
ABSTRACT
Peer relationship difficulties in adolescents with acquired brain injury (ABI) are under-recognized and targets for intervention are unclear. From a social constructionist position, this study aimed to engage with stakeholders to develop a collaborative understanding of peer relationship difficulties in adolescents with ABI and seek consultation on what might be required to improve them. Focus groups and semi-structured interviews were conducted with four stakeholder groups: adolescents with ABI (n = 4); parents of adolescents with ABI (n = 7); adults who sustained an ABI in adolescence (n = 2); and specialist practitioners (n = 3). Qualitative data were analysed using thematic analysis. The analysis yielded 11 themes, grouped into two domains. The first, understanding peer relationship difficulties, included themes from “exclusion and a need to belong”, to “loss of past self”. The second, supporting peer relationships, comprised themes of “building understanding” and “meaningful social connection”, amongst others. A logic model of stakeholder experiences of peer relationship difficulties was constructed. Difficulties with peers can increase vulnerability to feelings of loneliness, shame, and hopelessness for adolescents post-ABI. Stakeholders described that a meaningful intervention would be multi-layered, targeting change within the adolescent's environment and within the adolescent themselves. The presented logic model provides a framework for future intervention development.
Introduction
Adolescence represents a time for significant social development (Blakemore, Citation2008), marking the growth of independence and social identity through peer relationships, group membership, and belonging (Ownsworth, Citation2014; Tajfel, Citation1978). Consequently, adolescents may be more sensitive to peer acceptance and rejection than children or adults of working age (Steinberg & Morris, Citation2001).
Successful peer relationships in adolescence can be protective for mental health and resilience (van Harmelen et al., Citation2017). Conversely, difficulties with peers and lack of peer relationships can have significant social and emotional ramifications (Anderson et al., Citation2013), including loneliness, anxiety, and depression (Parker & Asher, Citation1987). Those with reduced social skills, physical disabilities, and difficulties with mood are at higher risk of peer rejection (King et al., Citation2010; Olweus, Citation1993; Vannatta et al., Citation2009). One of the groups at higher risk of difficulties establishing and maintaining peer relationships is persons with acquired brain injury (ABI).
ABI is a leading cause of death and disability worldwide (World Health Organisation, Citation2006), with an annual incidence rate in England of 400 per 100,000 for children younger than 15 years (Hospital Episode Statistics, Citation2013). ABI refers to several injury mechanisms that disrupt brain integrity after birth and can result in persistent physical, cognitive, emotional, social, and behavioural impairments (Anderson et al., Citation2011). Common causes of ABI include traumatic brain injury (TBI), caused by falls, assaults, and road traffic accidents; and non-traumatic injuries, caused by stroke, infection, hypoxia, and tumours (Barber et al., Citation2018).
The sequelae of ABI can be far-reaching, and those with ABI may have difficulties with fatigue, attention (Catroppa et al., Citation2011), self-awareness (Lloyd et al., Citation2021), executive functioning (Wade et al., Citation2010), memory (Mandalis et al., Citation2007), processing speed, intelligence (Anderson et al., Citation2012), communication (Turkstra et al., Citation2014), social functioning (Greenham et al., Citation2018), behaviour (Cole et al., Citation2008), and emotion regulation (Vasa et al., Citation2015). A further concern for persons with ABI is often the lack of physical evidence of disability, and therefore the “hidden” or “invisible” nature of the associated difficulties (Simpson et al., Citation2002). This may result in limited support and understanding from educational, social, and family environments (Keetley et al., Citation2019).
Consequently, children and adolescents with ABI may follow a different developmental trajectory to their peers and face secondary consequences for reduced quality of life (QoL). These include difficulties with identity, mood, and relationships; alongside future challenges with education, occupation, and criminal justice (Anderson et al., Citation2009; Arroyos-Jurado et al., Citation2006; Sariaslan et al., Citation2016; Williams, Citation2012). Research into the social outcomes of adolescents with ABI is expanding (Sirois et al., Citation2019; Tousignant et al., Citation2018); however, there is a scarcity of research exploring the intricacies of peer dynamics, which remain poorly understood.
Qualitative insights into peer relationships for adolescents with ABI have recently been reported in the context of identity change and adjustment post-injury. Conducting individual interviews with adolescents and their mothers, Glennon (Citation2019) identified “peer relatedness” to be important for the perception of the self of adolescents with ABI. Interestingly, explanations of perceived changes in identity for adolescents centred around accounts involving social relationships rather than parent relationships. Four of six adolescents spoke of peer rejection or friend withdrawal which was echoed by parents. This was reported to be a threat to self-identity with adolescents questioning their normalcy post-injury, particularly in the context of how they were perceived by others. Strategies for “fitting in” to support peer relatedness were described from adolescent accounts, such as using online forums. This study has provided important insights into how adolescents perceive their peer relationships post-injury and their role in self-identity. However, due to the focus of the study, opinions about the possible determinants for peer rejection or friend withdrawal were not explored in depth.
To understand the determinants of peer relationship difficulties following ABI, the underlying processes for adequate social functioning must be considered. The Socio-Cognitive Integration of Abilities Model (SOCIAL; Beauchamp & Anderson, Citation2010) offers a biopsychosocial framework to understand the development of the social skills needed to build and maintain peer relationships throughout childhood and adolescence. The model raises important considerations for the emergence of social skills, mediated by typical brain development within a supportive family and social environment. The SOCIAL model suggests that the integrity of social skills is determined by adequate cognitive functioning, including attention and executive functioning, communication, and social cognition. The latter, referring to the ability to perceive and appropriately respond to the emotions of others, is supported by the theory of mind. This in turn facilitates the ability to understand the intentions, beliefs, and emotions of others, and respond with empathy (Adolphs, Citation1999).
Within the SOCIAL model, social skills encompass three social constructs which can be viewed alongside the International Classification of Functioning, Disability and Health (ICF) framework of disability: (a) social competence (i.e., function); (b) social adjustment (i.e., activity); and (c) social participation (i.e., participation; Anderson & Beauchamp, Citation2012). Social competence refers to the child's coordination of multiple sensory processes and resources in interactions to meet social demands (Anderson et al., Citation2013; Yeates et al., Citation2007), allowing for the development and maintenance of peer relationships over time (Iarocci et al., Citation2007). Social adjustment is defined as the degree to which children can adapt their social behaviour to perform competently (Crick & Dodge, Citation1994). Finally, social participation encompasses the number and quality of valued activities a child engages in with others in social environments (Fougeyrollas et al., Citation1998; Wade et al., Citation2018).
Children and adolescents with ABI have been reported to have difficulties with social skills, including the theory of mind (Turkstra et al., Citation2004), empathy (Dennis et al., Citation2013), and social participation, competence, and adjustment (Anderson et al., Citation2013; Sirois et al., Citation2019; Yeates et al., Citation2014) which can impact peer relationships. Yeates et al. (Citation2013) found that children with severe TBI (8–13 years) were reported by classmates to experience higher peer rejection-victimization than those with orthopaedic injuries and were less likely to have mutual friendships. The authors reported that this placed those with severe TBI at long-term risk of poorer psychological adjustment and quality of life due to a lack of reciprocal friendships. Indeed, it has previously been reported that the psychological difficulties associated with peer rejection may be protected against if children and adolescents with ABI have at least one friend (Heverly-Fitt et al., Citation2014).
Although the difficulties with social skills for children and adolescents with ABI are beginning to be investigated, what is less clear in the evidence-base is how to improve them, due to a dearth of intervention studies.
To support intervention efficacy for adolescent populations, it has been suggested that the use of peer coaches may promote greater influence on adolescent participants when compared to adults due to similarities in characteristics (e.g., shared interests; Braga et al., Citation2012). Using peer coaching, Wade et al. (Citation2018) piloted an app-based intervention to help adolescents (14–22 years) attain social participation goals across 10 coaching sessions. Post-intervention, participants reported higher levels of confidence in their social participation and viewed the coaching provided positively. However, it was reported that participants did not rate the programme as very useful overall. Technical challenges with the app were reported, which may have impacted upon participant perceptions of the programme, despite their positive experience of the coaching that they received.
