
ABSTRACT
We describe the results of a pilot randomized clinical trial of a mobile phone-based intervention, InTSHA: Interactive Transition Support for Adolescents with HIV, compared to standard care. Encrypted, closed group chats delivered via WhatsApp provided peer support and improved communication between adolescents with HIV, their caregivers, and healthcare providers. We randomized 80 South African adolescents ages 15 to 19 years with perinatally-acquired HIV to receive either the intervention (n=40) or standard of care (n=40). We measured acceptability (Acceptability of Intervention Measure [AIM]) and feasibility (Feasibility of Intervention Measure [FIM]) as primary outcomes. We evaluated impact on retention in care and viral suppression six months after randomization as secondary endpoints. We performed bivariable and multivariable analyses using logistic regression models to assess the effect of the InTSHA intervention compared to standard of care. Among the adolescents randomized to the InTSHA intervention, the median AIM was 4.1/5.0 (82%) and median FIM was 3.9/5.0 (78%). We found no difference in retention in care or in viral suppression comparing intervention and control groups. Among adolescents who attended three or more sessions, retention in care was 100% at 6 months. InTSHA is an acceptable and feasible mHealth intervention warranting further study in a larger population.
Sustainable Development Goals:
Introduction
With an estimated 320,000 adolescents with perinatally-acquired HIV (APHIV), South Africa has the largest burden of APHIV in the world (HIV/AIDS, 2020). Survivors of perinatally acquired HIV are now reaching adolescence and beyond, yet adolescents are often poorly prepared for transition from pediatric to adult services (Citation2019 ART Clinical Guidelines for the Management of HIV in Adults, Pregnancy, Adolescents, Children, Infants, and Neonates, Citation2019; Zanoni et al., Citation2020). Stigma, disclosure, and growth/developmental delay can affect ALPHIV which may require interventions different from adolescents with non-perinatally-acquired HIV (Pearlstein et al., Citation2014; Sherr et al., Citation2018). In many settings, APHIV transition to adult care at variable ages and developmental stages, without necessary preparation or support through the process (Kung et al., Citation2016). Outcomes among adolescents transitioning from pediatric to adult care are often worse than those remaining in pediatric care or those initiating treatment in adult care as older adolescents (Fish et al., Citation2014; Weijsenfeld et al., Citation2016; Zanoni et al., Citation2020). In South Africa, adolescents transitioning to adult care have shown lower viral suppression rates than those remaining in the pediatric clinic (Zanoni et al., Citation2020) and less than 25% of adolescents successfully transition to adult care while remaining retained in care and virally suppressed (Zanoni, Archary, et al., Citation2021bb). Effective interventions are clearly needed to improve clinical outcomes in this highly vulnerable population, particularly in older adolescents transferring clinical care (Goldstein et al., Citation2023).
Medical care during adolescence is typically complicated by increased generalized risk-taking behavior, as well as decreased caregiver involvement, which occur during a time of rapid physical, emotional, and cognitive development (American Academy of, American Academy of Family, & American College of Physicians-American Society of Internal, Citation2002; Freed & Hudson, Citation2006; Mellins et al., Citation2006; Vreeman et al., Citation2015). When adolescents transition to adult care, they often do not receive the coordinated services that they received under pediatric care, which could help address these challenges (Vreeman et al., Citation2015). Qualitative studies with adolescents and clinicians from sub-Saharan Africa suggest that peer support, collaboration with health providers, and communication between adult and pediatric providers might assist in transition to adult services (Kung et al., Citation2016; Pettitt et al., Citation2013; Zanoni et al., Citation2019).
The use of mobile phones among adolescents in South Africa is growing rapidly and offers an excellent opportunity to deliver a social support intervention (Smailhodzic et al., Citation2016). In 2018, 95% of South Africans had access to a mobile phone (Silver et al., Citation2019). Social media interventions delivered through mobile phones have been shown to support change across several modifiable factors, such as relationships, social support, and knowledge, in other contexts. A meta-analysis found that social support was the most common reason for patients to use social media for health purposes (Smailhodzic et al., Citation2016). Social media has also been used to improve the relationship between caregivers and patients when switching caregivers, a major barrier to transition for ALHIV in South Africa (Rupert et al., Citation2014; Wicks et al., Citation2010). Although results vary in different settings, another meta-analysis showed overall improved adherence and viral suppression among adults with HIV using social media-based health services technology (Mills et al., Citation2014). Currently, there is a lack of mHealth (mobile health using digital mobile technology) interventions that that have shown improvement in outcomes for adolescents with HIV during transition to adult care globally, including low to middle income countries (LMICs) (Goldstein et al., Citation2023).
