
Abstract
Background
Mental health literacy is important as it relates to understanding mental illness, increasing help-seeking efficacy, and reducing mental illness-related stigma. One method to improve the mental health literacy of young people is a digital video intervention.
Aims
A scoping review was conducted to map existing research in the area of digital video interventions for mental health literacy among young people.
Methods
The scoping review was conducted following the PRISMA-ScR checklist. All results were screened based on our inclusion criteria.
Results
Seventeen studies were selected for analysis. In most studies (n = 14), a digital video was the only intervention whereas three studies took a multi-intervention approach. Only two of the digital video interventions were co-created with people with mental illness or university students. All studies showed positive results in favor of digital video interventions in at least one component of mental health literacy or compared to one of the comparison conditions.
Conclusions
Digital video interventions represent effective tools for enhancing mental health literacy. However, there is a need for active involvement of end-users in co-creation and to attend to the production quality so that the digital video intervention is as relevant, informed, and effective as possible.
Introduction
Good mental health is important for the well-being of adolescents and young adults. As such, improving mental health outcomes in this population has been a special focus of policymaking in more recent years (Department of Health and Department for Education, Citation2017). Adolescence and young adulthood are especially critical times to learn about mental health given that approximately 75 percent of mental health problems are developed by the age of 24 (Kessler et al., Citation2005). An objective of mental health education is to enhance mental health literacy (Kelly et al., Citation2007).
Mental health literacy is defined as “understanding how to obtain and maintain positive mental health; understanding mental disorders and their treatments; decreasing stigma related to mental disorders; and, enhancing help-seeking efficacy (knowing when and where to seek help and developing competencies designed to improve one’s mental health care and self-management capabilities)” (Kutcher et al., Citation2016, p. 155). Not only an important outcome on its own terms, mental health literacy has been linked to improved mental health (e.g. Christensen et al., Citation2004; Kitchener & Jorm, Citation2006). Although other things play a role in the incidence of mental illness, including culture, early life events, and genetics, mental health education helps people to recognize mental disorders in themselves and others and access support early (Kelly et al., Citation2007). Mental health literacy is especially timely to study considering the unprecedented levels of mental illness currently being reported among young people (Guessoum et al., Citation2020; World Health Organization, Citation2017).
Digital video interventions and mental health literacy
One method of an educational intervention to improve mental health literacy among young people is digital media. Advancement in technology allows a larger number of people, including those living in remote areas, to access information online using computers and mobile phones (Salganik, Citation2019). Therefore, digital media can be a useful tool to disseminate mental health-related information. These digital media include, among others, digital videos, such as documentaries, informational videos, and movies (Janoušková et al., Citation2017).
Digital videos have been used in several studies to enhance mental health literacy (e.g. Clement et al., Citation2012; Kaplan et al., Citation2012; Ojio et al., Citation2020). For this review, digital video interventions are defined as digital videos that are aimed at improving the mental health literacy of viewers. Past research indicates that digital video interventions of this kind, when presented in an understandable and accessible way, are a useful modality for young people as compared to other comparable educational methods, such as a workshop, emails, and handbook (Tuong et al., Citation2014). Hence, digital video intervention tools have become increasingly popular and show good signs of efficacy in terms of improving mental health literacy among young people (e.g. Koike et al., Citation2016; Yamaguchi et al., Citation2019).
Co-creation of digital video interventions
As well as being efficacious, there are other advantages of digital media interventions. Notably, these interventions are well-placed to support the mental health of young people, since the modality of delivery reflects the way in which this population is increasingly consuming information (i.e. online visual content). Similarly, digital videos are an artistic endeavour that lends themselves well to the involvement of end-users in their creation. This is sometimes referred to as “co-creation”, which is defined as “the collaborative generation of knowledge by academics working alongside stakeholders from other sectors” (Greenhalgh et al., Citation2016, p. 393). To maximize the impact of co-creation, stakeholders (e.g. end-users, mental health practitioners, carers, media producers) must be actively involved in the development, production, implementation, and evaluation of new digital media (Jirotka et al., Citation2017). Stakeholder engagement provides a valuable methodology to facilitate open and constructive dialogue that can drive the development of meaningful media interventions (Webb et al., Citation2018) and generates an inclusive and representative exchange of cross-sector perspectives revealing the complexity of issues arising from the practical challenges (e.g. defining the key message and topics/content) inherited when producing digital media interventions. Accordingly, it is crucial for researchers to co-create digital video interventions with stakeholders. Thus, in this current paper, we will review the implementation and efficacy of co-created digital video interventions.
The present review
In the present review, then, we report an overview of existing research in digital video intervention (i.e. animations, movies, videos, digital stories) for mental health literacy among young people. A few systematic reviews are available on overlapping areas of interest (e.g. Janoušková et al., Citation2017; Tay et al., Citation2018). Janoušková et al. (Citation2017) conducted a systematic review examining the role of video (e.g. movie, documentary, interview) in improving mental illness-related stigma among young people. Tay et al. (Citation2018) conducted a systematic review, investigating the effect of information and communication technologies interventions (e.g. health e-cards, link website, PowerPoint slides) to improve mental health literacy. Yet, there is no overview of whether the digital video interventions used to improve mental health literacy had been co-created with end-users. Additionally, past reviews did not include a wider variety of video interventions, such as animation and digital storytellingFootnote1, which may be particularly suited for co-creation. Thus, the objectives of this scoping review were (1) to map existing research in the effect of digital video interventions (animations, digital stories, movies, and videos) on mental health literacy (knowledge and recognition of mental illness, help-seeking efficacy, and/or attitudes/stigma related to mental disorders) among young people and (2) to review the implementation and efficacy of co-created digital video interventions.
