
Abstract
Migration, displacement, and flight are major worldwide phenomena and typically pose challenges to mental health. Therefore, migrants’ mental health, and the factors which may predict it, have become an important research subject. The present population-based cross-national comparison study explores symptoms of depression, anxiety, and somatization, as well as quality-of-life in samples of ex-Soviet Jewish migrants settling in three new countries: Germany, Austria and Israel, as well as in a sample of non-migrant ex-Soviet Jews in their country of origin, Russia. In the current study, we investigate the relationship of perceived xenophobiа and antisemitism, acculturation attitudes, ethnic and national identity, as well as affiliation with Jewish religion and culture to the psychological well-being of these migrants. Furthermore, we consider xenophobic and antisemitic attitudes as well as the acculturation orientation of the new countries’ societies, assessed in the native control samples. Our data suggest that attitudes of the new country’s society matter for the mental health of this migrant group. We conclude that the level of distress among ex-Soviet Jewish migrants seems to depend, among other factors, on the characteristics of the new country and/or specific interactions of the migrant population with the society they are settling in.
Introduction
Being a major social phenomenon, migration has become an important field of research in the last decades. According to UN statistics 281 million people worldwide live abroad and this number is rising (McAuliffe & Triandafyllidou, Citation2021). Of these international migrants, Jews from the former Soviet Union (FSU), the migrant population under study in the present paper, constitute around 2 million people (Tolts, Citation2016). About 90% of ex-Soviet Jews left their country of origin behind between 1970 and 2010, mostly because of antisemitism or the prospect of economic improvement. They settled in several countries, mostly in Israel, North America, and Western Europe. A detailed description of this population can be found in Trilesnik et al. (Citation2022).
The process of migration poses many challenges to mental health. Moreover, post-migration stressors such as language barriers, bureaucratic hurdles, e.g. regarding resident status, socio-economic hardships, and difficulties in finding adequate jobs, as well as cultural adaptation and lack of a social network are likely to negatively impact upon acculturation and settling down. The psychological consequences of migration have, therefore, received increasing scientific attention. Researchers agree that the current data are partially inconclusive and that some important aspects are not sufficiently covered (Miller & Gross, Citation2004; Mirsky, Citation2009).
For instance, the current body of literature provides controversial findings on whether or not migration leads to impaired mental health. According to some studies, mostly from Israel and Germany, migrants suffer from higher rates of mental disorders and specifically display elevated prevalence rates for depression, anxiety, and schizophrenia compared to the majority population in the newFootnote1 country (Bermejo et al., Citation2010; Lindert et al., Citation2009; Mirsky et al., Citation2008; Selten et al., Citation2020). These findings support the ‘migration–morbidity hypothesis’, which proposes that migration leads to psychological distress (Mirsky, Citation2009). Other studies, however, mostly from the United States but also from Europe, find a lower prevalence of mental disorders in migrants (Carta et al., Citation2005; Dhadda & Greene, Citation2017; Glaesmer et al., Citation2009) and conclude an ‘absence of a generalized psychopathological risk among emigrants’ (Carta et al., Citation2006, p. 452). These studies are in line with the ‘healthy-immigrant hypothesis’, referring to a health advantage of foreign-born individuals (Vang et al., Citation2017).
Besides methodological differences these divergent findings are commonly regarded as resulting from characteristics of the migrant ethnicity or country of origin, e.g. its level of development (de Wit et al., Citation2008; Stompe et al., Citation2009). For example, Latino migrants have been shown to be the ‘healthy’ migrants (Alegria et al., Citation2008; Alegría et al., Citation2017), whereas Turkish, Moroccan, or Polish are the rather ‘morbid’ ones in most studies (Morawa & Erim, Citation2015). Jewish migrants from the FSU are also found to display higher levels of psychological distress and elevated prevalence rates of depressive, anxiety, and psychosomatic symptoms when compared to natives in the respective new countries (Aroian & Norris, Citation2003; Mirsky et al., Citation2008; Trilesnik et al., Citation2018; Ullmann et al., Citation2013).
Additionally, immigration policies and other variables of the new countries could be contributing factors to these reported differences. Some research suggests that selective immigration policies could lead to ‘healthier’ migrants whereas non-selective policies to more ‘morbid’ ones, explaining the better mental health of migrants in the United States (Mirsky et al., Citation2008). Other studies conclude that a legal resident status is associated with lower mental health burden (Laban et al., Citation2004). Nevertheless, the impact of a given new country on the mental health of migrants has so far barely been researched. Carta et al. (Citation2006) report a higher prevalence rate of depressive disorders among Sardinian migrants in Argentina than in France and in non-migrant Sardinians, which they attribute to worse economic conditions in Argentina. An association between higher GNP per capita of the new country and a lower prevalence rate of depression and anxiety in migrants was also discussed in a study by Lindert et al. (Citation2009). On the other hand, no significant differences were observed in the mental health of Latino migrants in Spain and the United States (Fortuna et al., Citation2016). Cross-country studies with Jewish migrants from the FSU have so far focused on particular aspects of mental health, such as demoralization in Israel and the United States (Flaherty et al., Citation1988), depression in women in these two countries (Miller & Gross, Citation2004), and health-related quality-of-life in Israel and Germany (Nesterko et al., Citation2018), all authors finding reduced symptomatic burden in Israel compared to the other countries.