InTSHA (Interactive Transition Support for Adolescents with HIV [isiZulu for “youth”]) is an mHealth intervention developed in South Africa using participant-centered design with input from South African adolescents, caregivers, and healthcare providers. Based on the Socioecological Model for Adolescent Readiness for Transition (SMART), the Right to Care Flipster (US Agency for International Development [USAID] supported adolescent support group curriculum), and GOTTRANSITION (US Department of Health and Human Services supported transition toolkit), the intervention was delivered through facilitated discussions using closed WhatsApp Chat groups (Zanoni et al., Citation2022).
We conducted a pilot randomized clinical trial (NCT03624413) of the InTSHA intervention compared to standard of care evaluating acceptability, feasibility, and preliminary effectiveness on retention in care and viral suppression among APHIV in South Africa.
Methods
Participant selection, enrollment, and randomization
The study was conducted in KwaZulu-Natal, South Africa. APHIV between the ages of 15 and 19 years from KwaMashu Poly Clinic who had not transitioned to adult care were offered enrollment during their routine outpatient appointments in pediatric care if they were on ART for at least 6 months and were fully aware of their HIV status. Enrollment occurred between April 2021 and January 2022. Participants were randomized (1:1) to receive the InTSHA intervention delivered via WhatsApp closed chat groups vs. standard of care. Randomization was performed using sealed envelopes containing study assignments. The research team was blinded to the contents of the envelopes which were created using block randomization by a computer-generated random number sequence then filled and sealed by non-research staff.
Participant consent
All participants under the age of 18 years provided written assent to participate. Written informed consent from caregivers was obtained for adolescents less than 18 years old. Adolescents 18 years old or older provided their own written consent. Assent and/or consent forms were offered in both English and isiZulu.
InTSHA intervention
We created InTSHA using a participant-centered approach in formative interviews with South African adolescents, caregivers, and healthcare providers, as described elsewhere (Zanoni et al., Citation2022). Participants randomized to the intervention group received the InTSHA intervention consisting of 10 modules delivered weekly through closed, encrypted and password-protected WhatsApp chat groups. Modules contained topics including: 1. online security; 2. HIV disclosure; 3. drug and substance abuse; 4. sexual and reproductive health; 5. gender roles and sexuality; 6. stigma; 7. HIV knowledge and healthcare navigation; 8. ART adherence and HIV resistance; 9. healthy relationships; and 10. career planning and future goals. These closed chat groups were facilitated by a research coordinator and included standardized text messages, images, and videos discussing each topic. Password-protected, closed group chats consisted of mixed genders and up to ten APHIV. Adolescents had access to the chat group outside of scheduled sessions to check in with group members, review content of the sessions, comment, or ask additional questions. Adolescents also had the opportunity to ask health-related questions to healthcare providers at the clinic via WhatsApp through separate, private messages. All discussions were monitored by clinical doctors trained in pediatric HIV for accuracy and clarity and to troubleshoot any concerns. To ensure access to mobile data during scheduled chats, 1 gigabyte of data was loaded onto each participants phones prior to scheduled chat discussions. The ten session intervention groups were conducted between July 2021 and December 2022.
Caregivers of adolescent participants were offered participation in separate closed, encrypted, and password – protected WhatsApp chat groups with weekly topics mirroring the adolescent topics to facilitate subsequent in person discussions between adolescents and their caregivers. Adolescents and caregivers did not attend the same WhatsApp chat groups.
Standard of care
Participants in the standard of care arm continued usual care at KwaMashu Poly Clinic. Adolescents typically transition to adult care after the age of 15 if they are aware of their HIV status and taking a fixed drug combination antiretroviral therapy (ART). Viral suppression is not a criterion for transition. Newly diagnosed adolescents older than 15 years typically initiate ART in adult clinics. In the adult clinic, adolescents are seen together with adults in the general clinic that also attends to patients with other chronic illnesses. Young adults with perinatally-acquired HIV and behaviorally-acquired HIV are seen in the same clinic. Participants have a visit with a healthcare provider every 3 months and collect medication monthly at an on-site pharmacy. Viral load monitoring occurs annually after the first 6 months on ART.