Barrera et al. (Citation2018) conducted an RCT to explore the efficacy of a social skills intervention on outcomes of social competence and QoL in young brain tumour survivors (8–16 years). This was an eight-week group-based intervention and included topics such as friendship making, managing bullying, conflict resolution, and empathy. Those in the experimental group showed significant improvements in self-rated empathy scores when compared to control participants. However, no intervention effect was observed in parent and teaching ratings of empathy, or on outcomes of QoL.
In a systematic review conducted with a non-ABI neurodevelopmental population, Andrews et al. (Citation2015) found adequate to strong evidence for the effectiveness of community integration interventions on community participation outcomes (including peer relationships), self-esteem, and QoL in children and adolescents. The authors recommended that participants should complete interventions with typically developing peers, and that future interventions should facilitate friendships alongside recreational participation and work on both individual (social skills) and environmental (community support) factors to support participation.
Research within paediatric neuropsychology is beginning to explore the social skills needed for peer relationships post-ABI; however, targets for intervention remain unclear and intervention efficacy is inconsistent. Although evidence for improving peer relationships through community integration has been identified in neurodevelopmental populations (Andrews et al., Citation2015), the presentation of adolescents with ABI may differ. The additional difficulties associated with ABI, such as loss of identity (Ownsworth, Citation2014), lack of understanding from others (Keetley et al., Citation2019), impaired self-awareness (Lloyd et al., Citation2021) and “hidden” difficulties (Simpson et al., Citation2002), and their impact on peer relationships remain largely unknown.
To inform the identified gaps in the evidence-base, there is a need to work with stakeholders (i.e., service users and providers) to understand the complexities of peer relationship difficulties for adolescents with ABI, the impact of these, and what might be needed to improve peer relationships. This “bottom up” approach would allow for the co-development of a meaningful intervention to support peer relationships and QoL post-ABI and could provide insights into the intervention priorities for stakeholders. Indeed, interpersonal relationships have previously been reported to be the highest priority for adolescents with TBI (Sirois et al., Citation2014).
Guidance from the Medical Research Council (MRC) for the development of complex interventions to promote worthwhile effects has recently been updated (Skivington et al., Citation2021). In the development process, existing evidence for intervention should be considered and relevant theories identified or developed, supplemented with new research with stakeholders, if necessary. In line with MRC guidelines, the intervention mapping (IM) framework (Bartholomew-Eldredge et al., Citation2016) offers a structured and iterative protocol that guides the co-design of health promotion interventions through systematic engagement with stakeholders. This ensures that the intervention suits the population need and context (Fernandez et al., Citation2019; Kok et al., Citation2015). IM comprises six steps, which provide a map for intervention design, supported by theoretical and empirical knowledge (O’Connor et al., Citation2018). IM has previously been used to improve social networks for diabetes management in minority families (Vissenberg et al., Citation2017), and communication between hospital staff and disabled children (Gumm et al., Citation2017).
A logic model is developed in step one of IM. This offers a framework to describe and understand the target problem for intervention, its impact on QoL, and its determinants. An environmental approach is used to identify determinants at an individual, community, and social level. This process includes (1) involving stakeholders; (2) searching empirical literature to identify determinants of behaviour; (3) identifying theories on determinants; and (4) conducting research to explore unanswered questions (Fernandez et al., Citation2019). In contrast to the traditional use of logic models (i.e., input and output), the logic model used by IM provides a visual representation of possible influential determinants for the target problem, and the relationships between them.
To guide future intervention development for peer relationship difficulties in adolescents with ABI (i.e., the target problem), the influential determinants need to be understood. Due to the scarcity of research exploring the intricacies of peer dynamics post-ABI, engagement with stakeholders promotes the suitability of any future intervention for the population served. Understanding stakeholder experiences can inform the gap within the paediatric neuropsychology literature and support the development of a logic model of the problem (step one of IM).
Aims and research questions
This study aimed to: (a) develop a collaborative understanding of peer relationships for adolescents with ABI; and (b) to seek the views of adolescents and other key stakeholders on what might be needed to improve them, and what the intervention goals might be. This study's methodology was guided by the IM protocol.
The following research questions (RQs) were proposed:
How are peer relationships in adolescence following ABI described by stakeholders?
What do stakeholders believe are the key determinants of peer relationship difficulties in adolescence following ABI?
What do stakeholders think needs to change to improve peer relationships in adolescents with ABI?
What do stakeholders think the intervention goals should be?
Methodology
Design
Qualitative methodology was employed using both focus groups and individual interviews. This methodology is well suited to the study as it can consider what is meaningful to stakeholders and can explore reported experiences in depth.
Thematic analysis (TA; Braun & Clarke, Citation2006, Citation2013) was the chosen method of data analysis as the study endeavoured to identify commonalities within stakeholder experiences and perspectives. Through TA, the researcher systematically identifies the salient themes or patterns of meaning that emerge from data items, alongside researcher reflexivity and judgement, which are then compared across the data set. Themes are not “discovered” but actively crafted to capture something important within the data that is relevant to the RQs (Braun & Clarke, Citation2006; Citation2016; Citation2019; Joffe, Citation2012).
Participants
Planning group
In line with IM protocol, a planning group (co-authors) was established comprising four clinical researchers within the field of speech and language therapy and neuropsychology, who provided consultation at various stages of the study. Members were contacted individually via email and invited to participate.
Stakeholder groups
Stakeholder groups, who had the experience of peer relationships for adolescents with ABI, were recruited through purposive sampling. Four stakeholder groups were invited to participate: (1) adolescents with ABI (12–17 years); (2) parents of adolescents with ABI (12–17 years); (3) adults who sustained an ABI in adolescence; and (4) practitioners working with adolescents with ABI. Both focus groups and interviews were employed due to time restrictions and the difficulties encountered when recruiting this population.
Recruitment strategy
The study was advertised by charity organizations over a five-month period using a recruitment poster shared on social media. Potential stakeholders were asked to contact the researcher via email or through the study's webpage. A consent to contact form, participant information sheet, and consent to participate form were then sent for completion. The participant information sheet included rationale for the research. The personal goals of the lead author were not included. A total of 27 potential stakeholders expressed interest in the study, of which 16 consented to participate (). The remaining 11 did not respond to further correspondence. No stakeholders withdrew from the research. To protect confidentiality, all identifiable information has been removed and all names used are pseudonyms.
Table 1. Parent and adolescent stakeholders.
Table 2. Adults with ABI stakeholders.
Table 3. Practitioner stakeholders.
Ethics
Ethical approval was granted by the School of Psychology Research Committee at the University of Exeter.
Procedure and data collection
For this study, the term peer relationships is used to comprise relationships of varying quality (Heverly-Fitt et al., Citation2014), including negative (i.e., victimization), neutral, and positive (i.e., friendships). Given the potentially ambiguous meaning of peer relationships for stakeholders, “friendships” was used by the researcher to encourage accessibility. Stakeholders describe participant groups that would benefit from the intervention (i.e., service users and providers).
Stage 1: Planning group survey
Planning group members were sent a survey to complete comprising open-ended questions seeking perspectives in line with the RQs. Their responses were analysed separately to inform the initial development of the logic model of peer relationship difficulties for stakeholder feedback. The logic model was created using the “multifactorial precede approach” (Green & Kreuter, Citation1999). Within this approach, the target problem for intervention, and its impact on QoL, is understood to be influenced by individual and environmental determinants.
Stage 2a: Stakeholder focus groups
Two focus groups were held at the University of Exeter. Parents and adolescents with ABI participated in separate focus groups to promote homogeneity within each group. These were moderated by two researchers; the lead author (male; BSc, MSc) and an independent researcher (female; BSc). Both moderators were doctoral-level students and employed as trainee clinical psychologists. The moderator role was maintained by facilitating group discussions and allowing each stakeholder to speak, rather than asking questions for a direct response (Braun & Clarke, Citation2013).
The topics for discussion included: (a) experiences of friendships for adolescents with ABI; (b) the difficulties associated with ABI and the impact of these on friendships; (c) educational, social, and community understanding of ABI; (d) psychological changes following ABI and the impact on friendships; (e) behavioural changes following ABI; (f) feedback on the planning group logic model of peer relationship difficulties; (g) what change is needed to improve peer relationships; and (h) perspectives on intervention design, methods, and goals. Additional prompts were included to probe for further discussion, if required. The adolescents with ABI focus group lasted 55 minutes, and the parent focus group lasted 90 minutes.
