
ABSTRACT
Background
Previous studies reported inconsistent outcomes on elastic taping for three potential reasons: 1) poor control of placebo effect; 2) no consensus regarding the optimal tape tension; and 3) lack of investigation on muscle endurance, as the proposed tape recoiling force may not promote peak force generation but exert a consistently low force and improve submaximal contraction.
Purpose
This study compared the effects of elastic tape and its tension on muscle activity and endurance in people with extremely positive and negative personal belief on elastic tape.
Methods
Using a validated instrument, we identified 20 participants with extremely positive personal belief on elastic tape (+ belief), and 20 with extremely negative personal belief (- belief). They performed wrist isometric endurance tests under three taping conditions (i.e. no tape, 50%, and 100% tension). We measured isometric wrist extensor muscle endurance, electromyography muscle activity, and self-perceived performance for each condition.
Results
The differences between the two groups in isometric muscle endurance (p = .85) and muscle activity (p = .53) were not statistically significant, regardless of tape conditions. However, participants with + belief reported better perceived performance than those with – belief (p < .001, partial eta squared = 0.70). Specifically, 100% tape tension yielded stronger self-perceived performance than 50% tension (Cohen’s d = 0.91) and no tape (Cohen’s d = 1.86). On the other hand, participants with – belief perceived similar performance across tape tensions (p = .55).
Conclusion
Elastic tape does not modulate muscle activity and enhance muscle endurance. People with a strong positive personal belief on elastic tape may perceive a better performance with a greater tape tension.
Introduction
Elastic tape is a globally used therapeutic modality by physiotherapists, health clinicians, athletes, and healthy individuals in a wide variety of backgrounds. Among different kinds of elastic tape, kinesiology tape (KT) is a common choice as it garnered increasing popularity since the 2008 Beijing Summer Olympics (Williams, Whatman, Hume, and Sheerin, Citation2012). Despite its wide prevalence, the efficacy and mechanism of KT is poorly understood.
KT is claimed to promote muscle activity through an application known academically as facilitatory KT (Kase, Wallis, and Kase, Citation2003), which is the application of KT from origin to insertion on a muscle, such that it may transmit a recoiling force to the underneath fascia (Vithoulka et al., Citation2010). This supposedly induces greater recruitment of muscle fibers in inactive motor units and hence facilitates muscle activity (Yam, Wong, and Fong, Citation2019). However, the current evidence base is contradictory, with some studies supporting the proposed mechanism of KT (Aktas and Baltaci, Citation2011; Alabbad and Muaidi, Citation2021; Cornwall et al., Citation2019; Huang, Hsieh, Lu, and Su, Citation2011; Lumbroso, Ziv, Vered, and Kalichman, Citation2014) while many other studies refute it with no changes in performance after the application of KT (Cheung et al., Citation2016; Hsiao et al., Citation2022; Wong, Cheung, and Li, Citation2012).
It is possible that the proposed recoiling force provided by KT does not promote peak power generation, but rather exerts a consistently small force that improves a sustained low load contraction. Hence, it is possible that KT may have a more significant effect on muscle endurance rather than strength. Research into the effects of KT on muscle endurance is limited. One study reported a significant decrease in the onset of muscle fatigue in the wrist extensors comparing KT to no taping (Zhang et al., Citation2016). On the other hand, another study did not find any significant changes in muscle fatigue in hand grip endurance test with and without KT (Limmer, Buck, de Marées, and Roth, Citation2020). It is important to note, however, that these studies opted to measure the fatiguability of the muscles, rather than true muscle endurance until failure.