Primary and secondary outcomes
As primary outcomes, we determined acceptability by the Acceptability of Implementation Measure (AIM) and feasibility by enrollment, participation, and the Feasibility of Implementation Measure (FIM) (Weiner et al., Citation2017). Both AIM and FIM are validated four question, five-point Likert-scale questionnaires with a range of 4–25. We used a threshold of 80% (median score of 4 out of 5 per question) to indicate acceptability and feasibility.
Although not powered to detect a difference in secondary outcomes, we also measured retention in care (i.e., pharmacy refill <7 days from scheduled date and no missed clinic appointments in the 6-month period after randomization) and viral suppression (i.e., viral load <200 copies/ml 6 months after randomization). We did not have resources to determine baseline or 6-month HIV resistance. To determine engagement with the intervention, we considered active participation in the intervention if participants responded to three or more text messages during each session. We also explored other factors influencing adolescent engagement in care (Zanoni, Archary, et al., Citation2021aa; Zanoni et al., Citation2019) including adolescent peer support (Child and Adolescent Social Support Scale) (Kerres Malecki & Kilpatrick Demary, Citation2002), self-esteem (Rosenberg Scale) (Rosenberg, Citation2015), depression (PHQ-9) (Kroenke et al., Citation2001), stigma (Internalized AIDS Stigma Scale) (Kalichman et al., Citation2009), connection to clinic (Working Alliance Inventory) (Horvath & Greenberg, Citation1989), and transition readiness (HIV Adolescent Readiness for Transition Scale [HARTS]) (Zanoni, Archary, Sibaya, et al., Citation2021). We performed an intention-to-treat analysis and followed the CONSORT guidelines in reporting.
Procedures
During visit one, we collected baseline demographic and health data via chart review and administered baseline questionnaires; viral load assessments were performed on all participants. Demographic and health data included age, sex at birth, age at diagnosis, history of opportunistic infections, length of time on ART, ART regimen, pre-initiation CD4, clinic visits, and pharmacy refill information. The second research visit took place during the latter of either 6 months after randomization or after completion of all 10 modules. During the second research visit, all participants completed follow-up questionnaires and had a viral load assessment. Participants randomized to the intervention arm also evaluated acceptability, feasibility, provided feedback and rationale for decreased participation of the InTSHA intervention after study exit. Additional data on vital status and location of care services was obtained through an existing patient tracker program.
Analysis
We examined the differences between the baseline characteristics of the control and InTSHA groups using independent sample t-tests and chi-square tests. Between-group changes in patient-reported outcomes were tested with independent sample t-tests. Acceptability and feasibility were determined by the median question score from the AIM and FIM measures with a threshold of 4.0/5.0 (80%) as acceptable and feasible. Active participation in the sessions was determined by responses to chats at the beginning and during the scheduled sessions. Participants who only responded after the session was complete or did not respond during the sessions were not considered active participants. We used bivariable logistic regression models to assess the effect of the InTSHA intervention compared to standard of care on retention in care and viral suppression, including the following potential covariates: age at ART initiation, sex assigned at birth (all participants were cis gendered), school attendance, drug use, alcohol use, social support, self-esteem, connection to clinical staff, and transition readiness. We then performed a multivariable analysis using multivariable logistic regression with Huber-White robust standard errors and covariates with a p-value of <0.2 on bivariate analysis. In the multivariable regression, we also assessed for interaction terms among the covariates and retained any interaction terms whose p-value was <0.05. In the multivariable analysis, we also evaluated attendance in the number of InTSHA sessions to estimate the dose response. Statistical analyses were performed with IBM SPSS Statistics (Version 29.0.0.0).
Ethics statement
Biomedical Research Ethics Counsel of the University of KwaZulu-Natal, KwaZulu-Natal Department of Health, Partners Healthcare/MassGeneral Brigham Research Ethics Board, and the Emory University Institutional Review Board approved this protocol.
Results
We screened 85 adolescents to participate in the study with 80 (94%) who agreed to enroll as indicated in . Eighty adolescents with HIV in South Africa were randomized to receive the InTSHA intervention (n = 40) or continue standard of care (n = 40). Baseline characteristics are shown in . At baseline, all participants were considered retained in care and 80% were virally suppressed to <200 copies/ml. All participants transitioned to adult care during the study period.
Figure 1. InTSHA Consort Diagram.