The focus group schedule was piloted with four adolescents without ABI prior to stakeholder focus groups to explore the clarity and meaningfulness of the questions, and to observe how adolescents responded. This supported the amendment of the schedule following feedback and researcher reflections. Data from the pilot focus group was not included in the analysis and was used to determine the appropriateness of adolescent responses. Feedback from the pilot group suggested that the topic areas were understandable and suitable for adolescents.
Stage 2b: Stakeholder interviews
Interviews with parents, adults, and practitioners were completed face-to-face or via telephone or Skype, depending on stakeholder preference and location. Eight interviews were completed in total, seven individually and one with a parent–child dyad. All interviews were conducted by the lead author and guided by an amended version of the focus group schedule to protect consistency of topic conversations. Interviews lasted between 50 and 110 minutes. There were no repeat interviews. The schedule was piloted with a psychological practitioner prior to interviews.
Transcription
All focus groups and interviews were audio-recorded and transcribed verbatim. Ten data items were collected in total (two focus group transcripts and eight interviews). The researcher listened to the recordings prior to transcription, supporting researcher immersion. Researcher reflections and field notes were made during focus groups, interviews, and data immersion.
Data analysis
It was recognized that the type of data collected from focus groups and interviews differed. Within focus groups, stakeholders engaged in interactional discussions and were able to build on the perspectives of others. This allowed for themes to be built upon by the group, as well as for conflicts of opinion to be shared. In contrast, interviews provided a question and response conversation between the researcher and the stakeholder. Due to limited focus group data, the data were analysed collectively. This allowed for similar emergent themes from the two data collection methods to be analysed and further explored.
The lead author conducted the analysis. Transcripts were read and re-read (Braun & Clarke, Citation2006; Citation2013). Data were analysed using NVivo qualitative software (QSR International) through inductive TA. This bottom-up approach allowed for codes and themes to emerge from what was communicated in the data. Although questions were guided by the SOCIAL model and the IM protocol, apparent themes within the analysis were data-driven and naturalistically occurring (Joffe, Citation2012). This allowed the researcher to be open to new emerging concepts within the field of research. To ensure fidelity to the methodology, data analysis was completed following detailed guidance outlined by Braun and Clarke (Citation2006; Citation2013).
Initial thoughts and codes, which were of interest for the analysis and the outlined RQs, were produced following familiarization with the data. below provides an example of coding applied to the presented data extracts. Coding was completed systematically and iteratively, and a complete coding process was utilized. Themes were constructed and informed by the repeated patterns of codes and how they interacted throughout the data set. These were reviewed to determine if they captured a coherent and meaningful narrative of the data. The data set was re-read throughout this process and additional codes and themes were noted. Three rounds of analysis were completed until data saturation was reached whereby no further themes emerged. The themes were refined and named to capture the essence of what was communicated in the data.
Table 4. Data extracts and coding examples.
The data analysed from stakeholder focus groups and interviews informed the first revision of the planning group's logic model of peer relationship difficulties, consistent with IM methodology. In this process, the data from communicated stakeholder experiences (i.e., codes) were organized by the categories within the logic model (i.e., determinants, target problem, and impact on QoL). These categories were consistent with some of the pre-determined topics for discussion within the focus groups and interviews to support the outlined RQs. Organizing the data according to the logic model categories provided a visual representation of the possible relationships between different parts of the data. This supported the development of themes to explore and interpret stakeholder experiences and perspectives, and how they connected to other themes.
Credibility checks
To ensure that the analysis was trustworthy (Nowell et al., Citation2017), a number of credibility checks took place. There was prolonged engagement with the data, including multiple rounds of analysis and several researcher transcriptions. A reflective journal was used to note down thoughts and assumptions, which were regularly reviewed during the research process to support researcher reflexivity. Analytic processes were discussed amongst peers and codes were reviewed by two peer researchers through the sharing and critical discussion of two coded transcripts (20% of the data) in a doctoral-level qualitative research seminar.
Consultation around the logic model of peer relationship difficulties was sought from planning group members following the revision of the initial logic model after stakeholder discussions and feedback. The revised model was shared with the planning group for feedback and reflection around the organization and interaction of the data (i.e., suitable determinant categorization). This resulted in four more revisions, until no further feedback was provided, and a consensus was reached. The fifth iteration of the logic model was then shared with adult-aged stakeholders for feedback around the credibility. This resulted in a sixth and final revision () after improving the accessibility of terminology. No further revisions to the model were made.
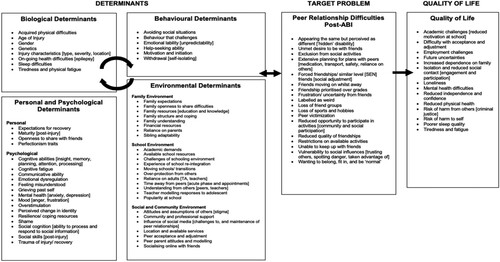
Figure 1. Logic model of peer relationship difficulties for adolescents with ABI (6th revision).
Although participants were not provided with transcripts, member-checking procedures were used with adult-aged stakeholders to gain feedback on emerging themes and the revised logic model of peer relationship difficulties to encourage the trustworthiness of the interpretations (Braun & Clarke, Citation2013).
Epistemology and researcher reflexivity
To promote credibility, qualitative research requires disclosure from the researcher around epistemological perspective, experience, assumptions, and biases that may influence analytic conclusions (Braun & Clarke, Citation2013; Joffe, Citation2012; Yardley, Citation2000). This study adopted a social constructionist position. Here, it was assumed that knowledge about the experience of peer relationship difficulties for adolescents with ABI is subjective and socially constructed by those who experience these, as well as by those who aim to understand these difficulties (Schwandt, Citation2003). From this position, the knowledge and experiences of peer relationship difficulties described in this study were constructed by the stakeholders and the researcher throughout the research process.
The lead author engaged in regular reflective conversations with research supervisors during the analysis. These conversations surfaced underlying assumptions and supported the lead author to consider their position within the research process and the creation of knowledge (Bradbury-Jones, Citation2007). The lead author has personal and clinical experience of peer relationship difficulties following ABI in adolescence. It was assumed that adolescents with ABI want to be treated as normal, peers find it difficult to understand ABI, and that successful peer relationships are a priority for adolescents. Regular reflective discussions supported the lead author to notice and manage their own position within the interpretation of the data.
Results
Themes
The analysis from stakeholder accounts yielded 11 themes organized into two domains: (1) understanding peer relationships difficulties (RQ one and two); and (2) improving peer relationships (RQ three and four). Some presented data excerpts have been modified to remove superfluous information that did not affect the overall meaning (Braun & Clarke, Citation2013; Sandelowski, Citation1994). For the purpose of the results, adolescents refer to those with ABI, and peers and friends are used for non-injured adolescents.
Understanding peer relationship difficulties
The following themes capture stakeholder understandings of peer relationship difficulties for adolescents and the key determinants that contribute to these.
Dropped and excluded
A pervasive sense of loss was portrayed by all stakeholders when describing friendships for adolescents. Parents and practitioners spoke particularly of the hardships adolescents experienced when attempting to maintain or re-integrate into friendship groups post-injury. Beth described these losses as feeling “dropped” by peers, depicting a powerful and emotive image associated with this loss.
I have only got three friends because all the friends I seem to make keep on dropping me and being horrible. (Beth, adolescent)
A common determinant for this loss was constructed by stakeholders where adolescents “drifted” from friends whilst recovering from injury. Louise spoke about feeling left behind by her peers, as they continued in their social development outside of school.
