
Abstract
Background
Staff working in people-oriented professions are vulnerable to burnout which is negatively associated with professional well-being and service-user care.
Aim
To investigate if interventions based on Acceptance and Commitment Therapy (ACT) are effective in reducing staff burnout.
Method
Systematic database and reference list searches were conducted resulting in the inclusion of 14 quantitative papers. A narrative synthesis, including extraction of individual effect sizes, was performed.
Results
All studies were controlled trials. The settings for ACT delivery were varied across health, social care, and public services. The ACT interventions demonstrated statistically significant effects in favour of ACT on the outcome measure subscales across the majority of studies (n = 9). Thirteen studies demonstrated an effect in favour of ACT in at least one outcome measure subscale. Positive aspects of work engagement varied according to a professional role.
Conclusions
The findings suggest that ACT-based interventions using a wide range of formats may have the potential to decrease burnout across a range of professional groups. However, samples were small in the studies reviewed and the interventions were not always defined. Further research would benefit from larger studies, incorporating process measures, with explicit protocols.
Introduction
People-oriented professions have been recognised as holding particular risks for professionals through burnout (Maslach & Goldberg, Citation1998). Burnout has been defined as “a syndrome of emotional exhaustion, depersonalization, and reduced personal accomplishment that can occur among individuals who do ‘people work’…” (Maslach, Citation1982, p. 3). Schaufeli and Buunk (Citation2003) consider burnout to be a specific chronic and multifaceted form of occupational stress including specifically the development of negative attitudes and behaviours towards service-users, the job, and the organisation (Schaufeli & Buunk, Citation2003). Thus, burnout is distinct from occupational stress and warrants specific attention in the context of the potential harm to staff and service users. Many measures have been utilised to measure burnout: see Platsidou and Daniilidou (Citation2016) and Qiao and Schaufeli (Citation2011) for brief overviews.
Professional burnout
Burnout has significant personal implications for staff including low mood, anxiety, hopelessness, physical symptoms, and memory and attentional difficulties (Lizano, Citation2015; PHE, Citation2016; Schaufeli & Buunk, Citation2003). In the mental health setting, burnout prevalence is estimated to be between 21 and 67% (Morse et al., Citation2012) and has been associated with negative service-user outcomes, such as lower service-user safety (Kowalski et al., Citation2010), negative attributions towards service-user behaviours (Bethay et al., Citation2009), disrupted care through staff turnover (Morse et al., Citation2012) and predictive of increased stigma towards mental illness by psychiatrists (Yavuz et al., Citation2020). These factors clearly impact service-user care. Staff well-being has been explicitly linked to National Health Service (NHS) quality and service-user care. NHS organisations that prioritised staff well-being achieved enhanced performance, improved patient care, and reduced staff absence (DoH, Citation2009). Greater support for staff well-being, emphasising the consequent impact on sustainable services, has also been called for in the joint Charter for Psychological Staff Well-being and Resilience (BPS, Citation2016).
Although burnout is considered a specific form of workplace stress, research into the more generic form is useful to understand the broader context considering burnout is often included within work stress reviews. Many attempts to address staff burnout through individual and systemic changes have been made. A Cochrane review of approaches to preventing occupational stress in healthcare workers (Marine et al., Citation2009) reported limited evidence for the effectiveness of person-directed interventions. The review included a range of interventions: cognitive-behavioural therapy, relaxation, music, massage, and multicomponent interventions. Encouragingly, a further review of burnout within mental health services, reported that 60% of included interventions effectively reduced burnout (Morse et al., Citation2012). Interventions in the second review included varied interventions: psychodynamic, cognitive-behavioural, supervision, psychosocial, and assertiveness.
Acceptance and commitment therapy
More recently, third-wave cognitive behavioural therapies including Acceptance and Commitment Therapy (ACT) have been utilised positively to address workplace stress and effectiveness (Flaxman et al., Citation2013; Moran, Citation2015). ACT is based on Relational Frame Theory (RFT) with philosophical roots in functional contextualism (Hayes et al., Citation2006). RFT posits that human language and cognition are bound into the ability to identify and generate relational links symbolically between stimuli; and are regulated by the relational context and the functional context of the behaviour (Hayes et al., Citation2006). ACT-based interventions have been utilised successfully to reduce stress reported by health care staff including support staff working with intellectual disabilities (McConachie et al., Citation2014) clinical psychology trainees (Stafford-Brown & Pakenham, Citation2012), and nurses (Bailey et al., Citation2021). Given the positive application of ACT within workplaces, the potential effectiveness of ACT to target burnout is of interest.
The focus of change with ACT is in the context of the distress rather than the content. Increasing psychological flexibility is central to the ACT model and intervention focus. Hayes et al. (Citation2006) describe the six processes of psychological flexibility as (a) acceptance: embracing private events without seeking to change them, (b) cognitive defusion: changing the interaction with one’s thoughts to diminish unhelpful function, (c) self as context: the context of verbal knowing rather than the content of knowing, (d) being present: experiencing the world directly, (e) values: qualities of purposive action, and (f) committed action: concrete goals consistent with values. The theory of change within ACT interventions is measured through these processes of psychological flexibility. In contrast, psychopathology in the ACT model is identified through six corresponding opposite processes of psychological inflexibility.
Psychological flexibility has been associated with increased openness to the acceptance of setbacks in the working environment for healthcare workers and the continued pursuit of valued living and working (Ramaci et al., Citation2019). Value congruence has been positively associated with greater staff well-being (Sagiv & Schwartz, Citation2000) and lower burnout (Veage et al., Citation2014). Furthermore, reduced value congruence has been associated with increased burnout (Towey-Swift & Whittington, Citation2021). Moreover, mindfulness and values-based processes have demonstrated a stronger and more consistent relationship with burnout than work-site factors (Vilardaga et al., Citation2011).
In summary, burnout has deleterious consequences for staff, service-users, and systems and research has evaluated the effectiveness of ACT in different populations, including those suffering from workplace stress. Thus, systematically examining the effectiveness of ACT in addressing burnout is timely and relevant to clinicians who have a role in supporting professional staff groups and systems. This review adopted a broad approach to defining professional groups to capture this emerging area of study. While idiosyncratic contributions to burnout may vary across and within professional groups, the concept as defined by Maslach (Citation1982) is the common experience. Furthermore, the ACT model is flexible and transdiagnostic (Gloster et al., Citation2020) so is broadly applicable.
