
ABSTRACT
Background
It has been two decades since the World Health Organization’s endorsement of the International Classification of Functioning, Disability and Health (ICF). It is timely to undertake a rigorous search that analyzes the discourses around the ICF’s conceptual framework within physiotherapy, the kinds of enquiry to date and the professional areas where this is happening and how.
Purpose
The aim of this research is to synthesize the literature related to how the physiotherapy profession (practice, research and education) thinks about and puts to use the WHO ICF.
Results
A final sample of 37 papers was agreed. Five overarching third-order interpretations were derived: (i) A way of thinking and practicing, (ii) Endorsed but not embedded, (iii) Striking a balance, (iv) Power of participation and (v) Moving forward. Together, these themes illustrate the evolving role of the ICF in physiotherapy over the previous two decades. They highlight the ICF’s potential for shaping the future of physiotherapy practice, education and research.
Conclusions
Work is needed to connect existing literature about the ICF and related models and embed the ICF, its language and philosophy across physiotherapy education and practice. Re-representation of the model might help address misinterpretation of the ICF, but fundamentally, embedding the ICF in entry-level curriculum is likely to be the most significant driver of change in practice.
Introduction
The World Health Organization’s International Classification of Functioning, Disability and Health (WHO ICF) represents a paradigm shift in health care. Fundamentally, the ICF represents a multidimensional way of thinking about health and functioning, moving away from a focus on disease and causation that has long dominated many health professions (Üstün et al., Citation2003). Endorsed in 2001, the ICF was adapted from the WHO’s International Classification of Impairments, Disabilities and Handicaps (ICIDH) (de Kleijn-de Vrankrijker, Citation2003) which was seen as being negatively focused and old-fashioned. It aims to integrate the medical and social models of health. The ICF arguably enables a more positive and universal way of thinking about the implications of disease and injuries, acknowledging that all people can experience a change to their health at any time (Iezzoni and Freedman, Citation2008; World Health Organization, Citation2001, Citation2002).
At the time of its launch, the WHO identified that the ICF was useful in individual, institutional and social contexts (World Health Organization, Citation2002). Specific applications proposed by the WHO include patient assessment and intervention planning, communication across teams and nations, data collection, quality assurance, community needs assessment and policy development (World Health Organization, Citation2002). Other applications have since been identified, including development of core sets, clinimetrics (i.e., development of assessment tools and batteries), framing of evidence-based clinical guidelines and educational materials (e.g., Heerkens, van der Brug, Ten Napel, and Van Ravensberg, Citation2003). The framework has two broad applications: conceptual and categorical (i.e., classification), although these are not mutually exclusive.
There are a number of published reviews about the ICF, with varying methodological or analytical emphasis. Some are concerned with understandings of specific areas of the ICF such as personal factors (Geyh et al., Citation2011; Geyh, Schwegler, Peter, and Müller, Citation2019), use of the ICF in certain areas of health care or particular practices (Alford, Remedios, Webb, and Ewen, Citation2013; Constand and Macdermid, Citation2014; Momsen et al., Citation2019) and geographical regions (Maribo et al., Citation2016) or certain applications of the ICF (Karlsson and Gustafsson, Citation2022). Some use the ICF as an analytical lens (i.e., van Uem et al., Citation2016); others adopt a specific practice focus.
Disciplinary-oriented reviews are helpful in showing the particular discourses that feature within a specific profession; here, how professions think about and put to use the ICF framework. Two reviews have addressed ICF use in physiotherapy. Allet, Bürge, and Monnin (Citation2008) conducted a critical review spanning 7.5 years (May 2001 to Nov 2007). They aimed to summarize the application of the ICF to physiotherapists’ daily practice and concluded that the ICF has clinical relevance across the areas of communication, assessment, intervention, outcomes and (to a lesser extent) guidelines. They did not locate literature relating to the use of the ICF in physiotherapy education. In a scoping review of 12 years of published literature, Escorpizo and Bemis-Dougherty (Citation2015) aimed to summarize the use of the ICF in physiotherapy practice and research (although also incorporating literature related to teaching). They concluded that the ICF was used in assessment and measurement tools and had been applied across the lifespan, with various health conditions and in various healthcare settings. They saw a need to determine the added contribution that the ICF makes to physiotherapy in order to trigger greater uptake within the profession. The search strategies for neither paper were extensive, meaning potentially insightful literature was overlooked. Furthermore, the methodological approaches of both studies yielded findings that described broad aspects of the literature. Over two decades since the WHO’s ICF endorsement, we believe it is timely to undertake a more rigorous search that analyzes the discourses around the ICF’s conceptual framework within physiotherapy, the kinds of enquiry to date and the professional areas where this is happening and how. The World Confederation of Physical Therapy (WCPT) explicitly identifies the ICF as a model that physiotherapists should recognize (World Physiotherapy, Citation2019); we were interested in whether and how this was happening. We collaborated to investigate How, and to what end, is the WHO ICF framework represented in physiotherapy?
Material and methods
We conducted a qualitative research synthesis informed by the method described by Major and Savin-Baden (Citation2010). A qualitative synthesis is a coherent analytical approach that gives fresh meaning to a body of work and aims to create new knowledge. The findings of a qualitative synthesis can only be derived from an analysis of the whole body of literature; the collective interpretations are greater than what can be gained from reading individual publications.
Search strategy and inclusion criteria
Sentinel papers and test searches were used to develop, evaluate and refine the search. The search strategy was developed collaboratively among the research team with a librarian. The search was conducted using the following databases: Medline (Ovid), CINAHL (EBSCOHost), Emcare (Ovid), ERIC (ProQuest), Web of Science and Scopus. The librarian translated the strategy for running on all these databases. outlines the inclusion and exclusion criteria.
Table 1. Inclusion and exclusion criteria.
Selection of relevant literature
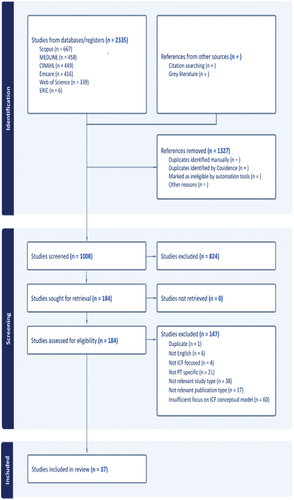
Databases were searched on March 15, 2023 and a total of 1022 records were obtained excluding duplicates. Covidence software (www.covidence.org) was used to first screen the titles and abstracts of these eligible search results. If it was difficult to determine eligibility based on title and abstract alone, full-text screening occurred. Both authors completed these processes. A final sample of 37 papers () was agreed.
Figure 1. Prisma flow diagram of search.
Data extraction and analysis
We completed three stages of analysis: (i) data extraction and first-order findings, (ii) second-order themes and (iii) third-order interpretations (Major and Savin-Baden, Citation2010; Noblit and Hare, Citation1988). The first stage served to create a summary of each literature source and begin the interpretative process (i.e., first-order findings represented our initial thoughts about the findings of each paper from the sample) (supplementary material). Analysis then involved considering the sample’s whole body of work to generate second-order themes (i.e., preliminary themes and concepts). Stages one and two were completed independently by the authors, then discussed to combine analyses. The final stage represents a synthesized analysis to generate themes that create a line of argument across the entire sample and offer new perspectives and understanding about the ICF that are not in view when papers are read separately. The movement from second-order themes to third-order interpretations can be seen within ; this was a collaborative stage of analysis between the two researchers.