You’re sick all the time which means you’re off sick even more than you already were, so things go on and people develop friendships in school, and you’re missing it all. I had a best friend when I fell ill, and I came back after not being sick and she’d made a new best friend. (Louise, adult)
Parents and practitioners emphasized the rejection and exclusion that adolescents can experience from peers within their accounts. These experiences commonly followed frustration from peers towards acquired cognitive and behavioural difficulties, such as impulsivity and forgetfulness. Being perceived as “weird” appeared frequently within conversations, capturing the negative label that adolescents can attract when returning to school whilst navigating acquired difficulties. Stakeholders spoke of perceptions of being weird being influenced by difficulties with processing social information and appropriateness of social responses. Challenges with self-awareness post-ABI may contribute to the difficulties in peer interactions.
When I am trying to be sarcastic, my voice doesn't sound it at all so people just think I am being really weird. I sometimes take people seriously and then they will be like, “It was a joke,” (Beth, adolescent)
Isolated and alone
Stakeholders constructed that isolation for adolescents was a significant consequence of exclusion or victimization from peers. Parents spoke of their children subsequently becoming dependent on the family or withdrawing onto online platforms. It was reported that this perpetuated isolation. Kelly spoke of her son's world becoming increasingly “insular and narrow,” and other parents shared their concerns for their children's futures.
… they do become so socially isolated they look more and more to the family, they spend more time by themselves or with adults, they lose their ability to act with age appropriate peers, the peers move on with everything. (Lucy, parent)
A need to belong
The importance of connection and belonging in adolescence was a prominent theme talked about by adult-aged stakeholders. Belonging was recognized to be a basic human need, and Kate, an adolescent, spoke of a best friend being there for emotional support. Stakeholders constructed from their experiences that successful peer relationships were important for psychological wellbeing. Louise powerfully shared a strong preference for friendship over academic performance. Parents suggested that this need was overlooked by educational environments primarily focusing on academic achievement.
I wouldn't have cared if I got my GCSE's as long as I still had my friends at school. I would rather I had peer interventions from psychologists at school than I had for educational stuff. I would rather I left school with no GCSE's and didn't get bullied. (Louise, adult)
Parents, practitioners, and adults described a sense of desperation for adolescents to not be perceived as different by their peers. Charlotte, a parent, described how adolescents want to fit in and be accepted by their friends. Considering this, parents spoke of the differences in their treatment priorities compared to their children's. Shirley, a parent, shared her desire for her daughter to receive support for her cognitive difficulties in school, yet spoke of her daughter's reluctance through fear of appearing different. Other parents echoed this.
Kids want to be normal as a teenager. They don't want to stand out, and by having some form of injury […] you want to be as normal as possible, and I think that's quite hard. (Carol, parent)
A desire to belong was purported to increase vulnerability from others. Adolescents were reported to become susceptible to undesirable social influences in attempt to connect with others. Shirley shared concerns for her daughter's safety in this regard. Practitioners spoke of adolescents undertaking a new role of being comical, entertaining, or useful to a new group of peers, increasing risk of exploitation from peers encouraging the provocation of teachers or engagement in criminal behaviour.
… they’re very keen to be part of something. So, they might get drawn into activities that are inadvisable or down-right dangerous, just in an attempt to be part of the group. (Jackie, practitioner).
No one understands
It was constructed that peer difficulties were influenced by the lack of understanding about ABI, and the associated assumptions and stigma. All stakeholder groups spoke of others misunderstanding ABI and its implications. This included peers, but also parents of peers, teachers, and the wider community. This incomprehension was recognized to be influenced by the “hidden” difficulties associated with ABI in contrast to a physical injury or disability, and adolescents talked about a lack of support at school.
They don't tell kids that this person has a brain injury or stop bullying them. They don't say anything about me, like how to treat me. It is horrible. (Kate, adolescent)
Parents spoke of the assumptions and stigma their children experienced. There was frequent reference to peers perceiving difficulties as non-existent or used as a mechanism to miss school or receive special attention. Parents described often “battling” with schools and other parents in an effort to “prove” their children's difficulties.
… we’ve got parents who are very much like, “Oh, she's just making a drama,” or “Just pull yourself together,” or “Is she really dizzy?” and “Does she just not want to be at school?.” (Charlotte, parent)
Restricted independence at a time for growth
Parents, practitioners, and adults with ABI suggested that adolescents are restricted in their opportunities for typical peer interaction, contributing to difficulties with peer relationships. This was particularly apparent for adolescents who sustained severe injuries, requiring specialist educational environments.
… they’ve gone from what was their typical trajectory to being completely taken out of their cohort of peers. So, they don't, certainly in their school hours, they don't have access to those peers anymore. I doubt how much access they have outside of school. (Ella, practitioner)
… no one is going to come and tell you a secret or include you in on something if there's an adult sitting there. So, no one's going to come over and give you all the gossip and dish the dirt if you’ve got an adult there, so you miss all that. (Jackie, practitioner)
You’re socially isolated because you can't keep up in the same way because of fatigue […], you’re not in school, you’re not allowed to play sports, you’re not allowed to go to the cinema, but then also, a kind of atmosphere becomes apparent … in that people don't believe you’re not well. (Louise, adult)
Loss of past self
A commonality surfaced around the grief adolescents and parents can experience following injury, grieving for what could have been. Changes in identity appeared to be frequent for adolescents following a loss of sports, academic abilities, peer groups, and family roles. Adolescents were reported to find this difficult to adjust to, and feelings of hopeless and uncertainty about the future were described, affecting QoL. Adult stakeholders spoke of referring to the “old” and “new” version of themselves. Kelly spoke of her son using a new name entirely. The impact of this resonated more if adolescents were able to remember their abilities before injury and finding themselves in conflict with the new sense of self.
In the context of peer relationships, stakeholders commonly associated the loss in past self with a loss of peer groups related to that identity. For example, the loss of teammates for sports, or a loss of motivation to be with high achieving peers when struggling academically.
Very lonely, very depressed, you don't have that sense of achievement anymore, you’ve completely lost your identity, and it just, it can lead to very downward spiral. (Louise, adult)
Challenges with acquired status
A number of determinants of peer relationship difficulties presented, within cognitive, emotional, and behavioural domains. Parents and practitioners spoke about the lability that adolescents post-ABI can present with, rapidly switching between intense emotions which peers can respond negatively towards.
… their mood and anxiety and not being able to keep on top of their emotions and having outbursts in school, which obviously leads to them being picked on even more and becoming even more socially isolated. (Hannah, practitioner)
… she's lost loads of confidence, so that makes it really hard to make friends when you’re really, really inward. (Carol, parent)
Improving peer relationships
The following themes comprise stakeholder perspectives on what might need to change to improve peer relationships for adolescents, and what the goals of an intervention might be.
Building understanding
There was a strong commonality shared around the need to increase understanding about ABI in others around adolescents. Parents, practitioners, and adults spoke of the benefit of teachers and peers receiving education around the impact of ABI and what the adolescent might be experiencing. This was hoped to reduce the assumptions and stigma shown by others that negatively impact peer relationships. This education and understanding may promote acceptance from others and facilitate compassion within the system around the adolescent, supporting social inclusion.
… because it's not talked about, I would love for them to do a massive assembly in the school and say, “This is what goes on,” […], so that it's not such a taboo thing and so children aren't so frightened about it … (Charlotte, parent)
Meaningful social connection
When considering the limited opportunities for peer interactions, parents advocated for meaningful social activities. Here, stakeholders reflected on being with others with ABI and participating in activities with non-injured friends. Ben recognized the benefit of being with others with ABI, promoting a sense of commonality and normalization. However, some parents and practitioners felt it to be more important to facilitate fun activities with peers. Louise reflected on her experience in adolescence, subsequently stating that solely socializing with others with disabilities would have furthered peer exclusion.
I didn't really like the whole pushing me to surround myself with other people with brain injury. Didn't like that because […] I wanted to be normal. (Louise, adult)
It's that her life is full of middle-aged women […] she has a teaching assistant and that, and they’re mainly middle-aged women, and actually I know that she responds a lot better to someone who is younger. (Carol, parent).
Support for the journey
Parents and adults reported feeling lost post-discharge, with many unanswered questions and concerns for the future. It was recognized that professional support fell away and parental help-seeking relied on family resources. Subsequently, early support, assessment, and education for the family about ABI was advocated for to support school re-integration and care planning.
… you’re not informed on who you are now or what struggles you might deal with, which means then your peers aren't informed of who you are now and what struggles you might be having to deal with. You don't even know, how are they meant to know? (Louise, adult).