Besides group-level factors there are also individual-level factors associated with the mental health of migrants. Such associations were shown, e.g. for income (Toselli et al., Citation2014), experience of discrimination (Straiton et al., Citation2019), attitude to acculturation (Balidemaj & Small, Citation2019; Berry et al., Citation1987), cultural identity (Beiser & Hou, Citation2017; Burnett-Zeigler et al., Citation2013), and religiosity (Bonelli & Koenig, Citation2013). These factors were also shown to be relevant for Jewish migrants from the FSU in Trilesnik et al. (Citation2018).
In the present paper we report on the mental health of ex-Soviet Jewish migrants, looking at depressive symptoms, anxiety, somatization, and quality-of-life in Austria, Germany, and Israel. These countries pursue different immigration policies and display different attitudes towards foreigners, allowing us to investigate a possible new country effect in a comparative cross-sectional design.
Objectives
The present study aims to address the following four questions: First, do ex-Soviet Jewish migrants display a higher mental health burden than the respective native population of the new country? Second, are there differences in the mental health burden of these migrants depending on the new country? Third, does the mental health burden of migrants differ from the mental health burden of Jews in Russia? And, finally, are the factors of acculturation, cultural identity, affiliation to Jewish religion, perceived antisemitism, and discrimination positively or negatively associated with the mental health burden in this migrant group, and is there an additional effect of the new country?
Methods
Study design
The present population-based study explores mental health and post-migration factors in Jewish migrants from the FSU in Germany, Austria, and Israel. We introduce a novel study design by combining two migration research paradigms: (a) comparing a single migrant population to the population in its country of origin as well as to the new country’s population and (b) studying the same migrant population in several countries with different migration conditions. Our study design is illustrated in . First, we compare ex-Soviet Jews in Russia, Germany, Austria, and Israel to the respective majority populations and second we compare these ex-Soviet Jewish subsamples to each other.
Figure 1. Study design: Cross-national comparison of a migrant group to new country’s population and population of the country of origin.
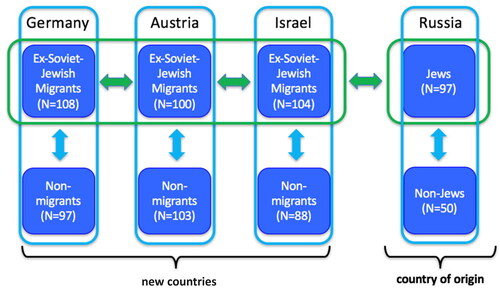
Sample
As displayed in , the overall study sample comprises eight subsamples with a total sample size of 747 participants. The migrant subsamples consist of first-generation Jewish migrants from the FSU residing in Austria, Germany, and Israel. The control groups consist of non-Jewish natives without migration backgrounds in these three countries. Russian-born Jews and non-Jewish Russians without migration backgrounds were recruited for the subsamples in Russia. Here, we adopt the definition of the Law of Return of Israel which regards one Jewish grandparent to be a necessary and sufficient condition to be considered Jewish. Lack of migration background is defined as having no foreign-born parents or grandparents, except for the case of Israel where it is defined as being born in Israel.
The data were collected by the first author between 2014 and 2017 in Vienna, Berlin, Tel Aviv, and St. Petersburg using purposive sampling due to the non-applicability of random sampling in this case and its general disadvantages in migrant populations. The control and migrant subsamples were matched by age and gender. The study participants gave their written consent for an anonymized data analysis. The study was approved by the Ethics Committee of Hannover Medical School, Germany. A more detailed description of the sample and data collection process can be found in Trilesnik et al. (Citation2022).
Measures
We collected the data using self-report questionnaires consisting of standardized and internationally well-established instruments. The migrant and the control group questionnaires were available in Russian, German, and Hebrew, as a paper-and-pencil and online version. Most of the chosen scales had pre-existing validated adaptations in the respective languages, others were translated and verified through back-translation. A pilot run established the psychometric properties of the scales’ adaptations (e.g. internal consistency above 0.7) and validated their cross-cultural equivalence.
Mental health
Mental health was assessed in terms of depressive symptoms, anxiety, somatization, and quality-of-life using the following instruments: the Beck Depression Inventory (BDI-II), the State-Trait-Anxiety-Inventory (STAI), the Brief Symptom Inventory (BSI), and the WHO Quality-of-Life Questionnaire (WHOQoL-BREF). BDI-II measures the presence and severity of depressive symptoms using 21 multiple-choice items coded from 0 to 3. A total score of 13 or greater indicates clinical depression. To assess anxiety, we used the trait subscale of STAI which contains 20 items rated on a four-point Likert-scale (1 = ‘almost never’ to 4 = ‘almost always’). Pathological anxiety is indicated by total scores above 44 (Chanin, Citation2002). Additionally, we measured depressive symptoms and anxiety as well as somatization with the respective BSI subscales, rated on a response scale from 0 to 4 (0 = ‘not at all’ to 4 = ‘extremely’). WHOQoL-BREF is a quality-of-life scale comprising 26 items quantified from 1 to 5.