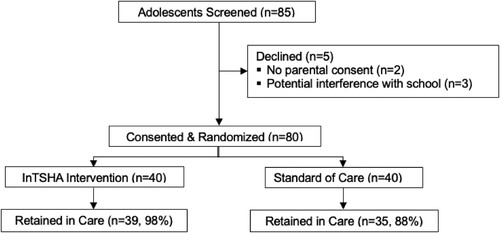
Table 1. Baseline characteristics of adolescents living with HIV in South Africa randomized to receive InTSHA intervention or standard of care.
Acceptability / feasibility
For participants randomized to the InTSHA intervention, the median acceptability score was 4.1/5.0 (82%) based on the AIM questionnaire, and feasibility was 3.9/5.0 (78%) based on the FIM. Attendance and participation in the intervention was variable. Of the adolescents randomized to the InTSHA intervention, 15 (38%) participants attended and were active contributing participants in 8–10 sessions; 9 participated in 5–7 (23%) sessions; 15 participants (38%) attended fewer than 5 sessions including 2 (5%) who only participated in the introductory session. Reasons for decreased participation included an inability to attend at the scheduled time of the chat, power outages or poor internet connection, an inability to use a shared phone during the scheduled chat, lost or stolen phone, timing of chats overlapped with school or extracurricular activities.
Preliminary effectiveness
We calculated preliminary effectiveness of the InTSHA intervention on retention in care and viral suppression six months after randomization. We found no statistical difference in retention in care among participants randomized to the InTSHA intervention compared to the control group (n = 39 [98%] vs n = 35 [88%]; OR 5.6 [95%CI 0.6–50.0; p = 0.20]), . Among adolescents attending 3 or more InTSHA sessions (n = 30 [75%]) retention in care was 100%. Retention in care increased by 60% for each session attended. There was no statistical difference in viral suppression among adolescents randomized to the InTSHA intervention compared to the control [n = 29 [73%] vs n = 33 [83%]; OR 0.6 (95%CI 0.2–1.6; p = 0.42)], . Among adolescents attending 3 or more InTSHA sessions viral suppression was 83% (n = 25).
Table 2. Chi-square tests comparing the retention and viral suppression between the control and InTSHA groups six months after randomization.
Exploratory outcomes
No significant differences were seen in peer support, depression, self-esteem, drug or alcohol use, school attendance, connection to clinical staff, stigma, or transition readiness in the InTSHA group compared to standard of care as indicated in . In bivariate logistic regression, there were no significant associations with retention in care, while younger age (OR 0.6, 95% CI 0.4–0.98; p = 0.04), baseline viral suppression (OR 11.7, 95% CI 3.3–40.9; p < 0.001), and not missing school (OR 0.7, 95% CI 0.4–0.97; p = 0.04) were associated with viral suppression as indicated in . In multivariable logistic regression, we found no significant associations with retention in care, while baseline viral suppression was associated with six-month viral suppression (aOR 9.1, 95% CI 2.4–34.2; p = 0.001), .
Table 3. Independent sample t-tests comparing the changes in patient-reported outcomes between the control and InTSHA groups.
Table 4. Univariate logistic regression of retention-in-care and viral suppression status at Month 6.
Table 5. Multivariate logistic regression of retention-in-care and viral suppression status at Month 6.
Discussion
Interest in the InTSHA intervention was evident by the high (94%) enrollment rate. Participants in the InTSHA group also reported a high degree of acceptability (82%). Although the InTSHA intervention was highly acceptable to adolescents in the study, full participation in the intervention was lower than anticipated. The median feasibility score of 78% fell below our threshold of 80%. Of the adolescents randomized to the InTSHA intervention, active participation (where participant sent and responded to messages during the scheduled session) in at least 50% of the sessions was only 60%. Despite high levels of interest and acceptability of the intervention, technical difficulties including power outages, poor internet connection, and use of shared phones contributed to decreased participation in the intervention. Our study provided sufficient cellular data to participate in scheduled group chats; however, socioeconomic pressure from costs of mobile phones and data plans outside of the research environment can be prohibitive for younger adolescents, particularly in LMICs, to consistently engage in mHealth interventions. The practice of sharing phones can reduce associated costs, but privacy, confidentiality, and regular access may be compromised (Akinfaderin-Agarau et al., Citation2012). We were able to use password protected chats within WhatsApp to overcome these barriers, which favors continued exploration of mHealth interventions. Participation in InTSHA among adolescents and caregivers also varied due to difficulty scheduling chat times that worked for all participants in an assigned closed group. Busy schedules and competing interests with extracurricular activities limited availability of participants to all participate at the same time. It is possible that the use of chatbots or artificial intelligence (AI) could mitigate scheduling conflicts but may reduce the benefits of direct peer interactions. These findings highlight the real-world challenges associated with evaluating applicability of mHealth interventions in different settings. Despite these logistical barriers, in this small pilot, InTSHA still showed potential effectiveness in improving retention in care. Larger studies evaluating the real-world uptake, effectiveness, and cost of mHealth interventions are required if they are going to be utilized and sustained for meaningful impact (Feroz et al., Citation2021).