Table 2. A way of thinking and practicing.
Table 3. Endorsed but not embedded.
Table 4. Striking a balance.
Table 5. Power of participation.
Table 6. Moving forward.
Reflexivity
The researchers are both academics from health professional backgrounds – a physiotherapist and a speech pathologist. Both have previously written together about the ICF but also bring particular disciplinary and educational perspectives and research expertise. Our different positions were a strength of the research, particularly with the framing of the research question, the search strategy parameters and analysis, and enabled the questioning of assumptions and biases.
Results
Our final sample comprised 37 papers indicated by an asterisk in the reference list (35 original works and a related commentary and response; ). Papers were published relatively consistently between 2004 and 2022, with the majority from North America (n = 24). Four professional endorsements were mostly published early (2005–2008, with one in 2022), nine case reports placed mainly in the middle period (2008–2018) and eight research papers using the ICF as a conceptual/analytic lens were published more recently (2011, 2016, 2021 and 2022). Sixteen conceptual papers spanned the entire period.
Figure 2. Publication types within our sample.
Five overarching third-order interpretations were derived and are outlined below. These interpretations are present across all papers in the sample, either overtly or with notable absence (e.g., participation focus; person perspective). Although described separately, there is considerable overlap of content within and across each interpretation. The papers supporting each second-order subtheme are identified in .
A way of thinking and practicing ()
The ICF offered the authors of included papers a worldview that is representative of a way of thinking and practicing (WTP). Ways of thinking and practicing (McCune and Hounsell, Citation2005) encompass a distinct mind-set, language, and behaviors that are integral to a particular discipline. These frameworks are essential in organizing and encapsulating a discipline’s core practices, values, philosophies and viewpoints. They emphasize the inseparable link between knowing and doing, that is, of “putting knowledge to work” (Barradell, Barrie, and Peseta, Citation2018 p.2). Ways of thinking and practicing can also help to nurture a comprehensive and interconnected perspective, encouraging therapists to consider diverse knowledge forms and their application in authentic contexts (Barradell, Barrie, and Peseta, Citation2018). Validation for the ICF as a WTP in physiotherapy was represented in the subthemes: Support for the ICF, Clinical reasoning and decision making, Provides structure, Making connections, Big picture perspective and Person centered.
Support for the ICF
This sample of studies indicates that the ICF enjoys substantial support within physiotherapy, with endorsements from professional bodies and integration into physiotherapy program curricula. Endorsement papers have helped shape the profession’s perspective, informing and encouraging the discipline to adopt the framework in different areas of practice, research and education. Acceptance of the ICF was assisted by its effective integration with familiar complementary approaches, such as professional guidelines and evidence-based practice and compatible models, like the Nagi model, and those related to clinical reasoning, motor learning and pain.
Clinical reasoning
The ICF was explicitly applied to clinical reasoning in almost half the papers in this synthesis. It facilitated reflection and reevaluation of interrelationships and decisions throughout treatment, helping therapists to examine the decisions behind their practice. That is, the ICF was understood to provide a systematic approach for clinicians to explore and clarify their thinking, ultimately enhancing the quality of care provided. Use of the ICF also supported other aspects of clinical reasoning including identifying case complexity and areas that had been overlooked in the clinical encounter, considering prognosis, prioritizing problems, developing high-level goals, linking intervention to goals, thinking beyond physical factors (i.e., physical impairments, speed, distance, and aids) typically considered the primary domain of physiotherapists, and adopting a person-centered approach.
Provides structure
Organizing professional knowledge is a feature of WTP. The authors of the included papers considered the ICF to be a valuable resource providing structure and a common language for understanding health-related states worldwide. Notably, the ICF’s structured approach was employed in organizing case report information or was incorporated in the development of various clinical reasoning tools to help guide stages of decision-making.
Making connections
Ways of thinking and practicing can foster an inclusive and integrated outlook, helping clinicians to make diverse connections. In our synthesis, this was apparent in facilitating connections across domains, enhancing communication and teamwork, advocating for consumers, conveying knowledge and skills, clarifying professional roles, particularly in the context of interdisciplinary care, and linking varied knowledge types with the ICF for practical purposes.
Big picture perspective
The ICF, as a WTP, offers a comprehensive and integrated perspective. Authors of our sample papers credited the ICF with fostering a profound, comprehensive understanding of health conditions, and addressing the unique needs of specific groups. Additionally, authors observed that the ICF played a vital role in identifying and addressing contextual factors, such as language barriers, interdisciplinary or support group referrals, and evaluating performance in relevant contexts. Moreover, authors commented that reflection using the ICF could help clinicians to identify overlooked areas of patient care.
Person centered
Across the reviewed articles, the ICF was portrayed as a framework that values a holistic and person-centered focus. Many papers emphasized that integrating the ICF across physiotherapy practice, education, and research fosters a shift toward a comprehensive and person-centered perspective, ultimately promoting better understanding and care for individuals with health conditions. This was seen to enhance physiotherapists’ understanding of an individual’s experience, disablement and living with a health condition.
In summary, the ICF is consistent with physiotherapy’s fundamental practices, values, philosophies and perspectives, aligning closely with WTP. The ICF is widely recognized and endorsed within the profession, helping to organize knowledge and enhance clinical reasoning. This highlights the ICF’s capacity to foster a comprehensive and interconnected perspective, bridging diverse knowledge forms and facilitating its application in authentic contexts.
Endorsed but not embedded ()
While the ICF may be familiar to physiotherapists, and its benefits were clearly recognized and applied in various ways (WTP above), our findings suggest that the ICF framework is espoused more than it is embedded. Here, we explore four related subthemes: Has it caught on? Familiarity, Practicalities and Perpetuating misunderstandings.
Has it caught on?
Several authors observed limited adoption of the ICF within physiotherapy practice, noting a slowness to embrace the framework, little evidence of its use in documentation and generally more work being needed to fully utilize the ICF. Two decades of potential global influence in physiotherapy are represented by only 35 qualitative papers and two related comments.
Familiarity
Authors commented that the ICF continues to suffer from a lack of familiarity within physiotherapy and that its limited application has hindered its potential to inform and revolutionize practice, research, education and administration. We observed restricted conceptual understanding of the ICF. For example, we noted poor distinction between the concepts of “activity” and “participation,” and an erroneous assumption of a direct relationship among the framework’s components. Several reasons were said to contribute to this lack of familiarity including challenges with academic learning, clinical educators’ limited grasp of the ICF’s intricacies, and the scarcity of comprehensive learning experiences during student placements.
Practicalities
Challenges related to resource availability were reported to obstruct ICF application in practice. These included limited access to interdisciplinary teams and restricted access to healthcare services. Not only was referral to important services affected by financial constraints (i.e., the lack of health insurance), it was also an important factor in reduced access to the number of available treatment sessions. In fieldwork contexts, factors such as high workloads, limited autonomy, time constraints, excessive paperwork, and high student numbers were identified as barriers to ICF application. Some authors reported that limited exposure to case studies in pre-clinical academic studies left students feeling unprepared for ICF application in practice and graduates explained that navigating different and potentially conflicting expectations and feedback from multiple clinical instructors was confusing.
Perpetuating misunderstanding
We observed confusion in implementing or representing the ICF model, including limited conceptual understanding and inconsistencies in terminology, resulting in unintended inaccuracies and misinterpretations. We also detected inconsistent reporting within case reports. Some used WHO sanctioned forms and diagrams, while others featured errors or confusing labeling conventions.