Empowerment
Parents, practitioners, and adults felt a need to support adolescents to change their relationship with ABI. They suggested that adolescents can feel powerless and hopeless in the context of injury. Kelly recognized the persistent negative messages that adolescents can experience from those around them that perpetuated feelings of hopelessness and shame.
… all they’re hearing in messages is “You’re making it up” “You’re skiving” they’re being rejected by their peer groups, they’re finding it really hard to interact with their peer groups, and they’re worrying about future relationships … . (Kelly, parent)
You’re empowering them to say to a teacher “I’m not being lazy, I’ve got an initiation problem”, it just changes the whole world. (Jackie, practitioner)
Logic model of peer relationship difficulties
The logic model () shows the variety of peer relationship difficulties that adolescents can experience and the long-term impact on QoL, as described by stakeholders. As presented, these difficulties were perceived as being influenced by the interactions between the outlined determinants. These may maintain peer relationship difficulties, or be further influenced by these difficulties, as represented by the bi-directional arrow. For example, being excluded from social activities (peer relationships difficulties post-ABI) may be influenced by emotional lability and withdrawal (behavioural determinants), time away from peers during recovery, and the attitudes and assumption of others (environmental determinants). Being excluded from social activities may further influence mental health and mood (psychological determinants), and a reliance on parents (environmental determinants). Adolescents may experience a loss of friendship group over time (peer relationships difficulties post-ABI) and reduced QoL, influenced by isolation and feelings of loneliness.
Supporting these determinants may be the focus of future meaningful interventions to improve the outcomes of adolescents, such as through emotional support, education for others, supporting contact with peers during recovery, and facilitating activities with others; as suggested by stakeholders.
Discussion
This study aimed to collaborate with key stakeholders to (a) understand peer relationship difficulties for adolescents with ABI (adolescents); and (b) seek their perspectives on what might be needed to improve these relationships and what the intervention goals might be. The complexities of peer relationship difficulties for adolescents have largely been under-recognized. The qualitative insights from this study endeavoured to inform this gap within the paediatric neuropsychology literature, and to support the development of a logic model (step one of IM) which can be used to guide future intervention development using IM methodology.
Stakeholder accounts supported that adolescents with ABI face difficulties in maintaining peer relationships. Consistent with previous research (Anderson et al., Citation2013; Yeates et al., Citation2007), difficulties with social competence and social participation for adolescents with ABI were constructed by stakeholders. There was a reference to the challenge of keeping up with social demands and activities whilst navigating the physical and cognitive consequences of ABI. This was suggested to invite negative attributions to be made by peers. Isolation and loneliness and restricted independence were identified as key determinants for social participation difficulties for adolescents with ABI. In line with findings by Anderson et al. (Citation2013), cognitive functioning and environment were identified by stakeholders as influential determinants for peer relationship difficulties.
Peer rejection and exclusion were also recognized, consistent with Glennon (Citation2019) and Yeates et al. (Citation2013). Stakeholder insights suggested that pre-injury friendships could be lost following ABI and that this was associated with peer separation during recovery, restricted peer interactions, and the negative assumptions associated with the “hidden” difficulties associated ABI (Simpson et al., Citation2002).
Stakeholder conversations and planning group perspectives indicated the determinants for peer relationship difficulties were broad. Consistent with previous research, difficulties with cognition (Anderson et al., Citation2012), social cognition (Tousignant et al., Citation2018), misunderstanding (Keetley et al., Citation2019), emotional lability (Vasa et al., Citation2015), and perceived changes in identity (Glennon, Citation2019; Ownsworth, Citation2014) were identified to negatively impact peer relationships. Stakeholders reported the lack of understanding about ABI to be an important determinant for peer difficulties. Some adolescents may return to school appearing unscathed yet can present as different to peers due to acquired cognitive, socio-cognitive, and emotional difficulties (Simpson et al., Citation2002). This may invite negative assumptions from peers towards the “realness” of difficulties, resulting in further rejection or peer frustration. Similarly, the emotional consequences associated with ABI (Sariaslan et al., Citation2016) and a change in identity (Ownsworth, Citation2014) reduced motivation for social participation, perpetuating feelings of loneliness (Parker & Asher, Citation1987) and dependency on the family. Further implications for QoL included future academic and vocational concerns (Sariaslan et al., Citation2016), reduced confidence, and risk of early contact with the criminal justice system (Williams, Citation2012), as reported by stakeholders.
The notion that adolescence is a time for belonging (Blakemore, Citation2008), peer emotional support (van Harmelen et al., Citation2017), and social identity (Tajfel, Citation1978) was supported. Successful peer relationships were a priority for some stakeholders over academic achievement, a priority previously reported by Sirois et al. (Citation2014). To support belonging and peer acceptance, stakeholders constructed that adolescents with ABI have desire to appear “normal” and may adjust friendship preferences to perform competently (Anderson & Beauchamp, Citation2012). This is consistent with the themes reported by Glennon (Citation2019) highlighting adolescent desires for peer relatedness and “fitting in” post-injury. However, as spoken about by stakeholders, this may also increase vulnerability for exploitation from others, compounded by socio-cognitive difficulties and understanding intentions of others (a determinant in the logic model). Difficulties with the theory of mind have previously been recognized post-ABI (Turkstra et al., Citation2004).
The themes and logic model offer guidance for the development of a future intervention, and stakeholders offered their perspectives on what is needed to support the needs of adolescents.
Stakeholder accounts suggested a preference for intervening within the adolescent's educational, community, and social environment over one-to-one interventions. This was primarily due to concerns around adolescent engagement through fear of being perceived as different and wanting to be a “normal” teenager and be with their friends. Environmental intervention included the need for increased awareness of ABI amongst peers, particularly in the context of “hidden” disability. An intervention might include educational sessions at schools for peers, or through additional teacher training. Furthermore, intervention resources could be used to develop additional online materials and videos that offer information about ABI.
Targeting social environments, stakeholders identified the lack of opportunities for adolescents to socialize with their peers outside of school in a meaningful way with shared value. A future intervention might consider social participation opportunities for adolescents with selected peers and/or others with ABI which involve a shared interest. The positive impact of group-based DJ-ing and outdoor activity programmes for adolescents with ABI has been recognized anecdotally, though this data is currently unvalidated.
A need for early support was identified by stakeholders, with many parents and adults describing the challenge of being discharged from the hospital with uncertainties about the future in the context of ABI. Early signposting for community and statutory support could provide access to additional resources to help facilitate the adolescent's reintegration into education and their peer environment. The extent to which an intervention could support this, and the context in which it is delivered, requires further consideration. However, working together with established voluntary and charity organisations may be important to support this.
Whilst stakeholders suggested environmental interventions would be important, it was noted however that individual emotional support would be of benefit to adolescents in their adjustment to ABI and returning to school. Stakeholders, particularly parents, believed that it would be helpful for the adolescent if this was facilitated by someone of a similar age (e.g., university students), showing support for the previously purported benefits of peer-led interventions (Braga et al., Citation2012). It was recognized that post-injury, adolescents are involved with a multitude of professionals who were often middle-aged, with incongruent characteristics. Peer coaches, offering emotional support to adolescents via a similar platform to that used in the Social Participation and Navigation (SPAN) programme (Wade et al., Citation2018), might be helpful for any future intervention development. Indeed, the authors reported that participants valued the peer-coaching aspect of the SPAN intervention.
In summary, a meaningful intervention to support peer relationships with adolescents post-ABI may need to be multifaceted to support adolescents at an individual (emotional support) and environmental level (building understanding), consistent with recommendations made by Andrews et al. (Citation2015). This could include providing education and resources about ABI to peers and schools, facilitating meaningful social activities with friends, offering emotional support, and early signposting for additional support post-injury. Empowering adolescents post-ABI was identified as an important intervention goal.
Theoretical implications
The determinants spoken about by stakeholders in this study offer support for the mediators and cognitive determinants identified by the SOCIAL model (Beauchamp & Anderson, Citation2010). Challenges within an adolescent's external environment (i.e., peer rejection, misunderstanding, and stigma), and difficulties with cognitive and socio-cognitive abilities were described by stakeholders as key influential determinants for peer relationship difficulties for adolescents with ABI. The presented interactions between these determinants are consistent interactions proposed within the SOCIAL model.
