgements
The funders of the study were involved in the study design but not in data analysis and data interpretation. Researchers from Maastricht University were fully independent in final decisions regarding this project and manuscript. The authors thank Nicolas van de Velde and Vasiliki Chounta for advice during attributes selection; Suus Koene (Maastricht University) for setting up the survey in Qualtrics; the Dutch Association for People living with HIV (and in particular Renée Finkenflügel) for support through the project (advice on participants’ documents, questionnaire and attributes review, media posts for participants’ recruitment); healthcare professionals for comments on attribute and level selection, and all the participants for their contribution in this study. Editorial support (in the form of writing assistance, including redrawing of figures, grammatical editing and referencing) was provided by Liz Morgan, PhD, at Fishawack Indicia Ltd., part of Fishawack Health, and was funded by GSK. Authors’ Contributions: IK, MH, JS, MS and HP designed the research study. IK and MH performed the research. IK, MH and CB analysed study results. IK and MH wrote the paper. All authors critically reviewed the paper.
Disclosure statement
HP and MS are employees of ViiV HealthCare. JS is an employee of GSK. MH, CB and IK have no conflict of interest to declare, except the funding of this study from ViiV Healthcare received through institution.
Additional information
Funding
References
- Aschenbrenner, D. S. (2021). First extended-release injectable drug therapy for HIV. American Journal of Nursing, 121(5), 24–25. https://doi.org/10.1097/01.Naj.0000751096.82989.00
- Beckham, S. W., Crossnohere, N. L., Gross, M., & Bridges, J. F. P. (2021). Eliciting preferences for HIV prevention technologies: A systematic review. The Patient, 14(2), 151–174. https://doi.org/10.1007/s40271-020-00486-9
- Bridges, J. F., Hauber, A. B., Marshall, D., Lloyd, A., Prosser, L. A., Regier, D. A., Johnson, F. R., & Mauskopf, J. (2011). Conjoint analysis applications in health–a checklist: A report of the ISPOR good research practices for conjoint analysis task force. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 14(4), 403–413. https://doi.org/10.1016/j.jval.2010.11.013
- Clark, M. D., Determann, D., Petrou, S., Moro, D., & de Bekker-Grob, E. W. (2014). Discrete choice experiments in health economics: A review of the literature. Pharmacoeconomics, 32(9), 883–902. https://doi.org/10.1007/s40273-014-0170-x
- Flexner, C., Owen, A., Siccardi, M., & Swindells, S. (2021). Long-acting drugs and formulations for the treatment and prevention of HIV infection. International Journal of Antimicrobial Agents, 57(1), Article 106220. https://doi.org/10.1016/j.ijantimicag.2020.106220
- Hauber, A. B., González, J. M., Groothuis-Oudshoorn, C. G., Prior, T., Marshall, D. A., Cunningham, C., IJzerman, M. J., & Bridges, J. F. P. (2016). Statistical methods for the analysis of discrete choice experiments: A report of the ISPOR conjoint analysis good research practices task force. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 19(4), 300–315. https://doi.org/10.1016/j.jval.2016.04.004
- Humphrey, J. M., Naanyu, V., MacDonald, K. R., Wools-Kaloustian, K., & Zimet, G. D. (2019). Stated-preference research in HIV: A scoping review. PLoS One, 14(10), Article e0224566. https://doi.org/10.1371/journal.pone.0224566
- Iacob, S. A., Iacob, D. G., & Jugulete, G. (2017). Improving the adherence to antiretroviral therapy, a difficult but essential task for a successful HIV treatment-clinical points of view and practical considerations. Frontiers in Pharmacology, 8, Article 831. https://doi.org/10.3389/fphar.2017.00831
- Joint United Nations Programme on HIV/AIDS (UNAIDS). (2014). 90-90-90: An ambitious treatment target to help end the AIDS epidemic. https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf
- Katz, I. T., Ryu, A. E., Onuegbu, A. G., Psaros, C., Weiser, S. D., Bangsberg, D. R., & Tsai, A. C. (2013). Impact of HIV-related stigma on treatment adherence: Systematic review and meta-synthesis. Journal of the International AIDS Society, 16(3 Suppl 2), Article 18640. https://doi.org/10.7448/IAS.16.3.18640
- Kruijshaar, M. E., Essink-Bot, M.-L., Donkers, B., Looman, C. W. N., Siersema, P. D., & Steyerberg, E. W. (2009). A labelled discrete choice experiment adds realism to the choices presented: Preferences for surveillance tests for barrett esophagus. BMC Medical Research Methodology, 9(1), Article 31. https://doi.org/10.1186/1471-2288-9-31
- Markham, A. (2020). Cabotegravir plus rilpivirine: First approval. Drugs, 80(9), 915–922. https://doi.org/10.1007/s40265-020-01326-8