Review question
Are interventions based on Acceptance and Commitment Therapy (ACT) effective in reducing burnout in staff groups?
Method
Protocol
The review followed a predetermined protocol (submitted to the University of Liverpool); however, the protocol was not formally registered with Prospero before the study. The key details are identified below. The search and screening activities were conducted in line with PRISMA guidance (www.prisma-statement.org).
Inclusion and exclusion criteria
Studies were selected for inclusion in the review if they satisfied the following predefined inclusion criteria:
The population under investigation was identified as a staff group in any profession.
The intervention was named explicitly as primarily an ACT intervention regardless of delivery format (no specific components were required to be included).
There was a comparator of any format.
Either burnout or compassion fatigue was assessed by any validated tool as an outcome measure.
The report was published in English.
As “work stress” is a large area of research that may subsume the concept of burnout, this term was included in the search strategy. Similarly, the Professional Quality of Life model incorporates “burnout” and “secondary traumatic stress” under the superordinate construct of “compassion fatigue” (Stamm, Citation2010) so the latter two terms were also included in the search strategy. However, identified studies were screened in relation to the inclusion criteria specified above.
While any measure deployed to measure burnout was eligible, the most widely used measure of burnout is the Maslach Burnout Inventory (MBI; Maslach et al., Citation1996). The MBI contains three subscales: emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA). High scores on EE and DP equate to high burnout but high scores on PA relate to high accomplishment (i.e. low burnout).
The requirement for the study to be published in English was due to the resource limitations of the project. Both peer-reviewed and grey literature studies were eligible. No additional exclusion criteria were specified.
Search strategy and selection criteria
The following databases were searched from their inception for articles published up until the end of September 2020 CINAHLplus, MEDLINE, PsychARTICLES, PsychINFO, PubMed, Science Direct, Scopus, Web of Science, and Open Grey. The search terms were based on the following combination: [(burnout OR compassion fatigue OR secondary traumatic stress, OR work stress) AND (Acceptance and Commitment Therapy OR Acceptance Commitment Therapy)]. There were no limiters to the searches.
Inclusion decisions were made in two stages. At stage 1 (screening), duplicates were removed, all titles and abstracts were reviewed for initial eligibility, and reasons for exclusion were recorded. At stage 2 (eligibility), the full-text articles identified as potentially eligible were obtained and reviewed again against the criteria to establish eligibility. At stage 1, a sample of 99 (42%) articles was independently screened by two of the authors. There was 96% agreement between these reviewers yielding a kappa of 0.86. At stage 2, all 50 studies were independently screened by two authors. There was 94% agreement between these reviewers yielding a kappa of 0.77. Disagreements at both stages were resolved through discussion or referral to the third author. The authors work in university and clinical settings and have expertise related to systematic review methods gained through peer-reviewed research and doctoral training. EndNote reference manager software was used to organise the initial search but no further software was used to screen or extract from studies.
Data extraction
Data on key pre-specified variables were extracted from the included studies under the following headings: study identifying information, author and year; participant details, staff group, and number; country; attrition; method; intervention; comparator; outcome measures; findings related to the burnout measure; test time points and follow-up details (see ). Three aspects of study design were also evaluated: randomisation, attrition, and missing value analysis. Data was also systematically extracted from each included study in line with the quality assessment tool displayed in . The quality of included studies was assessed by the Quality Assessment Tool for Studies with Diverse Design (QATSDD; Sirriyeh et al., Citation2012). This tool was selected due to its applicability to diverse research designs, and also its detailed 4-point rating format enabling more fine-grained assessments (range: not at all, very slightly, moderately, complete). Calculating a percentage score for each study to aid comparison is suggested. However, this was not calculated here as summary scores can be potentially misleading and lacking detail (O’Connor et al., Citation2015). The QATSDD gives equal weighting to each item of the tool, whereas the impact of each item on quality and bias is variable.
Table 1. Quality assessment.
Table 2. Study characteristics.
Data synthesis
This review used a narrative synthesis approach including quantitative extraction of effect sizes for each individual study. However, there was substantial heterogeneity in participant samples, intervention comparators, and the format and delivery of the intervention within the overall ACT framework. For these reasons, a meta-analysis was not considered to be appropriate. Data were not combined across studies, but effect sizes for the burnout outcome for ACT compared to control were calculated for each study to create a basis for common comparison across the sample.
Results
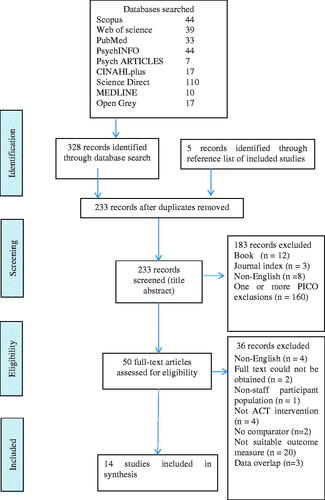
After de-duplication, 233 articles were screened at Stage 1, 50 full-text articles were reviewed at Stage 2, of which fourteen were included in the synthesis (see ).
Figure 1. Study selection flow diagram.
Quality assessment
Quality assessment ratings are reported in . Fenton et al. (Citation2015) suggest using the QATSDD as a dialogue instrument to enhance an in-depth understanding of the paper’s strengths and limitations. In this review, QATSDD ratings were scrutinised for the themes of quality and the impact on the research. All studies provided moderate to complete details regarding data collection, recruitment data, and fit of data collection. The majority (all but one) provided moderate to complete details regarding the: explicit theoretical framework, objectives of the research, research setting, fit of the method of analysis, and evaluation of the strengths and limitations. While the studies largely reported reliability and validity of the outcome measures used, few reported re-test within their own dataset. None of the studies detailed user involvement in the research planning or design. Consideration of appropriate sample size in the analysis was limited, possibly limiting the statistical power of the studies.
Study considerations
Randomisation
Thirteen studies were Randomised Controlled Trials (RCTs): five used randomly generated computer programmes for allocation (Barrett & Stewart Citation2020, Brinkborg et al., Citation2011; Clarke, Taylor, Bolderston, et al., Citation2015; Clarke, Taylor, Lancaster, et al., Citation2015; Luoma et al., Citation2007). The remaining eight were randomised but no specific details of the random sequence generation were provided. One additional study was a non-randomised Controlled Clinical Trial (CCT), allocating participants based on participant scheduling availability (Emery Citation2012).