Emotional difficulties (i.e., anxiety, hopelessness, shame, and lability) were also described by stakeholders to be influential determinants for peer relationship difficulties, impacting upon social competence and motivation for social participation. Emotional determinants appear to be omitted from the SOCIAL model. Across development, these determinants may have an important reciprocal role for facilitating successful peer relationships, which in turn, could support emotional difficulties for adolescents. The importance of a supportive external environment for the development of social and cognitive functioning is noted by authors, along with how difficulties in these areas might directly or indirectly affect the development of social skills. Indeed, successful peer relationships in adolescence can be protective for mental health and resilience (van Harmelen et al., Citation2017). With further evidence, future revisions of the SOCIAL model may consider the inclusion of emotional determinants and their role in the development of social skills in non-injured children and adolescents. Reviewing the evidence for social skill abilities (competence, adjustment, and participation) in those with a history of developmental trauma might support this addition. This might give note to the impact of core beliefs and perceived safeness with others on social functioning.
It would be of interest to contextualize the SOCIAL model for ABI populations. Unique to ABI is the presence of pre-injury social and cognitive processes that support the emergence of social skills. The presence of an injury might affect the expression of social skills due to a change within these processes. These changes might require intervention to support social functioning, though further research is needed. To support this, future research might investigate how ABI in childhood or adolescence may influence the expression and development of social skills. This might be in the context of reduced social opportunities due to difficulties with mood and peer rejection, as described by stakeholders in this study.
Clinical implications
The findings suggested that adolescents can experience difficulties with peer relationships and mental health, though they may not volunteer these difficulties through fear of appearing different. Consequently, their needs could be overlooked. Practitioners can hold this in mind and routinely enquire about an adolescent's mental health, alongside being curious about their support network beyond the family.
The risks and vulnerabilities associated with ABI and a need to belong were identified. This awareness can support clinicians to formulate risk and intervene appropriately. This awareness could also be shared with commissioners to seek funding for additional community resources to support social belonging for children and adolescents, such as youth clubs. Programmes that support positive social participation may reduce the risk of early contact with the criminal justice system (Williams, Citation2012).
Some stakeholders shared their priority for successful peer relationships over academic achievements. This understanding may inform rehabilitation goal planning and educational learning plans to support adolescents to engage and participate meaningfully with friends, subsequently supporting QoL.
The importance of building understanding about ABI for those around the adolescent (i.e., peers, teachers) was identified as a key part of a meaningful intervention. Understanding could be supported through the creation of online resources or videos made by adolescent stakeholders with ABI. Raising awareness about the impact of ABI on education amongst policy makers is one strategic aim of The National Acquired Brain Injury in Learning and Education Syndicate (N-ABLES), set up in 2018 (https://ukabif.org.uk/page/NABLES). The findings from this study can support this.
Social media could facilitate an adolescent-led project to disseminate informative videos. This may simultaneously empower adolescents to become experts. Safe use of social media may need to be individually assessed and moderated for adolescents post-ABI in the context of potential risk associated with social vulnerability and wanting to belong.
Strengths and limitations
The methodology of this study promoted collaboration with planning group members and key stakeholders to co-produce the logic model of the target problem for intervention through a rigorous process. Utilizing member-checking procedures throughout the study promoted the credibility of the findings and interpretations made. An additional strength included piloting the focus groups and interview schedules, allowing for the observation of responses and suitability to support the research aims.
A limitation includes the use of focus groups combined with individual interviews due to the difficulties encountered when attempting to recruit from the paediatric ABI population. Though focus groups and interviews were of a similar length, stakeholders who were interviewed had increased opportunity to contribute to the findings. Conversely, the richness of the data collected in interviews was limited due to question and response nature of the conversation. Stakeholders in the focus groups were able to construct opinions, share and build on each other's experiences, and discuss topics beyond scheduled topics that provided further insights.
Future research exploring commonalities in adolescent and parent experiences of ABI may benefit from solely using focus group methodology. This methodology promotes connectivity and peer support to an often isolated population. It can encourage social interaction and the sharing of social pressures amongst adolescents with ABI. Furthermore, it may allow parents and adolescents with ABI to feel less isolated in their experiences. The normalization and commonalities discussed amongst participants could promote the disclosure and sharing of experiences beyond an interview setting. However, it must be noted that the heterogeneity of ABI, and diversity in family resources and culture would likely affect the emergence of commonalities and shared opinions. With larger sample sizes, future research could consider weighting focus groups by group variances (e.g., injury type, age, social-economic status).
The parent and adolescent sample used within this study consisted of sample bias. All adolescents were aged 13 years and originated from a white middle-class background. This would have influenced adolescent and parental experiences following ABI, such as resources, access to services, and educational environments. This may contrast with experiences from stakeholders originating from Black, Asian, and minority ethnic or lower social-economic status backgrounds. Future research should consider recruiting stakeholder participants from diverse backgrounds. This may be achieved through close working between the researcher and statutory services to seek support for recruitment, such as in educational, health, and social care settings. This could support recruitment from a wider and more diverse population, beyond those who are supported by charity organizations.
Difficulties were experienced when recruiting from the ABI population within the available time restrictions. Adolescent stakeholders had limited representation due to the small sample size and their apparent reservations in conversation. Consequently, their perspectives may not have emerged as strongly in the analysis when compared to other stakeholder groups. Future research should consider using a larger sample of adolescents with ABI. Recruitment could be supported through engagement with health services, local communities, social media, and ABI charities.
Conclusion
Adolescents with ABI were reported to experience difficulties with peer relationships. At an important time for social development, peer rejection can increase feelings of isolation, loneliness, shame, and hopelessness. This can have further implications for mental health, peer relationships, and QoL. The individual, psychological, behavioural, and environmental determinants for peer relationship difficulties are broad. Reported stakeholder experiences offer new clinical and theoretical insights for the paediatric neuropsychology literature. A meaningful intervention would need to be multifaceted attempting to build understanding in others, facilitate opportunities for meaningful social connection, offer early support post-injury, and help manage psychological wellbeing. A primary focus would be to empower adolescents post-ABI. The presented logic model provides a robust understanding of peer relationship difficulties for adolescents with ABI that can be used to guide intervention development in future research.
Acknowledgements
Extended thanks to the Child Brain Injury Trust and Challenge Ahead.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adolphs, R. (1999). Social cognition and the human brain. Trends in Cognitive Sciences, 3(12), 469–479. https://doi.org/10.1016/S1364-6613(99)01399-6
- Anderson, V., & Beauchamp, M. H. (2012). SOCIAL: A theoretical model of the development of social neuroscience. In V. Anderson, & M. Beauchamp (Eds.), Developmental social neuroscience and childhood brain insult (pp. 3–20). Guildford Press.
- Anderson, V., Beauchamp, M. H., Yeates, K. O., Crossley, L., Hearps, S. J., & Catroppa, C. (2013). Social competence at 6 months following childhood traumatic brain injury. Journal of International Neuropsychological Society, 19(5), 539–550. https://doi.org/10.1017/S1355617712001543
- Anderson, V., Brown, S., & Newitt, H. (2009). Educational, vocational, psychosocial, and quality of life outcomes for adult survivors of childhood traumatic brain injury. Journal of Head Trauma Rehabilitation, 24(5), 303–312. https://doi.org/10.1097/HTR.0b013e3181ada830
- Anderson, V., Brown, S., Newitt, H., & Hoile, H. (2011). Long-term outcomes from childhood traumatic brain injury: Intellectual ability, personality, and quality of life. Neuropsychology, 25(2), 176–184. https://doi.org/10.1037/a0021217
- Anderson, V., Godfrey, C., Rosenfeld, J. V., & Catroppa, C. (2012). 10 years outcome from childhood traumatic brain injury. International Journal of Developmental Neuroscience, 30(3), 217–224. https://doi.org/10.1016/j.ijdevneu.2011.09.008
- Andrews, J., Falkmer, M., & Girdler, S. (2015). Community participation interventions for children and adolescents with neurodevelopmental intellectual disability: A systematic review. Disability and Rehabilitation, 10(10), 825–833. https://doi.org/10.3109/09638288.2014.944625
- Arroyos-Jurado, E., Paulsen, J. S., Ehly, S., & Max, J. E. (2006). Traumatic brain injury in children and adolescents: Academic and intellectual outcomes following injury. Exceptionality, 14(3), 125–140. https://doi.org/10.1207/s15327035ex1403_2
- Barber, S., Bate, A., Adcock, A., Harker, R., Roberts, N., Woodhouse, J., & Mackley, A. (2018). Acquired brain injury. https://researchbriefings.parliament.uk/ResearchBriefing/Summary/CDP-2018-0145#fullreport.