Methods
Study design
We conducted a scoping review to map the existing literature in this research area and also to discover research gaps (Arksey & O'Malley, Citation2005; Levac et al., Citation2010). We followed the five framework stages described by Arksey and O'Malley (Citation2005). The five framework stages are: (1) identifying the research question, (2) identifying relevant studies, (3) selecting studies, (4) charting the data, and (5) collating, summarizing, and reporting the results (Arksey & O'Malley, Citation2005, p. 22). The preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) was followed (Tricco et al., Citation2018).
Search strategy and data sources
Two of the authors (SI and VS) separately conducted literature searches relevant to our research question. Based on the relevant literature found during the initial searches, three of the authors (SI, EPV, TC) selected the search terms for the current scoping review during meetings. We combined the search terms in the following groups using Boolean operators:
Young*, Child*, Adolesc*, Teen*, Youth, Juvenile*, Pupil*, Student*, School*
Animat*, Film*, Movie*, Video*, “Digital stor*”
“Mental health”, “Mental illness”, Depres*, Anxiety
Literacy, Knowledge*, Awareness, Attitude*, Stigma*, Prejudice, Help-seeking
Research, Intervention*, Evaluate*, Result*, Outcome*, Impact, Effect, Educat*, Train*, Program*
Schizophr*, Psychiatr* (exclusions)
The search terms within groups were combined with OR whereas groups were combined with AND (or NOT for the exclusion group). The search coding was created by one of the authors (YL), a computer scientist with prior experience in coding for scoping reviews. Truncations were used for the search terms. We searched databases between 10 April and 17 May 2020 and between 24 November and 26 November 2020. The databases included PsycINFO, PubMed, Web of Science, and Scopes. We also manually searched Google Scholar, ProQuest Dissertations and Theses, and reference sections of relevant papers to capture any grey literature or additional publications. All results were imported to EndNote (version X9.3.3) for screening.
Study selection and data extraction
Studies were eligible for inclusion in this review if they met the following inclusion criteria:
Population: young people (mean age range: 15–25) in pre-clinical population
Concept: digital video interventions (video, animation, movie, digital story) aimed to improve mental health literacy (knowledge and recognition of mental illness, help-seeking efficacy, and/or attitudes/stigma related to mental disorders) of the viewers. Animation, for the current study, included an animated motion picture.
Context: studies published from 2005 onwards, in the English language, in any country; empirical studies using any methods
The age range of 15 to 25 was chosen for inclusion to capture both youth and young adults (e.g. Simpson, Citation2018; United Nations, Citation2013). Studies were excluded from this review if they met the following exclusion criteria: participants were from either a younger or older population, participants were from a clinical population, interventions used were games (e.g. video games, serious games, interactive games), or the contents of the digital video were not described in enough detail. After removing duplicate records, the titles and abstracts were screened for inclusion and exclusion criteria. Full texts of the remaining papers were then screened for inclusion and exclusion criteria by three of the authors (SI, EPV, TC). For each included study, we extracted characteristics of the studies and effects of the interventions, as shown on data charts ().
Table 1. Characteristics of the sources of evidence.
Table 2. Characteristics of the sources of evidence (continued).
Table 3. Effects of the interventions.
Table 4. Effects of the interventions (continued).
Results
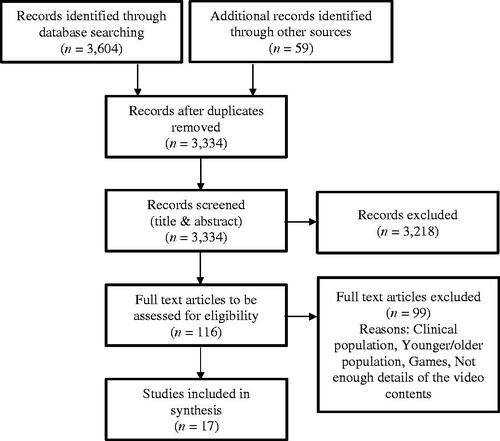
We identified 3663 studies. After removing 329 duplicates, we screened 3334 titles and abstracts for relevance. Of those, 3218 papers were excluded for not meeting our inclusion criteria. We reviewed the full texts of 116 studies. We excluded studies if the participants are from a clinical population if the mean age of the participants was younger or older than the one in our inclusion criteria, if the interventions used were games, or if the video contents were not described in enough detail. Finally, we selected 17 studies for analysis ().
Figure 1. Flow chart of study selection process.
Characteristics
The characteristics of the included studies are charted in and . Among the 17 papers, eight studies were conducted in the United States, four studies in Japan, two studies in the United Kingdom, and one study each in Canada, China, and Turkey. The majority of studies (n = 14) had only university or college students as their participants, and two studies had only secondary school students. Only one study recruited participants from outside of educational settings. The study designs included randomised controlled trial (RCT) design (n = 11), controlled before-and-after (CBA) design (n = 3), before-and-after (BA) design (n = 2), and cluster RCT (n = 1).