Attrition
Attrition rates were calculated from the total number of participants recruited, with participants included at the study endpoint. Attrition rates varied from 2% to 23% across conditions (see ). There was 80% or greater total participation in eight studies (Bethay et al., Citation2013; Brinkborg et al., Citation2011; Emery, Citation2012; Habibian et al. Citation2018, Hayes et al., Citation2004; Luoma & Vilardaga, Citation2013; Macías et al. Citation2019; Puolakanaho et al. Citation2020). Where attrition rates were reported separately for each condition, attrition across intervention and control conditions were similar, except Brinkborg et al. (Citation2011) where attrition was solely within the ACT condition. Where attrition reasons were reported (Barrett & Stewart, Citation2020; Bethay et al., Citation2013; Brinkborg et al., Citation2011; Clarke, Taylor, Bolderston, et al., Citation2015; Luoma & Vilardaga, Citation2013), these were reported as unknown/non-contactable, or within the themes of illness, schedule commitments, unrelated life event, technological difficulties, and changed mind. In two studies (Frögéli et al., Citation2019; Lloyd et al., Citation2013), no reasons for attrition were given. However, both studies reported no significant differences between responders and non-responders on the studied variables. Interestingly, Puolakanaho et al. (Citation2020) detected key differences at different study phases; finding no differences between dropouts or participants during the intervention stage, but observed higher burnout scores for dropouts in the pre-intervention stage; and during the follow-up phase, those who dropped out were less stressed with fewer psychological symptoms. Attrition reasons for the remaining six studies were not reported or unknown. The risk of bias from attrition for the majority of studies was limited by the high overall participation, and relatively similar attrition rates between conditions. Thus significant risk of bias from attrition is not presumed.
Missing data
Missing data were addressed through intention to treat (ITT) analysis in five studies (Barrett & Stewart, Citation2020; Brinkborg et al., Citation2011; Clarke, Taylor, Bolderston, et al., Citation2015; Clarke, Taylor, Lancaster, et al., Citation2015; Frögéli et al., Citation2019) and the “last data carried forward” method in one study (Luoma et al. Citation2007), limiting the bias in these studies. Of these five studies, three had high attrition (49% or greater; Clarke, Taylor, Bolderston, et al., Citation2015; Clarke, Taylor, Lancaster, et al., Citation2015; Frögéli et al., Citation2019). Four studies excluded participants with incomplete data from analysis (Bethay et al., Citation2013; Emery, Citation2012; Lloyd et al., Citation2013; Puolakanaho et al., Citation2020) possibly reducing the statistical power of the research. Three studies did not specify how they managed missing data (Hayes et al., Citation2004; Luoma & Vilardaga, Citation2013; Macías et al., Citation2019). Finally, Habibian et al. (Citation2018) reported no missing data. Consequently, the risk of bias for incomplete data is unclear.
Study characteristics
The included studies were published between 2004 and 2020. Summary details are outlined in . The studies were conducted in eight countries: five in the USA, three in the UK, two in Sweden, and one each in Finland, Iran, and Spain, with a further study recruiting multi-nationally from Ireland, the USA, and the Philippines. Ten studies were carried out with health and social care staff, two with unspecified government employees, one with teachers, and one with staff from various professions. The sample sizes, taken as the number of participants assessed at baseline, ranged from 22 to 168 participants. The total number of participants across the review was 1130.
The ACT interventions varied in length from one to eight sessions (median = 3 sessions) and of the nine studies reporting the intervention hours, interventions were delivered over 4.5–16 total hours (median = 9 h). In all but one study (Macías et al., Citation2019); the main ACT interventions were delivered in a group format. One study was delivered online (Barrett & Stewart, Citation2020). There were more studies with an active comparator intervention (alternative intervention: n = 9) than studies with inactive (waiting-list) controls. For the comparator, six studies used alternative educational teaching sessions, two used alternative therapeutic approaches, and one used reflection seminars.
Study design
All studies were controlled trials: thirteen RCTs and one non-randomised CCT. Two studies (Bethay et al., Citation2013; Luoma et al., Citation2007) combined the ACT intervention with additional training: Applied Behavioural Analysis (ABA) or Group Drug Counselling (GDC) implementation, respectively. The ABA and GDC training were used as the control condition, allowing for any additive effect of ACT to be measured. Three studies augmented ACT workshops with ACT-based continued input between sessions consisting of eight 1.5-h weekly face-to-face consultations (Luoma et al., Citation2007), six telephone consultations (Luoma & Vilardaga, Citation2013), and daily internet-based practice (Puolakanaho et al. Citation2020). The remaining ten studies delivered the ACT intervention as a standalone intervention. The protocols for the ACT interventions were available for five studies and referenced in three. Of those referenced, one protocol was retrieved (Frögéli et al., Citation2019) and the psychological flexibility processes were summarised in another (Lloyd et al., Citation2013). Of the available seven protocols or outlines, all explicitly identified addressing: values, committed action, and defusion. From available information Bethay et al. (Citation2013) and Lloyd et al. (Citation2013) addressed all areas of psychological flexibility apart from “self as context”; Macías et al. (Citation2019) addressed all but “present moment focus”, and Clarke, Taylor, Lancaster, et al. (Citation2015) addressed all but “acceptance” and “self as context”. The remaining three studies addressed all six processes.
There were two possible post-intervention assessment time points across the studies: immediately after completion of the intervention (post-intervention), and longer-term (follow-up). Eleven studies (all except Barrett & Stewart, Citation2020; Brinkborg et al., Citation2011; Macías et al., Citation2019) employed follow-up data collection points, ranging from 4 to 36 months post-intervention (median = 4 months). Two studies reported only pre-intervention and follow-up burnout outcome measures (Emery, Citation2012; Luoma & Vilardaga, Citation2013). Lloyd et al. (Citation2013) employed a four-point assessment: baseline, post-intervention (taken between workshops), and follow-up. The remaining six studies reported pre-intervention, post-intervention, and follow-up outcomes.
