Abstract
In a matter of mere months, humanity was unexpectedly struck by the appearance of SARS-CoV-2, shifting our perception as medical practitioners regarding our day-to-day activity. One especially disconcerting change was patient addressability to medical facilities, as well as access to proper healthcare in various fields. As these changes occurred rapidly, dermatologists too had to adapt by means of teledermatology, giving us back the ability to reach, treat, and comfort our patients. Among the individuals requiring special dermatological attention are those suffering from psoriasis, especially considering that the biological therapies employed in treating this debilitating disease become questionable in the circumstance of the current pandemic. As more evidence surfaces concerning the pathophysiology of SARS-CoV-2, we become closer to understanding which therapies may interfere with its clearance, and which are actually safe to use. This review aims to answer the question, are biological therapies warranted in the treatment of psoriasis during the COVID-19 outbreak, or should they be discontinued?
Disclosure statement
No potential conflict of interest was reported by the author(s).
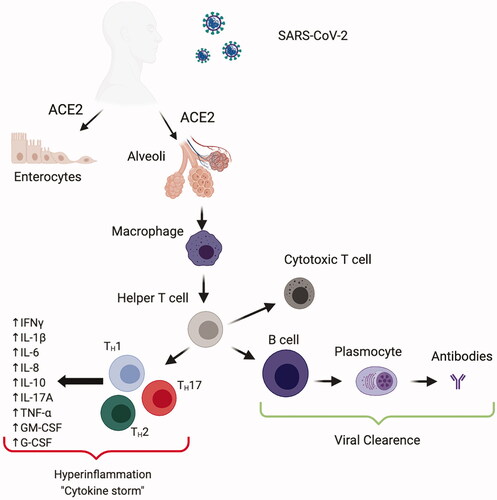
Figure 1. SARS-CoV-2 entry takes place through the airways. By means of a glycoprotein on the viral envelope, it ties to the angiotensin-converting enzyme 2 (ACE2) receptor on the surface of intestinal and alveolar cells. Once inside the organism, the virus is captured by macrophages and presented to T helper cells, triggering the differentiation of T cells and B cells. Adaptive immunity plays a major role in viral clearance through cytotoxic T cells (which destroy infected cells) and antibody-producing B cells. Hyperinflammation occurs due to an exaggerated and sustained combination of innate and adaptive immune responses initiated via T helper 1 (TH1), TH17 or TH2 cell activation. Regarding innate immune activation, concentration of numerous pro-inflammatory effector cytokines, for example TNF, IL-1β, IFNγ, IL-6, IL-8, IL-10, G-CSF and GM-CSF, alongside chemokines (MCP1, IP10 and MIP1α), are elevated in patients with COVID-19, which in turn may contribute to the ‘cytokine storm’ noted in those with severe disease.