The majority of the digital video interventions were documentaries (n = 8). Other studies used educational, knowledge-based videosFootnote2 (n = 5), interviews (n = 3), PhotovoiceFootnote3 (n = 1), movie (n = 1), movie-clips (n = 1), mass-media videoFootnote4 (n = 1), recoding of theatrical performance (n = 1), and animation (n = 1) as at least part of the digital video intervention. Regarding the content of the digital video interventions, most interventions contained personal experience of people who underwent mental health issues (n = 13), including challenges, symptoms, and recovery, and/or factual information (n = 9), including the prevalence of mental illness, biological factors, and mental health providers.
The duration of digital video interventions ranged from 2 min to 2 h and 15 min. In most studies (n = 14), a video was the only intervention, whereas three studies took a multi-intervention approach, which included, in addition to a digital video, a lecture (n = 3), direct contact with people with mental illness (n = 1), and discussion (n = 1). In terms of co-creation, only two of the 17 studies stated that the digital video intervention used for the study had been co-created with people with mental illness (n = 1) or university students (n = 1).
The digital video interventions were compared to no intervention (n = 4), direct contact with people with mental illness (n = 3), lectures (n = 2), different mental health-related videos (n = 2), the same video but in different frequencies or order (n = 2), self-study (n = 2), simulation (n = 1), or control conditions unrelated to mental health (n = 4). Two of the studies did not have a control group as they compared scores of the same person before and after the intervention (i.e. within-subject design).
Whilst five of the studies focused on schizophrenia, other studies addressed serious mental illness or mental health in general (n = 12). Regarding the outcomes, mental health-related stigma or attitudes were examined in the majority of the studies (n = 13), and knowledge and recognition of mental illness were investigated in eight of the 17 studies. Help-seeking behavior was examined only in six of the included studies.
In four of the 17 included studies, participants responded to the outcome measurements only immediately after the intervention (i.e. post-test). Follow-up times varied between one week and 24 months (1 week: n = 3, 2 weeks: n = 4, 3 weeks: n = 1, 1 month: n = 5, 2 months: n = 1, 4 months: n = 1, 12 months: n = 1, 24 months: n = 1).
Synthesis of results
The results are organized by effects of digital video interventions on three components of mental health literacy: (1) knowledge and recognition of mental illness, (2) help-seeking efficacy, and (3) attitudes/stigma related to mental illness ( and ). Each of these sections describes single- and multi-intervention studies. Finally, we explore the studies which used digital video interventions that had been co-created with end-users.
1. Effects of the digital video interventions on knowledge and recognition of mental illness
Eight studies investigated the effects of digital video interventions on knowledge and recognition of mental illness.
A digital video as a single intervention
In five of the eight studies, a digital video was the only intervention. The majority of the digital video interventions produced outcomes in favor of the video condition. Digital video interventions that differed largely in terms of type (e.g. documentaries, the video with biomedical messages, the video with recommended messages advocated by experts) and duration (ranging between four and 30 min) enhanced knowledge of mental illness (e.g. Kern et al., Citation2017; Ojio et al., Citation2020). Ojio et al. (Citation2020) examined the effect of the educational videos (i.e. biomedical messages and recommended messages advocated by experts) on knowledge of mental illness (i.e. treatability of illness, the efficacy of medication, and social recognition) and found that the effect lasted even 12 months after the intervention. Yamaguchi et al. (Citation2019) showed that a 30-min video (i.e. interviews of people with mental illness and general mental illness-related knowledge) also improved mental illness-related knowledge (i.e. treatability of illness, the efficacy of medication, and social recognition) compared to a control condition 24 months after the intervention.
When compared to attending a lecture, mixed results were found. Owen (Citation2007) revealed that participants who watched movie clips and documentaries including myths and facts about mental illness had higher knowledge about a diagnosis of schizophrenia than those who attended a lecture on the same topic. However, Clement et al. (Citation2012) demonstrated that the levels of knowledge were not significantly different between the group who watched a documentary about personal experiences of mental illness and the group who attended a lecture covering stigma and other aspects of mental health.
Yamaguchi et al. (Citation2019) found no differences in the improvement of knowledge (i.e. treatability of illness, the efficacy of medication, and social recognition) between the group who watched the video (i.e. interviews of people with mental illness and general mental illness-related knowledge) and the group who studied mental illness on the internet independently.
A multi-intervention approach, including a digital video
Three of the eight studies took a multi-intervention approach, which includes a digital video intervention. Altindag et al. (Citation2006) showed that attending a lecture, meeting a person with schizophrenia, and watching a movie increased medical students’ knowledge about schizophrenia. Ojio (Citation2015) found that secondary school students who attended lectures about mental illness, watched animations, and had discussions about ideas to help adolescents with mental distress also increased their knowledge about mental health (e.g. symptoms, medication) after the intervention. Chan et al. (Citation2009) showed secondary school students who watched a documentary after attending a lecture showed a higher level of factual knowledge about schizophrenia (e.g. cause, treatment) than those who attended a lecture only. In contrast, secondary school students who watched a documentary before attending a lecture did not differ in the level of knowledge compared to the lecture-only group (Chan et al., Citation2009).