- Marsh, K., van Til, J. A., Molsen-David, E., Juhnke, C., Hawken, N., Oehrlein, E. M., Choi, Y. C., Duenas, A., Greiner, W., Haas, K., Hiligsmann, M., Hockley, K. S., Ivlev, I., Liu, F., Ostermann, J., Poder, T., Poon, J. L., & Muehlbacher, A. (2020). Health preference research in Europe: A review of Its Use in marketing authorization, reimbursement, and pricing decisions-report of the ISPOR stated preference research special interest group. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 23(7), 831–841. https://doi.org/10.1016/j.jval.2019.11.009
- Mills, E. J., Nachega, J. B., Bangsberg, D. R., Singh, S., Rachlis, B., Wu, P., Wilson, K., Buchan, I., Gill, C. J., & Cooper, C. (2006). Adherence to HAART: A systematic review of developed and developing nation patient-reported barriers and facilitators. PLoS Medicine, 3(11), Article e438. https://doi.org/10.1371/journal.pmed.0030438
- Murray, M., Antela, A., Mills, A., Huang, J., Jäger, H., Bernal, E., Lombaard, J., Katner, H., Walmsley, S., Khuong-Josses, M. A., Hudson, K., Dorey, D., Griffith, S., Spreen, W., Vanveggel, S., Shaefer, M., Margolis, D., & Chounta, V. (2020). Patient-reported outcomes in ATLAS and FLAIR participants on long-acting regimens of cabotegravir and rilpivirine over 48 weeks. AIDS and Behavior, 24(12), 3533–3544. https://doi.org/10.1007/s10461-020-02929-8
- Nachega, J. B., Parienti, J. J., Uthman, O. A., Gross, R., Dowdy, D. W., Sax, P. E., Gallant, J. E., Mugavero, M. J., Mills, E. J., & Giordano, T. P. (2014). Lower pill burden and once-daily antiretroviral treatment regimens for HIV infection: A meta-analysis of randomized controlled trials. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America, 58(9), 1297–1307. https://doi.org/10.1093/cid/ciu046
- Orkin, C., Arasteh, K., Górgolas Hernández-Mora, M., Pokrovsky, V., Overton, E. T., Girard, P. M., Oka, S., Walmsley, S., Bettacchi, C., Brinson, C., Philibert, P., Lombaard, J., St Clair, M., Crauwels, H., Ford, S. L., Patel, P., Chounta, V., D'Amico, R., Vanveggel, S., … Spreen, W. R. (2020). Long-Acting cabotegravir and rilpivirine after oral induction for HIV-1 infection. New England Journal of Medicine, 382(12), 1124–1135. https://doi.org/10.1056/NEJMoa1909512
- Overton, E. T., Richmond, G., Rizzardini, G., Jaeger, H., Orrell, C., Nagimova, F., Bredeek, F., García Deltoro, M., Swindells, S., Andrade-Villanueva, J. F., Wong, A., Khuong-Josses, M. A., Van Solingen-Ristea, R., van Eygen, V., Crauwels, H., Ford, S., Talarico, C., Benn, P., Wang, Y., … Spreen, W. (2020). Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: A randomised, multicentre, open-label, phase 3b, non-inferiority study. The Lancet, 396(10267), 1994–2005. https://doi.org/10.1016/S0140-6736(20)32666-0
- Paterson, D. L., Swindells, S., Mohr, J., Brester, M., Vergis, E. N., Squier, C., Wagener, M. M., & Singh, N. (2000). Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Annals of Internal Medicine, 133(1), 21–30. https://doi.org/10.7326/0003-4819-133-1-200007040-00004
- Reed Johnson, F., Lancsar, E., Marshall, D., Kilambi, V., Mühlbacher, A., Regier, D. A., Regier, D., Bresnahan, B. W., Kanninen, B., & Bridges, J. F. (2013). Constructing experimental designs for discrete-choice experiments: Report of the ISPOR conjoint analysis experimental design good research practices task force. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 16(1), 3–13. https://doi.org/10.1016/j.jval.2012.08.2223
- Simoni, J. M., Beima-Sofie, K., Mohamed, Z. H., Christodoulou, J., Tapia, K., Graham, S. M., Ho, R., & Collier, A. C. (2019). Long-acting injectable antiretroviral treatment acceptability and preferences: A qualitative study Among US providers, adults living with HIV, and parents of youth living with HIV. AIDS Patient Care and STDs, 33(3), 104–111. https://doi.org/10.1089/apc.2018.0198
- Simoni, J. M., Tapia, K., Lee, S. J., Graham, S. M., Beima-Sofie, K., Mohamed, Z. H., Christodoulou, J., Ho, R., & Collier, A. C. (2020). A conjoint analysis of the acceptability of targeted long-acting injectable antiretroviral therapy among persons living with HIV in the U.S. AIDS and Behavior, 24(4), 1226–1236. https://doi.org/10.1007/s10461-019-02701-7
- Swindells, S., Andrade-Villanueva, J. F., Richmond, G. J., Rizzardini, G., Baumgarten, A., Masiá, M., Latiff, G., Pokrovsky, V., Bredeek, F., Smith, G., Cahn, P., Kim, Y. S., Ford, S. L., Talarico, C. L., Patel, P., Chounta, V., Crauwels, H., Parys, W., Vanveggel, S., … Spreen, W. R. (2020). Long-acting cabotegravir and rilpivirine for maintenance of HIV-1 suppression. New England Journal of Medicine, 382(12), 1112–1123. https://doi.org/10.1056/NEJMoa1904398
- van Sighem, A. I., Wit, F. W. N. M., Boyd, A., Smit, C., Matser, A., & Reiss, P. (2019). Monitoring Report 2019. Human Immunodeficiency Virus (HIV) Infection in the Netherlands. Stichting HIV Monitoring. https://www.hiv-monitoring.nl/application/files/4115/7616/1682/HIV_Monitoring_Report_2019_update_dec_2019.pdf
- Zhou, M., Thayer, W. M., & Bridges, J. F. P. (2018). Using latent class analysis to model preference heterogeneity in health: A systematic review. Pharmacoeconomics, 36(2), 175–187. https://doi.org/10.1007/s40273-017-0575-4