In response to this inconsistent evidence base, recent reports have suggested that a placebo effect may be interacting with participants to form stronger positive effects (Au et al., Citation2017). Some studies have decided to control the placebo effect by using a deceptive design whereby participants who had never heard of KT before had facilitatory KT applied to their bodies under the guise of muscle sensors (Au et al., Citation2017; Cheung et al., Citation2016; Poon et al., Citation2015). These studies were unable to find any increases in muscle performance or activation, indicating that a placebo effect may explain the inconsistent findings in the previous studies. However, these results cannot be generalized to the broader population who are aware of KT. In this population, personal belief on KT will vary depending on the individual. In theory, individuals who believe in the effect of a treatment, are more likely to receive a placebo effect (Price, Finniss, and Benedetti, Citation2008). Mak et al. (Citation2019) tested for the presence of this phenomenon by comparing the effect of facilitatory KT on regular users to non-KT users. They reported that facilitatory KT increased maximal grip strength in KT users but not among KT non-users. In the present study, we intended to build upon this literature by employing a similar study design to study the effect of facilitatory KT on muscle endurance.
Another reason for contradictory findings across previous KT studies is due to varied KT application method. When scoping the literature, studies utilized a range of 0% to 100% stretch (Csapo et al., Citation2012; Limmer, Buck, de Marées, and Roth, Citation2020). Other studies did not indicate how much tension was put through the KT (Zhang et al., Citation2016) while most studies either used a 25–50% tension range (Au et al., Citation2017; MacPhail et al., Citation2018) or 75–100% tension range (Cheung et al., Citation2016; Mak et al., Citation2019). The lack of consistency regarding the stretch of KT may also affect the result of the experiments, leading to inconsistencies within the body of evidence. Hence, in this study, we compared the effect of facilitatory KT on isometric muscle endurance in people with strong personal belief on KT, as they are more prone to be affected by placebo effect through the positive expectancy theory (Price, Finniss, and Benedetti, Citation2008). We hypothesized that there would be an increase in isometric muscular endurance and muscle activity in people with positive personal belief on KT, but not in those with negative personal belief. We also examined the effects of different tensions of KT on muscle endurance. We hypothesized that a KT with 100% tension would provide strongest amount of recoil and hence provide the greater effect than taping with 50% tension or no-tape condition.
Methods
Participants
We recruited 20 participants with extremely positive personal belief on KT (+ belief) and 20 participants with extremely negative personal belief on KT (- belief) in this study via convenient sampling () using a previously established instrument (Jensen and Karoly, Citation1991). Specifically, we asked all potential participants to rate their personal belief of KT on a scale of +5 (i.e. strongly believes a treatment) to −5 (i.e. strongly disbelieves a treatment) where participants with + belief were classified as those who rate their belief on KT ≥ +4 and participants with – belief were classified as ≤ −4. According to Jensen and Karoly (Citation1991) the placebo component for an active treatment can be maximized in participants with + belief, while participants with – belief may have little influence. All participants were adults over the age of 18, and they were free of any active or previous musculoskeletal conditions in the upper limb in the past 12 months. Participants with previous surgery in the upper limb were excluded. The experimental procedures were reviewed and approved by the Western Sydney University Human Ethics Committee (Reference: H14774), and all participants provided written consents prior to the tests.
Table 1. Demographic data of participants split by personal belief on KT.
We estimated our sample size based on the results reported by Mak et al. (Citation2019) which had similar research question and experimental procedure with our present study. Given the Cohen’s f effect size of 0.36, alpha at 0.05, and beta at 0.2, 40 participants were deemed sufficient to power this study.
Experimental procedures
The participants attended a single individual face-to-face testing session. In the testing session, three conditions were tested. The conditions tested were facilitatory KT applied under 50% tension, 100% tension, and no taping on the dominant arm. According to Kase, Wallis, and Kase (Citation2003) 100% tension is defined by stretching the KT to 140% of the original length and 50% is defined by stretching to 120% of the original length. Therefore, in order to make sure that the correct tension was applied, we measured participants’ forearm length (i.e. distance between lateral epicondyle and radial styloid) and adjusted KT length accordingly (Mak et al., Citation2019). For example, a 20-cm KT was used for participant with 28-cm forearm length in the 100% tension condition. We applied KT to participants’ extensor digitorum from lateral epicondyle to radial styloid with participants’ wrist and elbow positioned in neutral and 90-degree flexion, respectively. In this experiment, participants’ tissue tension was not considered. All of conditions were tested in a random order for each participant. As directed by Kase, Wallis, and Kase (Citation2003), facilitatory KT was applied from the origin to insertion of the wrist extensors to elicit muscle facilitation effects. These taping procedures were performed by a musculoskeletal physiotherapist with more than 10 years clinical experience.