2. Effects of the digital video intervention on help-seeking efficacy
Six of our 17 selected studies examined the effects of digital video interventions on help-seeking.
A digital video as a single intervention
In five of the six studies, a digital video was the only intervention. All studies comparing the participants’ scores before and after the intervention showed a significant increase in intentions to seek help (Kern et al., Citation2017; Ojio et al., Citation2020; Vinson et al., Citation2016). Ojio et al. (Citation2020) found that both videos (i.e. the video with biomedical messages and the video with recommended messages advocated by experts) increased intention to seek help, and no difference in the outcome was found between the two videos. Digital video interventions also yielded significantly more positive effects on the intention to seek help compared to no intervention (Demyan & Anderson, Citation2012; Kaplan et al., Citation2012). Kaplan et al. (Citation2012) revealed that participants who watched a documentary multiple times showed more positive attitudes toward help-seeking than those who watched the same documentary only once or those who did not receive any intervention.
Vinson et al. (Citation2016) showed both listening to a live presentation (of a person discussing his experience with panic disorder) and watching the video recording of the presentation decreased concerns about seeking therapy.
A multi-intervention approach, including a digital video
Only one of the six studies on help-seeking took a multi-intervention approach, including a digital video. Ojio (Citation2015) found that secondary school students who attended a lecture about mental illness, watched animations, and had discussions about ideas to help adolescents with mental distress increased both intentions to seek help and intentions to help peers with mental health problems after the intervention.
3. Effects of the digital video intervention on attitudes/stigma related to mental illness
Thirteen studies investigated the effects of digital video interventions on attitudes and stigma related to mental illness.
A digital video as a single intervention
In eleven of the thirteen studies, a digital video was the only intervention. When compared to before watching the digital video intervention, positive attitudes toward mental illness were significantly increased after watching the video in most studies, which varied largely in terms of the type of the intervention (educational videos, interview video, documentaries) and the duration of the intervention, ranging between 4 and 10 minutes (Corrigan et al., Citation2007; Kerby et al., Citation2008; Kern et al., Citation2017; Ojio et al., Citation2020; Vinson et al., Citation2016). The only area in which mental illness-related attitude did not improve compared to before watching the video was for athletes to think less of their teammates who received mental health treatment (Kerby et al., Citation2008). Ojio et al. (Citation2020) found that both videos (the video with biomedical messages and the video with recommended messages advocated by experts) increased the future behavioral intentions to interact with people with mental health problems, and no significant difference was found between the videos.
The digital video interventions also yielded more positive outcomes in attitudes and stigma compared to a lecture (Clement et al., Citation2012), no intervention (Faigin & Stein, Citation2008), and the control interventions unrelated to mental illness (Brown et al., Citation2010; Koike et al., Citation2016; Tippin & Maranzan, Citation2019; Yamaguchi et al., Citation2019). Watching the video showed greater improvement in the intentions to contact people with mental health problems in the future than studying independently about mental illness on the internet 12 months after the intervention (Koike et al., Citation2016), but the effect did not remain significant at 24 months (Yamaguchi et al., Citation2019).
In two of the three studies comparing the digital video interventions to direct contacts (i.e. meeting people with mental illness in person), no difference was found in attitudes toward mental illness (Clement et al., Citation2012; Vinson et al., Citation2016). However, Faigin and Stein (Citation2008) found that participants who watched a live theatrical performance about mental illness showed lower stigmatizing attitudes toward people with mental illness than those who watched the recording of the performance.
A multi-intervention approach, including a digital video
Two of the thirteen studies took a multi-intervention approach containing a digital video. Altindag et al. (Citation2006) showed that participants who attended a lecture, met a person with schizophrenia, and then watched a movie decreased in a desire to have social distance from people with schizophrenia. Chan et al. (Citation2009) demonstrated that participants who watched a documentary after attending a demythologizing lecture reported lower stigmatizing attitudes and lower desire for social distance than those who only attended the lecture. Participants who watched a documentary before attending a lecture also showed more positive attitudes in terms of social distance than those who only attended the lecture although no difference was found between the two groups in stigmatizing attitudes (Chan et al., Citation2009).
Co-creation
Only two of the 17 studies used digital video interventions that had been co-created with end-users. In one study, focus groups with university students were held to develop the digital video intervention that contains positive help-seeking messages tailored to this age group (Demyan & Anderson, Citation2012). In the other study, participants watched digital videos that had been co-created with people with mental illnesses using the Photovoice approach (Tippin & Maranzan, Citation2019). These co-created interventions led to positive outcomes in all aspects assessed, including help-seeking (Demyan & Anderson, Citation2012) and attitudes and stigma toward mental illness (Tippin & Maranzan, Citation2019).