Post-migration factors
Apart from mental health parameters we assessed post-migration factors such as perceived xenophobiа and antisemitism, acculturation attitudes, ethnic and national identity, as well as affiliation with the Jewish religion and culture in the migrant subsamples. To measure perceived xenophobic and antisemitic discrimination in everyday life we used a 6-item scale based on the Perceived Discrimination Scale (PDS) by Finch et al. (Citation2000), rated from 1 = ‘never’ to 4 = ‘always’ (e.g. ‘How often do people dislike you because you are a foreigner?’, ‘How often do people dislike you because you are Jewish?’). We used the Vancouver Index of Acculturation (VIA) to measure bonds to the culture of origin and interest in the new society (Ryder et al., Citation2000). Each of these two subscales contains 10 items rated on a 5-point Likert scale (e.g. ‘I often participate in [the culture in question] cultural traditions’). The categorization of the subscales’ values into ‘high’ and ‘low’ allows mapping them to the four acculturation strategies (integration, assimilation, separation, and marginalization) proposed by Berry et al. (Citation1989). Ethnic and national identity, i.e. Jewish, ex-Soviet, and the new country’s identity, were quantified by asking ‘How much do you identify with the [identity in question]?’ using visual analogue scale responses with endpoints ‘not at all’ and ‘very strongly’. Additionally, we included a question regarding cultural self-labelling (‘As what do you see yourself?’). Affiliation with Jewish religion and culture was measured using an adapted version of the Cultural and Religious American Jewish Identity Scale (C&R-AJIS) which consists of 18 religious identification items (e.g. ‘I observe the Sabbath’) and 15 cultural identification items (e.g. ‘I enjoy Jewish literature’), each rated on a 5-point Likert scale (Friedlander et al., Citation2010).
Factors of the new society
Furthermore, we considered xenophobic and antisemitic attitudes as well as the acculturation orientation of the new society. We measured xenophobic attitudes in the German, Austrian, and Israeli control subsamples using the 10-item scale (e.g. ‘foreigners exploit the social welfare system’) by Manzoni (Citation2007). Antisemitic attitudes were assessed only in the German and Austrian subsamples using a 10-item scale (e.g. ‘Jews have too much influence in [the country in question]’) from Zick et al. (Citation2011). Both scales are rated from 1 (‘strongly disagree’) to 4 (‘strongly agree’). For measuring the acculturation orientation of the new society we used the dominant group version of the 20-item Immigrant Acculturation Scale (IAS) by Berry et al. (Citation2006), which is rated on a 5-point Likert scale (e.g. ‘Migrants should have both ethnic and [national] friends’, 1 = ‘strongly disagree’ to 5 = ‘strongly agree').
Socio-demographics
Socio-demographic measures included age, gender, marital status, level of education, income, religious affiliation, and use of mental health services. Additionally, migration-specific questions about duration of residence, reasons for migration, resident status, and experience of multiple migrations were asked.
Statistical analysis
All analyses were performed using IBM SPSS Statistics 29. We first ran preliminary analyses to confirm scale reliability. Second, we described each variable in terms of its mean and standard deviation or frequency distribution. Third, we performed one-way ANOVA tests and chi-square tests to compare the subsamples as well as a Bonferroni post-hoc test to correct the significance level. Fourth, we analysed the differences in mental health between the subsamples using MANOVA, controlling for some socio-demographic confounders and applying a Bonferroni correction. Finally, to investigate the association between post-migration factors and mental health we conducted linear multiple regression analyses, including two country dummy variables to capture the new country factors.
Results
We found good internal consistency for the applied measures, confirming their reliability (Cronbach’s alpha between 0.80 and 0.97) except for IAS (Cronbach’s alpha between 0.49 and 0.76). A statistical description of the subsamples regarding socio-demographic variables is shown in , including a within-country analysis of migrant and control subsamples. A between-country analysis of the ex-Soviet Jewish subsamples in the three new countries and the country of origin regarding sociodemographic and post-migration factors is displayed in . In the following, our reported findings refer to , or both.
Table 1. Within-country analysis between migrants and controls regarding sociodemographic characteristics (one-way ANOVA/χ2-tests).
Table 2. Between-country analysis of Jewish migrants and Jews in Russia regarding sociodemographic characteristics and post-migration factors (one-way ANOVA/χ2-tests).