Before data collection, participants underwent a 5-minute standardized warm up protocol (Zhang et al., Citation2016) with wrist flexion and extension stretching exercises (Mak et al., Citation2019). Immediately after this, the first KT condition was applied onto the participant’s wrist extensors. The participant was then asked to sit on a chair with their arm supported and wrist hanging off the plinth. The plinth was then raised such that the elbow was flexed at 90 degrees. In that position, the participant was asked to hold a 3-kg dumbbell with their dominant arm in a pronated position for as long as they could. The test was repeated another 2 times and the longest time the patient could maintain their wrist in neutral position within a 5-degree leeway was taken (Au et al., Citation2017). The procedure was repeated with all the other taping conditions in a randomized order. A minimum 60-minute between condition and 15-minute inter-set rest period was prescribed, as supported by a previous muscle physiology study (Cornwall, Krock, and Wagner, Citation1994).
Isometric muscle performance was quantified by the longest time the participant could maintain their wrist in neutral position within a 5-degree leeway, which was monitored by a motion capture system (Vicon, Oxford, UK). We attached reflective markers on the lateral epicondyle, medial epicondyle, radial styloid, ulnar styloid, and head of the third metacarpal (Turner, Forrester, Mears, and Roberts, Citation2020) and we referred to the International Society of Biomechanics recommendations (Wu et al., Citation2005) on the wrist joint coordinate system. Surface EMG activity of the wrist extensors was simultaneously measured by an Ag/AgCl electrode (SX230, Biometrics Limited, Newport, UK) operating at 1,000 Hz. To reduce impedance, the skin of the tested forearm was shaved, cleaned with alcohol, and lightly rubbed with sandpaper before applying the EMG electrodes. We referred to a method previously described for electrode placement (Cai, Au, An, and Cheung, Citation2016). In brief, the tape was hole punched according to participants’ forearm length and the muscle bulk position, with the predetermined tension for each condition. Conductive gel was applied to the electrode and surface EMG placement was determined and standardized according to the protocol described in a previous study (Hermens, Freriks, Disselhorst-Klug, and Rau, Citation2000). EMG activity of the first and last second of the isometric endurance test was discarded to remove movement artifacts. Change in EMG activity was calculated as the difference of root-mean-square measured between the first and last 10 second data. After each muscle endurance test was performed, the participants were asked to rate their self-perceived performance using the visual analogue scale, which is a 100-mm horizontal line with anchor lines at 0 (worst performance) and 10 (best performance) (Mak et al., Citation2019).
Statistical analysis
All data was analyzed using the SPSS (version 23, IBM, Chicago, IL, USA). We used Chi square test to compare gender distribution between the two groups, and independent samples t tests for body height and weight comparison. After confirming data normality using Shapiro–Wilk test, repeated measures ANOVA was used to test the interaction effect between personal belief (i.e. + belief vs – belief) and taping condition (i.e. 50% tension, 100% tension, and no taping) on muscle endurance (i.e. performance time, change in muscle activity, and self-perceived performance). If indicated, we also conducted pairwise comparisons with Bonferroni adjustment. The global alpha level was set at 0.05.
Results
Characteristics between the two groups of participants were matched in terms of gender distribution, body weight, and body height (p > .05, ). Repeated measures ANOVA revealed that there was no significant interaction effect between personal belief and KT tension on performance time (F (1.60,61.04) = 0.18, p = .79, partial eta squared = 0.01). We also did not observe any significant main effect of personal belief (F (1,38) = 0.04, p = .85, partial eta squared = 0.00) and KT tension (F (1.60,61.04) = 0.91, p = .39, partial eta squared = 0.02) on performance time (, ).
Figure 1. Effect of KT tension on muscle endurance performance in participants with extremely positive (+ belief) and extremely negative personal belief on KT (- belief).