In short, while the ICF is recognized within physiotherapy, its comprehensive integration remains a challenge. Limited familiarity, an initial focus on impairments in students’ education, workplace barriers, and ongoing confusion in implementation all contribute to its limited practical application.
Striking a balance ()
This third-order interpretation delves into the tensions that physiotherapists must negotiate within the complex arena in which they practice, study and research. It encapsulates three related subthemes: Disability paradox; Disconnect between biomedical and social; and Mismatch between patient and therapist.
Disability paradox
The disability-specific papers in our sample addressed the concept of the disability paradox in physiotherapy, highlighting the necessity of transcending the limitations of the medical and social models of care in isolation. Authors advocated for the integration of a biopsychosocial model, supported by the ICF, noting that it aligns with the profession’s ethical standards and emphasizing the importance of recognizing personal biases and cultural sensitivities among practitioners. By incorporating the ICF framework, authors argued that physiotherapy could move toward a more comprehensive, person-centered approach, ultimately enhancing the quality of care provided to individuals with disabilities. This perspective recognizes that disability is shaped by societal factors and authors stressed the importance of considering social, political, and economic influences to support patients in achieving independence based on their unique goals.
Disconnect between (bio)medical and social
Across our sample, the ICF was referred to as either or even both a disablement and an enablement model. Many authors did not explicitly specify which approach they were applying, but the differences in their perspectives were evident.
Our review revealed a pervasive bias in the literature, present not only in case reports but also in conceptual papers. A primary focus was on utilizing the ICF to identify impairments and limitations, with a strong emphasis on dysfunction and biomedical causative factors. This emphasis often obscured the positive aspects of ICF domains, such as strengths, resources, and contextual factors. Consequently, this skewed perspective overlooks the full spectrum of capabilities and facilitators within the ICF framework. Nonetheless, some authors advocated for a more holistic understanding of patient experiences by integrating sociocultural viewpoints into physiotherapy. They recognized the ICF’s value in not only acknowledging challenges but also emphasizing an individual’s health by identifying their capabilities. They noted that the ICF’s comprehensive framework enabled systematic assessment of an individual’s functioning, considering not only physical issues but also personal and environmental factors as vital mediators. Therapists integrated these elements to create person-centered interventions that addressed impairments, facilitated the development of meaningful goals, and enhanced the individual’s functional capacity within their specific environment.
Mismatch between patient and therapist
While many of the papers in our synthesis acknowledged the importance of personal perspectives in adopting a person-centered approach to health care, recent research papers in our sample showed a mismatch between patients’ and therapists’ perspectives. For instance, physiotherapists and patients assigned different meanings to exercise and physical activity, with physiotherapists often prioritizing biomedical aspects. Similarly, formal outcome measures often failed to capture patients’ highly valued personal and contextual recovery factors beyond motor aspects. Researchers explained that recognizing these disparate notions is essential for a comprehensive understanding of recovery, and the ICF can help broaden physiotherapists’ focus.
In summary, the “Striking a balance” theme highlights the importance of navigating the complex interplay of diverse perspectives in order to foster a holistic, person-centered approach to care.
Power of participation ()
Across the sample, we detected limited thinking about and toward participation generally, with a stronger focus on impairment and, to a lesser extent, activity. This theme underscores the transformative potential of participation in harnessing the unifying capabilities of the ICF to move beyond a predominantly biomedical approach and embrace all its domains. It encompasses four subthemes: Is practice as biopsychosocial as physiotherapists think it is? ICF is a unifying framework; Beyond body functions and body structures; and Reorienting the model.
Is practice as biopsychosocial as physiotherapists think it is?
Some authors indicated a stark contrast between espoused biopsychosocial ideals and the reality of physiotherapy practice; others revealed it within their own work. This disparity resulted in errors and potential misunderstandings (see Endorsed but not embedded). For instance, while acknowledging that the ICF enabled holistic evaluation, facilitating the selection of patient-specific goals and interventions, some case reports did not consider contextual factors. Certainly, presentation of musculoskeletal conditions fits within a biomedical model; however, authors missed opportunities to adopt a broader, biopsychosocial perspective. This disconnect highlighted the need to move away from perpetuating biomedical thinking and instead embrace a more comprehensive outlook.
ICF is a unifying framework
The ICF serves as a unifying framework that transcends disciplinary boundaries and geographical settings, providing a comprehensive understanding of health-related states (World Health Organization, Citation2002). Rooted in a biopsychosocial perspective, the ICF was acknowledged to facilitate a shift from concentrating solely on disablement to enabling individuals. Moreover, we found that, when used, the ICF’s visually intuitive unifying representation enhanced its effectiveness in conveying information completely, accurately, and in an accessible format.
Beyond body functions and body structures
Several authors emphasized that promoting functioning and participation involves consideration of factors across all ICF components. By shifting the focus from viewing disability as a static process to understanding it as a dynamic interaction, therapists were able to gain a broader view of individuals’ abilities. Furthermore, embracing ICF principles was said to allow physiotherapists to fulfill both moral and legal obligations, prioritizing wellbeing and overall quality of life.
Reorienting the model
Researchers proposed innovative ways to rethink the ICF model, explicitly shifting the focus from impairment toward participation. One suggestion involved “reading” the model from right-to-left to begin the examination process with life goals and functionally based activities. Another approach suggested flipping the model upside down, emphasizing the influence of an individual’s circumstances on their health and wellbeing and the need for participatory-focused interventions and tools.
In conclusion, the “Power of Participation” theme highlights the imperative of moving beyond a predominant biomedical perspective within physiotherapy practice. It underscores the ICF’s potential as a unifying framework; one that facilitates the transition from impairment-focused thinking to holistic enablement, placing participation at the core of a more comprehensive outlook on patient wellbeing.
Moving forward ()
The final major theme in our analysis encompasses three subthemes that collectively offer many strategies for catalyzing a transformative shift to promote and embed the use of the ICF in physiotherapy: How to create transformative shift; Changes needed across education and policy; and The importance of research.
How to create transformative shift
To effectively incorporate the ICF framework into physiotherapy practice, authors recommended an incremental approach when introducing its concepts and terminology so as to optimize accessibility. It was suggested that therapists interested in integrating the ICF into their clinical practice should embrace the ICF’s conceptual model to document their clinical decision-making process, rather than being deterred by any perceived complexity regarding its classification and coding system. This shift in thinking fundamentally depends on familiarity with the model, related vocabulary and underlying definitions. See WTP theme for valued ICF contributions to clinical practice.
Key strategies for maximizing the ICF’s potential in advancing physiotherapy practice included promoting interprofessional collaboration, clarifying intersections in assessment and treatment planning, developing effective assessment tools, and ensuring reliable data dissemination. There was also a call for creating interventions and tools that reflect the participatory aspect of exercise and physical activity. Additionally, authors emphasized the importance of partnerships with individuals with disabilities and human rights activism to foster a more informed, person-centered approach in physiotherapy. This broader outlook aims to cultivate awareness and inclusivity within physiotherapy.
Changes needed across education and policy
Authors advocated for significant changes in physiotherapy education, proposing that including the ICF and its resources would enhance students’ clinical reasoning, research-practice links, and understanding of socio-political-cultural perspectives. They recommended methods such as incorporating disability experiences to foster empathy and critical thinking, especially in collaboration with individuals with disabilities.