Discussion
This scoping review mapped existing research in the area of digital video interventions for mental health literacy among the non-clinical youth population. While the majority of studies assessed mental illness-related stigma and attitudes, fewer studies investigated knowledge and recognition of mental health as well as help-seeking efficacy. Large variations were found among the studies in terms of the interventions (types, durations, single intervention/multi-interventions, co-created/not co-created) and methodologies. However, all studies showed positive results in favor of digital video interventions in at least one component of mental health literacy (i.e. knowledge and recognition, help-seeking efficacy, stigma) or compared to one of the comparison conditions (e.g. no intervention). Thus, in general, participants reported an increase in knowledge and recognition of mental illness and help-seeking efficacy, and a decrease in stigmatizing attitudes (e.g. negative emotions, perceived dangerousness) and desire for social distance.
The digital video interventions seem to be particularly effective to increase help-seeking efficacy as all of the digital video interventions included in the current review increased help-seeking efficacy. Additionally, the majority of the studies revealed that digital video interventions were effective in improving knowledge and recognition of mental illness although a few studies showed that a comparison condition (a lecture or a self-study) had the same impact as the digital video intervention (Clement et al., Citation2012; Yamaguchi et al., Citation2019). Digital video interventions also improved mental illness-related attitudes in most studies though one study showed no change to think less of teammates who received mental health treatment (Kern et al., Citation2017), and another found that meeting with a person with mental illness decreased stigma more than the digital video intervention (Faigin & Stein, Citation2008). Overall, the results indicate that digital video interventions can be effective tools to increase mental health literacy among young people.
However, the balance of evidence is inconclusive given the heterogeneity in reporting and lack of clarity in video content and development in some studies. In what follows, we discuss research gaps as well as pertinent issues, including co-creation and stakeholder engagement, presentation and exploration of media interventions, and single and multi-intervention approaches. We finish by stating the limitations of the current review and recommendations and suggestions for future studies.
Co-creation and stakeholder engagement
Only two studies used digital video interventions that had been co-created with end-users. Both interventions successfully enhanced mental health literacy, including higher help-seeking efficacy (Demyan & Anderson, Citation2012) and lower mental illness-related stigma (Tippin & Maranzan, Citation2019).
Co-creation is an important practice to maximize impact on the target population as it includes end-users as essential stakeholders during the development, production, implementation, and evaluation of new digital media (Jirotka et al., Citation2017). Stakeholder engagement is one of the pillars for responsible research and innovation (RRI) and a key element for developing new media interventions in a socially desirable and acceptable way (Jirotka et al., Citation2017). When researchers co-create such interventions with young people, they must consider the wide societal implications (e.g. sustainability training/skills required to deliver the intervention) and possible problems of the new media usages in the real world (e.g. bandwidth issues in rural areas, limited mobile data) as described by Fleming et al. (Citation2018).
Digital storytelling is a powerful process for co-creation, as it allows marginalized people to script, film, and produce videos of their own stories with support from an experienced facilitator (Whitley et al., Citation2020). Digital storytelling has been found to be an effective approach to help the storytellers to process their mental health issues (De Vecchi et al., Citation2016). However, the current review found no empirical research examining if digital stories can improve the mental health literacy of the viewers, specifically of young people. The recent study by Whitley et al. (Citation2020) is the first of its kind to investigate the effect of digital stories created by people with severe mental illness on stigma in viewers, and they found that such digital stories had a positive impact on the viewers’ attitudes. Although this study was not included in the current review as the age of the viewers did not meet our inclusion criteria, the results of the study show a great potential of digital stories as an intervention to improve the mental health literacy of the viewers, including young people.
Photovoice is another type of approach, which allows co-creation, and is shown to be effective in lowering mental illness-related stigma and social distance of the viewers (Tippin & Maranzan, Citation2019). Animation is also a useful medium for co-creation, which enables anonymity for the collaborators (Dunn et al., Citation2018). However, to the best of our knowledge, no studies have examined the effects of co-created animations on mental health literacy among young people.
Presentation and exploration of media interventions
Most studies did not explicitly show links to the digital intervention that they used in their research. Whilst older studies might have had journal style requirements that prevented the authors from including links, we advise future studies to include links to the digital intervention. For researchers and media producers interested in developing new digital video interventions, this is a missed opportunity. Exploring the visual nature, editing style, contents, dialogues, scripts, and intention of the characters is vital to identify the elements that contribute to effective learning, attitudinal changes, and engagement with the media content. This rationale also applies to the tools, software, and program being used. Information, such as what programs worked well, what setup was chosen, how the documenting process was integrated within the work, would inform other researchers and provide a different starting point. While being able to see the final media product is highly advisable, it is also desirable to report the actual process of producing a digital video production. Another issue to consider is that not every project might stay online indefinitely, therefore capturing the visual nature in published literature seems also vital for archival purposes.
Single intervention approach vs. multi-intervention approach
Among the 17 studies included in this review, 14 studies used a single intervention approach (i.e. a digital video intervention was the only intervention in the study) whereas three used a multi-intervention approach (i.e. a digital video intervention was applied in combination with other interventions, such as a lecture). The results from these studies show that both approaches effectively enhance at least one component of mental health literacy (knowledge and recognition of mental illness, help-seeking efficacy, and/or attitudes/stigma related to mental disorders). No study thus far, however, has directly compared whether a single intervention approach is as effective as a multi-intervention approach concerning digital video interventions. Such comparisons can be informative given that a single intervention approach would certainly reduce the time and cost for the researchers, collaborators, participants, and ultimately end-users if the effectiveness of the two approaches is comparable.