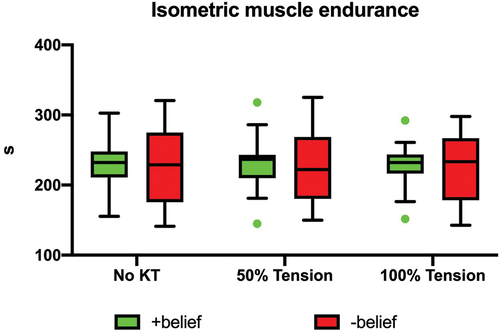
Table 2. Mean and 95% confidence intervals of dependent variables in relation to personal belief and tape tension.
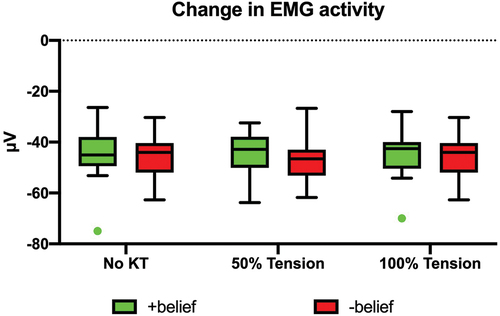
Similarly, repeated measures ANOVA revealed no significant interaction effect between personal belief and KT tension on changes in muscle activity (F (2,76) = 0.77, p = .47, partial eta squared = 0.02). Furthermore, no statistical main effect of personal belief (F (1,38) = 0.41, p = .53, partial eta squared = 0.01) and KT tension (F (2,76) = 0.23, p = .79, partial eta squared = 0.01) on changes in muscle activity was found (, ).
Figure 2. Effect of KT tension on EMG activity in participants with extremely positive (+ belief) and extremely negative personal belief on KT (- belief).
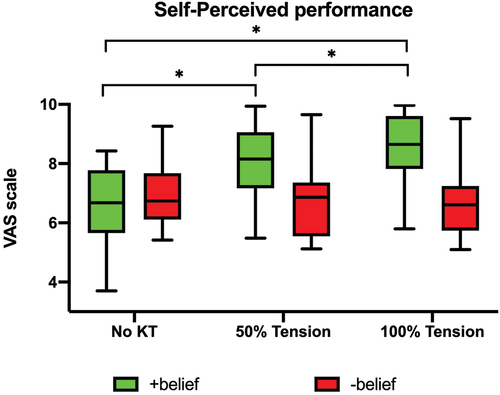
However, there was a significant interaction effect between personal belief and KT tension on self-perceived performance (F (2,76) = 28.92, p < .001, partial eta squared = 0.43). We found a significant main effect of KT tension on self-perceived performance in participant with + belief (F (1.24,23.61) = 43.23, p < .001, partial eta squared = 0.70), but not for participants with – belief (F (2,38) = 0.60, p = .55, partial eta squared = 0.03). Pairwise comparisons suggested a significant greater perceived performance when participants with + belief received 100% tension, when compared with 50% tape (p < .001, Cohen’s d = 0.91) and no taping (p > .001, Cohen’s d = 1.86). Participants in the 50% tension also reported a better performance when compared with no tape condition (p < .001, Cohen’s d = 1.20) (, ).
Figure 3. Effect of KT tension on self-perceived performance in participants with extremely positive (+ belief) and extremely negative personal belief on KT (- belief).
Discussion
This study investigated the effect of faciliatory KT on wrist muscle endurance performance, muscle activity, and self-perceived performance between people with different personal belief on KT. In contrast with our original hypothesis, we found that facilitatory KT, regardless of tape tension, did not improve muscle endurance performance and change muscle activity, regardless of participants’ personal belief on KT. However, participants with + belief perceived a better performance with a greater tension of KT, while the perceived performance of participants with – belief was not affected by KT tension.