The mean age of our study participants does not vary significantly between the subsamples, ranging from 38 to 41 years. The gender distribution is even in all subsamples except for the control group in Israel which has significantly more female participants. Remarkably, the rate of university degrees is high in the overall sample, reflecting a high level of education in this migrant population. However, there are some significant differences in education and income levels between the subsamples. In the within-country analysis we found that migrants in Israel are significantly more educated and migrants in Austria have significantly lower incomes than their respective controls. Additionally, in the between-country analysis migrants in Austria reported significantly fewer university degrees and less income than those in Germany and Israel. Notably, the migrant subsamples do not differ in duration of residence (on average 17 years) and reasons for migration (over 80% report so-called pull factors, e.g. prospect of economic improvement).
However, the post-migration factors vary significantly between the migrant subsamples. Bonds to home culture are similarly strong in all migrant subsamples, while interest in the new culture is significantly stronger in Israel and Germany than in Austria. Correspondingly, whereas for ex-Soviet Jews in Germany and Israel integration is the most common acculturation strategy (over 59%), separation is the most frequent strategy in Austria, with only 41% adopting integration. Similarly, there is no difference in ex-Soviet identity levels between the subsamples, yet in the Austrian and German migrant subsamples Jewish identity is stronger and identity of the new country weaker than in the Israeli one. The Austrian migrant subsample displays the strongest affiliation to Jewish religion and culture, whereas the Israeli one displays the weakest. Furthermore, ex-Soviet Jews face less xenophobic discrimination in Israel than in Austria and Germany, where the frequency of xenophobic and antisemitic experiences is similar.
Regarding the first research question, whether the mental health burden in ex-Soviet Jewish migrants is higher as compared to the respective population of the new country, the four within-country MANOVA analyses demonstrate significant mental health differences between the subsamples (). The analyses were performed controlling for income and education levels as main differing sociodemographic factors. Ex-Soviet Jews in Austria are significantly more depressed and anxious and report less quality-of-life than the Austrian control group (BDI: F = 10.545, p < 0.001; STAI: F = 27.147, p < 0.001; BSI-A: F = 5.456, p < 0.05; QoL: F = 20.364, p < 0.001). In Germany, ex-Soviet Jews are also more anxious and report lower quality-of-life when compared to the control group (STAI: F = 7.374, p < 0.01; QoL: F = 5.103, p < 0.05). However, the German control group displays more psychosomatic complaints (BSI-S: F = 4.615, p < 0.05). Furthermore, it is notable that ex-Soviet Jews in Israel are less anxious than the Israeli control group and do not differ from them in terms of the other mental health parameters (BSI-A: F = 5.265, p < 0.05). In Russia, Jews are more anxious and have more psychosomatic complaints compared to the control group. However, after a Bonferroni correction, significant differences can be demonstrated only in Austria in terms of symptoms of depression, anxiety, and quality-of-life and in Germany in terms of anxiety between the ex-Soviet Jews and controls. In spite of these elevated levels of distress, over 75% of the participants in each of the migrant subsamples have never used mental health care services, whereas this rate is around 50% in the control groups.
Table 3. Within-country analysis between migrants and controls regarding mental health parameters, controlling for income and education (four separate MANOVA analyses).
A between-country MANOVA analysis was conducted regarding the second and the third research questions on whether there are differences in the mental health burden in the migrant group depending on the new country and whether the mental health burden of migrants differs from that of Jews in Russia (). Despite significant differences in resident status we did not control for it, following the conclusion that resident status does not play a role for mental health in this migrant group, neither in Germany nor in Austria (Trilesnik et al., Citation2022). Considering income and education levels, we found significant mental health differences only in terms of anxiety, specifically ex-Soviet Jews in Austria and Germany are more anxious than those in Israel (STAI: F = 34.118, p < 0.001). Moreover, we found the highest levels of distress in terms of symptoms of depression, anxiety, and quality-of-life in the Jewish subsample in Russia (BSI-D: F = 4.311, p < 0.01; STAI: F = 34.118, p < 0.001; QoL: F = 6.467, p < 0.001).
Table 4. Between-country analysis of ex-Soviet Jews in three new countries and the country of origin regarding mental health parameters, controlling for income and education (MANOVA analysis).
To answer our fourth research question on the association between post-migration factors and the mental health of migrants we applied multiple linear regression analyses, considering the new country’s factors as separate variables. As can be seen in , different factors explain the variance in the individual mental health parameters. In particular, perceived xenophobia plays a detrimental role for symptoms of depression (BSI) and perceived antisemitism for quality-of-life. Regarding acculturation, higher interest in the new culture was found to predict lower depression values (BDI) and higher quality-of-life, while stronger bonds to home culture predict lower depression (BSI), anxiety (BSI), and somatization values, as well as quality-of-life. Additionally, affiliation with Jewish religion is linked positively to quality-of-life, while Jewish, ex-Soviet, and the new country’s identity do not predict mental health parameters. Finally, the new country’s dummy variable plays a role for anxiety (STAI).
Table 5. Factors explaining mental health in migrants in the combined sample in Austria, Germany, and Israel (multiple linear regression).