Limitations and future directions
The current study is the first scoping review to map the effect of digital video interventions (i.e. animations, digital stories, movies, videos) on mental health literacy among the non-clinical samples of young people. This paper is also the first to explore the co-creative aspect of digital video intervention in the existing literature. The findings should help to shape and inform future research and practice.
However, several limitations of the study should be noted. First, the current review includes only studies published in English and may lack diversity in the sample. The countries in which the studies were conducted are from different parts of the world, including those with English as a non-native language (i.e. China, Japan, Turkey). However, all studies were conducted in upper-middle-income and high-income countries. As already highlighted in previous reviews, more research is still needed including lower-income countries (Janoušková et al., Citation2017). Digital video interventions may be particularly useful in such countries given the cost-effectiveness (Clement et al., Citation2012). It will also be important for future studies to compare the effects of the digital video interventions across different ethnicities, races, and cultural backgrounds (e.g. among Black, Asian and other minority ethnic communities). Second, the current review focused on the impact of digital video intervention on mental health literacy among the non-clinical youth population. It would be interesting for future studies to compare the effects of the interventions between clinical and non-clinical populations. Third, in the current review, we included digital video interventions addressing a wide range of mental health issues, including serious mental illness and schizophrenia. As some disorders, such as schizophrenia, are less common compared to others, such as depression and anxiety (WHO, Citation2019), and that people may hold different attitudes toward specific conditions (van Zelst, Citation2009), we need to be mindful of its potential effect when we develop new digital video interventions.
Future studies should be conducted in a more diverse context. In the current review, the vast majority of the studies were conducted in educational settings (i.e. schools, colleges, and universities). Therefore, future researchers should evaluate the effectiveness of digital video interventions, which are delivered in other contexts, for example, where young people can access their smartphones, TVs, or computers. Such an approach can also help the digital intervention to reach a wider audience, with more diverse backgrounds, such as in education, socioeconomic status, and culture.
As discussed, future researchers should co-create a digital video intervention with end-users and show it as an intervention to viewers. Certain media and approaches, such as digital storytelling, Photovoice, and animation, may be particularly suited for co-creation. Additionally, interventions should incorporate specific issues and pressures young people currently face, such as the impact of social media on anxiety and depressed mood (Thorisdottir et al., Citation2019), the effects of the current Covid-19 pandemic on social isolation (Brooks et al., Citation2020), as well as new contemporary issues linked to perfectionism (Curran & Hill, Citation2019). Hence, it is crucial to involve young people as well as other stakeholders in identifying these new mediating factors.
External validity, scalability, and dissemination/curation strategies of certain interventions are also important aspects to consider in future methods or analyses to further understand the extent to which results can be generalized beyond each study. Another challenge is the diversity of study designs and outcome measures used, preventing meta-analyses or comparable summary effects. A related issue was that very few studies preregistered their methods and analyses, making it difficult to know what and how it was developed, and the intended analyses to be conducted. As we move forward, it will be important for researchers to pre-register their methods and archive their materials on an open science framework.
Conclusions
Digital video interventions represent effective tools for engaging audiences. This review indicates that although the extent of this efficacy is mixed, there is nevertheless a pattern of findings that trend in the direction of the video interventions. But these are tentative conclusions, and the balance of evidence is inconclusive given the lack of clarity in video content and development in some studies and heterogeneity in reporting. In particular, there is a need for the active involvement of end-users in co-creation and to attend to the production quality so that the digital video intervention is as relevant, informed, and effective as possible.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 A creative arts process, which is used to capture a personal story, using video, imagery, music, and voice (Lambert, Citation2010).
2 The focus of the videos was on mental illness-related knowledge, such as biological mechanism.
3 A grassroots process by which members of a marginalised group, such as people with mental illness, document and convey their experience” (Tippin & Maranzan, Citation2019, p. 1), using participant-produced photos, participatory analysis (e.g. interpreting the photos through discussions), and narrative summaries (e.g. explaining how the photos call attention to a specific theme)