These results are not in line with previous research which reported a promotion of muscle strength by KT in regular users (Mak et al., Citation2019). In our study, the placebo effect in the + belief group was expected to enhance their performance. However, we did not detect a placebo effect and there were no changes in performance between the two groups. Whilst our study recruited individuals who believed in the effect of KT, it may be possible that regular KT users have a stronger belief in KT that results in a stronger placebo effect and hence muscle performance. In terms of changes in muscle activity, our results are consistent with past results which indicate that there were no significant differences between participants with different personal belief on KT (Cai, Au, An, and Cheung, Citation2016; Pires et al., Citation2020). Our study also found that KT was unable to initiate changes in EMG activity regardless of the tape tension. Hence, our study refutes the proposed mechanism of KT wherein a recoiling force acts upon the muscle fascia to facilitate the recruitment of muscle fibers. Some studies have put forth alternative mechanisms for KT. For example, one study suggests that KT may increase intramuscular blood flow (Álvarez-Álvarez et al, Citation2014). This would decrease the accumulation of metabolites and algogenic substances and ultimately improve muscle’s resistance to fatigue. An established mechanism of KT is yet to be found and hence further research into its mechanism is needed.
Self-perceived performance was the only outcome measure with a significant difference between participants with different personal belief on KT. Interestingly, despite a lack of an improvement in muscle performance, participants with + belief rated their self-perceived performance higher than those with – belief. This is not in agreeance with previous studies (Cai, Au, An and Cheung, Citation2016; MacPhail et al., Citation2018; Mak et al., Citation2019) that reported non-significant influence of personal belief on perceived performance. A possible reason for this disparity is that these past studies used dynamic tests in their study design. During dynamic movements, the lack of consistent tension may have affected the participant’s ability to sense the KT, which could have led to poorer self-perceived performance. Additionally, these previous studies did not blind their participants to their performance in the collected outcome measures. For example, Cai, Au, An and Cheung (Citation2016) and MacPhail et al. (Citation2018) used a hand-held dynamometer to collect grip strength data, hence providing an objective measurement for participants to see how well they were performing. In our study, participants were not told their performance (i.e. muscle endurance time) and EMG data was processed after data collection. Hence, when asked to rate their performance on the visual analogue scale, participants solely relied on their subjective opinion. Therefore, it may be possible that the positive belief on KT in the + belief group was translated through to a higher self-perceived performance.
Furthermore, our study showed that 100% tension led to stronger self-perceived performances than 50% tension and no KT in participants with + belief. A possible explanation for this may be due to the design of the isometric muscle endurance test. The mechanical stiffness of the KT when stretched to 100% tension may have provided a stronger proprioception and stability that helped participants maintaining their wrist position for longer, especially for participants who have a stronger belief on KT.
There are a couple clinical implications that may been drawn from this study. First, facilitatory KT does not enhance muscle endurance performance or induce changes in muscle activity during a submaximal low-load isometric task. Second, a placebo effect may not be detected if the users are not quantitatively informed on their performance. Lastly, higher tension of KT may elicit stronger self-perceived performance in people with stronger personal belief on KT. Self-confidence is well known to be a central tenant to success in athletes (Feltz, Citation1988). Athletes who reach a level of optimal self-confidence are able to increase their concentration and effort levels, as well as feel calm and relaxed under pressure (Kuloor and Kumar, Citation2020). Conversely, overconfidence and a lack of self-confidence can result in anxiety, indecisiveness, and break concentration (Kuloor and Kumar, Citation2020). Hence, the use of KT is justified if clinicians are aware that the individual’s personal belief will promote a meaningful effect on their athletic performance.
There are several limitations to the study. Firstly, this study utilized convenience sampling, and this may introduce biases to the study. Secondly, because the KT was hole-punched to place the EMG electrodes onto the skin, this may have compromised the integrity and hence mechanism of the KT. Thirdly, we did not record participants’ physical activity level and exercise habit, as they may affect the neuromuscular system and potentially the outcome of the present study. Lastly, our study recruited young and healthy adults. As such, these results may not be generalized to individuals with injuries or pathologies.