Fieldwork plays a pivotal role in physiotherapy education, allowing students to consolidate and extend their academic learning. Placements were suggested as opportunities for students to engage with the ICF, thereby boosting their confidence and competence in its application. Furthermore, there was an emphasis on enhancing critical thinking and decision-making skills before embarking on fieldwork to address concerns raised by clinical educators regarding students’ reasoning capacity. Authors also acknowledged a gap in clinical educators’ understanding of the ICF, which might be transmitted to students. They suggested using ICF language in student assessment documents and offering ICF training for therapists to bridge this knowledge gap.
The ICF’s potential to drive policy change was recognized, as it encourages exploration of non-traditional treatments and changes to service delivery methods. Papers focused on disability underscored the importance of adopting a socio-political perspective and engaging in political activism to address health policy issues.
The importance of research
The significance of research emerged as a vital aspect of advancement, encompassing three main aspects: its purpose, application and dissemination.
Purpose
Integrating the ICF framework into physiotherapy research was recommended to enhance understanding and care for individuals managing health conditions. Specific suggestions involved incorporating research questions related to patient and consumer perspectives and their inclusion in care plans, utilizing the ICF Dictionary to provide precise terms for indexing and searching research databases, and, in the context of physiotherapy’s pivotal role in physical activity and exercise, exploring epigenetic adaptations through the lens of the ICF framework.
Application
Some authors supported the specific application of the ICF in research. Recommendations included the use of shared outcome measures in research and clinical settings and advocating for the development of outcome measures for specific ICF domains and qualifiers (e.g., participation).
Dissemination
In this synthesis, there was a recommendation for physiotherapists to drive significant changes across various aspects of ICF-related research such as: the establishment of translational research agendas, standardized clinical case reporting anchored in the ICF framework, making better use of the ICF’s consistent terminology across research and practice domains to facilitate seamless knowledge transfer, and the pivotal role physiotherapists might play disseminating information about the ICF and its resources.
In conclusion, this final theme encapsulates strategies for promoting and embedding the use of the ICF in physiotherapy: initiating transformative shifts, implementing changes in education and policy, and emphasizing the role of research. The findings indicate that to advance, physiotherapy should gradually embrace the ICF, advocate for education reform, and leverage research to unlock the framework’s potential for enhancing patient care and rehabilitation outcomes.
Discussion
Collectively, these five themes illustrate the evolving role of the ICF in physiotherapy over the previous two decades. The first theme Ways of thinking and practicing highlights the ICF’s alignment with professional philosophies. However, the Endorsed but not embedded theme reveals the challenges inhibiting widespread integration of the framework. Striking a balance emphasizes the ICF’s role in harmonizing diverse perspectives, Power of participation calls for a holistic shift and Moving forward provides a roadmap for its transformative potential. Together, they underscore the ICF’s potential for shaping the future of physiotherapy practice, education, and research.
While the ICF has a theoretical underpinning, its primary strength is its diverse application potential. Application was a key focus of much of our sample, including clinical reasoning, goal setting and outcome measure selection. A core benefit is the ICF’s ability to connect and align various facets of physiotherapy practice from assessment through to intervention. The ICF’s integrative feature is supported by its universal language, facilitating connections with other disciplines and enhancing healthcare integration. However, given that physiotherapy tends to be a pragmatic profession, we are surprised that the ICF does not feature more frequently in physiotherapy research, education or practice. To an extent this may be attributed to our research question and inclusion/exclusion criteria, but the literature base is still small for a two-decade period. Another possible reason is the degree to which the profession supports the ICF globally and across sectors. The ICF is embedded within World Physiotherapy’s Physiotherapist Education Framework (World Physiotherapy, Citation2021), specifically that clinical reasoning should identify areas of the ICF to guide physiotherapy assessment, diagnosis and intervention. Yet, World Physiotherapy’s members vary in terms of how explicitly they express this within their own chapters and regions. For example, the American Physical Therapy Association published an endorsement of the ICF, stating “The American Physical Therapy Association endorses the World Health Organization’s International Classification of Functioning, Disability and Health (ICF). ICF language shall be incorporated into all relevant Association publications, documents, and communications through existing planned review and revision cycles” (American Physical Therapy Association, Citation2020). Conversely, a search of the Australian Physiotherapy Association’s website reveals a handful of newsletter articles that reference the ICF yet nothing from a higher organizational level. Given these disparate positions, the ICF’s limited depiction in physiotherapy literature and its scattered international uptake is perhaps less surprising.
The ICF affords a holistic view of health and wellbeing – both strengths and needs – and this broad perspective helps to facilitate consideration of various roles within the interdisciplinary team. Working alongside other disciplines, which is supported via the application of the ICF (World Health Organization, Citation2010), was rarely reported in the studies we analyzed, although some authors mentioned that physiotherapy intervention fit within a broader team of either healthcare professionals or an educational setting (e.g., Baker, Dominguez, and Perdomo, Citation2018; Congdon et al., Citation2010; Falvey and Crankshaw, Citation2015; Furze et al., Citation2013; Goldstein, Cohn, and Coster, Citation2004). Conversely, there were cases where consultation with or referral to other team members was not considered in spite of very real needs, usually, but not always, because of the patient’s lack of health insurance (e.g., Baker, Dominguez, and Perdomo, Citation2018; Brady, Citation2013; Congdon et al., Citation2010). For example, in one case (Baker, Dominguez, and Perdomo, Citation2018) the patient had significant upper quadrant musculoskeletal, neuromuscular and cardiopulmonary limitations associated with the medical and surgical treatment of stage IV thyroid cancer, with associated speech and swallowing disorders but was not referred to a speech-language pathologist. The lack of mention of interdisciplinary collaboration may have been an artifact of our search strategy, which was restricted to physiotherapy alone, although it is reasonable to expect physiotherapists to consider teamwork, especially as part of contemporary practice.
Physiotherapy, closely aligned with medicine, has traditionally embraced a biomedical approach to health (Nicholls, Citation2018; Nicholls and Gibson, Citation2010). In today’s evolving healthcare landscape, which increasingly emphasizes the biopsychosocial model, questions arise regarding how physiotherapy understands and incorporates this new paradigm into its practice and research. Some scholars have identified issues within physiotherapy, including an oversimplified, reductionist understanding, a tendency to overlook cultural, social and interpersonal factors, and feeling ill-equipped to fully embrace a biopsychosocial approach (Butler, Evans, Greaves, and Simpson, Citation2004; Cormack, Stilwell, Coninx, and Gibson, Citation2022; Coronado and Bialosky, Citation2017; Daluiso-King and Hebron, Citation2022; Gervais-Hupé, Filleul, Perreault, and Hudon, Citation2023; Mescouto, Olson, Hodges, and Setchell, Citation2022; Wallden, Citation2015). To address this, scholars have suggested behavior change techniques (Gervais-Hupé, Filleul, Perreault, and Hudon, Citation2023) and reevaluation of the biopsychosocial model (Cormack, Stilwell, Coninx, and Gibson, Citation2022; Daluiso-King and Hebron, Citation2022; Mescouto, Olson, Hodges, and Setchell, Citation2022). Surprisingly, adoption of the ICF, with its inherent biopsychosocial framework, has not been proposed by these scholars. Moreover, there is a body of literature in both physiotherapy specifically (i.e., this sample) and health care more generally (Iezzoni and Freedman, Citation2008; Üstün et al., Citation2003; van der Veen et al., Citation2023) that suggests that the ICF embodies the paradigm shift advocated by physiotherapy scholars. While some may argue for focusing on the biopsychosocial model, the ICF explicitly addresses the often-overlooked contextual factors.