4 The video was presented within public service announcements in a commercial television programming style.
References
- Altindag, A., Yanik, M., Ucok, A., Alptekin, K., & Ozkan, M. (2006). Effects of an antistigma program on medical students’ attitudes towards people with schizophrenia. Psychiatry and Clinical Neurosciences, 60(3), 283–288. https://doi.org/10.1111/j.1440-1819.2006.01503.x
- Arksey, H., & O'Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
- Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–920. https://doi.org/10.1016/S0140-6736(20)30460-8
- Brown, S. A., Evans, Y., Espenschade, K., & O'Connor, M. (2010). An examination of two brief stigma reduction strategies: Filmed personal contact and hallucination simulations. Community Mental Health Journal, 46(5), 494–499. https://doi.org/10.1007/s10597-010-9309-1
- Chan, J. Y., Mak, W. W., & Law, L. S. (2009). Combining education and video-based contact to reduce stigma of mental illness: “The Same or Not the Same” anti-stigma program for secondary schools in Hong Kong. Social Science & Medicine, 68(8), 1521–1526. https://doi.org/10.1016/j.socscimed.2009.02.016
- Christensen, H., Griffiths, K. M., & Jorm, A. F. (2004). Delivering interventions for depression by using the internet: Randomised controlled trial. British Medical Journal, 328(7434), 260–265. https://doi.org/10.1136/bmj.37945.566632.EE
- Clement, S., Van Nieuwenhuizen, A., Kassam, A., Flach, C., Lazarus, A., De Castro, M., McCrone, P., Norman, I., & Thornicroft, G. (2012). Filmed v. live social contact interventions to reduce stigma: Randomised controlled trial. British Journal of Psychiatry, 201(1), 57–64. https://doi.org/10.1192/bjp.bp.111.093120
- Corrigan, P. W., Larson, J., Sells, M., Niessen, N., & Watson, A. C. (2007). Will filmed presentations of education and contact diminish mental illness stigma? Community Mental Health Journal, 43(2), 171–181. https://doi.org/10.1007/s10597-006-9061-8
- Curran, T., & Hill, A. P. (2019). Perfectionism is increasing over time: A meta-analysis of birth cohort differences from 1989 to 2016. Psychological Bulletin, 145(4), 410–429. https://doi.org/10.1037/bul0000138
- De Vecchi, N., Kenny, A., Dickson-Swift, V., & Kidd, S. (2016). How digital storytelling is used in mental health: A scoping review. International Journal of Mental Health Nursing, 25(3), 183–193. https://doi.org/10.1111/inm.12206
- Demyan, A. L., & Anderson, T. (2012). Effects of a brief media intervention on expectations, attitudes, and intentions of mental health help seeking. Journal of Counseling Psychology, 59(2), 222–229. https://doi.org/10.1037/a0026541
- Department of Health and Department for Education (2017). Transforming children and young people’s mental health provision: a Geen Paper. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/664855/Transforming_children_and_young_people_s_mental_health_provision.pdf
- Dunn, V., O’Keeffe, S., Stapley, E., & Midgley, N. (2018). Facing shadows: Working with young people to coproduce a short film about depression. Research Involvement and Engagement, 4(1), 46. https://doi.org/10.1186/s40900-018-0126-y
- Faigin, D. A., & Stein, C. H. (2008). Comparing the effects of live and video-taped theatrical performance in decreasing stigmatization of people with serious mental illness. Journal of Mental Health, 17(6), 594–606. https://doi.org/10.1080/09638230701505822
- Fleming, T., Bavin, L., Lucassen, M., Stasiak, K., Hopkins, S., & Merry, S. (2018). Beyond the trial: Systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. Journal of Medical Internet Research, 20(6), e199. https://doi.org/10.2196/jmir.9275
- Greenhalgh, T., Jackson, C., Shaw, S., & Janamian, T. (2016). Achieving research impact through co-creation in community-based health services: Literature review and case study. The Milbank Quarterly, 94(2), 392–429. https://doi.org/10.1111/1468-0009.12197
- Guessoum, S. B., Lachal, J., Radjack, R., Carretier, E., Minassian, S., Benoit, L., & Moro, M. R. (2020). Adolescent psychiatric disorders during the COVID-19 pandemic and lockdown. Psychiatry Research, 291, 113264. https://doi.org/10.1016/j.psychres.2020.113264
- Janoušková, M., Tuskova, E., Weissova, A., Trancik, P., Pasz, J., Evans-Lacko, S., & Winkler, P. (2017). Can video interventions be used to effectively destigmatize mental illness among young people? A systematic review. European Psychiatry, 41, 1–9. https://doi.org/10.1016/j.eurpsy.2016.09.008
- Jirotka, M., Grimpe, B., Stahl, B., Eden, G., & Hartswood, M. (2017). Responsible research and innovation in the digital age. Communications of the ACM, 60(5), 62–68. https://doi.org/10.1145/3064940
- Kaplan, S. A., Vogel, D. L., Gentile, D. A., & Wade, N. G. (2012). Increasing positive perceptions of counseling: The importance of repeated exposures. The Counseling Psychologist, 40(3), 409–442. https://doi.org/10.1177/0011000011414211
- Kelly, C. M., Jorm, A. F., & Wright, A. (2007). Improving mental health literacy as a strategy to facilitate early intervention for mental disorders. The Medical Journal of Australia, 187(S7), S26–S30. https://doi.org/10.5694/j.1326-5377.2007.tb01332.x
- Kerby, J., Calton, T., Dimambro, B., Flood, C., & Glazebrook, C. (2008). Anti-stigma films and medical students’ attitudes towards mental illness and psychiatry: Randomised controlled trial. Psychiatric Bulletin, 32(9), 345–349. https://doi.org/10.1192/pb.bp.107.017152
- Kern, A., Heininger, W., Klueh, E., Salazar, S., Hansen, B., Meyer, T., & Eisenberg, D. (2017). Athletes connected: Results from a pilot project to address knowledge and attitudes about mental health among college student-athletes. Journal of Clinical Sport Psychology, 11(4), 324–336. https://doi.org/10.1123/JCSP.2016-0028
- Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
- Kitchener, B. A., & Jorm, A. F. (2006). Mental health first aid training: Review of evaluation studies. Australian & New Zealand Journal of Psychiatry, 40(1), 6–8. https://doi.org/10.1080/j.1440-1614.2006.01735.x
- Koike, S., Yamaguchi, S., Ojio, Y., Ohta, K., Shimada, T., Watanabe, K., Thornicroft, G., & Ando, S. (2016). A randomised controlled trial of repeated filmed social contact on reducing mental illness-related stigma in young adults. Epidemiology and Psychiatric Sciences, 27(2), 199–208. https://doi.org/10.1017/S2045796016001050
- Kutcher, S., Wei, Y., & Coniglio, C. (2016). Mental health literacy: Past, present, and future. The Canadian Journal of Psychiatry, 61(3), 154–158. https://doi.org/10.1177/0706743715616609
- Lambert, J. (2010). Digital storytelling cookbook. Digital Diner Press.