- Barrera, M., Atenafu, E. G., Sung, L., Bartels, U., Schulte, F., Chung, J., Cataudella, D., Hancock, K., Janzen, L., Saleh, A., Strother, D., Downie, A., Zelcer, S., Hukin, J., & McConnell, D. (2018). A randomised control intervention trial to improve social skills and quality of life in paediatric brain tumour survivors. Psycho-Oncology, 27(1), 91–98. https://doi.org/10.1002/pon.4385
- Bartholomew-Eldredge, L. K., Markham, C. M., Ruiter, R. A. C., Fernandez, M. E., Kok, G., & Parcel, G. S. (2016). Planning health promotion programs: An intervention mapping approach (4th ed.). Jossey-Bass.
- Beauchamp, M. H., & Anderson, V. (2010). SOCIAL: An integrative framework for the development of social skills. Psychological Bulletin, 136(1), 39–64. https://doi.org/10.1037/a0017768
- Blakemore, S. J. (2008). The social brain in adolescence. Nature Reviews, 9(4), 267–277. https://doi.org/10.1038/nrn2353
- Bradbury-Jones, C. (2007). Enhancing rigor in qualitative health research: Exploring subjectivity through Peshkin’s I’s. Journal of Advanced Nursing, 59(3), 290–298. https://doi.org/10.1111/j.1365-2648.2007.04306.x
- Braga, L. W., Rossi, L., Moretto, A. L. L., da Silva, J. M., & Cole, M. (2012). Empowering preadolescents with ABI through metacognition: Preliminary results of a randomised clinical trial. Neurorehabilitation, 30(3), 205–212. https://doi.org/10.3233/NRE-2012-0746
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
- Braun, V., & Clarke, V. (2013). Successful qualitative research: A practical guide for beginners. Sage.
- Braun, V., & Clarke, V. (2016). (Mis)conceptualising themes, thematic analysis, and other problems with Fugard and Potts’ (2015) sample-size tool for thematic analysis. International Journal of Social Research Methodology, 19(6), 739–743. https://doi.org/10.1080/13645579.2016.1195588
- Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise, and Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
- Catroppa, C., Anderson, V., Godfrey, C., & Rosenfeld, J. V. (2011). Attentional skills 10 years post-paediatric traumatic brain injury. Brain Injury, 25(9), 858–869. https://doi.org/10.3109/02699052.2011.589794
- Cole, W. R., Gerring, J. P., Gray, R. M., Vasa, R. A., Salorio, C. F., Grados, M., Christensen, J. R., & Slomine, B. S. (2008). Prevalence of aggressive behaviour after severe paediatric traumatic brain injury. Brain Injury, 22(12), 932–939. https://doi.org/10.1080/02699050802454808
- Crick, N., & Dodge, K. (1994). A review and reformulation of social information-processing mechanisms in children’s social adjustment. Psychological Bulletin, 115(1), 74–101. https://doi.org/10.1037/0033-2909.115.1.74
- Dennis, M., Simic, N., Agostino, A., Taylor, H. G., Bigler, E. D., Rubin, K., Vannatta, K., Gerhardt, C. A., Stancin, T., & Yeates, K. O. (2013). Irony and empathy in children with traumatic brain injury. Journal of International Neuropsychological Society, 19(3), 338–348. https://doi.org/10.1017/S1355617712001440
- Fernandez, M. E., Ruiter, R. A. C., Markham, C. M., & Kok, G. (2019). Intervention mapping: Theory- and evidence-based health promotion program planning: Perspective and examples. Frontiers in Public Health, 7(209), 1–8. https://doi.org/10.3389/fpubh.2019.00209.
- Fougeyrollas, P., Noreau, L., Bergeron, H., Cloutier, R., Dion, S. A., & St-Michel, G. (1998). Social consequences of long term impairments and disabilities: Conceptual approach and assessment of handicap. International Journal of Rehabilitation Research, 21(2), 127–142. https://doi.org/10.1097/00004356-199806000-00002
- Glennon, C. (2019). Exploring identity following adolescent acquired brain injury from the perspectives of adolescents and their parents [Unpublished doctoral dissertation]. University of East Anglia.
- Green, L. W., & Kreuter, M. W. (1999). Health promotion and planning: An educational and ecological approach (3rd ed.). Mayfield.
- Greenham, M., Gordon, A. L., Cooper, A., Ditchfield, M., Coleman, L., Hunt, R. W., Mackay, M. T., Monagle, P., & Anderson, V. (2018). Social functioning following paediatric stroke: Contribution of neurobehavioural impairment. Developmental Neuropsychology, 43(4), 312–328. https://doi.org/10.1080/87565641.2018.1440557
- Gumm, R., Thomas, E., Lloyd, C., Hambly, H., Tomlinson, R., Logan, S., & Morris, C. (2017). Improving communication between staff and disabled children in hospital wards: Testing the feasibility of a training intervention developed through intervention mapping. BMJ Paediatrics Open, 1(1), 1–7. https://doi.org/10.1136/bmjpo-2017-000103
- Heverly-Fitt, S., Wimsatt, M. A., Menzer, M. M., Rubin, K. H., Dennis, M., Taylor, H. G., Stancin, T., Gerhardt, C. A., Vannatta, K., Bigler, E. D., & Yeates, K. O. (2014). Friendship quality and psychosocial outcomes among children with traumatic brain injury. Journal of the International Neuropsychological Society, 20(7), 684–693. https://doi.org/10.1017/S1355617714000393
- Hospital Episode Statistics. (2013). Hospital episodes statistics. Admitted Patient Care, England. https://digital.nhs.uk/data-and-information/publications/statistical/hospital-admitted-patient-care-activity/hospital-episode-statistics-admitted-patient-care-england-2012-13
- Iarocci, G., Yager, J., & Elfers, T. (2007). What gene-environment interactions can tell us about social competence in typical and atypical populations. Brain and Cognition, 65(1), 112–127. https://doi.org/10.1016/j.bandc.2007.01.008
- Joffe, H. (2012). Thematic analysis. In D. Harper, & A. Thompson (Eds.), Qualitative research methods in mental health and psychotherapy: A guide for students and practitioners (pp. 209–223). Wiley-Blackwell.
- Keetley, R., Radford, K., & Manning, J. C. (2019). A scoping review of the needs of children and young people with acquired brain injuries and their families. Brain Injury, 33(9), 1117–1128. https://doi.org/10.1080/02699052.2019.1637542
- King, S., MacDonald, A. J., & Chambers, C. T. (2010). Perceptions of healthy children toward peers with a chronic condition. Children’s Health Care, 39(3), 199–213. https://doi.org/10.1080/02739615.2010.493766
- Kok, G., Gottlieb, N. H., Peters, G. Y., Mullen, P. D., Parcel, G. S., Ruiter, R. A. C., Fernandez, M. E., Markham, C., & Bartholomew, L. K. (2015). A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychology Review, 10(3), 297–312. https://doi.org/10.1080/17437199.2015.1077155
- Lloyd, O., Ownsworth, T., Fleming, J., Jackson, M., & Zimmer-Gembeck, M. (2021). Impaired self-awareness after paediatric traumatic brain injury: Protective factor or liability? Journal of Neurotrauma, 38(5), 616–627. https://doi.org/10.1089/neu.2020.7191
- Mandalis, A., Kinsella, G., Ong, B., & Anderson, V. (2007). Working memory and new learning following paediatric traumatic brain injury. Developmental Neuropsychology, 32(2), 683–701. https://doi.org/10.1080/87565640701376045
- Nowell, L. S., Norris, J. M., White, D. E., & Moules, N. J. (2017). Thematic analysis: Striving to meet the trustworthiness criteria. International Journal of Qualitative Methods, 16(1), 1–13. https://doi.org/10.1177/1609406917733847
- O’Connor, A., Blewitt, C., Nolan, A., & Skouteris, H. (2018). Using intervention mapping for child development and wellbeing programs in early childhood education and care setting. Evaluation and Program Planning, 68(2018), 57–63. https://doi.org/10.1016/j.evalprogplan.2018.02.011.