Despite an international increase in ICF implementation (Leonardi et al., Citation2022) and its proven versatility in clinical practice, public health, health information and health sciences (Cieza and Kostansjek, Citation2021), implementation levels remain low globally (Leonardi et al., Citation2022). Physiotherapy also appears to lag behind, with a noticeable gap between theory and practice. Bridging this gap requires synthesizing existing recommendations and connecting both bodies of literature, translating findings into research, practice and education, and critically examining the profession’s underlying assumptions (Barradell, Citation2021; Ghul and Marsh, Citation2013; Gibson, Nicholls, Setchell, and Synne Groven, Citation2018; Nicholls, Citation2018; Nicholls and Gibson, Citation2010; Shaw and deForge, Citation2012). The ICF, with its paradigm-shifting potential, presents a compelling case for this transformation.
Person centered practice is another theoretical concept that shares the ICF’s philosophical intentions related to enablement, the need for a therapeutic alliance and tailored individual approaches. Like the profession’s utilization and enactment of a biopsychosocial approach, the willingness and capabilities of physiotherapists to enact or achieve person-centered practice are considered to be mixed (Mudge, Stretton, and Kayes, Citation2014; Naylor, Killingback, and Green, Citation2023). Such literature provides further support to the profession for the need to critically revisit what the profession is and what it does.
It was interesting to note that some authors within our sample either advocated for or developed different ways to represent the ICF. There are similar suggestions in other ICF literature (Heerkens et al., Citation2018; Mitra and Shakespeare, Citation2019; Ravenek et al., Citation2013; Simon and Kraus de Camargo, Citation2019; Sykes, Maribo, Stallinga, and Heerkens, Citation2021). The proffered reasons for new representations seem to be researcher preference (Danneels et al., Citation2011), to aid clarity or shift understanding (Ramsey, Preston, Barredo, and Lehman, Citation2019; Ravenek et al., Citation2013; Simon and Kraus de Camargo, Citation2019; Stennett, de Souza, and Norris, Citation2021), to address weaknesses of the ICF (Heerkens et al., Citation2018; Mitra and Shakespeare, Citation2019; Ravenek et al., Citation2013; Sykes, Maribo, Stallinga, and Heerkens, Citation2021) and to incorporate the ICF with other models (evidently to enhance the value of the ICF on its own) (Rundell, Davenport, and Wagner, Citation2009a; van der Veen et al., Citation2023).
The existing ICF framework is deceptively simple yet unfortunately can be associated with considerable confusion. Notably, the work of Ramsey, Stennett and their respective colleagues offers potentially valuable insights for future exploration. Their re-representations stay true to the intention of the ICF and include all original framework elements without altering their descriptions. Specifically, Ramsey and her team proposed a novel perspective by inserting an arrow to prompt a right-to-left reading of the model (Ramsey, Preston, Barredo, and Lehman, Citation2019). This alteration changes the focus of understanding, shifting attention from impairment to emphasize participation. In a similar vein, Stennett, De Souza, and Norris (Citation2021) flipped the ICF representation upside down, directing attention toward contextual factors. This approach shifts the focus toward the individual and their unique circumstances, instead of emphasizing the diagnosis. Both re-representations have the potential to enhance physiotherapy practice and education, fostering a more person-centered and holistic approach, which aligns with the biopsychosocial principles of the model.
Notably, Simon and Kraus de Camargo’s (Citation2019) combine both these actions, offering a comprehensive perspective on the ICF. Additionally, the Contexts of Participation tool (Ghul and Marsh, Citation2013) focuses on participation and relates it to WHO social determinants of health (Marmot et al., Citation2010), encouraging students to explore their own assumptions and patients’ personal and environmental factors in various scenarios. These innovative re-representations open up exciting possibilities for advancing the utility and understanding of the ICF in physiotherapy.
While extensive ICF resources are available through the WHO ICF website, and ICF training is often included in high-income country university programs, its integration into core curricula remains limited (Leonardi et al., Citation2022). We firmly advocate for the full integration of ICF content into entry-level physiotherapy curricula, with a goal for graduates to instinctively employ the ICF to drive meaningful change. Although literature on ICF integration into core health and social care programs is scarce, a growing body of papers offers valuable insights (e.g., de Brouwer et al., Citation2017; Geertzen, Rommers, and Dekker, Citation2011; Scholten, Barradell, Bickford, and Moran, Citation2021). Additionally, papers specific to physiotherapy (Sandborgh et al., Citation2018; Xiaofei, Zhouying, Hongwei, and Anqiao, Citation2022) enrich our understanding. Those relating to the application of the ICF to interprofessional learning are also noteworthy (Johnson et al., Citation2020; Moran, Bickford, Barradell, and Scholten, Citation2020; Nguyen, Fayed, Gorter, and Macdermid, Citation2016; Skarakis-Doyle and Doyle, Citation2008; Stephenson and Richardson, Citation2008). To fully unlock the ICF’s potential, it is essential to establish alignment between classroom learning and practical experiences, which necessitates the education and support of clinical educators. This alignment should prioritize repeated, developing exposure (Moran, Bickford, Barradell, and Scholten, Citation2020; Scholten, Barradell, Bickford, and Moran, Citation2021) and the critical questioning of assumptions (Roush and Sharby, Citation2011; Williams et al., Citation2019). Furthermore, it is imperative that professional organizations responsible for shaping the standards of physiotherapy education and entry-level competencies take explicit measures to incorporate the ICF framework into their documentation and assessment criteria, thereby advancing the quality of education and practice in the field.
Implications
The ICF aligns with professional philosophies and its strength lies in its versatility, connecting various facets of physiotherapy practice, education and research. Collaboration among World Physiotherapy regions and members would help to align and target priorities across areas of the physiotherapy profession. Endorsement of the ICF by all World Physiotherapy member organizations, together with explicit and consistent appearance of related material in member publications, is vital. The understanding that the ICF provides would enhance the profession’s desire for greater uptake of a biopsychosocial approach and the ensuing benefits to patient care.
Support from regulators, accrediting and other professional bodies would also help to enact change, particularly in entry-level education. To harness the ICF’s full potential, embedding its principles in physiotherapy curricula is crucial. The ICF should be a concept that students are repeatedly exposed to in both classroom and placement/fieldwork activities. Physiotherapy students become future educators and by signaling that the ICF is important, they are more likely to take this into their own practice.
The ICF is relevant to all health professions, and physiotherapy can learn from, with and alongside its interdisciplinary counterparts. While this research focuses on physiotherapy, the implications extend to other healthcare and rehabilitation disciplines. There is a need to connect existing ICF literature and related models and integrate the ICF’s language and philosophy into the education and practice of various rehabilitation fields.
Limitations
We chose to include papers that referenced the ICF in relation to physiotherapy practice, acknowledging that some papers using ICF-related terms might have been missed. While our search tended to capture literature that focused on certain isolated domains such as participation, we excluded such literature unless it related to the whole framework in some way. Nonetheless, we conducted a comprehensive search across relevant databases to ensure a valuable sample for analysis.