All but three studies (Habibian et al. Citation2018; Lloyd et al., Citation2013; Macías et al. Citation2019) reported on baseline comparisons between the intervention and control group. Nine studies reported no significant differences between groups at baseline: five reported outcome measure comparability, three reported demographic comparability, and one reported both. Clarke, Taylor, Lancaster, et al. (Citation2015) found baseline differences whereby the ACT group were significantly older with higher burnout scores at baseline than the comparator group (this was controlled for in analysis). Lloyd et al. (Citation2013) did not report baseline comparisons for the total sample but reported comparability between the intervention and control baseline measures related to attrition.
Burnout measures
The majority of the studies (n = 11) used the Maslach Burnout Inventory (MBI; Maslach et al., Citation1996) to measure burnout. The MBI was reported in three different ways: separate subscales, combined subscales (EE and DP), and total scores. One study used the Maslach and Jackson MBI (MJBI; Maslach & Jackson) containing three subscales similar to the standard MBI: EE, DP, and self-decreasing achievement. One study used the Bergen Burnout Inventory (BBI-15; Näätänen et al., Citation2003). The BBI-15 measures the same three theoretical domains as the MBI. Another used the Scale of Work Engagement and Burnout (SWEBO; Hultell & Gustavsson, Citation2010). The SWEBO contains two subscales, one measuring burnout and one measuring work engagement. In both subscales, high scores indicate high occurrence. Bethay et al. (Citation2013) additionally used the Burnout Believability Scale (BBS), adapted from the MBI to assess the believability of selected items.
Impact of ACT on burnout
Nine studies reported a statistically significant improvement in at least one measure of burnout compared to controls from baseline to post-intervention or follow-up. Of these, seven reported both post-intervention and follow-up data; all but one (Frögéli et al., Citation2019) found that improved burnout scores compared to baseline were sustained at follow-up. A further study reported reduced burnout but no significant group-by-time interaction (Barrett & Stewart, Citation2020). Clarke, Taylor, Bolderston, et al. (Citation2015) reported a statistically significant increase in burnout post-ACT intervention, before returning to pre-intervention levels at follow-up. Three studies found no statistically significant impact of ACT on burnout (Bethay et al., Citation2013; Clarke, Taylor, Lancaster, et al., Citation2015; Habibian et al., Citation2018). However, in Clarke, Taylor, Lancaster, et al.’s (Citation2015) study the burnout scores were higher for the ACT group than the control at baseline.
Effect size (ES)
The effect size was calculated to provide a common metric for comparison. Cohen’s d was calculated for each burnout measure based on between group measures at the last observation (i.e. follow-up data where reported or post-intervention only). reports the obtained effect sizes. As discussed, meta-analysis was considered but was not judged appropriate due to the heterogeneity of the participant populations and the interventions especially in the range of comparators, divergent formats, and unconfirmed content of the ACT interventions.
Table 3. Effect size of burnout measures between ACT intervention and control groups.
Most observed MBI ESs were in the predicted direction reporting reduced EE, DP, C, and increased PA/PE with effect sizes ranging from 0.2 to 0.5 which are considered small or moderate in size (Cohen, 1988, cited in Ellis, Citation2010, p. 41). The studies reporting a medium effect in burnout change scores all utilised samples of counsellors and health and social care staff and employed both waiting-list and active control comparisons.
The study reporting the largest effect (d = 3.19; Macías et al., Citation2019) utilised government staff delivering three individual sessions and yielding large ES in favour of ACT across all burnout subscales in the study. A large effect was also reported in reduced DP following six sessions with nursing staff (Habibian et al., Citation2018).
There were exceptions to these positive trends. Four studies demonstrated an effect in favour of the control group in one or two MBI subscales. In relation to the ACT condition: Brinkborg et al. (Citation2011) revealed lower PA (moderate ES) and Habibian et al. (Citation2018) also found lower PA (large ES). Bethay et al. (Citation2013) reported lower PA (small ES) and higher DP (large ES), and Luoma and Vilardaga (Citation2013) showed burnout (combined EE and DP) was higher in the ACT supplemented condition (small ES). Nonetheless, the remaining burnout subscales in these studies had ES in favour of the ACT condition. Two studies, using total scores, reported an effect in favour of controls. Frögéli et al. (Citation2019), utilising the SWWEBO, revealed a small ES in favour of control at 3 year follow-up; Barrett and Stewart (Citation2020), utilising the MBI, found a medium ES in favour of control at post-test. Both these studies had active control comparators.
Theory of change
Due to the largely unknown content of the ACT interventions, the theoretical processes of change within the ACT interventions were examined as part of the evidence synthesis of this review. Specifically, measures of psychological flexibility were examined. Three studies (Bethay et al., Citation2013; Habibian et al. Citation2018; Luoma et al., Citation2007) did not include process measures. Eleven studies included process measures of acceptance and action, believability, values, or mindful awareness. Eight studies measuring acceptance and action used versions of the Acceptance and Action Questionnaire (AAQ) and work-related AAQ. In mediation analysis, AAQ acceptance accounted for variance in burnout scores in three of the studies (Emery, Citation2012; Lloyd et al., Citation2013; Puolakanaho et al., Citation2020). Luoma and Vilardaga (Citation2013) reported increased acceptance and action over time with large between group effects in favour of intervention. Barrett and Stewart (Citation2020) reported no effect for condition or interaction but reported a significant negative correlation between burnout and WAAQ. Clarke, Taylor, Bolderston, et al. (Citation2015) did not examine the interaction with burnout, but the acceptance scores tracked the same pattern as burnout scores. Two studies (Barrett & Stewart, Citation2020; Brinkborg et al., Citation2011) reported no significant interaction between acceptance and burnout scores. However, in Brinkborg et al. (Citation2011) AAQ scores were high pre-intervention, giving little room for improvement (the mean score equated to 71% of the possible total score). Puolakanaho et al. (Citation2020) reported psychological flexibility mediated burnout; as measured through the processes of mindfulness, acceptance, and action, and automatic thought believability. Clarke, Taylor, Lancaster, et al. (Citation2015) measured valued living and reported no association between burnout and values scores. Emery (Citation2012) measured personal values, but values did not explain variance in burnout. Frögéli et al. (Citation2019) reported that changes in burnout were mediated by experiential avoidance and mindful awareness.