Conclusion
Kinesio tape is unable to promote muscle activity and improve muscle endurance performance, regardless of personal belief on KT. People with a positive belief on KT perceived a better performance with greater tape tension than those with negative belief.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Aktas G, Baltaci G 2011 Does Kinesiotaping Increase Knee Muscles Strength and Functional Performance? Isokinetics and Exercise Science 19: 149–155.
- Alabbad M, Muaidi Q 2021 The effect of the Kinesio tape on the muscle power performance of elite weightlifters. Journal of Bodywork and Movement Therapies 27: 26–33. 10.1016/j.jbmt.2021.02.027
- Álvarez-Álvarez S, José FG, Rodríguez-Fernández AL, Güeita-Rodríguez J, Waller BJ 2014 Effects of Kinesio® Tape in low back muscle fatigue: Randomized, controlled, doubled-blinded clinical trial on healthy subjects. Journal of Back and Musculoskeletal Rehabilitation 27(2): 203–212. 10.3233/BMR-130437
- Au IP, Fan PC, Lee WY, Leong MW, Tang OY, An WW, Cheung RT 2017 Effects of Kinesio tape in individuals with lateral epicondylitis: A deceptive crossover trial. Physiotherapy Theory and Practice 33(12): 914–919. 10.1080/09593985.2017.1359871
- Cai C, Au IP, An W, Cheung RT. Facilitatory and inhibitory effects of Kinesio tape: Fact or fad? Journal of science and medicine in sport / Sports Medicine Australia. 2016 Feb;19(2):109–112. doi: 10.1016/j.jsams.2015.01.010.
- Cheung RT, Yau QK, Wong K, Lau P, So A, Chan N, Kwok C, Poon KY, Yung PS 2016 Kinesiology tape does not promote vertical jumping performance: A deceptive crossover trial. Manual Therapy 21: 89–93. 10.1016/j.math.2015.06.001
- Cornwall MW, Jain TK, Holmgren S, Dorri A, Young C 2019 The effect of Kinesio tape on static foot posture, plantar pressure and rearfoot motion in individuals with pronated feet. International Journal of Sports Physical Therapy 14(3): 368–375. 10.26603/ijspt20190368
- Cornwall MW, Krock LP, Wagner LM 1994 Muscular fatigue and recovery following alternating isometric contractions at different levels of force. Aviation, Space, and Environmental Medicine 65(4): 309–314.
- Csapo R, Herceg M, Alegre LM, Crevenna R, Pieber K 2012 Do kinaesthetic tapes affect plantarflexor muscle performance? Do Kinaesthetic Tapes Affect Plantarflexor Muscle Performance? Journal of Sports Sciences 30(14):1513–1519. 10.1080/02640414.2012.712713
- Feltz DL. Self-confidence and sports performance. Exercise and sport sciences reviews. 1988;16:423–457.
- Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G 2000 Development of recommendations for SEMG sensors and sensor placement procedures. Journal of Electromyography and Kinesiology 10(5): 361–374. 10.1016/S1050-6411(00)00027-4
- Hsiao CK, Tsai YJ, Lu CW, Hsiung JC, Hsiao HY, Chen YC, Tu YK 2022 Effects of Kinesio taping on forearm supination/pronation performance fatigability. BMC Musculoskeletal Disorders 23(1): 131. 10.1186/s12891-022-05068-4
- Huang CY, Hsieh TH, Lu SC, Su FC 2011 Effect of the Kinesio tape to muscle activity and vertical jump performance in healthy inactive people. BioMedical Engineering OnLine 10(1): 70. 10.1186/1475-925X-10-70
- Jensen MP, Karoly P 1991 Motivation and expectancy factors in symptom perception: A laboratory study of the placebo effect. Psychosomatic Medicine 53(2): 144–152. 10.1097/00006842-199103000-00004
- Kase K, Wallis J, Kase T 2003 Clinical therapeutic applications of kinesio taping method. Albuquerque, NM, USA: Kinesio Taping Association.
- Kuloor H, Kumar A 2020 Self-confidence and sports. International Journal of Indian Psychology 8: 1–6.