In participants randomized to the InTSHA intervention, retention in care was 10% higher compared participants randomized to standard of care although this difference was not statistically significant. Retention in care appeared to increase with increased participation in the InTSHA intervention with a 60% increase in retention in care for each session attended and 100% retention with 3 or more sessions attended. This is one of the first mHealth interventions showing potentially positive outcomes among ALHIV who are transitioning to adult care (Goldstein et al., Citation2023). Historically, APHIV have poor retention in care and viral suppression during transitioning from pediatric to adult care; (Zanoni et al., Citation2020; Zanoni et al., Citation2017) however, retention in care in the InTSHA intervention group was 98% with viral suppression rate of 73%. Despite the uptake of social media and mHealth interventions addressing gaps in HIV continuum of care in LMICs, no prior interventions addressed transition to adult care (Goldstein et al., Citation2023). The InTSHA intervention incorporates easy to use existing technology that fills this gap.
To our knowledge, only one other ongoing study is using mHealth to support transition from pediatric to adult care for adolescents and young adults with HIV. Specifically, Hussen, et al. are evaluating a novel smart-phone app, iTransition, based on Social Cognitive Theory to support ALHIV in the United States (Tanner et al., Citation2021). Our study adds to the literature given that development, evaluation, and implementation of effective and accessible mHealth interventions are needed to improve healthcare transition outcomes for adolescents living with perinatally-acquired HIV in LMICs where most youth with perinatally-acquired HIV reside. Differences in internet and mobile phone use and access in LMICs may complicate the feasibility of mHealth interventions on large scales; moreover, desired features and acceptability may be influenced by different cultures and settings.
Mobile phone ownership by adolescents and participation in mHealth interventions have increased in recent years, especially in LMICs. (Smailhodzic et al., Citation2016) mHealth is a particularly promising strategy for interventions targeting adolescents who are often avid adopters of technology. Although mHealth technology can address several of the modifiable barriers to transition care highlighted by the Socioecological Model for Adolescent Readiness for Transition (SMART), other practical barriers remain. Structural barriers including power outages, limited internet access, and expense of data may limit the feasibility of mHealth interventions in certain areas. Few mHealth interventions have shown efficacy in health-related outcomes while continuing to engage adolescents in LMIC highlighting the challenge of affecting behavioral change among adolescents (Goldstein et al., Citation2023).
Our study also found improved viral suppression for younger adolescents and those who missed less school. Prior studies have found that reducing school absenteeism can affect retention in care among adolescents with HIV (Zanoni et al., Citation2019, Citation2017). Adolescent-friendly services often include expanded weekend or after-school options which can improve engagement in care (Zanoni et al., Citation2017, Citation2019). Future interventions should focus on initiatives to limit interference with school and improve school attendance which could affect important clinical outcomes.
Although the InTSHA intervention was designed to improve retention in care and viral suppression through mediation of peer and parental support, connection to clinical staff, self-esteem, and transition readiness, we found no difference in the intervention and standard of care in any of these parameters. However, this pilot study was powered on acceptability and feasibility and not retention in care, viral suppression, or exploratory outcomes. A qualitative analysis exploring these issues based on in-depth exit interviews will be published separately.
This study has several limitations. We found no difference in viral suppression six months after randomization in the intervention or standard of care groups. In this pilot study, we did not assess for HIV resistance at baseline and did not directly measure adherence to ART. An ongoing study is evaluating long-term outcomes at 12 months after randomization and is evaluating HIV resistance and ART adherence through tenofovir diphosphate levels.