Discussion
The present paper studies the mental health of ex-Soviet Jewish migrants in Austria, Germany, and Israel in comparison to their respective control groups and to non-migrant Jews in Russia. It also investigates how mental health in this migrant group is related to the new country, discrimination, and other post-migration factors.
As hypothesized in our first research question, we find differences in mental health levels between migrants and natives, even when controlling for income and education level. Ex-Soviet Jews in Austria and Germany display significantly more anxiety symptoms than the respective control groups. Additionally, ex-Soviet Jews in Austria are found to have significantly more symptoms of depression and lower quality-of-life than their controls. These results are in line with previous research on this migrant group (Trilesnik et al., Citation2018; Ullmann et al., Citation2013).
In Israel, on the other hand, the migrant subsample does not differ from its controls in the mental health parameters, although in other studies with only recent ex-Soviet Jewish migrants elevated levels of distress were found compared to the native Israeli population (Mirsky, Citation2009). To put our findings into context, we should consider the possibility that the lack of difference between migrants’ and natives’ mental health levels in Israel could be explained by a higher symptom load in these natives as compared to those in Austria and Germany. However, statistical analysis reveals that this is only the case for quality-of-life, with the German control subsample scoring lowest among the control subsamples on most other mental health parameters. Regarding our first research question, we conclude that ex-Soviet Jewish migrants are in general not more distressed than their respective majority populations. Whether or not they are more distressed seems to depend on the quality of their interaction with the new country.
Regarding our second research question, where we compare migrant mental health between the new countries, our study reveals that the Austrian and German migrant subsamples have significantly higher levels of anxiety than the Israeli one, again controlling for income and education levels. This finding is similar to Flaherty et al. (Citation1988), who showed that ex-Soviet Jews in the United States are more depressed than in Israel, despite having economic advantages. However, further research is needed to clarify the question of why there are significant differences only regarding the one mental health parameter ‘anxiety’ and not regarding the others. Nevertheless, the observation that the same migrant population reports different mental health outcomes regarding at least one parameter after settling in different countries provides some additional support to our conclusion above that characteristics of the new country and related variables can affect the mental health burden of migrated individuals.
Synthesizing the findings of our first and second research questions, ex-Soviet Jews in Israel seem to show better mental health than those in Germany and Austria, both from the within-country and the cross-country perspective. A possible explanation for this could lie in the fact that, as mentioned above, Germany, Austria, and Israel pursue different immigration policies and have different levels of acceptance towards Jewish migrants. In particular, Israel incentivizes Jewish immigration, grants citizenship on arrival, and provides some initial financial support. Until 2005, Germany invited ex-Soviet Jews to immigrate, issued permanent residence permits, and provided financial support via social welfare. After 2005, immigration to Germany became selective for ex-Soviet Jews. In Austria, Jewish migrants from the FSU arrive mostly on a temporary residence permit and receive no financial support. Furthermore, Austria is known to be among the rather xenophobic and antisemitic countries in Europe (Zeglovits et al., Citation2019), a view which is supported by the data in our control group. Moreover, Israel is a country of mostly (Jewish) migrants, naturally lowering the barriers for Jewish newcomers to integrate into the majority society and encouraging a greater sense of belonging to the new country. In Germany and Austria these barriers are more significant, resulting in a weaker sense of belonging, as reflected in the low national identity values and lower interest in the new culture in our data. Furthermore, ethnic density of this migrant group is higher in Israel (1.5 million ex-Soviet Jewish migrants or 17% of the population) than in Austria (20,000 or 0.22%) or Germany (230,000 or 0.28%) (Tolts, Citation2016). All of the factors above could contribute to explaining the different mental health outcomes in the migrant subsamples.
As for our third research question, we find that, in comparison to Jews living in Russia, the mental health burden of ex-Soviet Jewish migrants in Austria, Germany, and Israel is reduced. Additionally, Jews and non-Jews in Russia do not differ in their mental health parameters. These findings suggest on the one hand that ex-Soviet Jews are even more distressed prior to migration, partly explaining the gap between migrant and majority populations’ mental health. On the other hand, we find no evidence for a specific ethnic vulnerability of ex-Soviet Jews. Thus we cannot share the conclusion that ethnicity/heritage culture determines migrant mental health outcomes (Morawa & Erim, Citation2015) and neither such a hypothesis about ex-Soviet Jews in particular (Aroian & Norris, Citation2003). Instead, we attribute the observed low mental health levels of Jews and non-Jews in Russia to that country’s economic and political difficulties. We conclude that the symptomatic burden of the previously distressed ex-Soviet Jews decreases more or less, depending on the new country, while the process of migration per se does not lead to long-term negative consequences for mental health in this population.