Discussion
This review examined the current research evidence for the effectiveness of ACT-based interventions in reducing burnout in staff groups. A systematic search strategy was employed, identifying fourteen research studies for inclusion in the review. The ACT interventions were varied in delivery format and eleven of fourteen had a statistically significant impact on burnout in the desired direction compared to both waiting-list and active controls. The interventions returned effects in favour of ACT in the majority of subscales measured across studies. There is therefore moderate support for ACT interventions to reduce burnout across a range of professional settings. The weight of the evidence reviewed was in favour of ACT being an effective intervention to target burnout in staff groups. While this was observed across various group delivery formats, the greatest effect size was seen for the individually delivered intervention.
A narrative approach was adopted for this review due to the heterogeneity of the ACT intervention formats. Specifically the risk of unacceptable variability between interventions was unquantifiable as protocols were largely unavailable. While there were many similarities between studies, combining the results would not have been meaningful. Nonetheless, all of the studies reviewed were controlled trials, and thirteen were randomised, lending strength to the evidence base reviewed here. The majority of ACT interventions did have a statistically significant impact on burnout as compared to controls. However, the specific content of the ACT interventions was unclear and process measures were not routinely used. Therefore, there is limited evidence from which to promote a definitive conclusion that a specific type of ACT is an effective intervention for reducing staff burnout or to conclude which of the specific elements may be contributing the most effect.
While the population heterogeneity in the professions studied further prevents firm conclusions from being drawn about the effectiveness of ACT within a particular professional group, it does conversely however support preliminary assumptions about the broad applicability of the approach across varied staff groups.
Quality
The overall quality of studies reviewed was moderate to complete as rated by the QATSDD implying the findings were acceptably robust in this respect. The majority of studies were thorough and explicit in the theoretical framework, research design, and data collection, but there were small sample sizes and/or high attrition. None of the studies detailed user involvement in the design of the research. The impact of this absence is unknown but given workload (impacting schedule commitments) was cited as a reason for attrition (Barrett & Stewart, Citation2020; Brinkborg et al., Citation2011; Lloyd et al., Citation2013) participant involvement in design may have been useful to tailor a delivery format compatible with pressured services.
In addition to the QATSDD rating, potential methodological bias was reviewed. Measurement bias was low given the self-report nature and choice of the MBI measure in all but two studies. While the MBI is the most widely used burnout measure and has contributed to advancements in the field of burnout research, there are criticisms of it. Researchers have considered a personal accomplishment to be a consequence rather than a component of burnout, the MBI to have an exclusive focus on emotional functions, and the three-factor focus to be too narrow (Moreno-Jiménez et al., Citation2012). Nonetheless, the factor structure of the MBI has been demonstrated to be consistent across different languages and across countries with highly divergent health systems (Poghosyan et al., Citation2009). The MBI is considered the “gold standard” burnout measure (Maslach et al., Citation2009). The consistent use of the MBI and BBI gives confidence to the construct being measured and the reliability of comparison between studies. However, the randomisation method was not explicit or was inadequately defined for half of the studies and could have reduced the validity of the trials if it was flawed. The risk of bias from the non-blinding of participants and researchers was unclear but assumed to be moderately high across all included studies. The theoretical underpinnings of ACT are explicit in the interventions and the impossibility of blinding participants when the therapy involves engagement with the theoretical rationale has been acknowledged (Button & Munafo, Citation2015). This is reflective of challenges faced by psychotherapy research generally and does not set ACT apart from other psychological models in terms of the strength with which conclusions can be drawn.
Impact of ACT on burnout
The ACT interventions returned effects in favour of ACT for reducing burnout in eleven of the fourteen studies when compared to both waiting-list and active controls. Due to varied reporting of statistical significance in analyses, and the limitations of this approach to deduce effectiveness (Ellis, Citation2010), effect sizes were calculated to examine the practical significance through a common comparator. The study reporting the largest effect in burnout scores in favour of ACT was individually delivered. The studies observing large or medium effects (Cohen, 1988, cited in Ellis, Citation2010, p. 41) incorporated varied control conditions and had divergent intervention formats. Thus, the effectiveness of ACT interventions in reducing self-reported burnout scores in the staff groups reviewed appears robust regardless of the delivery format. Despite five studies not finding statistically significant effects of ACT on burnout, the calculated effect size of ACT vs. comparator for these studies were in favour of ACT in four of these studies: medium to large in one study, and small in the remaining three studies. Of note, one of these studies reported higher burnout scores for the ACT group at baseline compared to the comparator group possibly, therefore, underestimating the impact of ACT at follow-up. These findings are in keeping with broader burnout research, and show the magnitude of the effect size for ACT to be comparable if not slightly larger than for other comparator interventions. Meta-analysis of burnout interventions for mental health providers revealed person-directed interventions having a positive effect of small magnitude (Dreison et al., Citation2018). Meta-analysis of controlled studies testing the impact of other interventions on employee burnout including CBT, relaxation, interpersonal skills, and role-related skills revealed significant results for exhaustion and general burnout scales but effect sizes were small (Maricuţoiu et al., Citation2016).
Statistically significant results and effect sizes in favour of ACT were observed across both active and inactive control groups. This was consistent with the review of meta-analyses of ACT interventions, which found effects for ACT compared to non-active control and the majority of active control excluding specific therapy comparators (Gloster et al., Citation2020). Button and Munafo (Citation2015) assert comparison with waiting-list likely overestimates effectiveness, whereas comparison with active controls likely underestimates effectiveness. As the included studies contained active and inactive controls this potentially provides balance to the evidence, and concerns about non-specific therapeutic effects are less indicated.
Awa et al. (Citation2010) conclude in their review of burnout prevention that intervention programmes are beneficial and can be enhanced with refresher sessions. The current review identified both face-to-face and telephone ACT-based continued input had an effect on burnout levels. Indicating continued input or refresher sessions could be provided flexibly to meet individual needs and adapted to fit within operational constraints.
Professional role and efficacy
There appears to be a relationship between professional role and personal accomplishment. Half of the studies reporting no effect for ACT were in relation to personal accomplishment (PA) and involved frontline care staff: direct care staff and social workers. In contrast, studies reporting PA effects in favour of ACT all utilised staff holding therapy roles. Previous research has observed significant differences in personal efficacy across different occupational positions and settings (Ray et al., Citation2013). Adams et al.’s (Citation2017) systematic review of burnout across different professions observed higher PA amongst counsellors than social workers. They considered that counsellors work in more limited contexts with smaller groups and inbuilt boundaries which may be protective in relation to burnout. This suggests personal efficacy may interact with the professional role and influence the success of interventions targeting burnout for the PA domain.