Conclusion
InTSHA is a promising mHealth intervention using closed WhatsApp chat groups with adolescents, caregivers, and healthcare providers that may improve retention in care for adolescents living with HIV during transition from pediatric to adult care. Future studies should focus on addressing structural barriers to mHealth interventions in LMICs and methods of improving sustained engagement of adolescents. In addition, larger, adequately powered studies in different settings will be required to evaluate the effectiveness and mechanisms of effect for this intervention.
Author’s contributions
Dr. Zanoni conceptualized and designed the study, performed the literature review, assisted with the analysis, drafted the initial manuscript, reviewed, and revised the manuscript and approved the final manuscript as submitted. Ms. Sibaya coordinated the intervention, performed the data collection, contributed to the drafting of the manuscript, critically reviewed the manuscript, and approved the final manuscript as submitted. Mr. Musinguzi conducted the data analysis, critically reviewed the manuscript, and approved the final manuscript as submitted. Mr. Gethers conducted the data analysis, critically reviewed the manuscript, and approved the final manuscript as submitted. Dr. Archary assisted with the conceptualization and design of the study, contributed to the data collection, and critically reviewed the manuscript, and approved the final manuscript as submitted. Dr. Goldstein assisted analysis of formative work, assisted in the creation of the intervention, critically reviewed the manuscript, and approved the final manuscript as written. Ms. Bergam assisted analysis of formative work, assisted in the creation of the intervention, critically reviewed the manuscript, and approved the final manuscript as written. Dr. Psaros assisted with the conceptualization and design of the study, assisted in the analysis of formative work, contributed to the data collection, and critically reviewed the manuscript, and approved the final manuscript as submitted. Dr. Marconi assisted with the conceptualization and design of the study, contributed to the analysis plan, reviewed and revised the manuscript, and approved the final manuscript as submitted. Dr. Haberer assisted with the conceptualization and design of the study, contributed to the analysis plan, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Disclosure statement
JEH reports consulting for Merck and owns stock in Natera. VCM has received investigator-initiated research grants (to the institution) and consultation fees (both unrelated to the current work) from Eli Lilly, Bayer, Gilead Sciences and ViiV. BCZ has received consultation fees from Accordant a division of CVS. All other authors have no conflicts of interest relevant to this article to disclose.
Data availability statement
The data that support the findings of this study are available from the corresponding author, BZ, upon reasonable request.
Additional information
Funding
References
- Akinfaderin-Agarau, F., Chirtau, M., Ekponimo, S., & Power, S. (2012). Opportunities and limitations for using new media and mobile phones to expand access to sexual and reproductive health information and services for adolescent girls and young women in six Nigerian states. African Journal of Reproductive Health, 16(2), 219–230. https://www.ncbi.nlm.nih.gov/pubmed/22916554.
- American Academy of Pediatrics., American Academy of Family Physicians., & American College of Physicians-American Society of Internal Medicine. (2002). A consensus statement on health care transitions for young adults with special health care needs. Pediatrics, 110(6 Pt 2), 1304–1306. http://www.ncbi.nlm.nih.gov/pubmed/12456949.
- Feroz, A. S., Ali, N. A., Khoja, A., Asad, A., & Saleem, S. (2021). Using mobile phones to improve young people sexual and reproductive health in low and middle-income countries: A systematic review to identify barriers, facilitators, and range of mHealth solutions. Reproductive Health, 18(1), 9. https://doi.org/10.1186/s12978-020-01059-7
- Fish, R., Judd, A., Jungmann, E., O'Leary, C., & Foster, C. (2014). Mortality in perinatally HIV-infected young people in England following transition to adult care: An HIV Young Persons Network (HYPNet) audit. HIV Medicine, 15(4), 239–244. https://doi.org/10.1111/hiv.12091