Our focus on papers solely related to physiotherapy might have excluded those involving physiotherapists in interdisciplinary teams. While this choice may have influenced our interpretations, it was made to understand how the physiotherapy profession thought about and utilized the ICF; an initial screen of interdisciplinary literature revealed challenges in discerning how the ICF was understood by specific disciplines. Furthermore, our sample of 37 papers is considered large for a qualitative synthesis; expanding it with interdisciplinary team papers would have been impractical and less meaningful.
Our synthesis was restricted to literature from our search strategy (i.e., not gray literature) and papers published in English, but papers were from a mix of countries (despite the frequency of studies from North America).
Conclusion
In this systematic qualitative synthesis, the ICF framework has emerged as a valuable tool for the physiotherapy profession over the past two decades, signifying five key themes. These themes underscore its alignment with professional principles, widespread endorsement but incomplete integration, potential to harmonize diverse perspectives, a call for a holistic shift, and a roadmap for transformative impact.
The ICF’s strength lies in its versatility, connecting various facets of physiotherapy practice, education and research, from clinical reasoning to goal setting and outcome measurement, and extending its reach to interdisciplinary collaboration. However, its presence in physiotherapy literature and practice remains limited, perhaps due to varying global and sectoral support within the profession.
The ICF’s holistic perspective on health and wellbeing aligns with contemporary healthcare trends. However, physiotherapy’s historical biomedical focus poses challenges in embracing biopsychosocial models and person-centered practices, demanding critical examination of the assumptions that underpin the profession’s approach and a commitment to change. Some authors propose alternative ICF representations that emphasize participation and contextual factors, potentially fostering a more holistic approach and offering opportunities to shift the focus toward participation and contextual factors.
To harness the ICF’s full potential, embedding its principles in physiotherapy curricula is crucial. This will prepare future professionals to drive transformative change, entailing collaboration, interprofessional learning, and support from professional bodies.
In summary, the ICF framework is established as a valuable framework in physiotherapy and offers a holistic perspective with diverse applications. However, further integration requires concerted efforts in education, policy and research. The ICF can facilitate a transformative shift in physiotherapy, aligning the profession more closely with contemporary healthcare paradigms and promoting person-centered, biopsychosocial practice.
Acknowledgments
We extend sincere thanks to librarian Shannon Brown of Flinders University, who provided advice and conducted the database searches.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- *= literature included in the sample
- Alford V, Remedios L, Webb G, Ewen S 2013 The use of the International Classification of Functioning, Disability and Health (ICF) in indigenous healthcare: A systematic literature review. International Journal for Equity in Health 12: 32.
- Allet L, Bürge E, Monnin D 2008 ICF: Clinical relevance for physiotherapy? A critical review. Advances in Physiotherapy 10: 127–137.
- American Physical Therapy Association. 2020 Endorsement of International Classification of Functioning, Disability and Health. https://www.apta.org/apta-and-you/leadership-and-governance/policies/endorsement-icf
- Atama T, Leclair L, Pooyania S, Barclay R 2022 Stroke survivors and their physiotherapists’ perceptions of recovery: A multiple methods approach*. Physiotherapy Canada: 11. 10.3138/ptc-2021-0068
- Atkinson HL, Nixon-Cave K 2011 A tool for clinical reasoning and reflection using the International Classification of Functioning, Disability and Health (ICF) framework and patient management model*. Physical Therapy 91: 416–430.
- Baker J, Dominguez JF, Perdomo M 2018 The International Classification of Functioning, Disability, and Health model guides individualized care for a patient with cancer: A case report*. Rehabilitation Oncology 36: E1–E8.
- Barradell S 2021 Caring in and for physiotherapy through stewardship. Physiotherapy Theory and Practice 37: 663–671.
- Barradell S, Barrie S, Peseta T 2018 Ways of thinking and practicing: Highlighting the complexities of higher education curriculum. Innovations in Education and Teaching International 55: 266–275.
- Brady C 2013 Use of the International Classification of Functioning, Disability, and Health as a framework for clinical reasoning in the care of an older adult with advanced Parkinson Disease*. Academy of Geriatric Physical Therapy 20: 20–24.
- Butler CC, Evans M, Greaves D, Simpson S 2004 Medically unexplained symptoms: The biopsychosocial model found wanting. Journal of the Royal Society of Medicine 97: 219–222.
- Cieza A, Kostansjek N 2021 The International Classification of Functioning, Disability and Health: The first 20 years. Developmental Medicine & Child Neurology 63: 363–363.
- Congdon WV, Ghazinouri R, Doshi S, Sykes C, Abraham J 2010 Application of the ICF model in the acute care physical therapy management of a young man with pelvic chondrosarcoma following internal hemipelvectomy: A case report*. Rehabilitation Oncology 28: 3–9.
- Constand MK, Macdermid JC 2014 Applications of the International Classification of fFunctioning, Disability and Health in goal-setting practices in healthcare. Disability and Rehabilitation 36: 1305–1314.
- Cormack B, Stilwell P, Coninx S, Gibson J 2022 The biopsychosocial model is lost in translation: From misrepresentation to an enactive modernization. Physiotherapy Theory and Practice 39: 2273–2288.
- Coronado RA, Bialosky JE 2017 Manual physical therapy for chronic pain: The complex whole is greater than the sum of its parts. Journal of Manual and Manipulative Therapy 25: 115–117.
- Dalboni GL, Garcêz RL, Assis ÍC, Vaz DV 2022 Conceptions of disability among physiotherapists: An exploratory qualitative study*. Physiotherapy Theory and Practice 39: 1662–1671.
- Daluiso-King G, Hebron C 2022 Is the biopsychosocial model in musculoskeletal physiotherapy adequate? An evolutionary concept analysis. Physiotherapy Theory and Practice 38: 373–389.
- Danneels L, Beernaert A, De Corte K, Descheemaeker F, Vanthillo B, Van Tiggelen D, Cagnie B 2011 A didactical approach for musculoskeletal physiotherapy: The planetary model*. Journal of Musculoskeletal Pain 19: 218–224.
- Darrah J 2008 Using the ICF as a framework for clinical decision making in pediatric physical therapy*. Advances in Physiotherapy 10: 146–151.
- Davenport TE 2015 Clinical case reporting in the peer‐reviewed physical therapy literature: Time to move toward functioning*. Physiotherapy Research International 20: 220–230.
- de Brouwer CP, van Amelsvoort LG, Heerkens YF, Widdershoven GA, Kant IJ 2017 Implementing the ICF in occupational health; building a curriculum as an exemplary case. Work 57: 173–186.
- de Kleijn-de Vrankrijker MW 2003 The long way from the International Classification of Impairments, Disabilities and Handicaps (ICIDH) to the International Classification of Functioning Disability and Health (ICF). Disability and Rehabilitation 25: 561–564.
- de Rooij IJM, van de Port IGL, van der Heijden LLM, Meijer JG, Visser-Meily JMA 2021 Perceived barriers and facilitators for gait-related participation in people after stroke: From a patients’ perspective*. Physiotherapy Theory and Practice 37: 1337–1345.
- Eliassen M, Lahelle A 2021 Enhancing functional improvement in reablement–a qualitative study*. European Journal of Physiotherapy 23: 355–361.
- Escorpizo R, Bemis-Dougherty A 2015 Introduction to special issue: A review of the International Classification of Functioning, Disability and Health and physical therapy over the years. Physiotherapy Research International 20: 200–209.
- Escorpizo R, Cieza A 2009 On “Physical therapist management…” Rundell SD, et al. Phys Ther. 2009;89: 82–90. Physical Therapy 89: 308–310.