Theory of change
Despite notable differences between the included studies, the theory of change in the ACT model was partially supported. In line with the ACT theoretical assertion, measures of: “acceptance and action”, “believability”, and “mindful awareness”, were found to account for variance in burnout measures in the ACT intervention groups in this review. In further analysis of Puolakanaho et al.’s (Citation2020) data, Kinnunen et al. (Citation2020) demonstrated improving mindfulness facets, specifically non-judging, mediated the improvement in burnout dimensions. The therapeutic process of “values” was however not uniquely associated with burnout within this review. While the process measure findings provide a reassuring indication of the therapeutic mechanism, ACT process measures were not consistently utilised or reported. The strength and interaction effects of the six ACT processes on burnout are not possible to comment upon.
Burnout and attrition
Attrition is an important issue for interventions to be sustainable and effectively implemented in real-world practice. Although reasons for attrition were largely unknown, workload pressures were identified in three studies (Barrett & Stewart, Citation2020; Brinkborg et al., Citation2011; Lloyd et al., Citation2013). Burnout has an established relationship with workload (Morse et al., Citation2012) and workload pressures (PHE, Citation2016). Within this review, Puolakanaho et al. (Citation2020) found participants who dropped out pre-intervention had significantly higher burnout scores than those remaining in the study. Furthermore, Bethay et al. (Citation2013) only found a statistically significant impact of ACT on burnout when participants were stratified by distress. Consequently, those with increased distress may benefit most but may be absent from studies. Future research needs to be vigilant for the crossover of burnout correlates impacting upon attrition.
Strengths and limitations of the review
This review has several strengths and limitations. The predefined focus on a clearly defined ACT intervention combined with the inclusion of largely consistent trial designs and outcome measures enables some robust comparisons across studies to be made, notwithstanding the heterogeneity across these studies in certain detailed aspects. A second researcher independently cross-checked a sample of screened articles although doing this for all articles and extracted data would have been preferable Nonetheless, there was substantial agreement between researchers on the sample that was crosschecked. The quality tool QATSDD did provide valuable information about the quality of included studies but it was limited as it did not fully address potential bias; however, this was mitigated by addressing bias separately. The quality rating was not second-rated which would have been preferable, but unlikely to have significantly impacted the review findings. The sample sizes for all studies were modest at best, which limits the possible conclusions that can be derived from the research without meta-analysis. With small sample sizes, any difference between intervention and control risks being due to chance, or important differences may be missed (Bland, Citation2008) which weakens the strength of any conclusions concerning effectiveness.
Future research
Looking to the future, it would be beneficial to investigate a standardised ACT intervention protocol across different settings in larger samples or explicitly to identify the ACT processes being targeted. This may allow for meaningful future meta-analysis. Including process measures and their interaction with burnout measures would be valuable in establishing the effectiveness of the ACT interventions.
Conclusion
ACT interventions in this review were associated with a statistically significant reduction in burnout scores in half the included studies and an effect in favour of ACT compared to comparator on at least one burnout subscale in all but two studies. There is cautious optimism therefore that ACT-based interventions may have the potential to decrease burnout. But there is insufficient evidence at this time to identify ACT as a treatment of choice for burnout. Further large-scale studies with treatment protocols and comprehensive process measures are required. While the argument can be made that an intervention is better than no intervention, findings indicate that ACT is an encouraging area of further exploration in the field of burnout.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adams, C. J., Hough, H., Proeschold-Bell, R. J., Yao, J., & Kolkin, M. (2017). Clergy burnout: A comparison study with other helping professions. Pastoral Psychology, 66(2), 147–175. https://doi.org/10.1007/s11089-016-0722-4
- Awa, W. L., Plaumann, M., & Walter, U. (2010). Burnout prevention: A review of intervention programs. Patient Education and Counseling, 78(2), 184–190. https://doi.org/10.1016/j.pec.2009.04.008
- Bailey, A. K., Sawyer, A. T., & Robinson, P. S. (2021). A psychoeducational group intervention for nurses: Rationale, theoretical framework, and development. Journal of the American Psychiatric Nurses Association, 1–9. Epub ahead of print. https://doi.org/10.1177/10783903211001116
- Barrett, K., & Stewart, I. (2020). A preliminary comparison of the efficacy of online acceptance and commitment therapy (ACT) and cognitive behavioural therapy (CBT) stress management interventions for social and healthcare workers. Health and Social Care in the Community, 29, 113–126. https://doi.org/10.1111/hsc.13074
- Bethay, J.S., Wilson, K., G., & Moyer, K. H. (2009). Acceptance and commitment therapy training for work stress and burnout in mental health direct care providers. In J. T. Blackledge, J. Ciarrochi, & F. P. Deane (Eds.), Acceptance and commitment therapy: Contemporary theory, research and practice (pp. 223–246). Australian Academic Press.
- Bethay, J. S., Wilson, K. G., Schnetzer, L. W., Nassar, S. L., & Bordieri, M. J. (2013). A controlled pilot evaluation of acceptance and commitment training for intellectual disability staff. Mindfulness, 4(2), 113–121. https://doi.org/10.1007/s12671-012-0103-8
- Bland, M. (2008, July). Some problems with sample size. Paper Presented at the Joint Meeting of the Dutch Pathological Society and the Pathological Society of Great Britain & Ireland, Leeds, UK.
- Brinkborg, H., Michanek, J., Hesser, H., & Berglund, G. (2011). Acceptance and commitment therapy for the treatment of stress among social workers: A randomized controlled trial. Behaviour Research and Therapy, 49(6–7), 389–398. https://doi.org/10.1016/j.brat.2011.03.009
- British Psychological Society (2016). Charter for psychological staff wellbeing and resilience. Retrieved from http://www.bps.org.uk/system/files/Public%20files/Comms-media/press_release_and_charter.pdf
- Button, K., S., & Munafo, M. R. (2015). Addressing risk of bias in trials of cognitive behavioral therapy. Shanghai Archives of Psychiatry, 27(3), 144–148. https://doi.org/10.11919/j.issn.1002-0829.215042
- Clarke, S., Taylor, G., Lancaster, J., & Remington, B. (2015). Acceptance and commitment therapy based self-management versus psychoeducation training for staff caring for clients with a personality disorder: A randomized controlled trial. Journal of Personality Disorders, 29(2), 163–176. https://doi.org/10.1521/pedi_2014_28_149
- Clarke, S., Taylor, G., Bolderston, H., Lancaster, J., & Remington, B. (2015). Ameliorating patient stigma amongst staff working with personality disorder: Randomized controlled trial of self-management versus skills training. Behavioural and Cognitive Psychotherapy, 43(6), 692–704. https://doi.org/10.1017/S1352465814000320
- Department of Health (2009). NHS health and well-being. Final report, November 2009. Department of Health.