In the fourth research question we explored the relationship between mental health burden on the one side and the new country as well as various post-migration factors (perceived discrimination, acculturation attitude, cultural identity, and affiliation to Jewish religion and culture) on the other, also taking into account socio-demographic differences (income, education, resident status). Our findings show that the new country’s variables predict anxiety in our sample even when considering all the factors mentioned above. This is a very important finding, showing that migrant mental health is affected, not surprisingly, by the new country’s characteristics, e.g. immigration policies, integration efforts, ethnic density, and openness towards and acceptance of foreigners (i.e. xenophobic and antisemitic attitudes) in the majority population. Other important predictors for mental health parameters are income, education, perceived xenophobia and antisemitism, interest in the new culture, bonds to home culture and affiliation to Jewish religion.
To sum up, the present study provides some evidence that the elevated mental health burden among ex-Soviet Jewish migrants cannot be attributed to being Jewish, or exclusively to the migration process per se. Rather, the symptom load seems to depend on the quality of interaction between the migrants and the new society. It seems that in new countries where mutual interest and acceptance prevail in the interactions, mental health among migrants is better, whereas in countries with less harmonious interactions their mental health is worse.
Limitations and strengths
Our study has both particular limitations and strengths. First, due to our cross-sectional study design no conclusions about causality can be drawn. Second, the representativeness of our subsamples for the studied population cannot be verified since the data were collected via purposive sampling (for reasons outlined above). Third, unaccounted for variables might explain some of the difference in mental health between the migrant subsamples and confound our results about the new country effect (e.g. physical health, with better physical health possibly being correlated to migration to hot climates like Israel). Finally, we use mental health data of Russian Jews collected in 2017 to estimate the mental health of ex-Soviet Jewish migrants prior to migration, which mostly dates back to the period of 1980 to 2010.
On the other hand, the main strength of our study is its unique study design, assessing a single migrant population in its country of origin and several new countries, as well as comparing it against control groups in each of these. Despite having eight subsamples we could ensure reasonable subsample sizes and high assessment comparability due to, e.g., recruitment of all study participants by the first author. Furthermore, the use of multilingual questionnaires (in the languages of the respective new country and the country of origin) is an important feature that allowed long-time and recent migrants to participate in the study independently of their language skills.
Acknowledgments
The authors gratefully thank Andreas Pähler for editing the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 In the present article, we chose to use the term “new” country instead of the more common terms “host” or “receiving” countries to avoid the association with host–parasite relationship with a possible connotation of migrant inferiority or host–guest relationship, in which case it is expected that migrants may go back.
References
- Alegría, M., Álvarez, K., & DiMarzio, K. (2017). Immigration and Mental Health. Current Epidemiology Reports, 4(2), 145–155. https://doi.org/10.1007/s40471-017-0111-2
- Alegria, M., Canino, G., Shrout, P. E., Woo, M., Duan, N., Vila, D., Torres, M., Chen, C., & Meng, X.-L. (2008). Prevalence of mental illness in immigrant and non-immigrant U.S. Latino groups. The American Journal of Psychiatry, 165(3), 359–369. https://doi.org/10.1176/appi.ajp.2007.07040704
- Aroian, K. J., & Norris, A. E. (2003). Depression trajectories in relatively recent immigrants. Comprehensive Psychiatry, 44(5), 420–427. https://doi.org/10.1016/S0010-440X(03)00103-2
- Balidemaj, A., & Small, M. (2019). The effects of ethnic identity and acculturation in mental health of immigrants: A literature review. The International Journal of Social Psychiatry, 65(7-8), 643–655. https://doi.org/10.1177/0020764019867994
- Beiser, M., & Hou, F. (2017). Predictors of positive mental health among refugees: Results from Canada’s General Social Survey. Transcultural Psychiatry, 54(5-6), 675–695. https://doi.org/10.1177/1363461517724985
- Bermejo, I., Mayninger, E., Kriston, L., & Härter, M. (2010). [Mental disorders in people with migration background compared with German general population]. Psychiatrische Praxis, 37(5), 225–232. https://doi.org/10.1055/s-0029-1223513
- Berry, J. W., Kim, U., Minde, T., & Mok, D. (1987). Comparative studies of acculturative stress. International Migration Review, 21(3), 491–511. https://doi.org/10.1177/019791838702100303
- Berry, J. W., Kim, U., Power, S., Young, M., & Bujaki, M. (1989). Acculturation attitudes in plural societies. Applied Psychology, 38(2), 185–206. https://doi.org/10.1111/j.1464-0597.1989.tb01208.x
- Berry, J. W., Phinney, J. S., Sam, D. L., & Vedder, P. (2006). Immigrant Youth: Acculturation, Identity, and Adaptation. Applied Psychology, 55(3), 303–332. https://doi.org/10.1111/j.1464-0597.2006.00256.x
- Bonelli, R. M., & Koenig, H. G. (2013). Mental disorders, religion and spirituality 1990 to 2010: A systematic evidence-based review. Journal of Religion and Health, 52(2), 657–673. https://doi.org/10.1007/s10943-013-9691-4
- Burnett-Zeigler, I., Bohnert, K. M., & Ilgen, M. A. (2013). Ethnic identity, acculturation and the prevalence of lifetime psychiatric disorders among black, Hispanic, and Asian adults in the U.S. Journal of Psychiatric Research, 47(1), 56–63. https://doi.org/10.1016/j.jpsychires.2012.08.029
- Carta, M. G., Bernal, M., Hardoy, M. C., & Haro-Abad, J. M, Report on the Mental Health in Europe Working Group (2005). Migration and mental health in Europe (the state of the mental health in Europe working group: Appendix 1). Clinical Practice and Epidemiology in Mental Health, 1, 13. http://www.ncbi.nlm.nih.gov/pubmed/16135246 https://doi.org/10.1186/1745-0179-1-13
- Carta, M. G., Reda, M. A., Consul, M. E., Brasesco, V., Cetkovich-Bakmans, M., & Hardoy, M. C. (2006). Depressive episodes in Sardinian emigrants to Argentina: Why are females at risk? Social Psychiatry and Psychiatric Epidemiology, 41(6), 452–456. https://doi.org/10.1007/s00127-006-0052-4
- Chanin, J. L. (2002). Исследование тревожности. In Диагностикаэмоционально-нравственногоразвития. (pp. 124–126). Речь.