- Escorpizo R, Stucki G, Cieza A, Davis K, Stumbo T, Riddle DL 2010 Creating an interface between the International Classification of Functioning, Disability and Health and physical therapist practice*. Physical Therapy 90: 1053–1063.
- Falvey JR, Crankshaw A 2015 Application of ICF model to a patient with home mechanical ventilation: A case report with 1-year follow-up*. Cardiopulmonary Physical Therapy Journal 26: 15–21.
- Furze J, Nelson K, O’Hare M, Ortner A, Threlkeld AJ, Jensen GM 2013 Describing the clinical reasoning process: Application of a model of enablement to a pediatric case*. Physiotherapy Theory and Practice 29: 222–231.
- Geertzen J, Rommers G, Dekker R 2011 An ICF-based education programme in amputation rehabilitation for medical residents in the Netherlands. Prosthetics and Orthotics International 35: 318–322.
- Gervais-Hupé J, Filleul A, Perreault K, Hudon A 2023 Implementation of a biopsychosocial approach into physiotherapists’ practice: A review of systematic reviews to map barriers and facilitators and identify specific behavior change techniques. Disability and Rehabilitation 45: 2263–2272.
- Geyh S, Peter C, Müller R, Bickenbach JE, Kostanjsek N, Üstün BT, Stucki G, Cieza A 2011 The personal factors of the International Classification of Functioning, Disability and Health in the literature–a systematic review and content analysis. Disability and Rehabilitation 33: 1089–1102.
- Geyh S, Schwegler U, Peter C, Müller R 2019 Representing and organizing information to describe the lived experience of health from a personal factors perspective in the light of the International Classification of Functioning, Disability and Health (ICF): A discussion paper. Disability and Rehabilitation 41: 1727–1738.
- Ghul R, Marsh I 2013 Teaching participation in occupations to first year occupational therapy students: An action research study. The British Journal of Occupational Therapy 76: 101–107.
- Gibson BE, Nicholls DA, Setchell J, Synne Groven K 2018 Working against the grain: Criticality for an otherwise physiotherapy. In: Gibson B, Nicholls D, Setchell J Synne Groven K Eds Manipulating practices: A critical physiotherapy reader, pp. 14–32. Oslo, Norway: Cappelen Damm Akademisk/Nordic Open Access Scholarly Publishing.
- Gilchrist LS, Galantino ML, Wampler M, Marchese VG, Morris GS, Ness KK 2009 A framework for assessment in oncology rehabilitation*. Physical Therapy 89: 286–306.
- Goldstein DN, Cohn E, Coster W 2004 Enhancing participation for children with disabilities: Application of the ICF enablement framework to pediatric physical therapist practice*. Pediatric Physical Therapy 16: 114–120.
- Heerkens YF, de Weerd M, Huber M, de Brouwer CP, van der Veen S, Perenboom RJ, van Gool CH, Ten Napel H, van Bon-Martens M, Stallinga HA, et al. 2018 Reconsideration of the scheme of the International Classification of Functioning, Disability and Health: Incentives from the Netherlands for a global debate. Disability and Rehabilitation 40: 603–611.
- Heerkens Y, van der Brug Y, Ten Napel H, Van Ravensberg D 2003 Past and future use of the ICF (former ICIDH) by nursing and allied health professionals. Disability and Rehabilitation 25: 620–627.
- Helgeson K, Smith AR Jr 2008 Process for applying the International Classification of Functioning, Disability and Health model to a patient with patellar dislocation*. Physical Therapy 88: 956–964.
- Iezzoni LI, Freedman VA 2008 Turning the disability tide: The importance of definitions. JAMA 299: 332–334.
- Jette AM 2005 Editor’s note. The changing language of disablement*. Physical Therapy 85: 118–119.
- Jette AM 2006 Toward a common language for function, disability, and health*. Physical Therapy 86: 726–734.
- Jiandani MP, Mhatre BS 2018 Physical therapy diagnosis: How is it different?*. Journal of Postgraduate Medicine 64: 69–72.
- Johnson AM, Woltenberg LN, Heinss SH, Carper R, Taylor S, Kuperstein J 2020 Whole person health: Using experiential learning and the ICF model as a tool for introductory interprofessional collaborative practice. Journal of Allied Health 49: 86–92.
- Josephson I, Bülow P, Hedberg B 2011 Physiotherapists’ clinical reasoning about patients with non-specific low back pain, as described by the International Classification of Functioning, Disability and Health*. Disability and Rehabilitation 33: 2217–2228.
- Kang TW, Cynn HS 2017 Progressive intervention strategy for the gait of sub-acute stroke patient using the International Classification of Functioning, Disability, and Health tool*. Neuro Rehabilitation 40: 473–481.
- Karlsson E, Gustafsson J 2022 Validation of the International Classification of Functioning, Disability and Health (ICF) core sets from 2001 to 2019 – a scoping review. Disability and Rehabilitation 44: 3736–3748.
- Killick L, Davenport TE 2014 Pain worlds: Towards the integration of a sociocultural perspective of pain in clinical physical therapy*. Physiotherapy Research International 19: 193–204.
- Leonardi M, Lee H, Kostanjsek N, Fornari A, Raggi A, Martinuzzi A, Yáñez M, Almborg A-H, Fresk M, Besstrashnova Y 2022 20 years of ICF—International Classification of Functioning, Disability and Health: Uses and applications around the world. International Journal of Environmental Research and Public Health 19: 11321.
- Maart S, Sykes C 2022 Expanding on the use of the International Classification of Functioning, Disability and Health: Examples and resources*. South African Journal of Physiotherapy 78: 5.
- Major CH, Savin-Baden M 2010 Qualitative research synthesis. The scholarship of integration in practice. In: Savin-Baden M Major C Eds New approaches to qualitative research. Wisdom and uncertainty, pp. 108–118. London: Routledge.
- Manns PJ, Darrah J 2006 Linking research and clinical practice in physical therapy: Strategies for integration*. Physiotherapy 92: 88–94.
- Maribo T, Petersen KS, Handberg C, Melchiorsen H, Momsen AMH, Nielsen CV, Leonardi M, Labriola M 2016 Systematic literature review on ICF from 2001 to 2013 in the Nordic countries focusing on clinical and rehabilitation context. Journal of Clinical Medicine Research 8: 1–9.
- Marmot M, Allen J, Goldblatt P, Boyce T, Mcneish D, Grady M, Geddes I 2010 The Marmot review: Fair society, healthy lives. The Strategic Review of Health Inequalities in England Post-2010. London, UK: UCL Institute of Health Equity.
- McCune V, Hounsell D 2005 The development of students’ ways of thinking and practising in three final-year biology courses. Higher Education 49: 255–289.
- Mescouto K, Olson RE, Hodges PW, Setchell J 2022 A critical review of the biopsychosocial model of low back pain care: Time for a new approach? Disability and Rehabilitation 44: 3270–3284.
- Mitra S, Shakespeare T 2019 Remodeling the ICF. Disability and Health Journal 12: 337–339.
- Momsen A, Stapelfeldt C, Rosbjerg R, Escorpizo R, Labriola M, Bjerrum M 2019 International classification of Functioning, Disability and Health in vocational rehabilitation: A scoping review of the state of the field. Journal of Occupational Rehabilitation 29: 241–273.
- Moran M, Bickford J, Barradell S, Scholten I 2020 Embedding the International Classification of Functioning, Disability and Health in health professions curricula to enable interprofessional education and collaborative practice. Journal of Medical Education and Curricular Development 7: 238212052093385.