- Dreison, K., C., Luther, L., Bonfils, K., A., Sliter, M.T., Grew, J., H., & Salyers, M., P. (2018). Job burnout in mental health providers: A meta-analysis of 35 years of intervention research. Journal of Occupational Health Psychology, 23(1), 18–30. https://doi.org/10.1037/ocp0000047
- Ellis, P. D. (2010). The essential guide to effect sizes. Cambridge University Press.
- Emery, D. W. (2012). Crisis in education: A call to ACT (72), ProQuest Information & Learning, US. Retrieved from ProQuest database http://gateway.proquest.com/openurl?url_ver=Z39.88-2004&rft_val_fmt=info:ofi/fmt:kev:mtx:dissertation&res_dat=xri:pqdiss&rft_dat=xri:pqdiss:3466610
- Fenton, L., Lauckner, H., & Gilbert, R. (2015). The QATSDD critical appraisal tool: comments and critiques. Journal of Evaluation in Clinical Practice, 21(6), 1125–1128. https://doi.org/10.1111/jep.12487
- Flaxman, P. E., Bond, F. W., & Livheim, F. (2013). The mindful and effective employee. New Harbinger Publications Inc.
- Frögéli, E., Rudman, A., & Gustavsson, P. (2019). Preventing stress-related ill health among future nurses: Effects over 3 years. International Journal of Stress Management, 26(3), 272–286. https://doi.org/10.1037/str0000110
- Gloster, A. T., Walder, N., Levin, M. E., Twohig, M. P., & Karekla, M. (2020). The empirical status of acceptance and commitment therapy: A review of meta-analyses. Journal of Contextual Behavioral Science, 18, 181–192. https://doi.org/10.1016/j.jcbs.2020.09.009
- Habibian, Z., Sadri, Z., & Nazmiyeh, H. (2018). Effects of group acceptance and commitment therapy-based training on job stress and burnout among pediatric oncology and special disease nurses. Iranian Journal of Pediatric Hematology & Oncology, 8(2), 118–125.
- Hayes, S. C., Bissett, R., Roget, N., Padilla, M., Kohlenberg, B. S., Fisher, G., Masuda, A., Pistorello, J., Rye, A. K., Berry, K., & Niccolls, R. (2004). The impact of acceptance and commitment training and multicultural training on the stigmatizing attitudes and professional burnout of substance abuse counselors. Behavior Therapy, 35(4), 821–835. https://doi.org/10.1016/S0005-7894(04)80022-4
- Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and commitment therapy: Model, processes and outcomes. Behaviour Research and Therapy, 44(1), 1–25. https://doi.org/10.1016/j.brat.2005.06.006
- Hultell, D., & Gustavsson, J. (2010). A psychometric evaluation of the Scale of Work Engagement and Burnout (SWEBO). Work, 37(3), 261–274. https://doi.org/10.3233/WOR-2010-1078
- Kinnunen, S., M., Puolakanaho, A., Tolvanen, A., Mäkikangas, A., & Lappalainen, R. (2020). Improvements in mindfulness facets mediate the alleviation of burnout dimensions. Mindfulness, 11(12), 2779–2792. https://doi.org/10.1007/s12671-020-01490-8
- Kowalski, C., Driller, E., Ernstmann, N., Alich, S., Karbach, U., Ommen, O., Schulz-Nieswandt, F., & Pfaff, H. (2010). Associations between emotional exhaustion, social capital, workload, and latitude in decision-making among professionals working with people with disabilities. Research in Developmental Disabilities, 31(2), 470–479. https://doi.org/10.1016/j.ridd.2009.10.021
- Lizano, E. L. (2015). Examining the impact of job burnout on the health and well-being of human service workers: A systematic review and synthesis. Human Service Organizations Management Leadership & Governance, 39(3), 167–181. https://doi.org/10.1080/23303131.2015.1014122
- Lloyd, J., Bond, F. W., & Flaxman, P. E. (2013). The value of psychological flexibility: Examining psychological mechanisms underpinning a cognitive behavioural therapy intervention for burnout. Work & Stress, 27(2), 181–199. https://doi.org/10.1080/02678373.2013.782157
- Luoma, J. B., Hayes, S. C., Twohig, M. P., Roget, N., Fisher, G., Padilla, M., Bissett, R., Holt, C., & Kohlenberg, B. (2007). Augmenting continuing education with psychologically focused group consultation: Effects on adoption of group drug counseling. Psychotherapy, 44(4), 463–469. https://doi.org/10.1037/0033-3204.44.4.463
- Luoma, J. B., & Vilardaga, J. P. (2013). Improving therapist psychological flexibility while training acceptance and commitment therapy: A pilot study. Cognitive Behaviour Therapy, 42(1), 1–8. https://doi.org/10.1080/16506073.2012.701662
- Macías, J., Valero-Aguayo, L., Bond, F. W., & Blanca, M. J. (2019). The efficacy of functional-analytic psychotherapy and acceptance and commitment therapy (FACT) for public employees. Psicothema, 31(1), 24–29. https://doi.org/10.7334/psicothema2018.202
- Maricuţoiu, L. P., Sava, F. A., & Butta, O. (2016). The effectiveness of controlled interventions on employees’ burnout: A meta-analysis. Journal of Occupational and Organizational Psychology, 89(1), 1–27. https://doi.org/10.1111/joop.12099
- Marine, A., Ruotsalainen, J. H., Serra, C., & Verbeek, J. H. (2009). Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews, 2009(1), 1–42. https://doi.org/10.1002/14651858.CD002892.pub2
- Maslach, C. (1982). Burnout–The cost of caring. Prentice-Hall International.
- Maslach, C., & Goldberg, J. (1998). Prevention of burnout: New perspectives. Applied and Preventive Psychology, 7(1), 63–74. https://doi.org/10.1016/S0962-1849(98)80022-X
- Maslach, C., Jackson, S. E., & Leiter, M. P. (1996). The Maslach Burnout Inventory (3rd ed.). Consulting Psychologists Press.