- Olweus, D. (1993). Bullying at school: What we know and what we can do. Blackwell.
- Ownsworth, T. (2014). Self-identity after brain injury. Psychology Press.
- Parker, J. G., & Asher, S. R. (1987). Peer relations and later life personal adjustment: Are low-accepted children at risk? Psychological Bulletin, 102(3), 357–389. https://doi.org/10.1037/0033-2909.102.3.357
- Sandelowski, M. (1994). Notes of qualitative methods: Notes on transcription. Research in Nursing & Health, 18(6), 479–482. https://doi.org/10.1002/nur.4770170410
- Sariaslan, A., Sharp, D. J., D’Onofrio, B. M., Larsson, H., & Fazel, S. (2016). Long-term outcomes associated with traumatic brain injury in childhood and adolescence: A nationwide Swedish cohort study of a wide range of medical and social outcomes. PLoS Medicine, 13(8), 5–19. https://doi.org/10.1371/journal.pmed.1002103
- Schwandt, T. A. (2003). Three epistemological stances for qualitative inquiry: Interpretivism, hermeneutics, and social constructionism. In N. Denzin, & Y. Lincoln (Eds.), The landscape of qualitative research: Theories and issues (pp. 292–331). Sage.
- Simpson, G., Simons, M., & McFadyen, M. (2002). The challenges of a hidden disability: Social work practice in the field of traumatic brain injury. Australian Social Work, 55(1), 24–37. https://doi.org/10.1080/03124070208411669
- Sirois, K., Boucher, N., & Lepage, C. (2014). Current needs, the future of adolescent and young adults having sustained a moderate or severe traumatic brain injury (TBI) and the potential of their social participation. Open Journal of Therapy and Rehabilitation, 2(1), 45–55. https://doi.org/10.4236/ojtr.2014.21009.
- Sirois, K., Tousignant, B., Boucher, N., Achim, A. M., Beauchamp, M. H., Bedell, G., Massicotte, E., Vera-Estay, E., & Jackson, P. L. (2019). The contribution of social cognition in predicting social participation following moderate and severe TBI in youth. Neuropsychological Rehabilitation, 29(9), 1383–1398. https://doi.org/10.1080/09602011.2017.1413987
- Skivington, K., Matthews, L., Simpson, S. A., Craig, P., Baird, J., Blazeby, J. M., Boyd, K. A., Craig, N., French, D. P., McIntosh, E., Petticrew, M., Rycroft-Malone, J., White, M., & Moore, L. (2021). A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ, 374(2061), 1–11. https://doi.org/10.1136/bmj.n2061.
- Steinberg, L., & Morris, A. S. (2001). Adolescent development. Annual Review of Psychology, 52(1), 83–110. https://doi.org/10.1146/annurev.psych.52.1.83
- Tajfel, H. (1978). Social categorisation, social identity, and social comparisons. In H. Tajfel (Ed.), Differentiation between social groups (pp. 61–76). London: Academic Press.
- Tousignant, B., Jackson, P. L., Massicotte, E., Beauchamp, M. H., Achim, A. M., Vera-Estay, E., Bedell, G., & Sirois K.. (2018). Impact of traumatic brain injury on social cognition in adolescents and contribution of other higher order cognitive functions. Neuropsychological Rehabilitation, 28(3), 429–447. https://doi.org/10.1080/09602011.2016.1158114
- Turkstra, L. S., Dixon, T. M., & Baker, K. K. (2004). Theory of mind and social beliefs in adolescents with traumatic brain injury. Neurorehabilitation, 19(3), 245–256. https://doi.org/10.3233/NRE-2004-19307
- Turkstra, L. S., Politis, A. M., & Forsyth, R. (2014). Cognitive-communication disorders in children with traumatic brain injury. Developmental Medicine & Child Neurology, 57(3), 217–222. https://doi.org/10.1111/dmcn.12600
- van Harmelen, A. L., Kievit, R. A., Ioannidis, K., Neufeld, S., Jones, P. B., Bullmore, E., Dolan, R., Fonagy, P., & Goodyer I. (2017). Adolescent friendships predict later resilient functioning across psychosocial domains in a healthy community cohort. Psychological Medicine, 47(13), 2312–2322. https://doi.org/10.1017/S0033291717000836
- Vannatta, K., Gartstein, M. A., Zeller, M., & Noll, R. B. (2009). Peer acceptance and social behaviour during childhood and adolescence: How important are appearance, athleticism, and academic competence? International Journal of Behavioral Development, 33(4), 303–311. https://doi.org/10.1177/0165025408101275
- Vasa, R. A., Suskauer, S. J., Thorn, J. M., Kalb, L., Grados, M. A., Slomine, B. S., Salorio, C. F., & Gerring, J. P. (2015). Prevalence and predictors of affective lability after paediatric traumatic brain injury. Brain Injury, 29(7-8), 921–928. https://doi.org/10.3109/02699052.2015.1005670
- Vissenberg, C., Nierkens, V., Uitewaal, P. J. M., Middlekoop, B. J. C., Nijpels, G., & Stronks, K. (2017). Development of the social network-based intervention “powerful together with diabetes” using intervention mapping. Frontiers in Public Health, 5(334), 1–27. https://doi.org/10.3389/fpubh.2017.00334.
- Wade, S. L., Bedell, G. M., King, J. A., Jacquin, M., Turkstra, L. S., Haarbauer-Krupa, J., Johnson, J., Salloum, R., & Narad, M. E. (2018). Social Participation and Navigation (SPAN) program for adolescents with acquired brain injury: Pilot findings. Rehabilitation Psychology, 63(3), 327–337. https://doi.org/10.1037/rep0000187
- Wade, S. L., Waiz, N. C., Carey, J., Williams, K. M., Cass, J., Mark, E., & Yeates, K. O. (2010). A randomised trial of teen online problem solving for improving executive function deficits following paediatric traumatic brain injury. Journal of Head Trauma Rehabilitation, 25(6), 409–415. https://doi.org/10.1097/HTR.0b013e3181fb900d
- Williams, H. (2012). Repairing shattered lives: Brain injury and its implications for criminal justice. Retrieved from: https://www.barrowcadbury.org.uk/wp-content/uploads/2012/11/Repairing-Shattered-Lives_Report.pdf.
- World Health Organisation. (2006). International classification of functioning. World Health Organisation.
- Yardley, L. (2000). Dilemmas in qualitative health research. Psychology and Health, 15(2), 215–228. https://doi.org/10.1080/08870440008400302
- Yeates, K. O., Bigler, E. D., Abildskov, T., Dennis, M., Gerhardt, C. A., Vannatta, K., Rubin, K. H., Stancin, T., & Taylor, H. G. (2014). Social competence in paediatric traumatic brain injury: From brain to behaviour. Clinical Psychological Science, 2(1), 97–107. https://doi.org/10.1177/2167702613499734
- Yeates, K. O., Bigler, E. D., Dennis, M., Gerhardt, C. A., Rubin, K. H., Stancin, T., Taylor, H. G., & Vannatta, K. (2007). Social outcomes in childhood brain disorder: A heuristic integration of social neuroscience and developmental psychology. Psychological Bulletin, 133(3), 535–556. https://doi.org/10.1037/0033-2909.133.3.535
- Yeates, K. O., Gerhardt, C. A., Bigler, E. D., Abildskov, T., Dennis, M., Rubin, K. H., Stancin, T., Taylor, H. G., & Vannatta, K. (2013). Peer relationships of children with traumatic brain injury. Journal of the International Neuropsychological Society, 19(5), 518–537. https://doi.org/10.1017/S1355617712001531