- Mudge S, Stretton C, Kayes N 2014 Are physiotherapists comfortable with person-centred practice? An autoethnographic insight. Disability and Rehabilitation 36: 457–463.
- Naylor J, Killingback C, Green A 2023 What are the views of musculoskeletal physiotherapists and patients on person-centred practice? A systematic review of qualitative studies. Disability and Rehabilitation 45: 950–961.
- Nguyen T, Fayed N, Gorter JW, Macdermid J 2016 Enhancing interprofessional education and practice: Development and implementation of a new graduate-level course using the International Classification of Functioning, Disability, and Health. Journal of Interprofessional Care 30: 385–387.
- Nicholls DA 2018 The end of physiotherapy. Abingdon, Oxon: Routledge.
- Nicholls DA, Gibson BE 2010 The body and physiotherapy. Physiotherapy Theory and Practice 26: 497–509.
- Noblit GW, Hare RD 1988 Meta-ethnography: Synthesizing qualitative studies. Newbury Park, CA: Sage.
- Peters-Brinkerhoff C 2016 Perspectives on teaching the International Classification of Functioning, Disability, and Health model to physical therapy students*. Journal of Allied Health 45: 236–242.
- Qutishat D, Al-Yahya E, Mohammad MT, Muhaidat J, Al-Khlaifat L, Okasheh R 2021 The application of the International Classification of Functioning, Disability and Health as a framework in clinical reasoning; educators’ and graduates’ perspectives: A qualitative study*. Physical Therapy Reviews 26: 34–41.
- Ramsey CR, Preston A, Barredo R, Lehman D 2019 Using the International Classification of Functioning, Disability, and Health to guide students’ clinical approach to aging with pathology: Aging with multiple sclerosis example*. Topics in Geriatric Rehabilitation 35: 209–216.
- Ravenek M, Skarakis-Doyle E, Spaulding S, Jenkins M, Doyle P 2013 Enhancing the conceptual clarity and utility of the International Classification of Functioning, Disability & Health: The potential of a new graphic representation. Disability and Rehabilitation 35: 1015–1025.
- Roush SE, Sharby N 2011 Disability reconsidered: The paradox of physical therapy*. Physical Therapy 91: 1715–1727.
- Rundell SD, Davenport TE, Wagner T 2009a Author response*. Physical Therapy 89: 309–310.
- Rundell SD, Davenport TE, Wagner T 2009b Physical therapist management of acute and chronic low back pain using the World Health Organization’s International Classification of Functioning, Disability and Health*. Physical Therapy 89: 82–90.
- Sandborgh M, Dean E, Denison E, Elvén M, Fritz J, Wågert PVH, Moberg J, Overmeer T, Snöljung Å, Johansson A-C, et al. 2018 Integration of behavioral medicine competencies into physiotherapy curriculum in an exemplary Swedish program: Rationale, process, and review. Physiotherapy Theory and Practice 36: 365–377.
- Scholten I, Barradell S, Bickford J, Moran M 2021 Twelve tips for teaching the International Classification of Functioning, Disability and Health with a view to enhancing a biopsychosocial approach to care. Medical Teacher 43: 293–299.
- Schwab SM, Zeleznik AJ 2020 Using the language of the ICF to distinguish physical therapy and occupational therapy services in the acute care setting*. Journal of Acute Care Physical Therapy 11: 40–43.
- Shaw JA, DeForge RT 2012 Physiotherapy as bricolage: Theorizing expert practice. Physiotherapy Theory and Practice 28: 420–427.
- Shields RK, Dudley-Javoroski S 2022 Epigenetics and the International Classification of Functioning, Disability and Health model: Bridging nature, nurture, and patient-centered population health*. Physical Therapy 102. 10.1093/ptj/pzab247
- Simon L, Kraus de Camargo O 2019 The ICF in clinical practice: Case scenarios and exercises. In: Kraus De Camargo O, Simon L, Ronen G Rosenbaum P Eds ICF: A hands-on approach for clinicians and families 1st, pp. 60–75. London: Mac Keith Press.
- Skarakis-Doyle E, Doyle PC 2008 The ICF as a framework for interdisciplinary doctoral education in rehabilitation: Implications for speech-language pathology. International Journal of Speech-Language Pathology 10: 83–91.
- Stennett AM, De Souza LH, Norris M 2021 Flipping the ICF: Exploring the interplay of theory and the lived experience to reconsider physical activity in community-dwelling people with multiple sclerosis*. Frontiers in Rehabilitation Sciences 2. 10.3389/fresc.2021.7106182
- Stephenson R, Richardson B 2008 Building an interprofessional curriculum framework for health: A paradigm for health function. Advances in Health Sciences Education 13: 547–557.
- Sykes C 2008 The International Classification oF functioning,Ddisability and Health: Relevance and applicability to physiotherapy*. Advances in Physiotherapy 10: 110–118.
- Sykes CR, Maribo T, Stallinga HA, Heerkens Y 2021 Remodeling of the ICF: A commentary. Disability and Health Journal 14: 100978.
- Üstün TB, Chatterji S, Bickenbach J, Kostanjsek N, Schneider M 2003 The International Classification of Functioning, Disability and Health: A new tool for understanding disability and health. Disability and Rehabilitation 25: 565–571.
- van der Veen S, Evans N, Huisman M, Welch Saleeby P, Widdershoven G 2023 Toward a paradigm shift in healthcare: Using the International Classification of Functioning, Disability and Health (ICF) and the capability approach (CA) jointly in theory and practice. Disability and Rehabilitation 45: 2382–2389.
- vanSant AF 2006 *The International Classification of Functioning, Disability and Health. Pediatric Physical Therapy 18: 237.
- van Uem JM, Marinus J, Canning C, van Lummel R, Dodel R, Liepelt-Scarfone I, Berg D, Morris ME, Maetzler W 2016 Health-related quality of life in patients with Parkinson’s disease—a systematic review based on the ICF model. Neuroscience & Biobehavioral Reviews 61: 26–34.
- Wallden M 2015 “But we’re infinitely more complex than a car”: A systems approach to health & performance. Journal of Bodywork and Movement Therapies 19: 697–711.
- Williams G, Hassett L, Clark R, Bryant A, Olver J, Morris ME, Ada L 2019 Improving walking ability in people with neurologic conditions: A theoretical framework for biomechanics-driven exercise prescription. Archives of Physical Medicine and Rehabilitation 100: 1184–1190.
- World Health Organization 2001 International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization.
- World Health Organization 2002 ICF beginner’s guide: Towards a common language for functioning, disability and health: ICF. Geneva: World Health Organization.
- World Health Organization 2010 Framework for action on interprofessional education and collaborative practice health professions networks nursing & midwifery human resources for health. Geneva, Switzerland: World Health Organization.
- World Physiotherapy. 2019 Descriptions of physical therapy Policy Statement. https://world.physio/sites/default/files/2020-07/PS-2019-Description-of-physical-therapy.pdf
- World Physiotherapy. 2021 Physiotherapist education framework. https://world.physio/what-we-do/education/physiotherapist-education-framework
- Xiaofei X, Zhouying Q, Hongwei S, Anqiao L 2022 Development of programmes and curriculum of physical therapy at undergraduate level using ICF and rehabilitation competency framework. Chinese Journal of Rehabilitation Theory and Practice 12: 295–305.