- Limmer M, Buck S, de Marées M, Roth R 2020 Acute effects of kinesio taping on muscular strength and endurance parameters of the finger flexors in sport climbing: A randomised, controlled crossover trial. European Journal of Sport Science 20(4): 427–436. 10.1080/17461391.2019.1633415
- Lumbroso D, Ziv E, Vered E, Kalichman L 2014 The effect of kinesio tape application on hamstring and gastrocnemius muscles in healthy young adults. Journal of Bodywork and Movement Therapies 18(1): 130–138. 10.1016/j.jbmt.2013.09.011
- MacPhail AJ, Au IP, Chan M, Mak DN, An WW, Chan ZY, Zhang JH, Wong K, So A, Chan N, et al. 2018 Type effect of inhibitory KT tape on measured vs. perceived maximal grip strength. Journal of Bodywork and Movement Therapies 22(3): 639–642. 10.1016/j.jbmt.2017.10.011
- Mak DN, Au IP, Chan M, Chan ZY, An WW, Zhang JH, Draper D, Cheung RT 2019 Placebo effect of facilitatory Kinesio tape on muscle activity and muscle strength. Physiotherapy Theory and Practice 35: 157–162. 10.1080/09593985.2018.1441936
- Pires LG, Padula RS, Junior MADL, Santos I, Almeida MO, Tomazoni SS, Costa LCM, Costa LOP 2020 Can Kinesio Taping® influence the electromyographic signal intensity of trunk extensor muscles in patients with chronic low back pain? A randomized controlled trial. Brazilian Journal of Physical Therapy 24(6): 539–549. 10.1016/j.bjpt.2019.12.001
- Poon KY, Li SM, Roper MG, Wong MK, Wong O, Cheung RT 2015 Kinesiology tape does not facilitate muscle performance: A deceptive controlled trial. Manual Therapy 20(1): 130–133. 10.1016/j.math.2014.07.013
- Price DD, Finniss DG, Benedetti F 2008 A comprehensive review of the placebo effect: Recent advances and current thought. Annual Review of Psychology 59(1): 565–590. 10.1146/annurev.psych.59.113006.095941
- Turner J, Forrester SE, Mears A, Roberts JR 2020 The influence of tracking marker locations on three-dimensional wrist kinematics. Journal of Science and Medicine in Sport 23(10): 985–990. 10.1016/j.jsams.2020.03.011
- Vithoulka I, Beneka A, Malliou P, Aggelousis N, Karatsolis K, Diamantopoulos K 2010 The effects of Kinesio-Taping® on quadriceps strength during isokinetic exercise in healthy non athlete women. Isokinetics and Exercise Science 18(1): 1–6. 10.3233/IES-2010-0352
- Williams S, Whatman C, Hume PA, Sheerin K 2012 Kinesio taping in treatment and prevention of sports injuries: A meta-analysis of the evidence for its effectiveness. Sports Medicine 42(2): 153–164. 10.2165/11594960-000000000-00000
- Wong OM, Cheung RT, Li RC 2012 Isokinetic knee function in healthy subjects with and without Kinesio taping. Physical Therapy in Sport 13(4): 255–258. 10.1016/j.ptsp.2012.01.004
- Wu G, van der Helm F, Dirkvan Veeger H, Makhsous M, Van Roy P, Anglin C, Nagels J, Karduna AR, McQuade K, Wang X, et al. 2005 ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion - Part II: Shoulder, elbow, wrist and hand. Journal of Biomechanics 38(5): 981–992. 10.1016/j.jbiomech.2004.05.042
- Yam TT, Wong MS, Fong SS 2019 Effect of Kinesio taping on electromyographic activity of leg muscles during gait in children with developmental coordination disorder: A randomized controlled trial. Medicine 98(6): e14423. 10.1097/MD.0000000000014423
- Zhang S, Fu W, Pan J, Wang L, Xia R, Liu Y 2016 Acute effects of Kinesio taping on muscle strength and fatigue in the forearm of tennis players. Journal of Science and Medicine in Sport 19(6): 459–464. 10.1016/j.jsams.2015.07.012