- de Wit, M. A. S., Tuinebreijer, W. C., Dekker, J., Beekman, A.-J. T. F., Gorissen, W. H. M., Schrier, A. C., Penninx, B. W. J. H., Komproe, I. H., & Verhoeff, A. P. (2008). Depressive and anxiety disorders in different ethnic groups: A population based study among native Dutch, and Turkish, Moroccan and Surinamese migrants in Amsterdam. Social Psychiatry and Psychiatric Epidemiology, 43(11), 905–912. https://doi.org/10.1007/s00127-008-0382-5
- Dhadda, A., & Greene, G. (2017). The Healthy Migrant Effect” for mental health in England: propensity-score matched analysis using the EMPIRIC Survey. Journal of Immigrant and Minority Health, 20, 799–808. https://doi.org/10.1007/s10903-017-0570-z
- Finch, B. K., Kolody, B., & Vega, W. A. (2000). Perceived discrimination and depression among Mexican-origin adults in California. Journal of Health and Social Behavior, 41(3), 295–313. https://doi.org/10.2307/2676322
- Flaherty, J. A., Kohn, R., Levav, I., & Birz, S. (1988). Demoralization in Soviet-Jewish immigrants to the United States and Israel. Comprehensive Psychiatry, 29(6), 588–597. https://doi.org/10.1016/0010-440X(88)90079-X
- Fortuna, L. R., Álvarez, K., Ramos Ortiz, Z., Wang, Y., Mozo Alegría, X., Cook, B. L., & Alegría, M. (2016). Mental health, migration stressors and suicidal ideation among Latino immigrants in Spain and the United States. European Psychiatry: The Journal of the Association of European Psychiatrists, 36, 15–22. https://doi.org/10.1016/j.eurpsy.2016.03.001
- Friedlander, M. L., Friedman, M. L., Miller, M. J., Ellis, M. V., Friedlander, L. K., & Mikhaylov, V. G. (2010). Introducing a brief measure of cultural and religious identification in American Jewish identity. Journal of Counseling Psychology, 57(3), 345–360. https://doi.org/10.1037/a0019577
- Glaesmer, H., Wittig, U., Brähler, E., Martin, A., Mewes, R., & Rief, W. (2009). Sind Migranten häufiger von psychischen Störungen betroffen? Eine Untersuchung an einer repräsentativen Stichprobe der deutschen Allgemeinbevölkerung [Are migrants more susceptible to mental disorders? A study on a representative sample of the German general population]. Psychiatrische Praxis, 36(1), 16–22. https://doi.org/10.1055/s-2008-1067566
- Laban, C. J., Gernaat, H. B. P. E., Komproe, I. H., Schreuders, B. A., & De Jong, J. T. V. M. (2004). Impact of a long asylum procedure on the prevalence of psychiatric disorders in Iraqi asylum seekers in The Netherlands. The. The Journal of Nervous and Mental Disease, 192(12), 843–851. https://doi.org/10.1097/01.nmd.0000146739.26187.15
- Lindert, J., Ehrenstein, O., Priebe, S., Mielck, A., & Brähler, E. (2009). Depression and anxiety in labor migrants and refugees–a systematic review and meta-analysis. Social Science & Medicine (1982), 69(2), 246–257. https://doi.org/10.1016/j.socscimed.2009.04.032
- Manzoni, P. (2007). Machbarkeitsstudie zu einem Monitoring über Fremdenfeindlichkeit und rechtsextreme Orientierungen in der Schweiz [Feasibility study of the xenophobia and far-right orientation in Switzerland]. Fachstelle für Rassismusbekämpfung, Generalsekretariat des Eidgenössischen Departements des Innern.