- Maslach, C., Leiter, M., & Schaufeli, W. B. (2009). Measuring burnout. In S. Cartwright & C. L. Cooper (Eds.), The Oxford handbook of organizational well-being (pp. 86–108). Oxford University Press.
- McConachie, D. A. J., McKenzie, K., Morris, P. G., & Walley, R. M. (2014). Acceptance and mindfulness-based stress management for support staff caring for individuals with intellectual disabilities. Research in Developmental Disabilities, 35(6), 1216–1227. https://doi.org/10.1016/j.ridd.2014.03.005
- Moran, D. J. (2015). Acceptance and commitment training in the workplace. Current Opinion in Psychology, 2, 26–31. https://doi.org/10.1016/j.copsyc.2014.12.031
- Moreno-Jiménez, B., Barbaranelli, C., Galvez, H. M., & Garrosa Hernández, E. (2012). The physician burnout questionnaire: A new definition and measure. TPM Testing, Psychometrics, Methodology in Applied Psychology, 19, 325–344.
- Morse, G., Salyers, M., Rollins, A., Monroe-DeVita, M., & Pfahler, C. (2012). Burnout in mental health services: A review of the problem and its remediation. Administration and Policy in Mental Health, 39(5), 341–352. https://doi.org/10.1007/s10488-011-0352-1
- Näätänen, P., Aro, A., Matthiesen, S., & Salmela-Aro, K. (2003). Bergen Burnout Indicator-15. Edita.
- O’Connor, S. R., Tully, M. A., Ryan, B., Bradley, J. M., Baxter, G. D., & McDonough, S. M. (2015). Failure of a numerical quality assessment scale to identify potential risk of bias in a systematic review: A comparison study. BMC Research Notes, 8(1), 224–230. https://doi.org/10.1186/s13104-015-1181-1
- Platsidou, M., & Daniilidou, A. (2016). Three scales to measure burnout of primary school teachers: Empirical evidence on their adequacy. International Journal of Educational Psychology, 5(2), 164–186. https://doi.org/10.17583/ijep.2016.1810
- Poghosyan, L., Aiken, L. H., & Sloane, D. M. (2009). Factor structure of the Maslach Burnout Inventory: An analysis of data from large scale cross-sectional surveys of nurses from eight countries. International Journal of Nursing Studies, 46(7), 894–902. https://doi.org/10.1016/j.ijnurstu.2009.03.004
- Public Health England (2016). Interventions to prevent burnout in high risk individuals: Evidence review. Public Health England.
- Puolakanaho, A., Tolvanen, A., Kinnunen, S. M., & Lappalainen, R. (2020). A psychological flexibility-based intervention for burnout: A randomised controlled trial. Journal of Contextual Behavioral Science, 15, 52–67. https://doi.org/10.1016/j.jcbs.2019.11.007
- Qiao, H., & Schaufeli, W. B. (2011). The convergent validity of four burnout measures in a Chinese sample: A confirmatory factor-analytic approach. Applied Psychology, 60 (1), 87–111. https://doi.org/10.1111/j.1464-0597.2010.00428.x
- Ramaci, T., Bellini, D., Presti, G., & Santisi, G. (2019). Psychological flexibility and mindfulness as predictors of individual outcomes in hospital health workers. Frontiers in Psychology, 10, 1302. https://doi.org/10.3389/fpsyg.2019.01302
- Ray, S. L., Wong, C., White, D., & Heaslip, K. (2013). Compassion satisfaction, compassion fatigue, worklife conditions, and burnout among frontline mental health care professionals. Traumatology, 19(4), 255–267. https://doi.org/10.1177/1534765612471144
- Sagiv, L., & Schwartz, S. (2000). Value priorities and subjective well-being: Direct relations and congruity effects. European Journal of Social Psychology, 30(2), 177–198. https://doi.org/10.1002/(SICI)1099-0992(200003/04)30:2<177::AID-EJSP982>3.0.CO;2-Z
- Schaufeli, W. B., & Buunk, B. P. (2003). Burnout: An overview of 25 years of research and theorizing. In M. J. Schabracq, J. A. M. Winnubst, & C. L. Cooper (Eds.), The handbook of work & health psychology (2nd ed., pp. 383–425). John Wiley & Son.
- Sirriyeh, R., Lawton, R., Gardner, P., & Armitage, G. (2012). Reviewing studies with diverse designs: The development and evaluation of a new tool. Journal of Evaluation in Clinical Practice, 18(4), 746–752. https://doi.org/10.1111/j.1365-2753.2011.01662.x
- Stafford-Brown, J., & Pakenham, K. I. (2012). The effectiveness of an ACT informed intervention for managing stress and improving therapist qualities in clinical psychology trainees. Journal of Clinical Psychology, 68(6), 592–513. https://doi.org/10.1002/jclp.21844
- Stamm, B. H. (2010). The Concise ProQOL Manual (2nd ed.). ProQOL.org.
- Towey-Swift, K., & Whittington, R. (2021). Person-job congruence, compassion and recovery attitude in Community Mental Health Teams. Journal of Mental Health Online, 30(4), 431–439. https://doi.org/10.1080/09638237.2019.1608931
- Veage, S., Deane, F. R., Andresen, R., Oades, L. G., Crowe, T. P., & Ciarrochi, J. (2014). Value congruence, importance and success and in the workplace: Links with well-being and burnout amongst mental health practitioners. Journal of Contextual Behavioral Science, 3(4), 258–264. https://doi.org/10.1016/j.jcbs.2014.06.004
- Vilardaga, R., Luoma, J. B., Hayes, S. C., Pistorello, J., Levin, M. E., Hildebrandt, M. J., Kohlenberg, B., Roget, N. A., & Bond, F. (2011). Burnout among the addiction counseling workforce: The differential roles of mindfulness and values-based processes and work-site factors. Journal of Substance Abuse Treatment, 40(4), 323–335. https://doi.org/10.1016/j.jsat.2010.11.015
- Yavuz, K. F., Nalbant, A., Ulusoy, S., Esen, B., Burhan, H. S., & Kara, T. (2020). Burned out and avoided: Stigmatizing processes among psychiarists. Medicina Academica Mostariensia, 8(1–2), 463–470.