- Freed, G. L., & Hudson, E. J. (2006). Transitioning children with chronic diseases to adult care: Current knowledge, practices, and directions. The Journal of Pediatrics, 148(6), 824–827. https://doi.org/10.1016/j.jpeds.2006.02.010
- Goldstein, M., Archary, M., Adong, J., Haberer, J. E., Kuhns, L. M., Kurth, A., Ronen, K, Lightfoot, M, Inwani, I, John-Stewart, G, Garafalo, R, & Zanoni, B. C. (2023). Systematic review of mHealth interventions for adolescent and young adult HIV prevention and the adolescent HIV continuum of care in low to middle income countries. AIDS and Behavior, 27(Suppl 1), 94–115. https://doi.org/10.1007/s10461-022-03840-0
- Horvath, A. O., & Greenberg, L. S. (1989). Development and validation of the working alliance inventory. Journal of Counseling Psychology, 36(2), 223. https://doi.org/10.1037/0022-0167.36.2.223
- Kalichman, S. C., Simbayi, L. C., Cloete, A., Mthembu, P. P., Mkhonta, R. N., & Ginindza, T. (2009). Measuring AIDS stigmas in people living with HIV/AIDS: The Internalized AIDS-Related Stigma Scale. AIDS Care, 21(1), 87–93. https://doi.org/10.1080/09540120802032627
- Kerres Malecki, C., & Kilpatrick Demary, M. (2002). Measuring perceived social support: Development of the child and adolescent social support scale (CASSS). Psychology in the Schools, 39(1), 1–18. https://doi.org/10.1002/pits.10004
- Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
- Kung, T. H., Wallace, M. L., Snyder, K. L., Robson, V. K., Mabud, T. S., Kalombo, C. D., & Bekker, L. G. (2016). South African healthcare provider perspectives on transitioning adolescents into adult HIV care. South African Medical Journal, 106(8), 804–808. https://doi.org/10.7196/SAMJ.2016.v106i8.10496
- Mellins, C. A., Brackis-Cott, E., Dolezal, C., & Abrams, E. J. (2006). Psychiatric disorders in youth with perinatally acquired human immunodeficiency virus infection. Pediatric Infectious Disease Journal, 25(5), 432–437. https://doi.org/10.1097/01.inf.0000217372.10385.2a
- Mills, E. J., Lester, R., Thorlund, K., Lorenzi, M., Muldoon, K., Kanters, S., Linnemayer, S., Gross, R., Calderon, Y., Amico, K. R., Thirumurthy, H., Pearson, C., Remien, R. H., Mbuagbaw, L., Thabane, L., Chung, M. H., Wilson, I. B., Liu, A., Uthman, O. A.…Nachega, J. (2014). Interventions to promote adherence to antiretroviral therapy in Africa: A network meta-analysis. The Lancet HIV, 1(3), e104–e111. https://doi.org/10.1016/S2352-3018(14)00003-4
- Pearlstein, S. L., Mellins, C. A., Dolezal, C., Elkington, K. S., Santamaria, E. K., Leu, C. S., Cruz, J. E., & Abrams, E. J. (2014). Youth in transition: life skills among perinatally HIV-infected and HIV-exposed adolescents. Journal of Pediatric Psychology, 39(3), 294–305. https://doi.org/10.1093/jpepsy/jst077
- Pettitt, E. D., Greifinger, R. C., Phelps, B. R., & Bowsky, S. J. (2013). Improving health services for adolescents living with HIV in sub-Saharan Africa: A multi-country assessment. African Journal of Reproductive Health, 17(4 Spec No), 17–31.
- Rosenberg, M. (2015). Society and the adolescent self-image. Princeton University Press.
- Rupert, D. J., Moultrie, R. R., Read, J. G., Amoozegar, J. B., Bornkessel, A. S., O'Donoghue, A. C., & Sullivan, H. W. (2014). Perceived healthcare provider reactions to patient and caregiver use of online health communities. Patient Education and Counseling, 96(3), 320–326. https://doi.org/10.1016/j.pec.2014.05.015
- Sherr, L., Cluver, L. D., Toska, E., & He, E. (2018). Differing psychological vulnerabilities among behaviourally and perinatally HIV infected adolescents in South Africa - Implications for targeted health service provision. AIDS Care, 30(sup2), 92–101. https://doi.org/10.1080/09540121.2018.1476664
- Silver, L. V., EA; Mordecai, M;, Cha, J., ; Rasmussen, R., & ; Rainie, L. (2019). Mobile divides in emerging economies. Pew Research Center. https://www.pewresearch.org/internet/2019/11/20/mobile-divides-in-emerging-economies/.
- Smailhodzic, E., Hooijsma, W., Boonstra, A., & Langley, D. J. (2016). Social media use in healthcare: A systematic review of effects on patients and on their relationship with healthcare professionals. BMC Health Services Research, 16(1), 442. https://doi.org/10.1186/s12913-016-1691-0
- South African National Department of Health. (2019). 2019 ART Clinical Guidelines for the Management of HIV in Adults, Pregnancy, Adolescents, Children, Infants, and Neonates. South African National Department of Heath.