- Levac, D., Colquhoun, H., & O'Brien, K. K. (2010). Scoping studies: Advancing the methodology. Implementation Science, 5(1), 69. https://doi.org/10.1186/1748-5908-5-69
- Ojio, Y. (2015, July 3). Development of a mental health literacy program for secondary school students and its effects: In-school mental health literacy education. Working Paper Series in Young Scholar Training Program, Center for Excellence in School Education, Graduate School of Education, The University of Tokyo.
- Ojio, Y., Yamaguchi, S., Ohta, K., Ando, S., & Koike, S. (2020). Effects of biomedical messages and expert-recommended messages on reducing mental health-related stigma: A randomised controlled trial. Epidemiology and Psychiatric Sciences, 29, e74. https://doi.org/10.1017/S2045796019000714
- Owen, P. (2007). Dispelling myths about schizophrenia using film. Journal of Applied Social Psychology, 37(1), 60–75. https://doi.org/10.1111/j.0021-9029.2007.00147.x
- Salganik, M. J. (2019). Bit by bit: Social research in the digital age. Princeton University Press.
- Simpson, A. R. (2018). Changes in young adulthood. https://hr.mit.edu/static/worklife/youngadult/changes.htm
- Tay, J. L., Tay, Y. F., & Klainin-Yobas, P. (2018). Effectiveness of information and communication technologies interventions to increase mental health literacy: A systematic review. Early Intervention in Psychiatry, 12(6), 1024–1037. https://doi.org/10.1111/eip.12695
- Thorisdottir, I. E., Sigurvinsdottir, R., Asgeirsdottir, B. B., Allegrante, J. P., & Sigfusdottir, I. D. (2019). Active and passive social media use and symptoms of anxiety and depressed mood among Icelandic adolescents. Cyberpsychology, Behavior, and Social Networking, 22(8), 535–542. https://doi.org/10.1089/cyber.2019.0079
- Tippin, G. K., & Maranzan, K. A. (2019). Efficacy of a photovoice‐based video as an online mental illness anti‐stigma intervention and the role of empathy in audience response: A randomized controlled trial. Journal of Applied Social Psychology, 49(6), 381–394. https://doi.org/10.1111/jasp.12590
- Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850
- Tuong, W., Larsen, E. R., & Armstrong, A. W. (2014). Videos to influence: A systematic review of effectiveness of video-based education in modifying health behaviors. Journal of Behavioral Medicine, 37(2), 218–233. https://doi.org/10.1007/s10865-012-9480-7
- United Nations (2013). Definition of youth. https://www.un.org/esa/socdev/documents/youth/fact-sheets/youth-definition.pdf
- van Zelst, C. (2009). Stigmatization as an environmental risk in schizophrenia: A user perspective. Schizophrenia Bulletin, 35(2), 293–296. https://doi.org/10.1093/schbul/sbn184
- Vinson, E. S., Abdullah, T., & Brown, T. L. (2016). Mental illness stigma intervention in African Americans examining two delivery methods. Journal of Nervous and Mental Disease, 204(5), 400–403. https://doi.org/10.1097/NMD.0000000000000458
- Webb, H., Koene, A., Patel, M., & Vallejos, E. P. (2018, July). Multi-stakeholder dialogue for policy recommendations on algorithmic fairness [Paper presentation]. Proceedings of the 9th International Conference on Social Media and Society, Copenhagen, Denmark. https://doi.org/10.1145/3217804.3217952
- Whitley, R., Sitter, K. C., Adamson, G., & Carmichael, V. (2020). Can participatory video reduce mental illness stigma? Results from a Canadian action-research study of feasibility and impact. BMC Psychiatry, 20(1), 16. https://doi.org/10.1186/s12888-020-2429-4
- World Health Organization. (2017). Depression and other common mental disorders: Global health estimates. http://apps.who.int/iris/bitstream/10665/254610/1/WHO-MSD-MER-2017.2-eng.pdf?ua=1
- World Health Organization. (2019). Mental disorders. https://www.who.int/news-room/fact-sheets/detail/mental-disorders
- Yamaguchi, S., Ojio, Y., Ando, S., Bernick, P., Ohta, K., Watanabe, K. I., Thornicroft, G., Shiozawa, T., & Koike, S. (2019). Long-term effects of filmed social contact or internet-based self-study on mental health-related stigma: A 2-year follow-up of a randomised controlled trial. Social Psychiatry and Psychiatric Epidemiology, 54(1), 33–42. https://doi.org/10.1007/s00127-018-1609-8