- McAuliffe, M., & Triandafyllidou, A. (Eds.). (2021). World Migration Report 2022. International Organization for Migration (IOM). https://publications.iom.int/books/world-migration-report-2022
- Miller, A. M., & Gross, R. (2004). Health and depression in women from the former Soviet Union living in the United States and Israel. Journal of Immigrant Health, 6(4), 187–196. https://doi.org/10.1023/B:JOIH.0000045256.45988.6a
- Mirsky, J. (2009). Mental health implications of migration. Social Psychiatry and Psychiatric Epidemiology, 44(3), 179–187. https://doi.org/10.1007/s00127-008-0430-1
- Mirsky, J., Kohn, R., Levav, I., Grinshpoon, A., & Ponizovsky, A. M. (2008). Psychological distress and common mental disorders among immigrants: Results from the Israeli-based component of the world mental health survey. The Journal of Clinical Psychiatry, 69(11), 1715–1720. https://doi.org/10.4088/jcp.v69n1106
- Morawa, E., & Erim, Y. (2015). Health-related quality of life and sense of coherence among polish immigrants in Germany and indigenous poles. Transcult Psychiatry, 52(3), 376–395. https://doi.org/10.1177/1363461514565851
- Nesterko, Y., Ulitsa, N., Friedrich, M., & Glaesmer, H. (2018). Do they feel the same way? health-related quality of life and satisfaction with life in Jewish immigrants from the former Soviet Union in Germany and Israel. Journal of Cross-Cultural Psychology, 49(4), 618–634. https://doi.org/10.1177/0022022118759223
- Ryder, A. G., Alden, L. E., & Paulhus, D. L. (2000). Is acculturation unidimensional or bidimensional? A head-to-head comparison in the prediction of personality, self-identity, and adjustment. Journal of Personality and Social Psychology, 79(1), 49–65. https://doi.org/10.1037//0022-3514.79.1.49
- Selten, J.-P., van der Ven, E., & Termorshuizen, F. (2020). Migration and psychosis: A meta-analysis of incidence studies. Psychological Medicine, 50(2), 303–313. https://doi.org/10.1017/S0033291719000035
- Stompe, T., Ritter, K., & Schrank, B. (2009). [Depression and culture]. Neuropsychiatrie : Klinik, Diagnostik, Therapie Und Rehabilitation : Organ Der Gesellschaft Osterreichischer Nervenarzte Und Psychiater, 23(4), 253–262.
- Straiton, M. L., Aambø, A. K., & Johansen, R. (2019). Perceived discrimination, health and mental health among immigrants in Norway: The role of moderating factors. BMC Public Health, 19(1), 325. https://doi.org/10.1186/s12889-019-6649-9
- Tolts, M. (2016). Demography of the Contemporary Russian-Speaking Jewish Diaspora [Published Version, 2016]. In Z. Gitelman (ed.), The New Jewish Diaspora: Russian-Speaking Immigrants in the United States, Israel, and Germany (pp. 23–40) Rutgers University Press.
- Toselli, S., Gualdi-Russo, E., Marzouk, D., Sundquist, J., & Sundquist, K. (2014). Psychosocial health among immigrants in central and southern Europe. European Journal of Public Health, 24(Suppl 1), 26–30. https://doi.org/10.1093/eurpub/cku100
- Trilesnik, B., Graef-Calliess, I. T., Stompe, T., & Fydrich, T. (2022). Religiosity, perceived anti-Semitism, xenophobia and mental health: Experiences of Jewish immigrants from the former Soviet Union in Austria and Germany. Transcultural Psychiatry. https://doi.org/10.1177/13634615221107204
- Trilesnik, B., Koch, S., & Stompe, T. (2018). [Mental health, acculturation and religiosity in Jewish migrants from the former Soviet Union in Austria]. Neuropsychiatrie : Klinik, Diagnostik, Therapie Und Rehabilitation : Organ Der Gesellschaft Osterreichischer Nervenarzte Und Psychiater, 32(2), 84–92. https://doi.org/10.1007/s40211-018-0265-2
- Ullmann, E., Barthel, A., Licinio, J., Petrowski, K., Bornstein, S. R., & Strauß, B. (2013). Increased rate of depression and psychosomatic symptoms in Jewish migrants from the post-Soviet-Union to Germany in the 3rd generation after the Shoa. Translational Psychiatry, 3(3), e241. https://doi.org/10.1038/tp.2013.17
- Vang, Z. M., Sigouin, J., Flenon, A., & Gagnon, A. (2017). Are immigrants healthier than native-born Canadians? A systematic review of the healthy immigrant effect in Canada. Ethnicity & Health, 22(3), 209–241. https://doi.org/10.1080/13557858.2016.1246518
- Zeglovits, E., Unterhuber, P., & Sommer, F. (2019). Antisemitismus-Studie 2018: Ergebnisanalyse im Überblick. Antisemitismus. https://www.antisemitismus2018.at/die-studie/
- Zick, A., Küpper, B., & Hövermann, A. (2011). Intolerance, Prejudice and Discrimination—A European Report. https://pub.uni-bielefeld.de/record/2018626