- Tanner, A. E., Dowshen, N., Philbin, M. M., Rulison, K. L., Camacho-Gonzalez, A., Lee, S., Moore, S., Fortenberry, J. D., & Hussen, S. A. (2021). An intervention for the transition from pediatric or adolescent to adult-oriented HIV care: Protocol for the development and pilot implementation of iTransition. JMIR Research Protocols, 10(4), e24565. https://doi.org/10.2196/24565
- Vreeman, R. C., Scanlon, M. L., McHenry, M. S., & Nyandiko, W. M. (2015). The physical and psychological effects of HIV infection and its treatment on perinatally HIV-infected children. Journal of the International AIDS Society, 18(Suppl 6), 20258. https://doi.org/10.7448/IAS.18.7.20258
- Weijsenfeld, A. M., Smit, C., Cohen, S., Wit, F. W., Mutschelknauss, M., van der Knaap, L. C., & Young Adults Study Group. (2016). Virological and social outcomes of HIV-infected adolescents and young adults in The Netherlands before and after transition to adult care. Clinical Infectious Diseases: an Official Publication of the Infectious Diseases Society of America, 63(8), 1105–1112. https://doi.org/10.1093/cid/ciw487
- Weiner, B. J., Lewis, C. C., Stanick, C., Powell, B. J., Dorsey, C. N., Clary, A. S., Boynton, M. H., & Halko, H. (2017). Psychometric assessment of three newly developed implementation outcome measures. Implementation Science, 12(1), 108. https://doi.org/10.1186/s13012-017-0635-3
- Wicks, P., Massagli, M., Frost, J., Brownstein, C., Okun, S., Vaughan, T., Bradley, R., & Heywood, J. (2010). Sharing health data for better outcomes on PatientsLikeMe. Journal of Medical Internet Research, 12(2), e19. https://doi.org/10.2196/jmir.1549
- Zanoni, B. C., Archary, M., Sibaya, T., Goldstein, M., Bergam, S., Denton, D., Cordero, V., Peng, C., Psaros, C., Marconi, V. C., & Haberer, J. E. (2022). Mobile phone-based intervention among adolescents living with perinatally acquired HIV transitioning from pediatric to adult care: Protocol for the interactive transition support for adolescents living with HIV using social media (InTSHA) study. JMIR Research Protocols, 11(1), e35455. https://doi.org/10.2196/35455
- Zanoni, B. C., Archary, M., Sibaya, T., Musinguzi, N., & Haberer, J. E. (2020). Transition from pediatric to adult care for adolescents living with HIV in South Africa: A natural experiment and survival analysis. PLoS One, 15(10), e0240918. https://doi.org/10.1371/journal.pone.0240918
- Zanoni, B. C., Archary, M., Sibaya, T., Musinguzi, N., Kelley, M. E., McManus, S., & Haberer, J. E. (2021). Development and validation of the HIV adolescent readiness for transition scale (HARTS) in South Africa. Journal of the International AIDS Society, 24(7), e25767. https://doi.org/10.1002/jia2.25767
- Zanoni, B. C., Archary, M., Subramony, T., Sibaya, T., Psaros, C., & Haberer, J. E. (2021a). Disclosure, social support, and mental health are modifiable factors affecting engagement in care of perinatally-HIV infected adolescents: A qualitative dyadic analysis. AIDS and Behavior, 25(1), 237–248. https://doi.org/10.1007/s10461-020-02968-1
- Zanoni, B. C., Archary, M., Subramony, T., Sibaya, T., Psaros, C., & Haberer, J. E. (2021b). ‘It was not okay because you leave your friends behind’: A prospective analysis of transition to adult care for adolescents living with perinatally-acquired HIV in South Africa. Vulnerable Children and Youth Studies, 16(3), 206–220. https://doi.org/10.1080/17450128.2021.1876965
- Zanoni, B. C., Sibaya, T., Cairns, C., & Haberer, J. E. (2019). Barriers to retention in care are overcome by adolescent-friendly services for adolescents living with HIV in South Africa: A qualitative analysis. AIDS and Behavior, 23(4), 957–965. https://doi.org/10.1007/s10461-018-2352-6
- Zanoni, B. C., Sibaya, T., Cairns, C., Lammert, S., & Haberer, J. E. (2017). Higher retention and viral suppression with adolescent-focused HIV clinic in South Africa. PLoS One, 12(12), e0190260. https://doi.org/10.1371/journal.pone.0190260